Concurrent Validity, Test-Retest Reliability, and Sensitivity to Change of a Single Body-Fixed Sensor for Gait Analysis during Rollator-Assisted Walking in Acute Geriatric Patients

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population and Setting
2.3. Descriptive Measures
2.4. Gait Measurements
2.4.1. Test Procedure
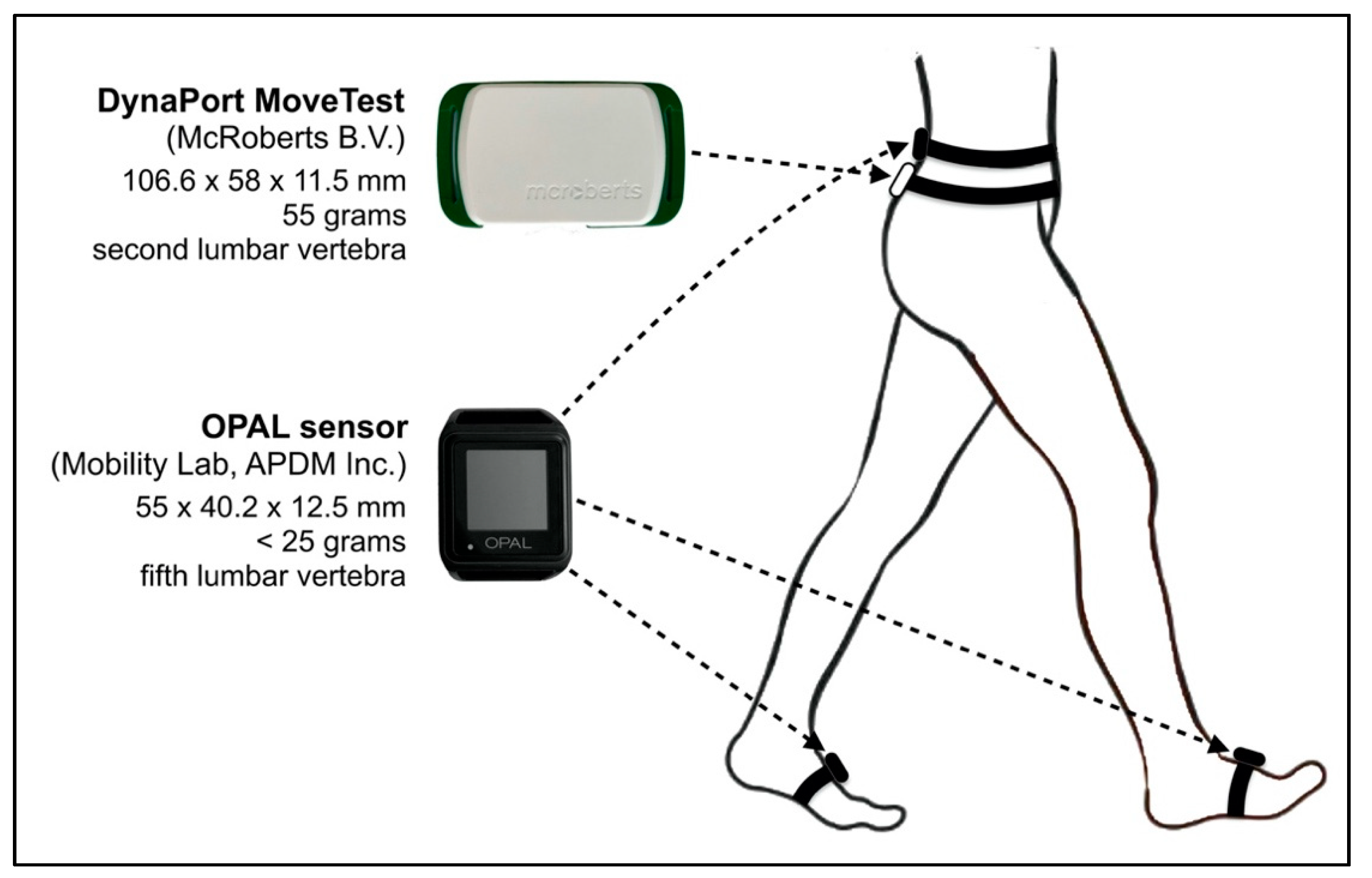
2.4.2. Instrumentation and Data Collection
2.5. Statistical Analysis
3. Results
3.1. Participant Characteristics
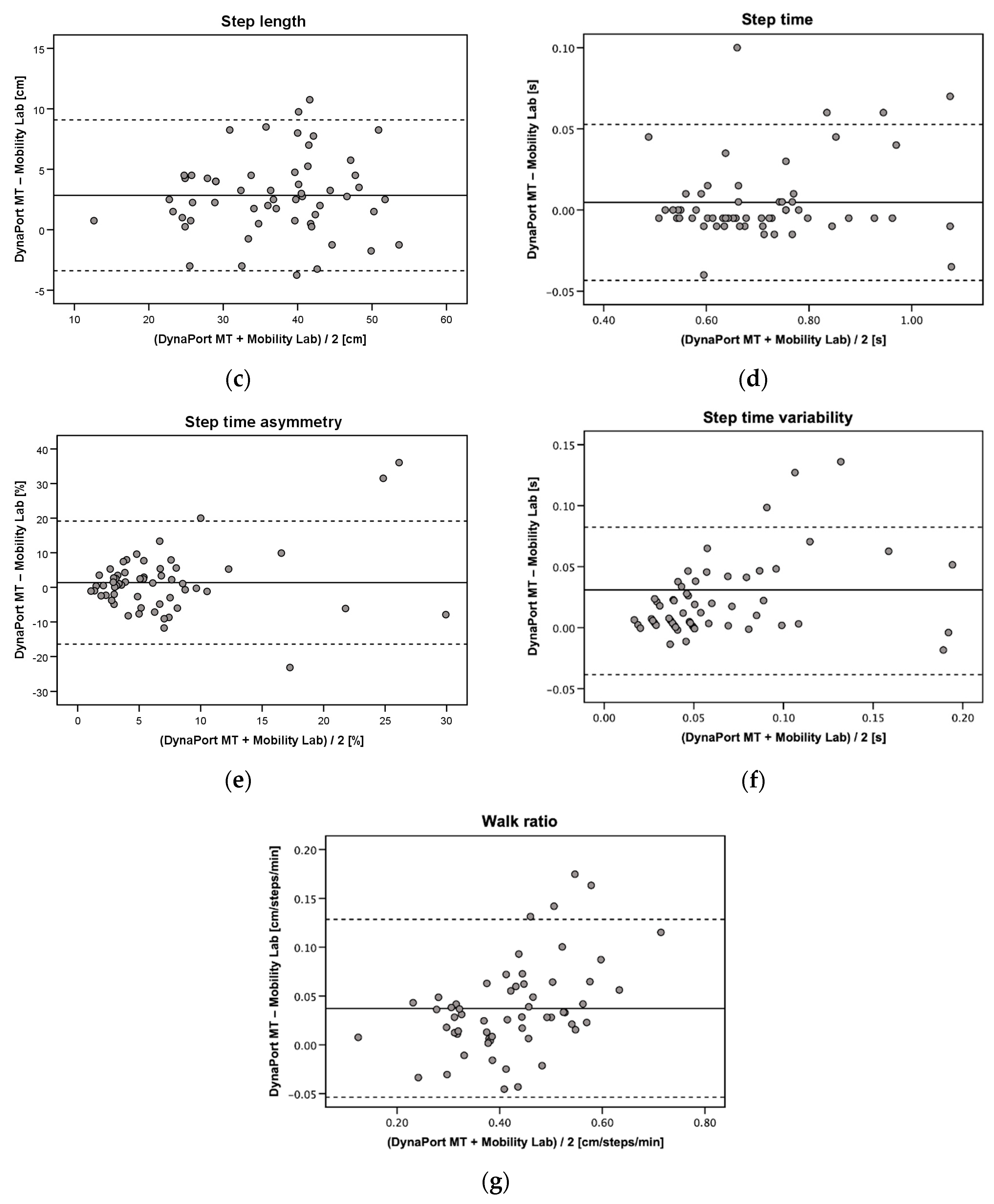
3.2. Concurrent Valdity
3.3. Test-Retest Reliability
3.4. Sensitivity to Change
4. Discussion
4.1. Concurrent Validity
4.2. Test-Retest Reliability
4.3. Sensitivity to Change
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mahlknecht, P.; Kiechl, S.; Bloem, B.R.; Willeit, J.; Scherfler, C.; Gasperi, A.; Rungger, G.; Poewe, W.; Seppi, K. Prevalence and burden of gait disorders in elderly men and women aged 60–97 years: A population-based study. PLoS ONE 2013, 8, e69627. [Google Scholar] [CrossRef] [PubMed]
- Verghese, J.; LeValley, A.; Hall, C.B.; Katz, M.J.; Ambrose, A.F.; Lipton, R.B. Epidemiology of gait disorders in community-residing older adults. J. Am. Geriatr. Soc. 2006, 54, 255–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verghese, J.; Holtzer, R.; Lipton, R.B.; Wang, C. Quantitative gait markers and incident fall risk in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64, 896–901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Kan, G.A.; Rolland, Y.; Andrieu, S.; Bauer, J.; Beauchet, O.; Bonnefoy, M.; Cesari, M.; Donini, L.M.; Gillette Guyonnet, S.; Inzitari, M.; et al. Gait speed at usual pace as a predictor of adverse outcomes in community-dwelling older people an International Academy on Nutrition and Aging (IANA) Task Force. J. Nutr. Health Aging 2009, 13, 881–889. [Google Scholar] [CrossRef]
- Perera, S.; Patel, K.V.; Rosano, C.; Rubin, S.M.; Satterfield, S.; Harris, T.; Ensrud, K.; Orwoll, E.; Lee, C.G.; Chandler, J.M.; et al. Gait Speed Predicts Incident Disability: A Pooled Analysis. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 63–71. [Google Scholar] [CrossRef]
- Sudarsky, L. Gait disorders: Prevalence, morbidity, and etiology. Adv. Neurol. 2001, 87, 111–117. [Google Scholar]
- Stolze, H.; Klebe, S.; Baecker, C.; Zechlin, C.; Friege, L.; Pohle, S.; Deuschl, G. Prevalence of gait disorders in hospitalized neurological patients. Mov. Disord. 2005, 20, 89–94. [Google Scholar] [CrossRef]
- Buurman, B.M.; Hoogerduijn, J.G.; de Haan, R.J.; Abu-Hanna, A.; Lagaay, A.M.; Verhaar, H.J.; Schuurmans, M.J.; Levi, M.; de Rooij, S.E. Geriatric conditions in acutely hospitalized older patients: Prevalence and one-year survival and functional decline. PLoS ONE 2011, 6, e26951. [Google Scholar] [CrossRef]
- Kuzuya, M. Era of geriatric medical challenges: Multimorbidity among older patients. Geriatr. Gerontol. Int. 2019, 19, 699–704. [Google Scholar] [CrossRef]
- Andela, R.M.; Dijkstra, A.; Slaets, J.P.; Sanderman, R. Prevalence of frailty on clinical wards: Description and implications. Int. J. Nurs. Pract. 2010, 16, 14–19. [Google Scholar] [CrossRef]
