Motor Control Training for the Shoulder with Smart Garments



 and
and
Abstract
:
1. Introduction
2. Technologies for Shoulder Posture Monitoring
3. System Design and Development
3.1. Requirements
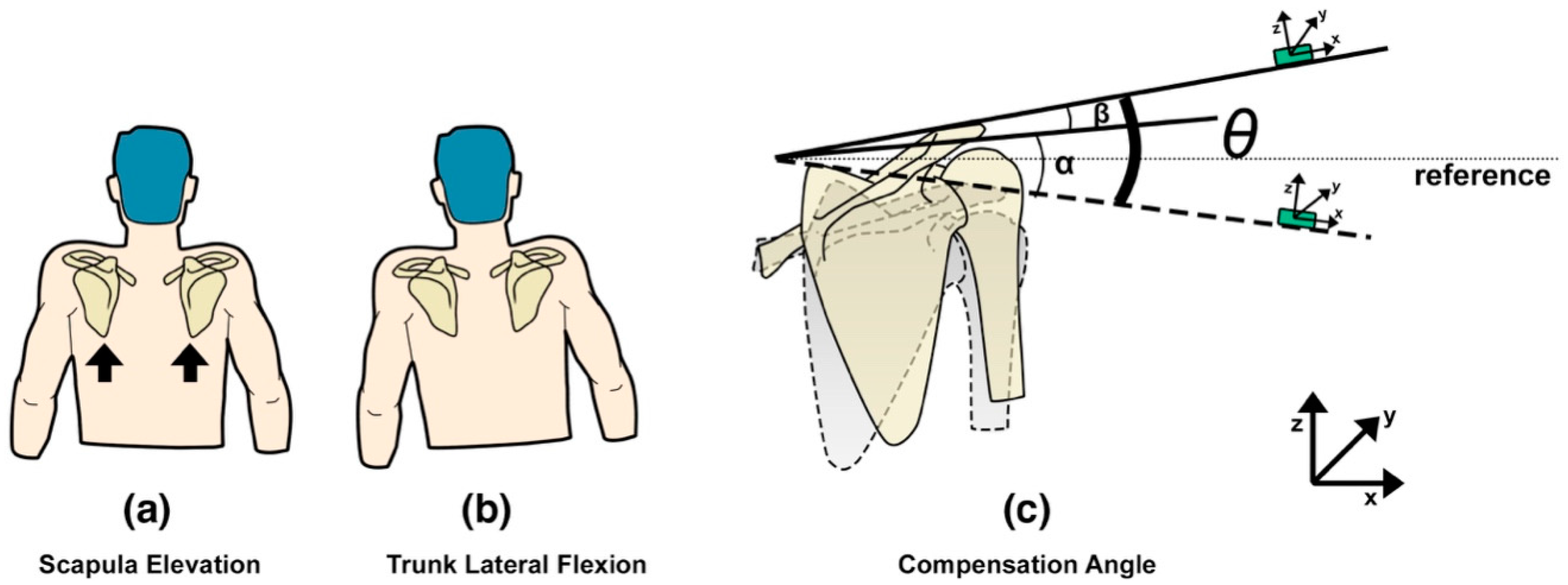
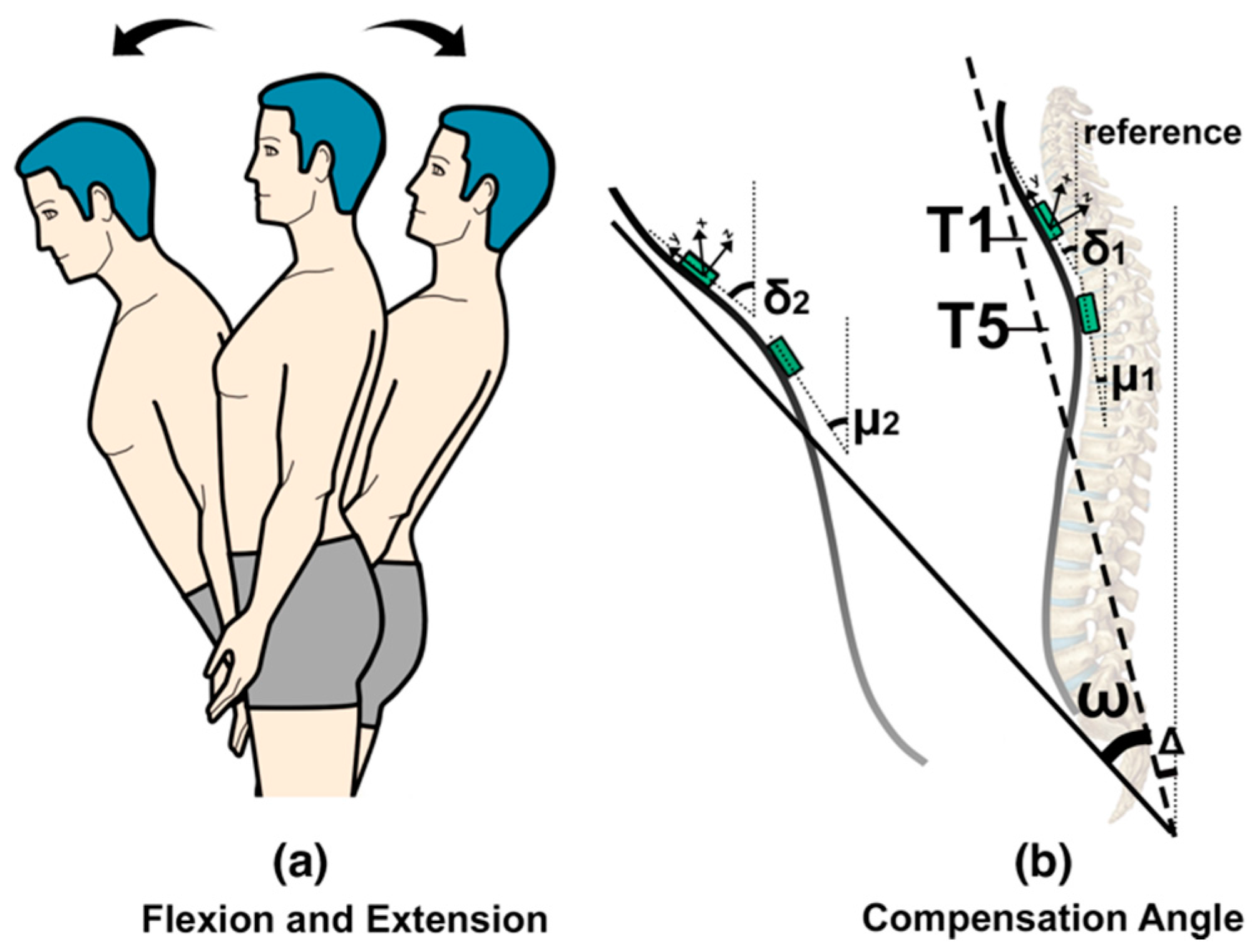
