1. Introduction
Worldwide, about one million heart surgeries are performed annually, which require extracorporeal circulation (ECC) using the heart-lung machine [
1]. The ECC includes various methods, such as dialysis, extracorporeal membrane oxygenation (ECMO) for respiratory support, extracorporeal life support (ECLS), and ventricular assist devices (VAD) for cardiac support [
2,
3,
4]. During ECC, the contact of blood with foreign surfaces can lead to life-threatening activation of coagulation. Therefore, anticoagulants, such as heparin, are used to prevent coagulation activation. Heparin binds to the enzyme inhibitor antithrombin III (AT) and leads to its activation due to conformational change. The activated AT interacts with the exosite II of thrombin and results in the inactivation of thrombin [
5]. However, some patients develop hypersensitivity reactions against heparin, such as ‘heparin-induced thrombocytopenia’ (HIT), which leads to a decrease in the platelet counts (thrombocytopenia) [
6]. Thus, research is performed to develop new drugs as anticoagulants. The DNA aptamer NU172 is selected against thrombin and specifically binds to the anionic binding site exosite I of thrombin, which has two exosites, exosite I and II. As a result, fibrinogen cannot be transformed into fibrin and the coagulation process is inhibited [
5,
7]. Thus, coagulation inhibiting aptamers, such as thrombin binding aptamer NU172, represent a promising alternative to the use of heparin in HIT patients during ECC.
Aptamers can fold into 3D structures and bind their targets with a high affinity and specificity [
8]. They can be used as theranostics and the modifications at defined positions enable the fine-tuning of their stability and bioavailability [
9]. A further great advantage of aptamers is their antagonizability by the use of complementary oligonucleotides, so-called antidotes (ADs). The drug-induced side effects can be significantly reduced by the use of antagonizable drugs and the blocking of their therapeutic effect after treatment. The three-dimensional (3D) structure of the aptamer can be changed by the addition of an AD, which hybridizes to the aptamer and abrogates the binding of the aptamer to its target [
10,
11,
12]. Thereby, the effect of aptamer-based drugs can be abolished.
ECC can last several hours, thus the continuous monitoring of the coagulation status during and after the ECC is important to prevent bleeding or thrombosis-related complications [
13]. Thrombin converts fibrinogen into insoluble fibrin [
14], which is then cross-linked with activated platelets, resulting in the generation of a platelet-fibrin network. This leads to an increase in viscous and elastic components of the blood viscosity [
15]. Thus, the viscoelastic properties of blood can be detected to monitor the coagulation status in real-time [
16].
Pechold and co-workers developed a piezo-based device, called piezoelectric axial vibrator (PAV) [
17,
18]. Using this device, the linear viscoelasticity of soft material fluids, such as blood, and low viscous polymeric solutions can be characterized at higher frequencies (1 to 1000 Hz) compared to currently used rheometers. PAV is able to measure blood coagulation in a physical reliable range with low measuring gaps such as 10 µm, where only a monolayer of blood cells can be formed.