- Lindemann, U. Spatiotemporal gait analysis of older persons in clinical practice and research. Z. Gerontol. Geriatr. 2020, 53, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Kressig, R.W.; Beauchet, O.; European, G.N.G. Guidelines for clinical applications of spatio-temporal gait analysis in older adults. Aging Clin. Exp. Res. 2006, 18, 174–176. [Google Scholar] [CrossRef] [PubMed]
- Kirtley, C. Clinical Gait Analysis: Theory and Practice; Elsevier: New York, NY, USA, 2006. [Google Scholar]
- Baker, R. Gait analysis methods in rehabilitation. J. Neuroeng. Rehabil. 2006, 3, 4. [Google Scholar] [CrossRef] [Green Version]
- Winter, D.A. Human balance and posture control during standing and walking. Gait Posture 1995, 3, 193–214. [Google Scholar] [CrossRef]
- Simon, S.R. Quantification of human motion: Gait analysis-benefits and limitations to its application to clinical problems. J. Biomech. 2004, 37, 1869–1880. [Google Scholar] [CrossRef]
- Shahabpoor, E.; Pavic, A. Measurement of Walking Ground Reactions in Real-Life Environments: A Systematic Review of Techniques and Technologies. Sensors 2017, 17, 2085. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Lach, J.; Lo, B.; Yang, G.-Z. Toward Pervasive Gait Analysis With Wearable Sensors: A Systematic Review. IEEE J. Biomed. Health Inform. 2016, 20, 1521–1537. [Google Scholar] [CrossRef]
- Muro-de-la-Herran, A.; Garcia-Zapirain, B.; Mendez-Zorrilla, A. Gait Analysis Methods: An Overview of Wearable and Non-Wearable Systems, Highlighting Clinical Applications. Sensors 2014, 14, 3362–3394. [Google Scholar] [CrossRef] [Green Version]
- Najafi, B.; Khan, T.; Wrobel, J. Laboratory in a box: Wearable sensors and its advantages for gait analysis. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2011, 2011, 6507–6510. [Google Scholar] [CrossRef]
- Tao, W.; Liu, T.; Zheng, R.; Feng, H. Gait analysis using wearable sensors. Sensors 2012, 12, 2255–2283. [Google Scholar] [CrossRef] [PubMed]
- Aminian, K.; Najafi, B. Capturing human motion using body-fixed sensors: Outdoor measurement and clinical applications. Comput. Animat. Virtual Worlds 2004, 15, 79–94. [Google Scholar] [CrossRef]
- Seel, T.; Raisch, J.; Schauer, T. IMU-based joint angle measurement for gait analysis. Sensors 2014, 14, 6891–6909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shull, P.B.; Jirattigalachote, W.; Hunt, M.A.; Cutkosky, M.R.; Delp, S.L. Quantified self and human movement: A review on the clinical impact of wearable sensing and feedback for gait analysis and intervention. Gait Posture 2014, 40, 11–19. [Google Scholar] [CrossRef]
- Caldas, R.; Mundt, M.; Potthast, W.; Buarque de Lima Neto, F.; Markert, B. A systematic review of gait analysis methods based on inertial sensors and adaptive algorithms. Gait Posture 2017, 57, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Fong, D.T.; Chan, Y.Y. The use of wearable inertial motion sensors in human lower limb biomechanics studies: A systematic review. Sensors 2010, 10, 11556–11565. [Google Scholar] [CrossRef] [Green Version]