3.2. Calculation Methods
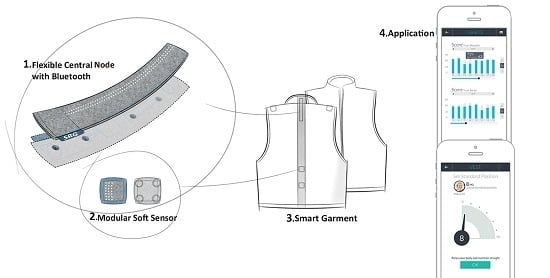
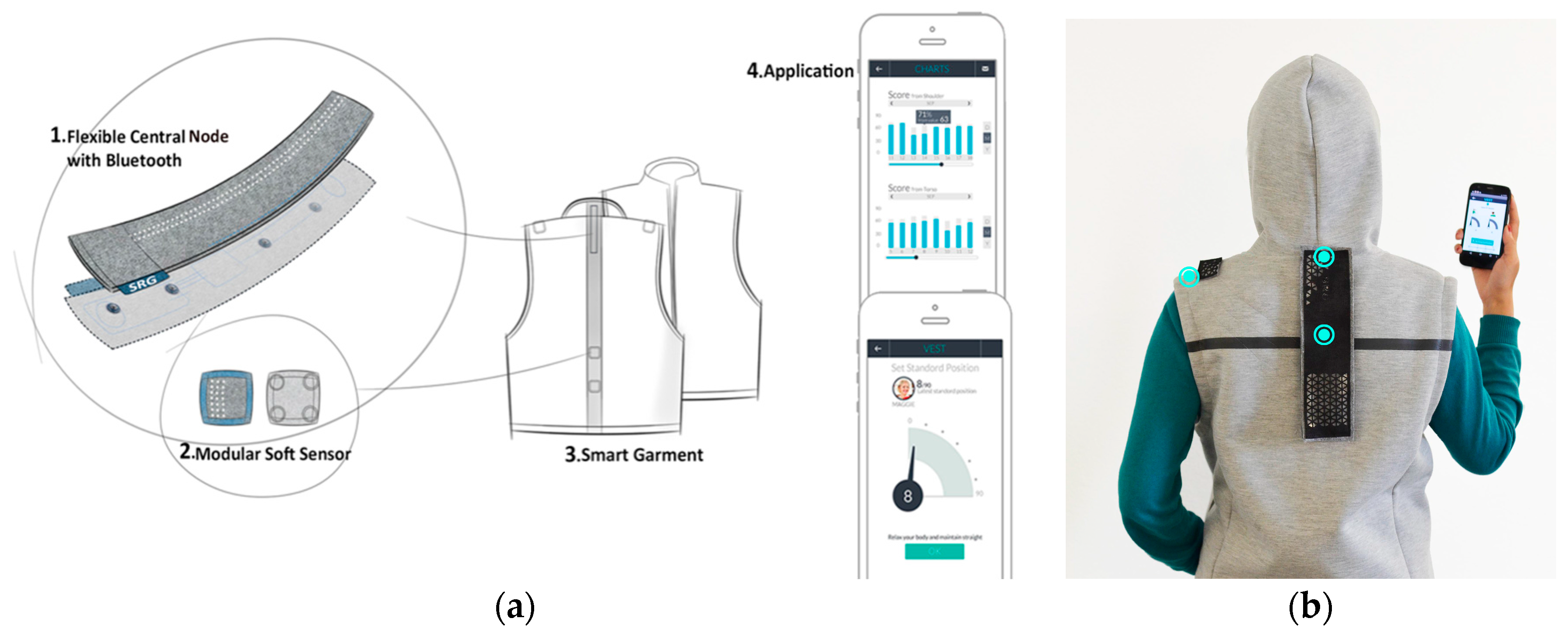
3.3. Zishi Concept and System Overview
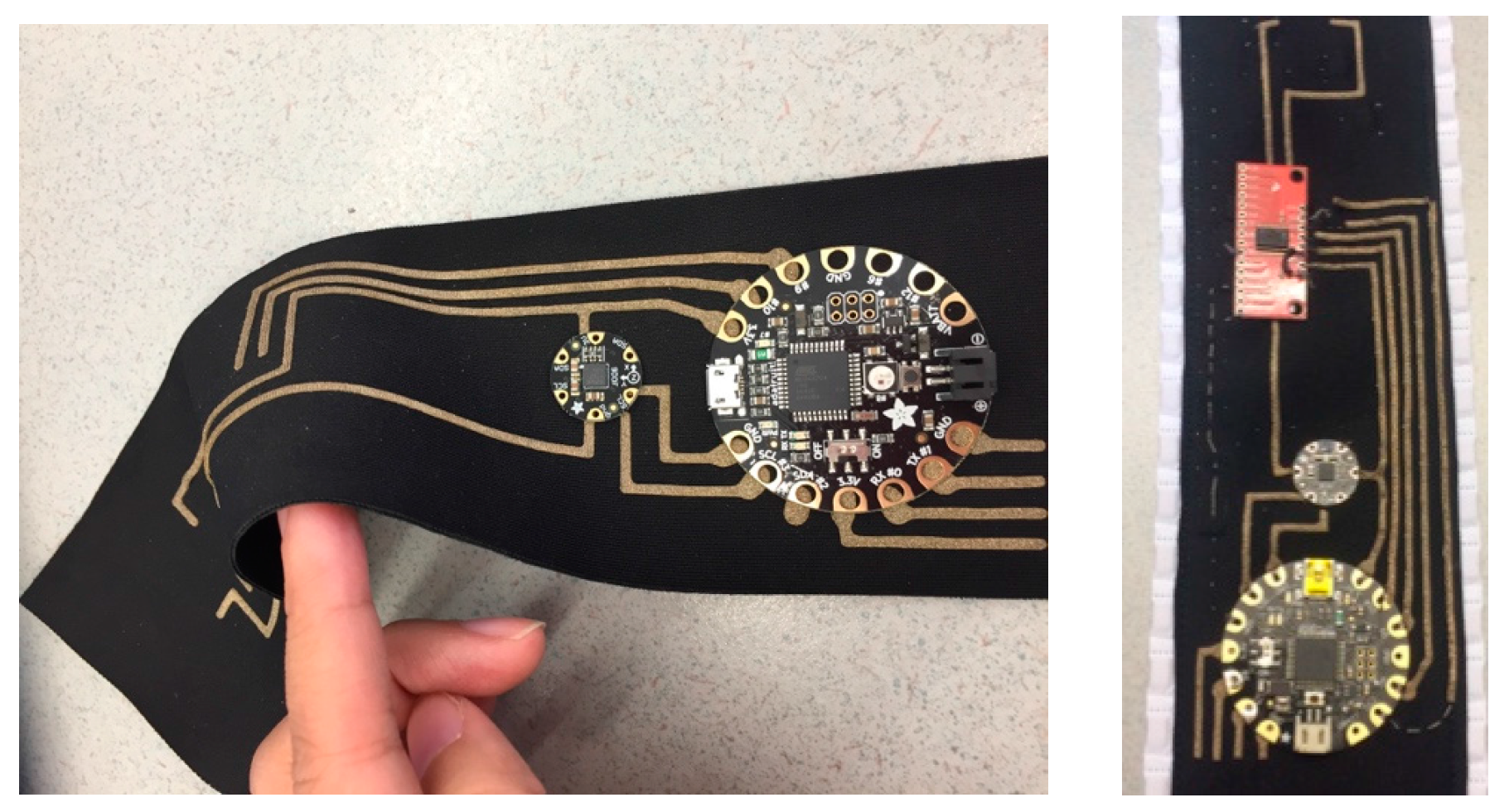
3.4. Garment Design and Conductive Textile Integration
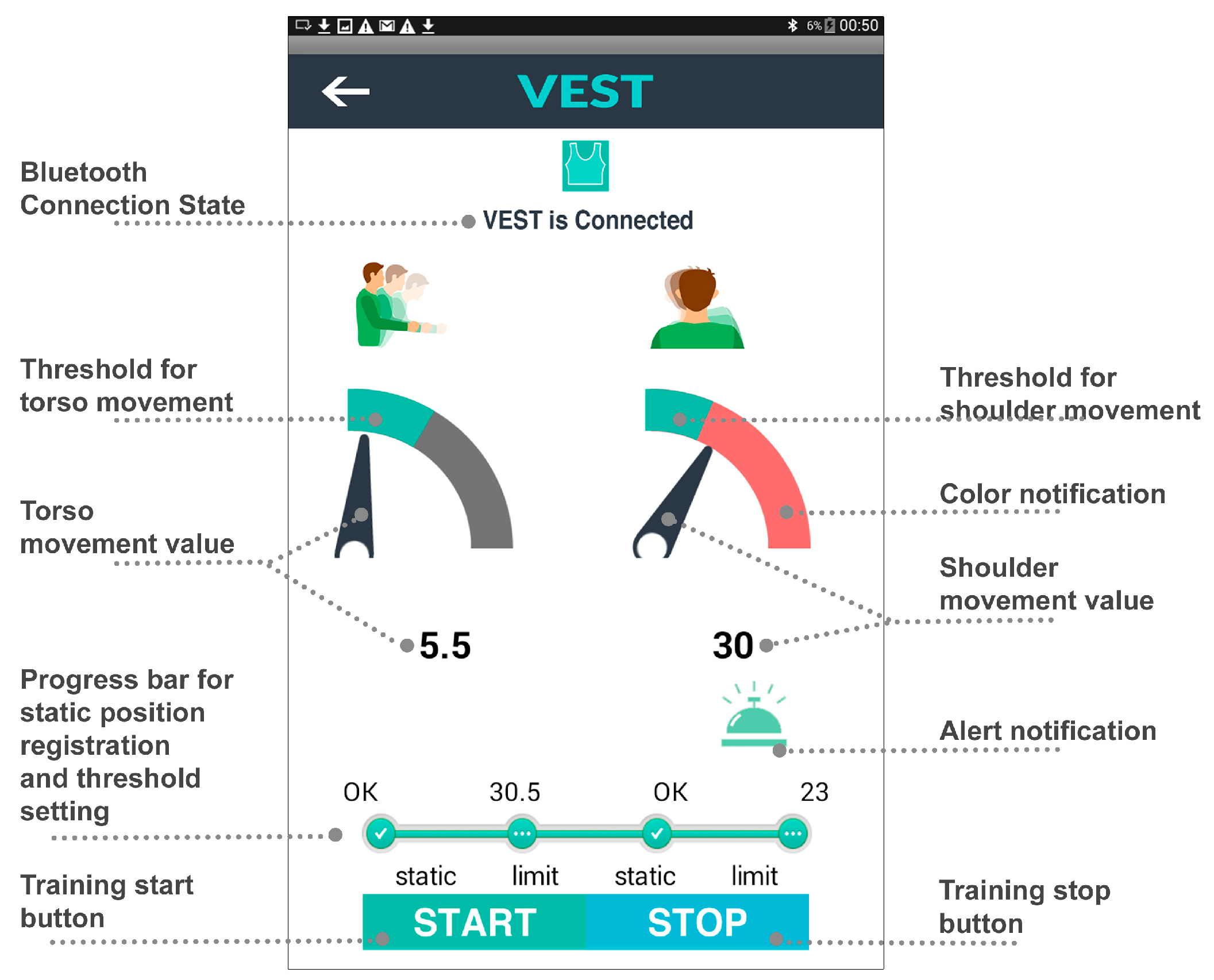