Currently, modern intensive care does not provide a comprehensive point-of-care (POC) solution for the detection of coagulation status and blood clotting problems. So far, a single medical device, which allows fast and reliable detection of the hemostasis status (coagulation, fibrinolysis, and platelet function) is lacking. The promising results of our recent studies with PAV [
19] and oscillatory rheometer [
20] indicate that the above mentioned clinical challenges of hemostasis monitoring could be solved by rheology.
Since the oscillation rheometer is too large and too expensive for the clinical routine and additionally susceptible to mechanical shock, in this study, an optimized piezo-based system (PIEZ) was developed based on PAV. By doubling the diameter of the measuring chamber and reducing the stiffness of the whole system, the optimized PIEZ is able to measure multiple layers of blood cells with a 50 µm gap. Furthermore, this gap height provides more space for the formation of a 3D clot. In contrast to Kirschenmann’s work [
17,
21], in this study, piezo tubes were used instead of glued piezos on a copper square tube and a heater was integrated. Using the new system, the viscoelastic properties of blood can be determined rheometrically and used to monitor hemostasis.
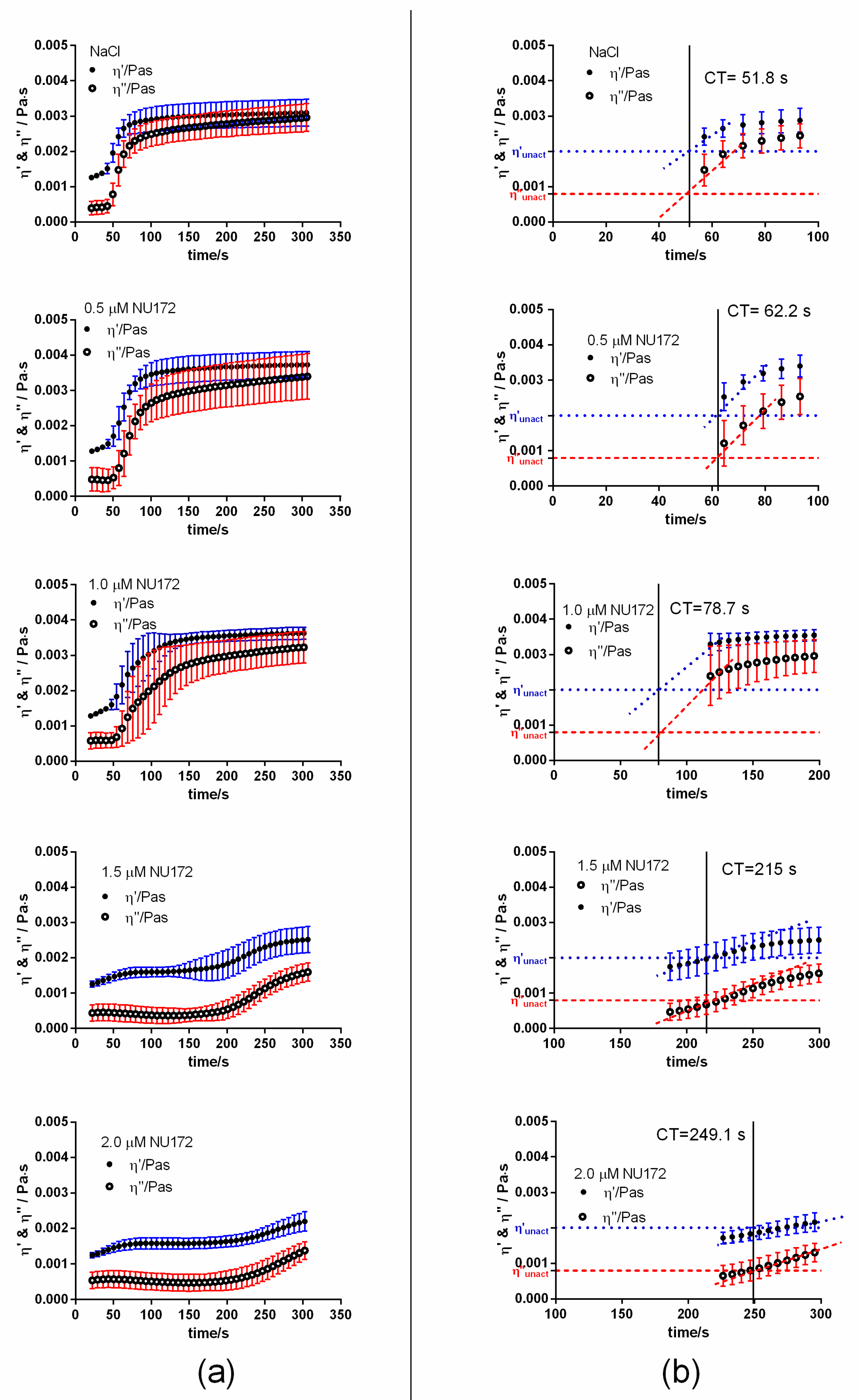
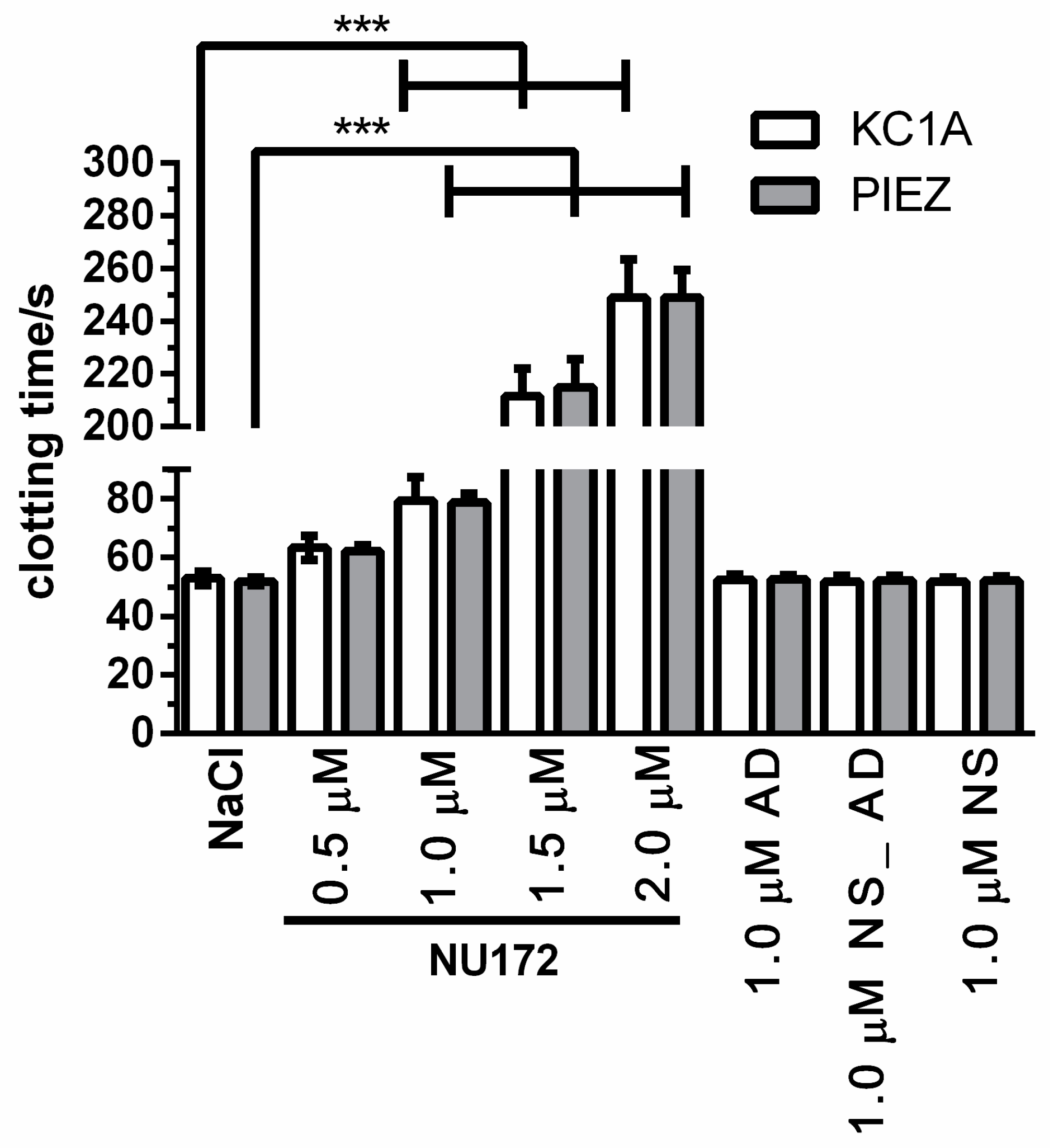
In this study, we examined the reliability and applicability of the PIEZ system for the evaluation of nucleic acid-based drugs influencing the coagulation, such as the thrombin aptamer (NU172). Therefore, the coagulation of blood samples was tested under static and dynamic conditions after the addition of NU172 by using PIEZ and a medical reference device (ball coagulometer (KC1A)) in comparison. Furthermore, the inhibition of thrombin aptamer by its AD was analyzed. In addition to the clotting time (CT), further rheological parameters such as the linear slopes (m) of the viscous and elastic components and the viscosity at a certain predefined time point were determined in order to obtain additional information about the coagulation process and clot firmness. During the coagulation, shear viscosity increases over time, and the linear slopes (m) of viscous and elastic components describe the increase of clot formation. The clot firmness, which is dependent on blood fibrinogen level, fibrin cross-linking, and platelet numbers can be obtained by a detected viscosity value at a certain time point. Finally, an in vitro rotation model was used to validate rheologically determined coagulation status. Blood counts were measured, and the thrombin markers (thrombin-antithrombin III (TAT) complex and fibrinopeptide A (FPA)) and the platelet activation marker (β-thromboglobulin (β-TG)) were quantified by enzyme-linked immunosorbent assays (ELISAs) after the incubation of blood with diverse aptamer-combinations.
2. Materials and Methods
2.1. Ethics Statement
The Ethics Committee of the University of Tuebingen approved the blood sampling procedures, and all subjects gave written informed consent (project approval number: 270/2010BO1).