- Kobsar, D.; Charlton, J.M.; Tse, C.T.F.; Esculier, J.-F.; Graffos, A.; Krowchuk, N.M.; Thatcher, D.; Hunt, M.A. Validity and reliability of wearable inertial sensors in healthy adult walking: A systematic review and meta-analysis. J. Neuroeng. Rehabil. 2020, 17, 62. [Google Scholar] [CrossRef] [PubMed]
- Morris, R.; Stuart, S.; McBarron, G.; Fino, P.C.; Mancini, M.; Curtze, C. Validity of Mobility Lab (version 2) for gait assessment in young adults, older adults and Parkinson’s disease. Physiol. Meas. 2019, 40, 095003. [Google Scholar] [CrossRef]
- Bertoli, M.; Cereatti, A.; Trojaniello, D.; Avanzino, L.; Pelosin, E.; Del Din, S.; Rochester, L.; Ginis, P.; Bekkers, E.M.J.; Mirelman, A.; et al. Estimation of spatio-temporal parameters of gait from magneto-inertial measurement units: Multicenter validation among Parkinson, mildly cognitively impaired and healthy older adults. Biomed. Eng. Online 2018, 17, 58. [Google Scholar] [CrossRef] [Green Version]
- Kluge, F.; Gaßner, H.; Hannink, J.; Pasluosta, C.; Klucken, J.; Eskofier, B.M. Towards Mobile Gait Analysis: Concurrent Validity and Test-Retest Reliability of an Inertial Measurement System for the Assessment of Spatio-Temporal Gait Parameters. Sensors 2017, 17, 1522. [Google Scholar] [CrossRef]
- Schmitz-Hübsch, T.; Brandt, A.U.; Pfueller, C.; Zange, L.; Seidel, A.; Kühn, A.A.; Paul, F.; Minnerop, M.; Doss, S. Accuracy and repeatability of two methods of gait analysis—GaitRite™ und Mobility Lab™—In subjects with cerebellar ataxia. Gait Posture 2016, 48, 194–201. [Google Scholar] [CrossRef]
- Saremi, K.; Marehbian, J.; Yan, X.; Regnaux, J.P.; Elashoff, R.; Bussel, B.; Dobkin, B.H. Reliability and validity of bilateral thigh and foot accelerometry measures of walking in healthy and hemiparetic subjects. Neurorehabil. Neural. Repair 2006, 20, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Houdijk, H.; Appelman, F.M.; Van Velzen, J.M.; Van der Woude, L.H.; Van Bennekom, C.A. Validity of DynaPort GaitMonitor for assessment of spatiotemporal parameters in amputee gait. J. Rehabil. Res. Dev. 2008, 45, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Aminian, K.; Trevisan, C.; Najafi, B.; Dejnabadi, H.; Frigo, C.; Pavan, E.; Telonio, A.; Cerati, F.; Marinoni, E.C.; Robert, P.; et al. Evaluation of an ambulatory system for gait analysis in hip osteoarthritis and after total hip replacement. Gait Posture 2004, 20, 102–107. [Google Scholar] [CrossRef]
- Mundt, M.; Batista, J.P.; Markert, B.; Bollheimer, C.; Laurentius, T. Walking with rollator: A systematic review of gait parameters in older persons. Eur. Rev. Aging Phys. Act. 2019, 16, 15. [Google Scholar] [CrossRef]
- Nguyen, A.; Roth, N.; Ghassemi, N.H.; Hannink, J.; Seel, T.; Klucken, J.; Gassner, H.; Eskofier, B.M. Development and clinical validation of inertial sensor-based gait-clustering methods in Parkinson’s disease. J. Neuroeng. Rehabil. 2019, 16, 77. [Google Scholar] [CrossRef]
- Hartmann, A.; Luzi, S.; Murer, K.; de Bie, R.A.; de Bruin, E.D. Concurrent validity of a trunk tri-axial accelerometer system for gait analysis in older adults. Gait Posture 2009, 29, 444–448. [Google Scholar] [CrossRef]