3.5. Feedback Strategy
4. Evaluating Patient Attitudes towards the System
4.1. Participants
4.2. Materials
4.3. Protocol
- (1)
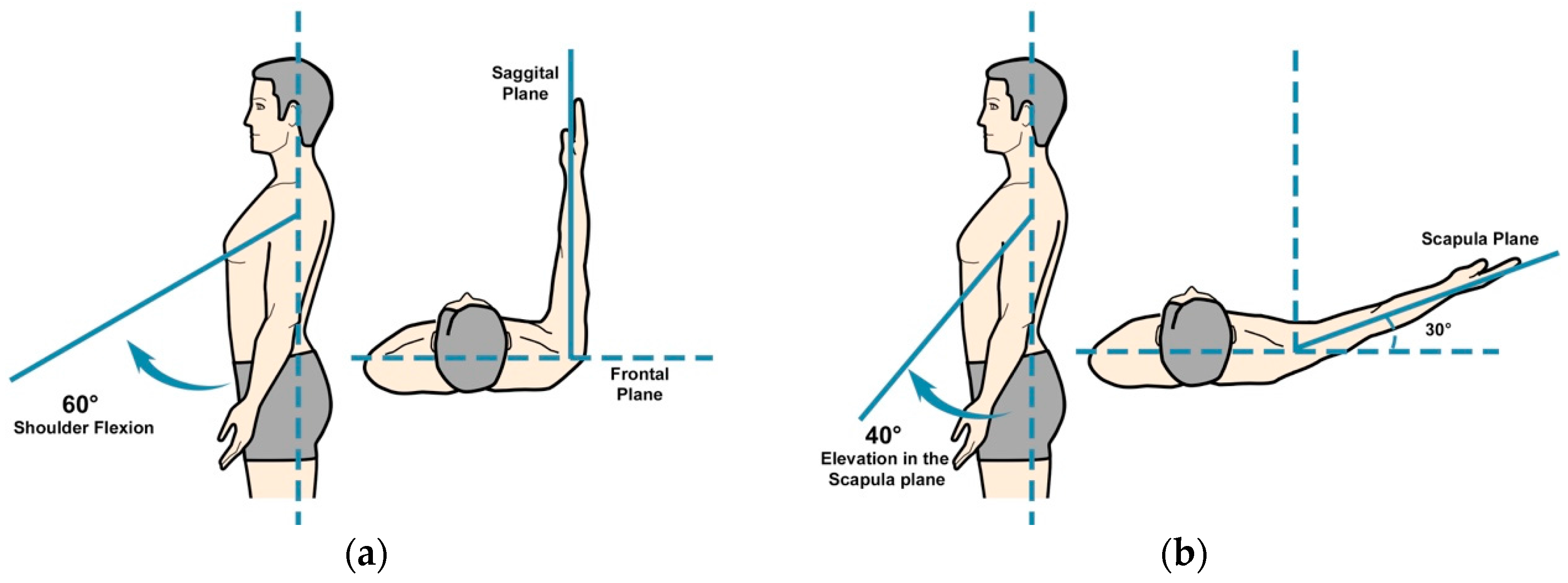
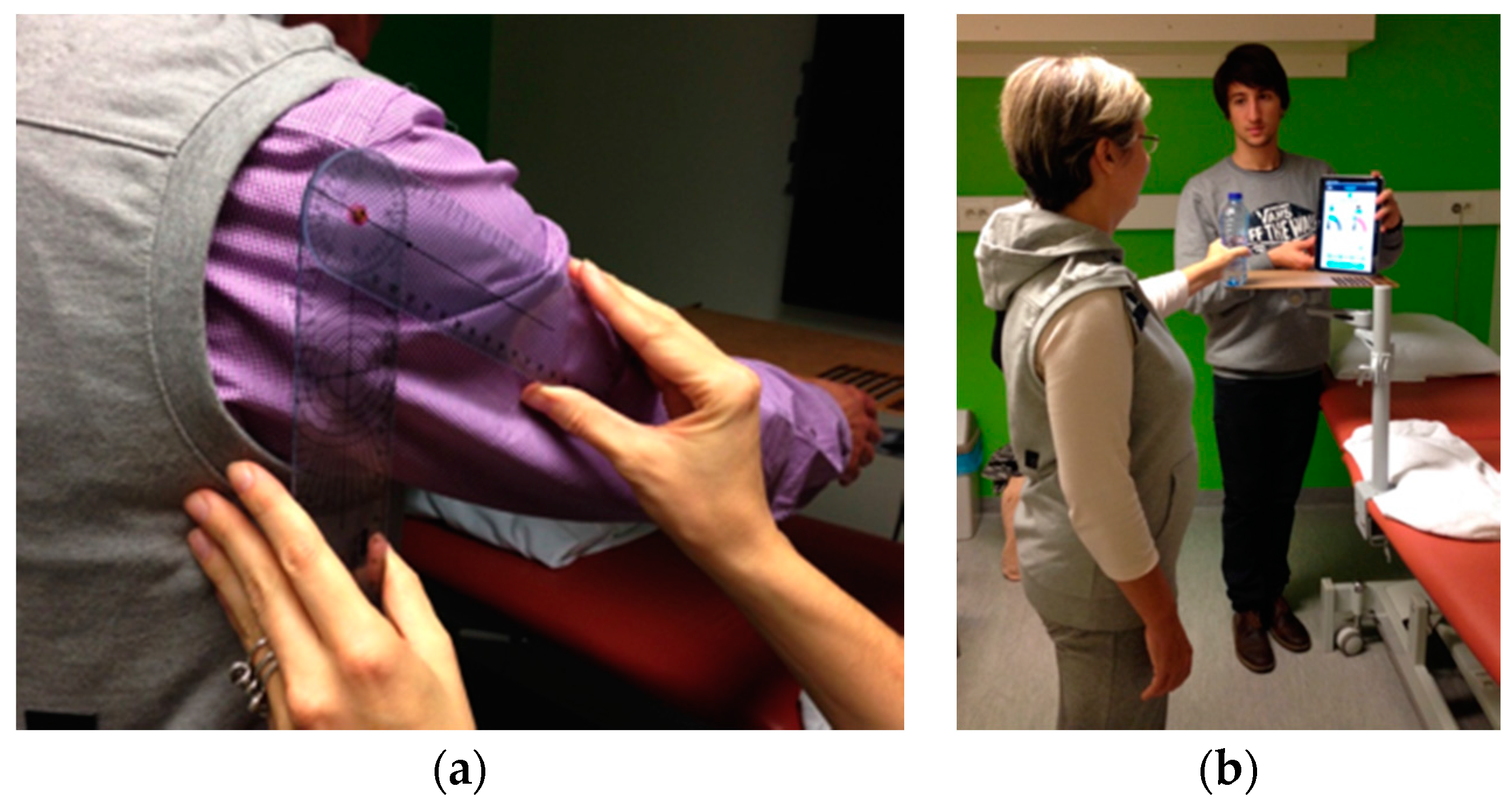
- Task 1: analytical shoulder flexion. The subject was asked to perform 60° of shoulder flexion with the thumb up and the elbow extended (see Figure 10a). A bar was placed in front of the patient at 60° to indicate the appropriate level of flexion. The range was determined with a goniometer, as shown in Figure 11a.