2.2. Oligonucleotides
The incubation of blood was performed with the thrombin binding aptamer (NU172) and its complementary single-stranded (ss) DNA (AD) (
Table 1). Furthermore, a nonsense aptamer (NS) and a nonsense antidote (NS_AD) were used as negative controls [
7]. All oligonucleotides were ordered HPLC-purified from Ella Biotech GmbH (Martinsried, Germany).
2.3. Blood Collection
Human whole blood was drawn by venipuncture into 3 mL blood collection tubes containing 1 U/mL sodium-heparin (Ratiopharm Merckle GmbH, Germany) or 0.106 mol/L trisodium citrate (S Monovette 3 mL 9NC, Sarstedt AG, Nümbrecht, Germany), which prevents the coagulation by reversible binding to calcium ions.
For all donors (age: 25 to 45 years, male or female), the following exclusion criteria were imperative: Smoking, pregnancy, and taking drugs (particularly drugs affecting the hemostasis, such as aspirin, oral contraceptives, and nonsteroidal anti-inflammatory drugs). The experiments with the in vitro rotation model were performed with heparinized blood of five different volunteers. The other experiments were repeated using the blood of the same volunteer.
2.4. Incubation of Blood with Oligonucleotides
To monitor the effect of NU172 on coagulation, citrated or heparinized blood was incubated for 2 min with 0.5, 1.0, 1.5, or 2.0 μM NU172. Then, 1.0 μM AD was added to the blood samples containing NU172. The rheological characteristics of blood and the CT were investigated using the PIEZ system. Furthermore, to validate the results, the CT was additionally measured using a ball coagulometer as a reference device. As controls, blood samples were also analyzed after the addition of 100 µL 0.9% NaCl without oligonucleotides and after the addition of 100 µL 0.9% NaCl containing 1.0 μM NS_AD, NS, or AD.
2.5. Initiation of Coagulation Activation
2.5.1. In Citrated Blood
The coagulation activators pathromtin SL and CaCl2 from the activated partial thromboplastin time (aPTT) assay (Siemens Healthcare Diagnostics Products GmbH, Marburg, Germany) were used to activate the coagulation in citrated blood. Therefore, 100 μL pathromtin SL was added to 100 μL citrated blood with and without oligonucleotides and incubated for 2 min at 37 °C. Afterwards, 100 μL CaCl2 (c = 0.025 mol/L) was added to initiate the coagulation. The samples (300 μl) were then simultaneously applied onto the measuring surface of PIEZ or into the cuvette of the ball coagulometer to measure the blood coagulation.
2.5.2. In Heparinized Blood
To initiate the coagulation in heparinized blood, 100 μL heparinized blood with and without oligonucleotides was incubated with the coagulation activators of the Heptest (Heptest Laboratories, Inc, St. Louis, USA). Therefore, 100 μL plasma cephalin was added and incubated for 2 min, and then 100 μL factor Xa containing CaCl2 was added. A total volume of 300 µL was transferred into the cuvette of the ball coagulometer or onto the measuring surface of the PIEZ.
2.6. Detection of Coagulation
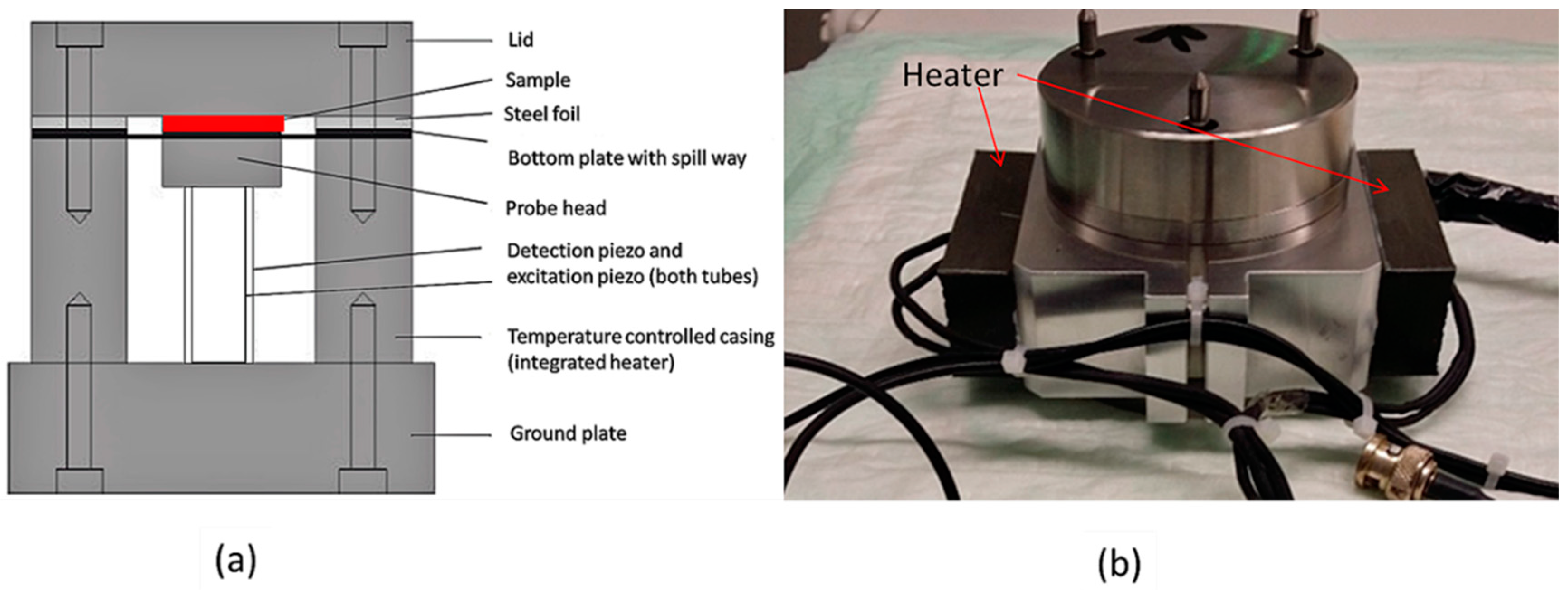
2.6.1. Optimized Piezo-Based Measuring Method (PIEZ)
To detect the viscoelastic properties of the blood and the CT, the optimized PIEZ system was designed and applied (
Figure 1). The lid of the system is fixed to the bottom plate to hermetically close the piezo system. The PIEZ system is connected to a computer and a lock-in amplifier sends the frequency, voltage, and a sinusoidal excitation to the excitation piezo. The bottom plate is moved by the excitation piezo, and a periodical squeeze flow of the sample is created within the measuring chamber. The deformation of the blood sample is measured by the detection of the complex voltage (U*) at the detection piezo and the phase shift between the excitation and detection piezo. Before starting the measurement, a reference reading was performed with an empty device to obtain U
0*. The system can only differentiate between unloaded and loaded sample measurement if the ratio |U*/U
0*| is smaller than 1.