- Hartmann, A.; Murer, K.; de Bie, R.A.; de Bruin, E.D. Reproducibility of spatio-temporal gait parameters under different conditions in older adults using a trunk tri-axial accelerometer system. Gait Posture 2009, 30, 351–355. [Google Scholar] [CrossRef]
- Zijlstra, A.; Zijlstra, W. Trunk-acceleration based assessment of gait parameters in older persons: A comparison of reliability and validity of four inverted pendulum based estimations. Gait Posture 2013, 38, 940–944. [Google Scholar] [CrossRef]
- Bautmans, I.; Jansen, B.; Van Keymolen, B.; Mets, T. Reliability and clinical correlates of 3D-accelerometry based gait analysis outcomes according to age and fall-risk. Gait Posture 2011, 33, 366–372. [Google Scholar] [CrossRef]
- Cole, M.H.; van den Hoorn, W.; Kavanagh, J.K.; Morrison, S.; Hodges, P.W.; Smeathers, J.E.; Kerr, G.K. Concurrent Validity of Accelerations Measured Using a Tri-Axial Inertial Measurement Unit while Walking on Firm, Compliant and Uneven Surfaces. PLoS ONE 2014, 9, e98395. [Google Scholar] [CrossRef]
- Rampp, A.; Barth, J.; Schülein, S.; Gaßmann, K.G.; Klucken, J.; Eskofier, B.M. Inertial sensor-based stride parameter calculation from gait sequences in geriatric patients. IEEE Trans. Biomed. Eng. 2015, 62, 1089–1097. [Google Scholar] [CrossRef] [PubMed]
- Schwenk, M.; Schmidt, M.; Pfisterer, M.; Oster, P.; Hauer, K. Rollator use adversely impacts on assessment of gait and mobility during geriatric rehabilitation. J. Rehabil. Med. 2011, 43, 424–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bateni, H.; Maki, B.E. Assistive devices for balance and mobility: Benefits, demands, and adverse consequences. Arch. Phys. Med. Rehabil. 2005, 86, 134–145. [Google Scholar] [CrossRef] [PubMed]
- Graafmans, W.C.; Lips, P.; Wijlhuizen, G.J.; Pluijm, S.M.; Bouter, L.M. Daily physical activity and the use of a walking aid in relation to falls in elderly people in a residential care setting. Z. Gerontol. Geriatr. 2003, 36, 23–28. [Google Scholar] [CrossRef] [Green Version]
- Bodilsen, A.C.; Klausen, H.H.; Petersen, J.; Beyer, N.; Andersen, O.; Jørgensen, L.M.; Juul-Larsen, H.G.; Bandholm, T. Prediction of Mobility Limitations after Hospitalization in Older Medical Patients by Simple Measures of Physical Performance Obtained at Admission to the Emergency Department. PLoS ONE 2016, 11, e0154350. [Google Scholar] [CrossRef]
- Webber, S.C.; St John, P.D. Changes in Intensity and Duration of Walking among Older Adults from In-Patient Geriatric Rehabilitation to Home. Physiother. Can. 2018, 70, 341–348. [Google Scholar] [CrossRef]
- Deutsches Institut für Medizinische Dokumentation und Information. OPS Version 2020—Kapitel 8: Nicht Operative Therapeutische Massnahmen, Frührehabillitative und Physikalische Therapie. Available online: https://www.dimdi.de/static/de/klassifikationen/ops/kode-suche/opshtml2020/block-8-55...8-60.htm (accessed on 28 July 2020).
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”a practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Bonett, D.G. Sample size requirements for estimating intraclass correlations with desired precision. Stats. Med. 2002, 21, 1331–1335. [Google Scholar] [CrossRef]