- (2)
- Task 2: functional shoulder flexion, placing a cooking pot. The subject was asked to place a cooking pot from a plate on a shelf that was located in front of him/her. The height of the shelf and the distance from the patient were standardized. The subject started with his arms alongside his body and with the elbows in 70° of flexion (determined with goniometry). The height of the shelf was adjusted accordingly. The patient had to perform 60° of shoulder flexion with extended arms, to place the pot on the shelf. Once subjects had placed the cooking pot on the shelf, they were asked to put it back on the shelf in front of them.
- (3)
- Task 3: analytical elevation in the scapular plane. The subject was asked to perform 40° of shoulder elevation in the scapular plane (30° in front of the frontal plane) with an extended elbow and with the thumb pointing upward (see Figure 10b). A bar was placed in the scapular plane, next to the patient at 40° of humerothoracic elevation to indicate the appropriate level of elevation. The range was determined with a goniometer.
- (4)
- Task 4: functional elevation in the scapular plane. The patient was asked to place a bottle of water (0.5 L) on a shelf that was located next to him in the scapular plane. The height of the shelf and the distance from the patient was standardized. At the starting position, the patient had his arms alongside his body and his elbows in 70° of flexion (measured with a goniometer). The bottle was in the hand of the tested arm side. The shelf was placed so that the patient had to perform 40° of scapular plane shoulder elevation with an extended arm to place the bottle on the shelf. Figure 11b shows a subject performing task 4.
4.4. Outcome Measures
4.4.1. Credibility and Expectancy
4.4.2. Intrinsic Motivation
4.4.3. Technology Acceptance and Usability
4.4.4. Credibility and Expectancy for Therapists
5. Results
5.1. Patients’ Evaluation
5.1.1. Measurement Results of Credibility and Expectancy
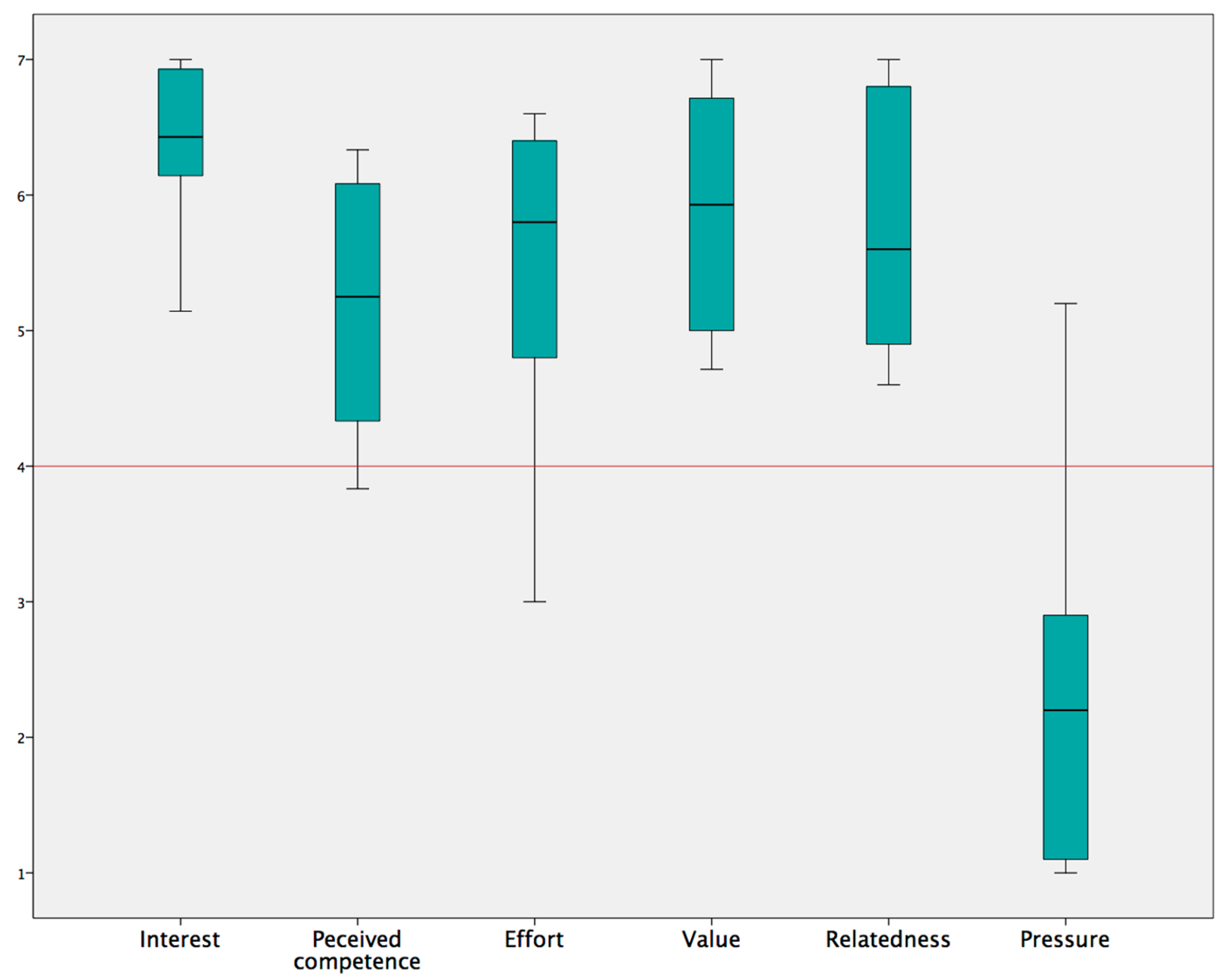
5.1.2. Measurement Results of Intrinsic Motivation
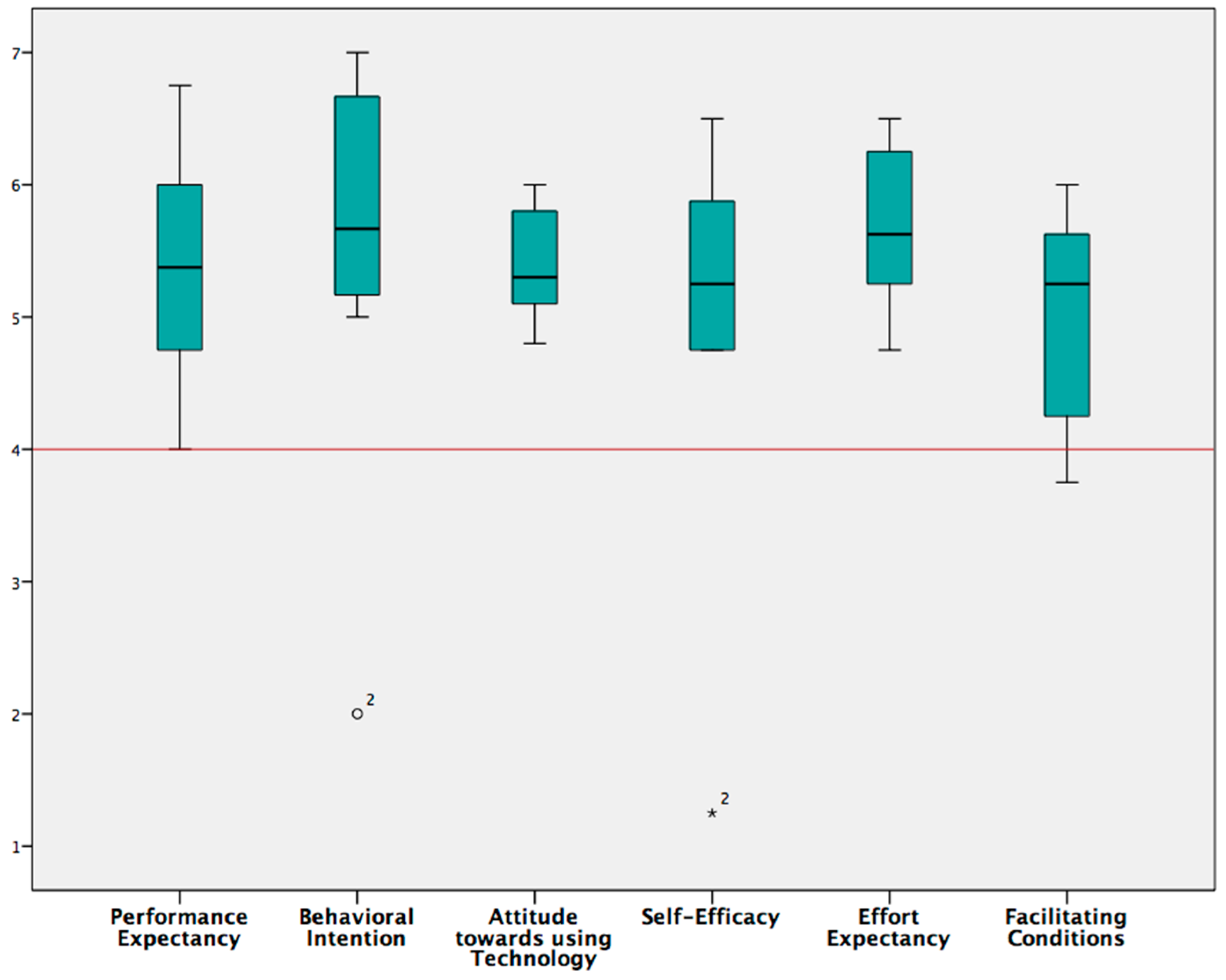
5.1.3. Technology Acceptance and Usability
5.2. Therapists’ Attitudes
6. Discussion and Future Work
7. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Ethical Statements
References
- Körver, R.J.P.; Senden, R.; Heyligers, I.C.; Grimm, B. Objective outcome evaluation using inertial sensors in subacromial impingement syndrome: A five-year follow-up study. Physiol. Meas. 2014, 35, 677–686. [Google Scholar] [CrossRef] [PubMed]
- Ketola, S.; Lehtinen, J.; Arnala, I.; Nissinen, M.; Westenius, H.; Sintonen, H.; Aronen, P.; Konttinen, Y.T.; Malmivaara, A.; Rousi, T. Does arthroscopic acromioplasty provide any additional value in the treatment of shoulder impingement syndrome? Bone Jt. J. 2009, 91, 1326–1334. [Google Scholar] [CrossRef] [PubMed]
- Luime, J.J.; Koes, B.W.; Hendriksen, I.; Burdorf, A.; Verhagen, A.P.; Miedema, H.S.; Verhaar, J. Prevalence and incidence of shoulder pain in the general population: A systematic review. Scand. J. Rheumatol. 2009, 33, 73–81. [Google Scholar] [CrossRef]
- Lindgren, I.; Jonsson, A.C.; Norrving, B.; Lindgren, A. Shoulder Pain after Stroke: A Prospective Population-Based Study. Stroke 2007, 38, 343–348. [Google Scholar] [CrossRef] [PubMed]