The complex shear modulus (G*) is determined by calculating the |U*/U
0*|ratio. G* consists of a real part, the elastic/storage modulus (G′), and an imaginary part, the viscous/loss modulus (G″). The complex shear viscosity (η*) can be calculated from the shear modulus and consists of a viscous (η′, real part) and an elastic (η″, imaginary part) component. Kirschenmann described the equation of motion of the piezo system in a point-mechanical approximation using a mass-spring system [
17]. This approximation allows the correlation between the |U*/U
0*| and the complex squeeze stiffness (K*). A continuum mechanical calculation is used to obtain a correlation between the K* and η*. Using these calculations, the correlation between the |U*/U
0*| and η* can be obtained [
19,
20,
21].
In the case of linear viscoelasticity,
K* can be calculated according to Equation (1).
In Equation (1),
R denotes the radius of the plate and
d is the gap width of the measuring chamber,
K* is the complex squeeze stiffness,
is the inertia term, and
G* is the complex shear modulus. In this equation, the dependence of
G* on geometry (
R and
d) is visible [
17].
The doubling of the radius leads to an approximately 16-fold change in
K*. Thus, the increase of the radius allowed the measurement of the blood samples with a measuring gap of 50 µm. The CT, m, and viscous and elastic components of the complex viscosity of the blood samples were determined at 300 s. The measurements were performed with 300 µL blood sample at 37 °C and at a frequency of 100 Hz. Citrated blood samples were activated by adding the coagulation activators pathromtin and CaCl
2. Heparinized blood was activated by adding plasma cephalin and factor X
a. The PIEZ system was calibrated prior to measurements using calibration fluids as previously described [
19].
2.6.2. Ball Coagulometer
As a reference device, the coagulation was simultaneously determined in 300 µL blood samples using a ball coagulometer (KC 1A, ABW Medizin und Technik GmbH, Germany). Prior to the measurement, the blood sample was filled in a cuvette containing a stainless steel ball and incubated for 2 min at 37 °C. In this coagulometer, a stainless steel ball is kept within a magnetic field. To initiate the coagulation process, citrated blood samples were activated by adding the coagulation activators pathromtin and CaCl
2. Heparinized blood samples were activated by adding plasma cephalin and factor X
a. The generation of fibrin threads leads to the displacement of the ball from the magnetic field. The change of position is then detected by a magnetic sensor and thereby, the CT in seconds is determined [
22,
23].
2.7. Simulation of ECC Using an in Vitro Rotation Model
To simulate ECC conditions, the aptamer incubation was performed with fresh human whole blood anticoagulated with 1 IU/mL heparin in a dynamic in vitro rotation model. Therefore, polypropylene round-bottom tubes (14 mL, BD Biosciences, New Jersey, USA) were filled with 13 mL blood without oligonucleotides (baseline) or with 1300 µL 0.9% NaCl as control, 1.0 μM NU172, AD, or NS. Additionally, 1.0 μM NU172 was added into heparinized blood and incubated for 2 min. Afterwards, 1.0 μM AD was added to the aptamer containing blood and incubated for 5 min to abrogate the inhibitory effect of the aptamer. The prepared tubes were transferred to a tube rotator (neoLab, Heidelberg, Germany) and incubated at 37 °C for 30 min and 10 rpm. Immediately after the addition of oligonucleotides (0 min) and after 30 min of dynamic incubation, blood samples were collected in tubes containing ethylenediaminetetraacetic acid (1.6 mg mL−1, EDTA, Sarstedt, Nümbrecht, Germany) for the detection of cell numbers and FPA. To detect thrombin-antithrombin III (TAT) complex, tubes containing 0.3 mL of citrate solution/3 mL blood and 0.106 M C6H5Na3O7 × 2H2O (Sartstedt, Nümbrecht, Germany) were used. For β-TG analysis, blood was transferred to 2.7 mL CTAD tubes with 270 μL of 0.109 M CTAD solution containing buffered sodium citrate, theophylline, adenosine, and dipyridamole (BD Vacutainer CTAD, Becton-Dickinson GmbH, Heidelberg, Germany) and stored for 15 min on ice. The EDTA and CTAD preparations were centrifuged at 2500 × g for 20 min at 4 °C, and the citrated blood preparations were centrifuged at 1800 × g for 18 min at RT. The blood plasma of each sample was shock frozen in liquid nitrogen and stored at −80 °C until further investigations. To determine the CT, the coagulation of the blood samples was initiated with plasma cephalin and factor Xa, and the blood samples were manually loaded into the PIEZ and the ball coagulometer.