- Wolak, M.E.; Fairbairn, D.J.; Paulsen, Y.R. Guidelines for estimating repeatability. Methods Ecol. Evol. 2012, 3, 129–137. [Google Scholar] [CrossRef]
- Sheikh, J.I.; Yesavage, J.A. Geriatric Depression Scale (GDS): Recent evidence and development of a shorter version. Clin. Gerontol. 1986, 5, 165–173. [Google Scholar] [CrossRef]
- Kempen, G.I.; Yardley, L.; van Haastregt, J.C.; Zijlstra, G.A.; Beyer, N.; Hauer, K.; Todd, C. The Short FES-I: A shortened version of the falls efficacy scale-international to assess fear of falling. Age Ageing 2008, 37, 45–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The barthel index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar] [PubMed]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- De Morton, N.A.; Davidson, M.; Keating, J.L. The de Morton Mobility Index (DEMMI): An essential health index for an ageing world. Health Qual. Life Outcomes 2008, 6, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zijlstra, W.; Hof, A.L. Assessment of spatio-temporal gait parameters from trunk accelerations during human walking. Gait Posture 2003, 18, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Micó-Amigo, M.E.; Kingma, I.; Ainsworth, E.; Walgaard, S.; Niessen, M.; van Lummel, R.C.; van Dieën, J.H. A novel accelerometry-based algorithm for the detection of step durations over short episodes of gait in healthy elderly. J. Neuroeng. Rehabil. 2016, 13, 38. [Google Scholar] [CrossRef] [Green Version]
- Moe-Nilssen, R.; Helbostad, J.L. Estimation of gait cycle characteristics by trunk accelerometry. J. Biomech. 2004, 37, 121–126. [Google Scholar] [CrossRef]
- Dijkstra, B.; Zijlstra, W.; Scherder, E.; Kamsma, Y. Detection of walking periods and number of steps in older adults and patients with Parkinson’s disease: Accuracy of a pedometer and an accelerometry-based method. Age Ageing 2008, 37, 436–441. [Google Scholar] [CrossRef] [Green Version]
- Portney, L.; Watkins, M.P. Foundation of Clinical Research. Application to Practice, 3rd ed.; Pearson Education: Upper Saddle River, NJ, USA, 2009; pp. 61–77. [Google Scholar]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Critchley, L.A.; Critchley, J.A. A meta-analysis of studies using bias and precision statistics to compare cardiac output measurement techniques. J. Clin. Monit. Comput. 1999, 15, 85–91. [Google Scholar] [CrossRef]
- Atkinson, G.; Nevill, A.M. Statistical methods for assessing measurement error (reliability) in variables relevant to sports medicine. Sports Med. 1998, 26, 217–238. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.L.; Hsieh, C.L.; Wu, R.M.; Tai, C.H.; Lin, C.H.; Lu, W.S. Minimal detectable change of the timed “up & go” test and the dynamic gait index in people with Parkinson disease. Phys. Ther. 2011, 91, 114–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Latorre, J.; Colomer, C.; Alcañiz, M.; Llorens, R. Gait analysis with the Kinect v2: Normative study with healthy individuals and comprehensive study of its sensitivity, validity, and reliability in individuals with stroke. J. Neuroeng. Rehabil. 2019, 16, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohannon, R.W.; Glenney, S.S. Minimal clinically important difference for change in comfortable gait speed of adults with pathology: A systematic review. J. Eval. Clin. Pract. 2014, 20, 295–300. [Google Scholar] [CrossRef]