- De Baets, L.; Van Deun, S.; Monari, D.; Jaspers, E. Three-dimensional kinematics of the scapula and trunk, and associated scapular muscle timing in individuals with stroke. Hum. Mov. Sci. 2016, 48, 82–90. [Google Scholar] [CrossRef] [PubMed]
- De Baets, L.; Jaspers, E.; Van Deun, S. Scapulohumeral control after stroke: A preliminary study of the test-retest reliability and discriminative validity of a clinical scapular protocol (ClinScaP). NeuroRehabilitation 2016, 38, 359–370. [Google Scholar] [CrossRef] [PubMed]
- De Baets, L.; Jaspers, E.; Janssens, L.; Van Deun, S. Characteristics of Neuromuscular Control of the Scapula after Stroke: A First Exploration. Front. Hum. Neurosci. 2014, 8, 933. [Google Scholar] [CrossRef] [PubMed]
- Finley, M.A.; Lee, R.Y. Effect of sitting posture on 3-dimensional scapular kinematics measured by skin-mounted electromagnetic tracking sensors. Arch. Phys. Med. Rehabil. 2003, 84, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Levin, M.F.; Kleim, J.A.; Wolf, S.L. What Do Motor “Recovery” and “Compensation” Mean in Patients Following Stroke? Neurorehabil. Neural Repair 2008, 23, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Lorussi, F.; Carbonaro, N.; De Rossi, D.; Paradiso, R.; Veltink, P.; Tognetti, A. Wearable Textile Platform for Assessing Stroke Patient Treatment in Daily Life Conditions. Front. Bioeng. Biotechnol. 2016, 4, 28. [Google Scholar] [CrossRef] [PubMed]
- Worsley, P.; Warner, M.; Mottram, S.; Gadola, S.; Veeger, H.E.J.; Hermens, H.; Morrissey, D.; Little, P.; Cooper, C.; Carr, A. Motor control retraining exercises for shoulder impingement: Effects on function, muscle activation, and biomechanics in young adults. J. Shoulder Elb. Surg. 2013, 22, e11–e19. [Google Scholar] [CrossRef] [PubMed]
- Mottram, S.L. Dynamic stability of the scapula. Man. Ther. 1997, 2, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Timmermans, A.A.A.; Seelen, H.A.M.; Geers, R.P.J.; Saini, P.K.; Winter, S.; Te Vrugt, J.; Kingma, H. Sensor-Based Arm Skill Training in Chronic Stroke Patients: Results on Treatment Outcome, Patient Motivation, and System Usability. IEEE Trans. Neural Syst. Rehabil. Eng. 2010, 18, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Markopoulos, P.; Bin, Y.; Chen, W.; Timmermans, A. Interactive wearable systems for upper body rehabilitation: A systematic review. J. Neuroeng. Rehabil. 2017, 14, 20. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, S.K.; Massie, C.L.; Malcolm, M.P.; Levin, M.F. Does Provision of Extrinsic Feedback Result in Improved Motor Learning in the Upper Limb Poststroke? A Systematic Review of the Evidence. Neurorehabil. Neural Repair. 2010, 24, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Dunne, A.; Do-Lenh, S.; O’Laighin, G.; Shen, C.; Bonato, P. Upper Extremity Rehabilitation of Children with Cerebral Palsy Using Accelerometer Feedback on a Multitouch Display. In Proceedings of the 32th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC 2010), Buenos Aires, Argentina, 31 August–4 September 2010; pp. 1751–1754. [Google Scholar]
- Alankus, G.; Kelleher, C. Reducing Compensatory Motions in Motion-Based Video Games for Stroke Rehabilitation. Hum.–Comput. Interact. 2014, 30, 232–262. [Google Scholar] [CrossRef]
- Ploderer, B.; Fong, J.; Withana, A.; Klaic, M.; Nair, S.; Crocher, V.; Vetere, F.; Nanayakkara, S. ArmSleeve: A Patient Monitoring System to Support Occupational Therapists in Stroke Rehabilitation; ACM: New York, NY, USA, 2016; pp. 700–711. [Google Scholar]