2.8. Blood Cell Count Analysis
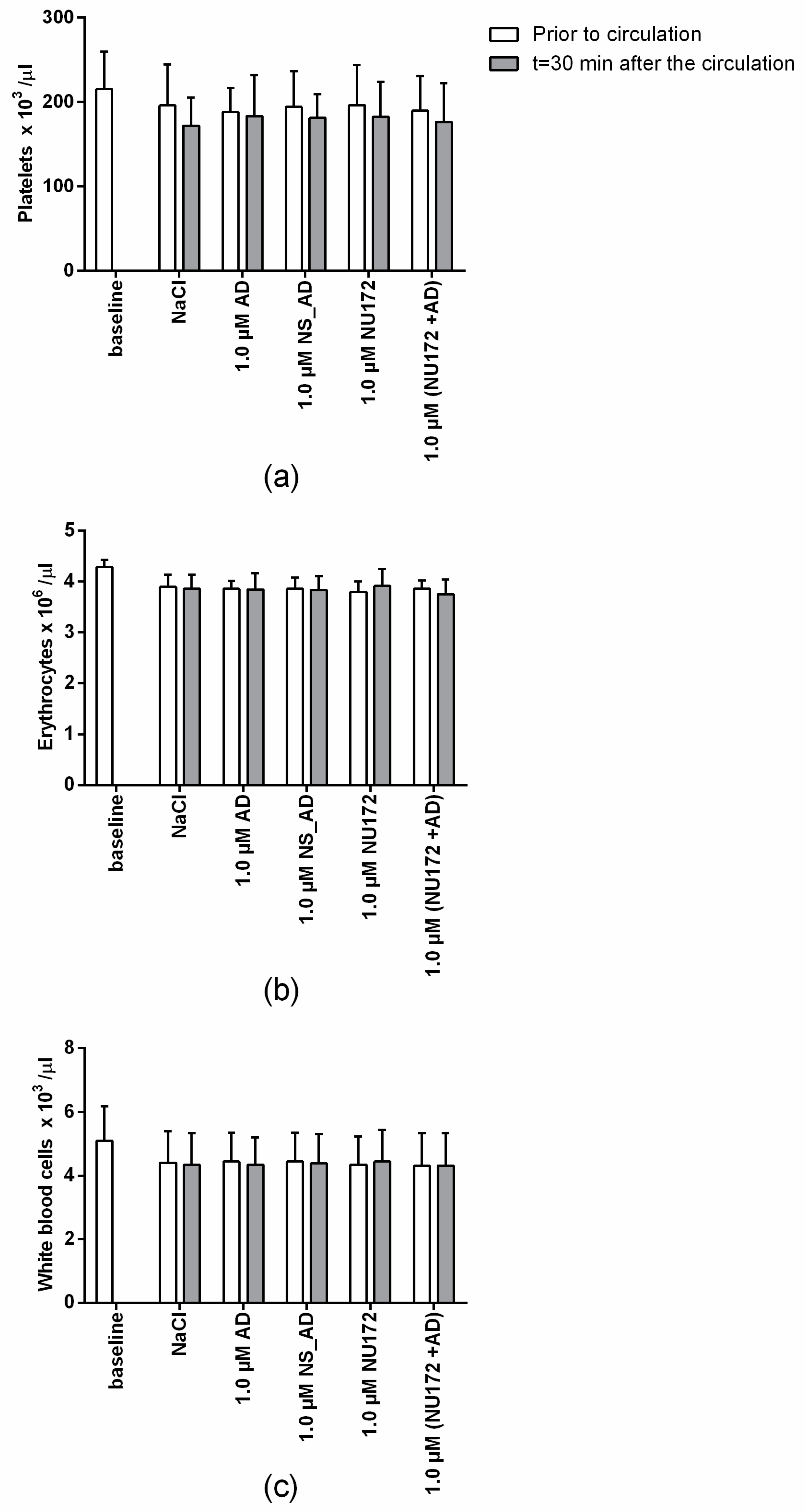
The number of erythrocytes, leukocytes, and platelets in blood samples was measured using an automated cell count system (ABX Micros 60, HORIBA ABX SAS, Montpellier, France) before and after the incubation in rotation model.
2.9. Detection of FPA, TAT, and β-TG
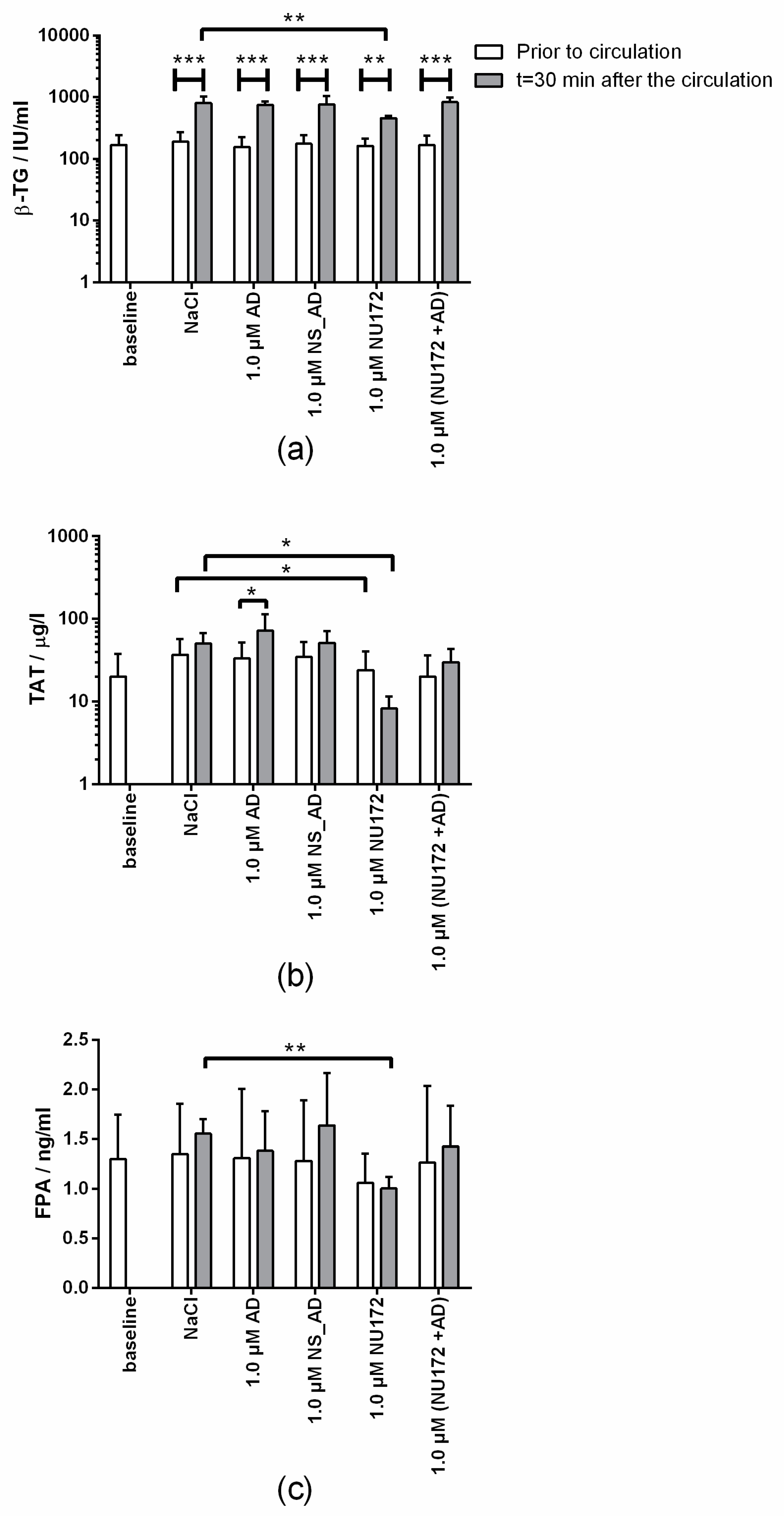
During coagulation, the conversion of prothrombin to thrombin is a key event in the formation of a fibrin clot. The most important coagulation inhibitor is AT neutralizing thrombin by forming a TAT complex. As a result, thrombin irreversibly loses its enzymatic activity. Thus, the TAT concentration in plasma is an indirect marker for the detection of coagulation activation. Another indirect thrombin marker is FPA, which is released whenever thrombin converts fibrinogen into fibrin. Both plasma concentrations serve as indirect markers for the detection of coagulation activation. The platelet marker β-TG is released from α-granules and provides information about the platelet activation [
22,
23,
24].