- Chui, K.; Hood, E.; Klima, D. Meaningful Change in Walking Speed. Top. Geriatr. Rehabil. 2012, 28, 97–103. [Google Scholar] [CrossRef]
- Perera, S.; Mody, S.H.; Woodman, R.C.; Studenski, S.A. Meaningful change and responsiveness in common physical performance measures in older adults. J. Am. Geriatr. Soc. 2006, 54, 743–749. [Google Scholar] [CrossRef]
- Husted, J.A.; Cook, R.J.; Farewell, V.T.; Gladman, D.D. Methods for assessing responsiveness: A critical review and recommendations. J. Clin. Epidemiol. 2000, 53, 459–468. [Google Scholar] [CrossRef]
- Lindemann, U.; Schwenk, M.; Schmitt, S.; Weyrich, M.; Schlicht, W.; Becker, C. Effect of uphill and downhill walking on walking performance in geriatric patients using a wheeled walker. Z. Gerontol. Geriatr. 2017, 50, 483–487. [Google Scholar] [CrossRef]
- Byun, S.; Han, J.W.; Kim, T.H.; Kim, K.W. Test-Retest Reliability and Concurrent Validity of a Single Tri-Axial Accelerometer-Based Gait Analysis in Older Adults with Normal Cognition. PLoS ONE 2016, 11, e0158956. [Google Scholar] [CrossRef] [Green Version]
- Godfrey, A.; Del Din, S.; Barry, G.; Mathers, J.C.; Rochester, L. Instrumenting gait with an accelerometer: A system and algorithm examination. Med. Eng. Phys. 2015, 37, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Brach, J.S.; Perera, S.; Studenski, S.; Newman, A.B. The reliability and validity of measures of gait variability in community-dwelling older adults. Arch. Phys. Med. Rehabil. 2008, 89, 2293–2296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henriksen, M.; Lund, H.; Moe-Nilssen, R.; Bliddal, H.; Danneskiod-Samsøe, B. Test-retest reliability of trunk accelerometric gait analysis. Gait Posture 2004, 19, 288–297. [Google Scholar] [CrossRef]
- Bodilsen, A.C.; Juul-Larsen, H.G.; Petersen, J.; Beyer, N.; Andersen, O.; Bandholm, T. Feasibility and inter-rater reliability of physical performance measures in acutely admitted older medical patients. PLoS ONE 2015, 10, e0118248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, W.; Regterschot, G.R.H.; Schaabova, H.; Baldus, H.; Zijlstra, W. Test-retest reliability of a pendant-worn sensor device in measuring chair rise performance in older persons. Sensors 2014, 14, 8705–8717. [Google Scholar] [CrossRef]
- Washabaugh, E.P.; Kalyanaraman, T.; Adamczyk, P.G.; Claflin, E.S.; Krishnan, C. Validity and repeatability of inertial measurement units for measuring gait parameters. Gait Posture 2017, 55, 87–93. [Google Scholar] [CrossRef] [Green Version]
- Fortinsky, R.H.; Covinsky, K.E.; Palmer, R.M.; Landefeld, C.S. Effects of functional status changes before and during hospitalization on nursing home admission of older adults. J. Gerontol. A Biol. Sci. Med. Sci. 1999, 54, M521–M526. [Google Scholar] [CrossRef]