- Beursgens, L.; Timmermans, A.; Markopoulos, P. Playful ARM hand training after stroke. In Proceedings of the CHI ‘12 Extended Abstracts on Human Factors in Computing Systems, Austin, TX, USA, 5–10 May 2012; pp. 2399–2404. [Google Scholar]
- Lin, W.-Y.; Chou, W.-C.; Tsai, T.-H.; Lin, C.-C.; Lee, M.-Y. Development of a Wearable Instrumented Vest for Posture Monitoring and System Usability Verification Based on the Technology Acceptance Model. Sensors 2016, 16, 2172. [Google Scholar] [CrossRef] [PubMed]
- Robert-Lachaine, X.; Mecheri, H.; Larue, C.; Plamondon, A. Validation of inertial measurement units with an optoelectronic system for whole-body motion analysis. Med Biol Eng Comput. 2016, 55, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Seymour, S. Fashionable Technology: The Intersection of Design, Fashion, Science, and Technology; Springer: Berlin, Germany, 2012. [Google Scholar]
- Wang, Q.; Markopoulos, P.; Chen, W. Smart rehabilitation garment design for arm-hand training. In Proceedings of the 8th International Conference on Pervasive Computing Technologies for Healthcare Oldenburg, Germany, 20–23 May 2014; pp. 328–330. [Google Scholar]
- Bhomer, M.; Tomico, O.; Hummels, C. Vigour: Smart textile services to support rehabilitation. In Proceedings of the Nordic Design Research Conference, Copenhagen, Denmark, 9–12 June 2013; pp. 505–506. [Google Scholar]
- Fleury, A.; Sugar, M.; Chau, T. E-textiles in Clinical Rehabilitation: A Scoping Review. Electronics 2015, 4, 173–203. [Google Scholar] [CrossRef]
- Cancela, J.; Pastorino, M.; Tzallas, A.; Tsipouras, M.; Rigas, G.; Arredondo, M.; Fotiadis, D. Wearability Assessment of a Wearable System for Parkinson’s Disease Remote Monitoring Based on a Body Area Network of Sensors. Sensors 2014, 14, 17235–17255. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Chen, W.; Markopoulos, P. Smart Garment Design for Rehabilitation. In ICTs for Improving Patients Rehabilitation Research Techniques; Communications in Computer and Information Science; Springer: Berlin/Heidelberg, Germany, 2014; Volume 515, pp. 260–269. [Google Scholar]
- Wang, Q.; Chen, W.; Timmermans, A.A.A.; Karachristos, C.; Martens, J.B.; Markopoulos, P. Smart Rehabilitation Garment for posture monitoring. In Proceedings of the 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC 2015), Milan, Italy, 25–29 August 2015; pp. 5736–5739. [Google Scholar]
- Wang, Q.; Toeters, M.; Chen, W.; Timmermans, A.; Markopoulos, P. Zishi: A Smart Garment for Posture Monitoring. In Proceedings of the CHI ‘12 Extended Abstracts on Human Factors in Computing Systems, Austin, TX, USA, 5–10 May 2012; pp. 3792–3795. [Google Scholar]
- Wu, G.; van der Helm, F.C.T.; DirkJan Veeger, H.E.J.; Makhsous, M.; Van Roy, P.; Anglin, C.; Nagels, J.; Karduna, A.R.; McQuade, K.; Wang, X.; et al. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion—Part II: Shoulder, elbow, wrist and hand. J. Biomech. 2005, 38, 981–992. [Google Scholar] [CrossRef] [PubMed]
- Van Vliet, P.M.; Wulf, G. Extrinsic feedback for motor learning after stroke: What is the evidence? Disabil. Rehabil. 2009, 28, 831–840. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Chen, W.; Markopoulos, P. Literature review on wearable systems in upper extremity rehabilitation. In Proceedings of the 36th International Conference on the IEEE BHI, Valencia, Spain, 1–4 June 2014; pp. 551–555. [Google Scholar]