The level of TAT complexes was determined according to the manufacturer’s instructions using Enzygnost TAT micro enzyme-linked immunosorbent assay (ELISA, Siemens Healthcare Diagnostics Products, Marburg Germany). Furthermore, the amount of β-TG (Asserachrom β-TG, Diagnostica Stago, Asnières sur Seine Cedex, France) and FPA (MyBioSource, Inc. San Diego, USA) were determined in the plasma samples.
2.10. Statistical Analyses
Data are presented as means ± standard deviation (SD). Normally distributed data were analyzed using two-way ANOVA with Bonferroni’s multiple comparison test to determine differences between more than two groups. T-test was performed to compare two groups. Statistical significant differences were defined as p < 0.05. The calculations of the mean, SD, and m by regression analysis were performed using Microsoft Excel 2013. Statistical analyses were performed using GraphPad Prism Version 6 (GraphPad Software, La Jolla, San Diego, CA, USA). Diagrams of rheological measurements over time were drawn using Origin Pro 8 (Origin Lab Corporation, Northhampton, USA).
4. Discussion
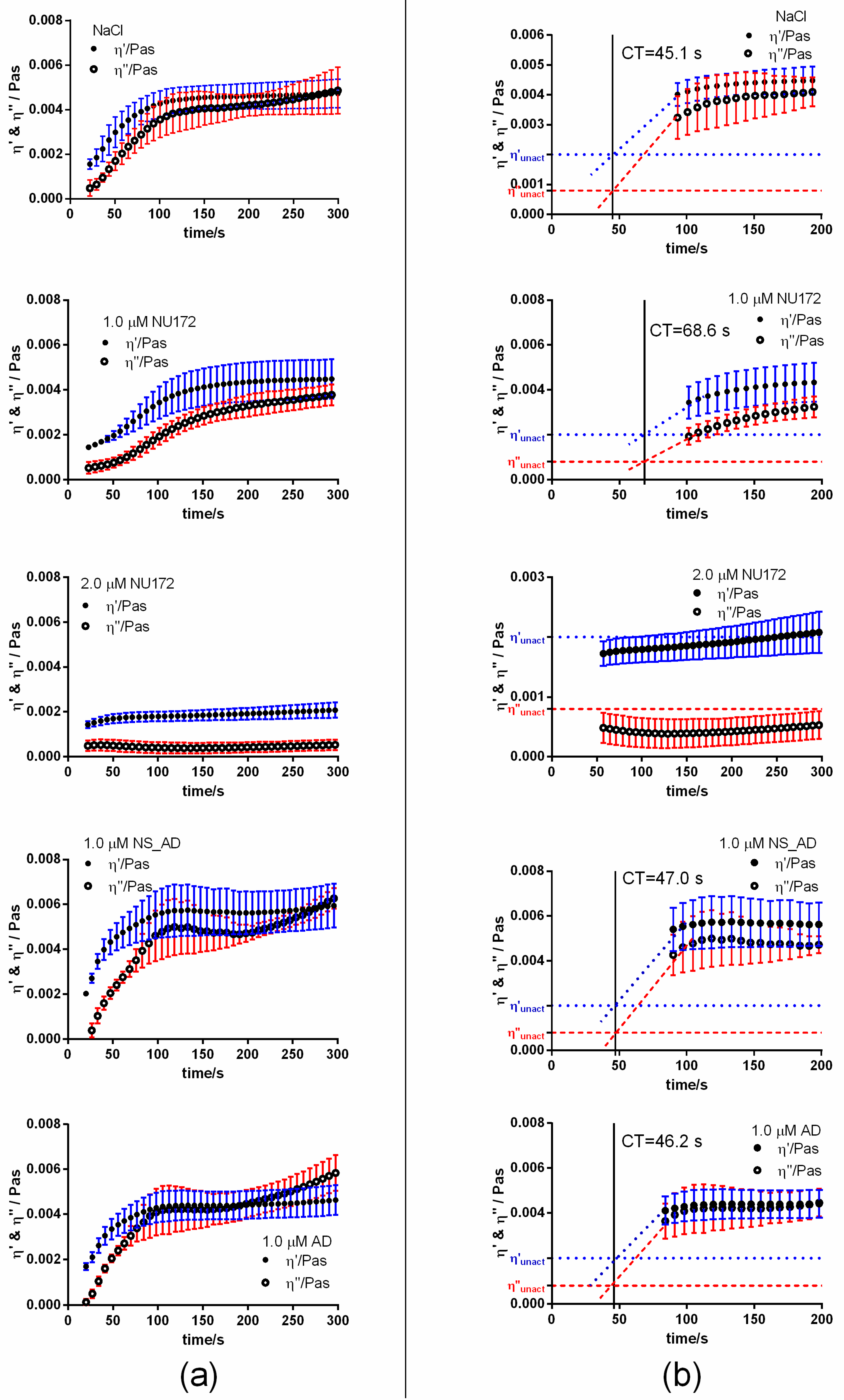
In this study, a new optimized PIEZ was developed to evaluate the blood coagulation status by detecting the rheological characteristics of the sample. The sensitivity for blood rheology measurements was optimized by doubling the diameter of the measuring chamber and reducing the mechanical stiffness of the former PAV system. Using the new PIEZ, the influence of thrombin binding aptamer NU172 on coagulation inhibition could be determined in citrated as well as heparinized blood samples. The CTs obtained by PIEZ measurements were comparable to those measured with the medical reference system, the ball coagulometer KC 1A. As an additional feature, PIEZ allowed the detection of slope m of viscous (η′) and elastic (η″) components, which describe the kinetics of the coagulation process as a change of shear viscosity over time. The detection of shear viscosity (η′ and η″ components) at a given time provides information about the proportion of each component in the sample. In addition, the detection of shear viscosity 300 s after the initiation of coagulation gives an indication of the rigidity of the resulting blood clot.