- Zisberg, A.; Shadmi, E.; Sinoff, G.; Gur-Yaish, N.; Srulovici, E.; Admi, H. Low mobility during hospitalization and functional decline in older adults. J. Am. Geriatr. Soc. 2011, 59, 266–273. [Google Scholar] [CrossRef]
- Covinsky, K.E.; Palmer, R.M.; Fortinsky, R.H.; Counsell, S.R.; Stewart, A.L.; Kresevic, D.; Burant, C.J.; Landefeld, C.S. Loss of independence in activities of daily living in older adults hospitalized with medical illnesses: Increased vulnerability with age. J. Am. Geriatr. Soc. 2003, 51, 451–458. [Google Scholar] [CrossRef]
- Gill, T.M.; Gahbauer, E.A.; Han, L.; Allore, H.G. Functional trajectories in older persons admitted to a nursing home with disability after an acute hospitalization. J. Am. Geriatr. Soc. 2009, 57, 195–201. [Google Scholar] [CrossRef]
- Mahoney, J.E.; Sager, M.A.; Jalaluddin, M. New walking dependence associated with hospitalization for acute medical illness: Incidence and significance. J. Gerontol. A Biol. Sci. Med. Sci. 1998, 53, M307–M312. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | n = 58 |
|---|---|
| Age [years] | 83.7 ± 5.9 |
| Sex [female] | 39 (67.2) |
| Diagnoses [n] | 9.9 ± 5.3 |
| Medications [n] | 11.1 ± 4.3 |
| Fall in the previous year 1 [n] | 45 (78.9) |
| Mini-Mental State Examination [pt.] | 22.7 ± 4.7 |
| Geriatric Depression Scale [pt.] | 5.3 ± 3.3 |
| Falls Efficacy Scale-International [pt.] | 10 [7–26] |
| EuroQol-5 Dimensions [pt.] | 0.68 ± 0.24 |
| Barthel Index [pt.] | 72.1 ± 20.1 |
| Short Physical Performance Battery [pt.] | 4.3 ± 1.7 |
| Gait speed [m/s] | 0.45 ± 0.18 |
| De Morton Mobility Index [pt.] | 52.2 ± 8.1 |
| Handgrip strength [kg] | 16.9 ± 7.7 |
| Parameter | DynaPort MT (Mean ± SD) | Mobility Lab (Mean ± SD) | Bias (95% CI) | 95% LOA | PE | ICC2,1 (95% CI) |
|---|---|---|---|---|---|---|
| Gait speed [m/s] | 0.56 ± 0.18 | 0.56 ± 0.18 | 0.00 (–0.01 to 0.01) | –0.08 to 0.08 | 13.9 | 0.98 (0.96 to 0.99) |
| Cadence [steps/min] | 88.4 ± 16.5 | 88.5 ± 16.4 | –0.1 (–0.9 to 0.7) | –5.9 to 5.7 | 6.6 | 0.98 (0.97 to 0.99) |
| Step length [cm] | 38.0 ± 9.1 | 35.1 ± 8.9 | 2.8 (2.0 to 3.7) | –3.4 to 9.1 | 17.1 | 0.89 (0.55 to 0.96) |
| Step time [s] | 0.71 ± 0.15 | 0.71 ± 0.14 | 0.00 (–0.01 to 0.00) | –0.09 to 0.10 | 6.8 | 0.99 (0.98 to 0.99) |
| Step time asymmetry [%] | 7.67 ± 8.56 | 6.30 ± 6.60 | 1.37 (–1.02 to 3.75) | –16.41 to 19.15 | 254.6 | 0.29 (0.04 to 0.51) |
| Step time variability [s] | 0.07 ± 0.05 | 0.05 ± 0.04 | 0.02 (0.01 to 0.03) | –0.04 to 0.08 | 95.2 | 0.68 (0.31 to 0.84) |
| Walk ratio [cm/steps/min] | 0.44 ± 0.12 | 0.40 ± 0.10 | 0.04 (–0.05 to 0.03) | –0.05 to 0.13 | 21.5 | 0.87 (0.56 to 0.95) |
| Parameter | Pretest (Mean ± SD) | Retest (Mean ± SD) | Bias (95% CI) | 95% LOA | ICC2,1 (95% CI) | SEM (SEM%) | MDC95 (MDC95%) |
|---|---|---|---|---|---|---|---|
| Gait speed [m/s] | 0.60 ± 0.18 | 0.60 ± 0.20 | 0.00 (–0.03 to 0.03) | –0.19 to 0.18 | 0.89 (0.79 to 0.94) | 0.06 (10.6) | 0.18 (29.3) |
| Cadence [steps/min] | 90.1 ± 15.3 | 91.7 ± 16.7 | –1.7 (–3.7 to 0.3) | –13.9 to 10.6 | 0.92 (0.86 to 0.96) | 4.4 (4.9) | 12.2 (13.5) |
| Step length [cm] | 39.4 ± 9.4 | 38.9 ± 9.7 | 0.5 (–1.2 to 2.3) | –10.1 to 11.1 | 0.84 (0.72 to 0.91) | 3.8 (9.8) | 10.6 (27.0) |