- Roach, K.E.; Budiman Mak, E.; Songsiridej, N.; Lertratanakul, Y. Development of a Shoulder Pain and Disability Index. Arthritis Rheumatol. 1991, 4, 143–149. [Google Scholar] [CrossRef]
- Devilly, G.J.; Borkovec, T.D. Psychometric properties of the credibility/expectancy questionnaire. J. Behav. Ther. Exp. Psychiatry 2000, 31, 73–86. [Google Scholar] [CrossRef]
- McAuley, E.; Duncan, T.; Tammen, V.V. Psychometric Properties of the Intrinsic Motivation Inventory in a Competitive Sport Setting: A Confirmatory Factor Analysis. Res. Q. Exerc. Sport 1989, 60, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, V.; Mata, L.; Peixoto, F. Intrinsic Motivation Inventory: Psychometric Properties in the Context of First Language and Mathematics Learning. Psicol. Reflex. Crit. 2015, 28, 434–443. [Google Scholar] [CrossRef]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User acceptance of information technology: Toward a unified view. MIS Q. 2003, 27, 425–478. [Google Scholar]
- Lewis, J.R. IBM computer usability satisfaction questionnaires: Psychometric evaluation and instructions for use. Int. J. Hum.-Comput. Interact. 2009, 7, 57–78. [Google Scholar] [CrossRef]
- Timmermans, A.A.; Seelen, H.A.; Willmann, R.D.; Kingma, H. Technology-assisted training of arm-hand skills in stroke: Concepts on reacquisition of motor control and therapist guidelines for rehabilitation technology design. J. Neuroeng. Rehabil. 2009, 6, 1–18. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor | Neutral | Median(IQR) | Sig | |
|---|---|---|---|---|
| Credibility/Expectancy (CEQ) | Credibility | 13.5 | 22.5 (3.5) | 0.011 |
| Expectancy | 13.5 | 20.2 (3.55) | 0.012 | |
| Intrinsic Motivation (IMI) | Interest/Enjoyment | 4 | 6.43 (0.82) | 0.012 |
| Perceived competence | 4 | 5.25 (1.96) | 0.028 | |
| Effort/Importance | 4 | 5.8 (1.9) | 0.025 | |
| Value /Usefulness | 4 | 5.93 (1.93) | 0.012 | |
| Relatedness | 4 | 5.6 (2.05) | 0.012 | |
| Pressure/Tension | 4 | 2.2 (2) | 0.025 | |
| Technology Acceptance (UTAUT) | Performance expectancy | 4 | 5.37 (1.75) | 0.018 |
| Behavioral Intention | 4 | 5.67 (1.58) | 0.058 | |
| Attitude towards technology | 4 | 5.3 (0.85) | 0.012 | |
| Self-Efficacy | 4 | 5.25 (1.19) | 0.16 | |
| Effort expectancy | 4 | 5.62 (1) | 0.011 | |
| Facilitating conditions | 4 | 5.25 (1.44) | 0.024 | |
| Usability (CSUQ) | System usefulness | 4 | 5.63 (1.53) | 0.012 |
| Interface quality | 4 | 5.67 (1.33) | 0.011 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Q.; De Baets, L.; Timmermans, A.; Chen, W.; Giacolini, L.; Matheve, T.; Markopoulos, P. Motor Control Training for the Shoulder with Smart Garments. Sensors 2017, 17, 1687. https://doi.org/10.3390/s17071687
Wang Q, De Baets L, Timmermans A, Chen W, Giacolini L, Matheve T, Markopoulos P. Motor Control Training for the Shoulder with Smart Garments. Sensors. 2017; 17(7):1687. https://doi.org/10.3390/s17071687
Chicago/Turabian StyleWang, Qi, Liesbet De Baets, Annick Timmermans, Wei Chen, Luca Giacolini, Thomas Matheve, and Panos Markopoulos. 2017. "Motor Control Training for the Shoulder with Smart Garments" Sensors 17, no. 7: 1687. https://doi.org/10.3390/s17071687
APA StyleWang, Q., De Baets, L., Timmermans, A., Chen, W., Giacolini, L., Matheve, T., & Markopoulos, P. (2017). Motor Control Training for the Shoulder with Smart Garments. Sensors, 17(7), 1687. https://doi.org/10.3390/s17071687