At present, simple (e.g., ball coagulometer (KC 1A)) or sophisticated devices (e.g. rotational thromboelastometry (ROTEM)) are clinically used to analyze blood coagulation. Currently, new devices are being developed, such as cavitation rheology, which investigates the rheological properties of erythrocytes [
25,
26]. Thereby, a pulsed laser with a wavelength of 532 nm is focused on the sample for 6 ns. Due to the high intensities at the focal volume, an expanding bubble, called cavity, is formed. The bubbles reach a diameter of 90–120 µm before collapsing. The elastic properties of erythrocytes can be characterized by analyzing the shape recovery of the cells. Thus, this method can be applied to study the properties of blood cells, but it is not suitable for the monitoring of hemostasis. In contrast, the viscoelastic hemostatic assay, free oscillation rheology (FOR) might be a better suited rheological method for the detection of blood coagulation [
27,
28]. To obtain the CT, citrated blood or plasma is added at 37 °C to a free oscillating cuvette. A magnetic field initiates the oscillation every 2 s with a frequency of 11 Hz. An optical detector registers the damping and frequency of the container. During the coagulation process, the damping increases and the frequency decreases. Therefore, the endpoint of coagulation can be detected by a change in elasticity. This system is similar to thromboelastography (TEG) and ROTEM, but FOR is not a widely used method in investigations of coagulopathy during ECC [
29].
ROTEM is a medical device that is used in clinical practice [
30,
31,
32]. It uses a fixed cuvette (cup) with a cylindrical pin that is immersed into the cup filled with whole blood (gap of 1 mm between pin and cuvette wall). The movement of the rotating pin is restricted once the blood starts clotting. A spring affixed to the pin detects the restriction. The kinetic change is optically detected by an integrated computer (TEMogram). Using multiple cuvettes simultaneously with different reagents, the interactions of coagulation factors, inhibitors, and cellular components can be measured during the coagulation phase as well as subsequent fibrinolysis over time [
31,
33,
34,
35]. Currently, ROTEM remains the gold standard for sophisticated hemostasis monitoring [
29]. The first generation device, ROTEM delta is semi-automated with an automatic pipette system and manual connection of the pin-and-cup system. It requires limited manual training, special expertise in coagulation and extensive interpretation training. Especially, the first generation TEG, TEG 5000, is associated with extensive manual handling and shock-sensitivity. Thus, this device cannot be used at the patient´s bedside as it requires a low-vibration workstation. To solve these challenges, ROTEM sigma and TEG 6S were designed. These devices are cartridge-based, fully automated with preset reagents, no manual pipetting steps are required, and have decreased sensitivity to external vibrations. However, special extensive expertise is required for the interpretation of the results and the devices are expensive.
The new PIEZ in this study can monitor within five minutes the change of viscous and elastic components over time and provides reliable information about the blood coagulation. Furthermore, the piezo-based system is able to measure the coagulation status in real-time. Additionally, the PIEZ system is not susceptible to shock, which prevents disturbance of measurements and increases the reproducibility of results. Currently, the PIEZ system is a research instrument, and since it needs manual cleaning after each measurement, it is not applicable during ECC. However, after further improvement and optimization, the system might be also used at the patient´s bedside for continuous monitoring. The shear viscosity measured at a given time and the change in shear viscosity over time (m) using PIEZ system could be comparable to other viscoelastic monitoring devices, such as FOR [
36] or ROTEM [
30]. In further studies, PIEZ will be also compared with these devices. For further applications at the operation theater, hardware improvements and miniaturization of the PIEZ system are necessary. For example, a disposable measuring chamber could be created as a cuvette or using a microfluidic system, the measuring chamber could be connected to the ECC system for the continuous monitoring of the coagulation. In addition, a cleaning and waste reservoir could be integrated into the microfluidic system, and the pipetting steps could be minimized by automatization.
Aptamers are promising drug candidates with the ability to bind to specific targets, such as cells or proteins (growth factors, transcription factors, enzymes, immunoglobulins, and receptors) with high specificity and affinity and have the ability to modulate the targets’ activities [
11,
37,
38]. In this study, using the new PIEZ system, we were able to reliably measure the coagulation inhibiting effect of the thrombin binding aptamer NU172 after static and dynamic incubation and the ability of its complementary antidote (AD) to abrogate the coagulation inhibitory effect of NU172. In our previous study, the required time for the generation of double-stranded complexes was examined [
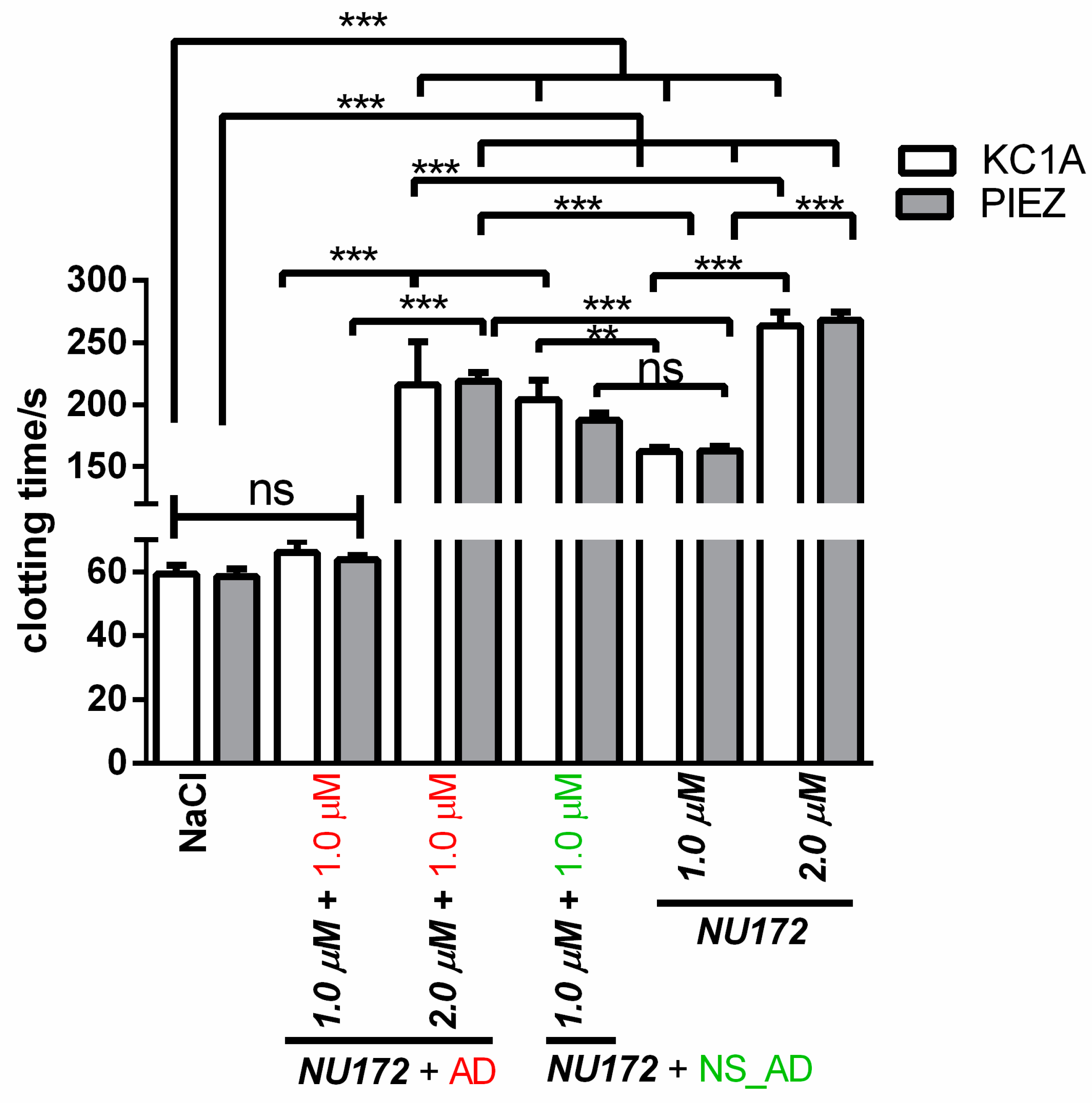
7], and it was found that the AD was able to bind already after 2 min to the NU172 aptamer, which resulted in rapid abrogation of the anticoagulant activity of NU172 after 5 min in whole blood.