| Step time [s] | 0.69 ± 0.13 | 0.68 ± 0.13 | 0.01 (–0.01 to 0.03) | –0.12 to 0.10 | 0.91 (0.84 to 0.95) | 0.04 (6.5) | 0.12 (18.0) |
| Step time asymmetry [%] | 8.8 ± 9.2 | 9.6 ± 9.9 | –0.8 (–3.1 to 1.5) | –15.0 to 13.4 | 0.72 (0.53 to 0.84) | 5.1 (55.7) | 14.2 (154.5) |
| Step time variability [s] | 0.07 ± 0.04 | 0.08 ± 0.06 | –0.01 (–0.02 to 0.01) | –0.09 to 0.08 | 0.58 (0.33 to 0.75) | 0.03 (42.3) | 0.09 (117.2) |
| Walk ratio [cm/steps/min] | 0.45 ± 0.12 | 0.44 ± 0.12 | 0.01 (–0.01 to 0.03) | –0.12 to 0.15 | 0.83 (0.71 to 0.91) | 0.04 (10.1) | 0.12 (28.1) |
| Parameter | T1 (Mean ± SD) | T2 (Mean ± SD) | p-Value 1 | SRM |
|---|---|---|---|---|
| Gait speed [m/s] | ||||
| Improved | 0.54 ± 0.17 | 0.66 ± 0.18 | <0.001 | 0.99 |
| Stable | 0.54 ± 0.19 | 0.57 ± 0.22 | 0.389 | 0.26 |
| Worsened | 0.65 ± 0.21 | 0.58 ± 0.20 | 0.260 | −0.52 |
| Cadence [steps/min] | ||||
| Improved | 91.1 ± 12.3 | 96.6 ± 8.1 | 0.011 | 0.60 |
| Stable | 84.7 ± 18.0 | 84.4 ± 16.2 | 0.923 | −0.03 |
| Worsened | 90.0 ± 21.9 | 84.0 ± 20.9 | 0.093 | −0.85 |
| Step length [cm] | ||||
| Improved | 35.0 ± 9.9 | 41.5 ± 11.4 | <0.001 | 0.97 |
| Stable | 37.4 ± 9.2 | 39.5 ± 9.8 | 0.192 | 0.40 |
| Worsened | 43.2 ± 4.8 | 41.0 ± 6.8 | 0.387 | −0.39 |
| Step time [s] | ||||
| Improved | 0.68 ± 0.11 | 0.64 ± 0.05 | 0.061 | −0.42 |
| Stable | 0.74 ± 0.16 | 0.75 ± 0.17 | 0.852 | 0.06 |
| Worsened | 0.71 ± 0.20 | 0.75 ± 0.19 | 0.124 | 0.76 |
| Step time asymmetry [%] | ||||
| Improved | 8.4 ± 9.8 | 7.3 ± 7.3 | 0.224 | −0.09 |
| Stable | 6.9 ± 6.7 | 6.6 ± 5.2 | >0.999 | −0.04 |
| Worsened | 11.7 ± 14.5 | 12.0 ± 12.6 | 0.893 | 0.02 |
| Step time variability [s] | ||||
| Improved | 0.09 ± 0.08 | 0.06 ± 0.05 | 0.884 | −0.25 |
| Stable | 0.07 ± 0.05 | 0.09 ± 0.10 | 0.822 | 0.30 |
| Worsened | 0.07 ± 0.05 | 0.08 ± 0.03 | 0.854 | 0.21 |
| Walk ratio [cm/min/steps] | ||||
| Improved | 0.39 ± 0.12 | 0.43 ± 0.13 | 0.008 | 0.62 |
| Stable | 0.45 ± 0.11 | 0.48 ± 0.11 | 0.219 | 0.38 |
| Worsened | 0.50 ± 0.14 | 0.51 ± 0.14 | 0.748 | 0.14 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Werner, C.; Heldmann, P.; Hummel, S.; Bauknecht, L.; Bauer, J.M.; Hauer, K. Concurrent Validity, Test-Retest Reliability, and Sensitivity to Change of a Single Body-Fixed Sensor for Gait Analysis during Rollator-Assisted Walking in Acute Geriatric Patients. Sensors 2020, 20, 4866. https://doi.org/10.3390/s20174866
Werner C, Heldmann P, Hummel S, Bauknecht L, Bauer JM, Hauer K. Concurrent Validity, Test-Retest Reliability, and Sensitivity to Change of a Single Body-Fixed Sensor for Gait Analysis during Rollator-Assisted Walking in Acute Geriatric Patients. Sensors. 2020; 20(17):4866. https://doi.org/10.3390/s20174866
Chicago/Turabian StyleWerner, Christian, Patrick Heldmann, Saskia Hummel, Laura Bauknecht, Jürgen M. Bauer, and Klaus Hauer. 2020. "Concurrent Validity, Test-Retest Reliability, and Sensitivity to Change of a Single Body-Fixed Sensor for Gait Analysis during Rollator-Assisted Walking in Acute Geriatric Patients" Sensors 20, no. 17: 4866. https://doi.org/10.3390/s20174866