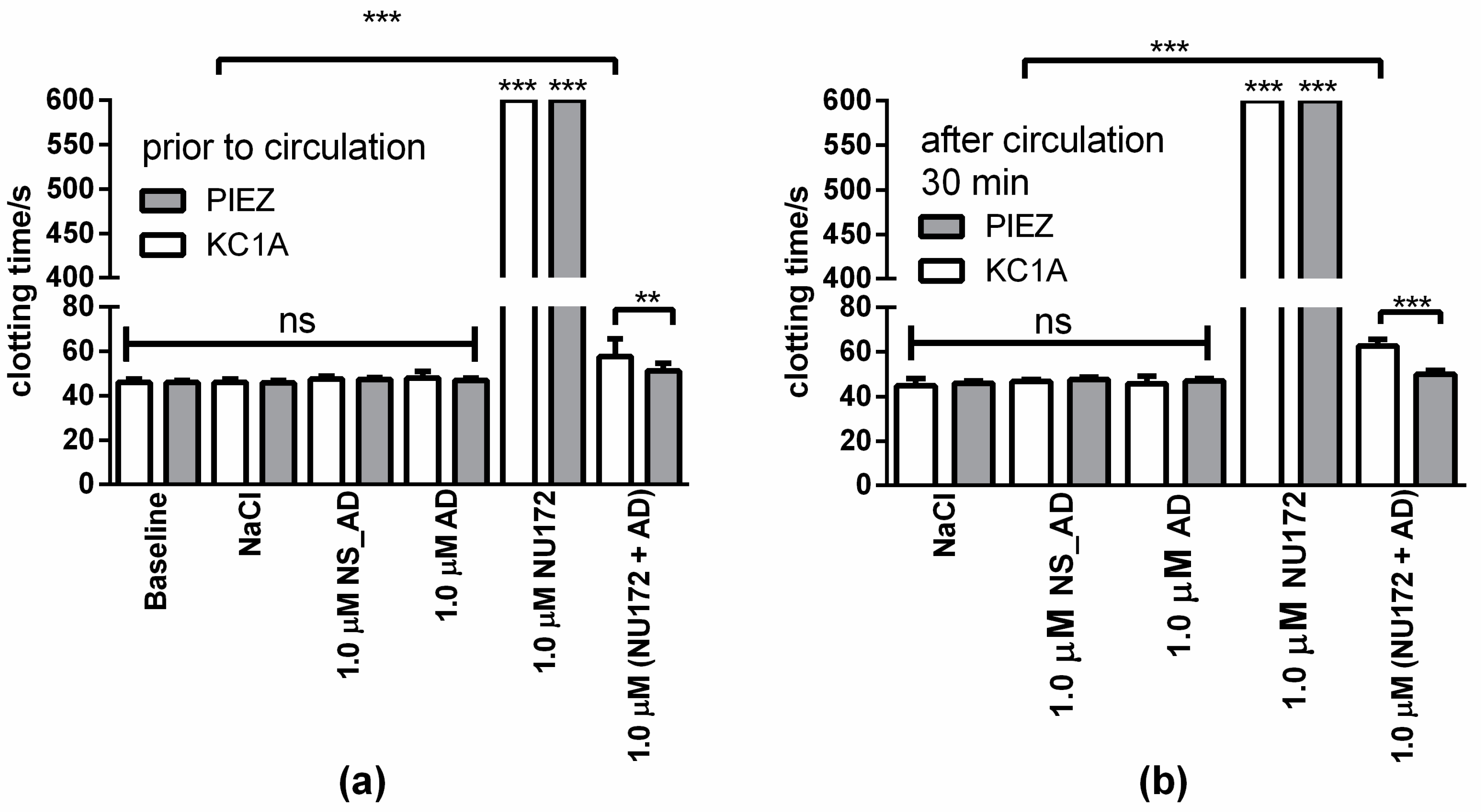
The addition of 1.0 µM NU172 into the blood led to prolonged CT and decreased m, η′, and η″ compared to the blood samples without oligonucleotide addition. Using PIEZ and different NU172 concentrations, the required aptamer concentration for efficient inhibition of coagulation could be determined. The in vitro rotation experiments with heparinized blood showed that the coagulation can be further inhibited by the addition of NU172 aptamer. Since the anticoagulant effect of aptamers can be rapidly interrupted by a corresponding AD, these aptamers are potent candidates for the applications during extracorporeal circulation in combination with a reduced heparin concentration or for substitution of heparin by a sufficient amount of aptamer in heparin-induced thrombocytopenia (HIT) patients.
In summary, the established PIEZ system is able to provide information in the form of CT, clot formation (m(η′), m(η″)), and clot firmness (η′and η″ at 300 s). The in vitro rotation experiments and the subsequent ELISA measurements confirmed the results obtained by using PIEZ and KC 1A. The addition of 1.0 µM NU172 into heparinized blood and the incubation at 37 °C for 30 min resulted in a significant reduction of β-TG, TAT, and FPA amounts compared to blood samples without NU172 addition. In this study, using the in vitro rotation model and the comparison with the ball coagulometer, a proof of concept was provided that the PIEZ can be used to analyze blood coagulation. In the next studies, we will perform blood coagulation analyses during a simulated ECC with a heart-lung machine and plan to optimize the system for automated blood sampling and blood coagulation analysis at defined time intervals. Furthermore, we aim to compare the PIEZ device with more sophisticated medical reference systems such as ROTEM or TEG.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}