The Feasibility of Longitudinal Upper Extremity Motor Function Assessment Using EEG



Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
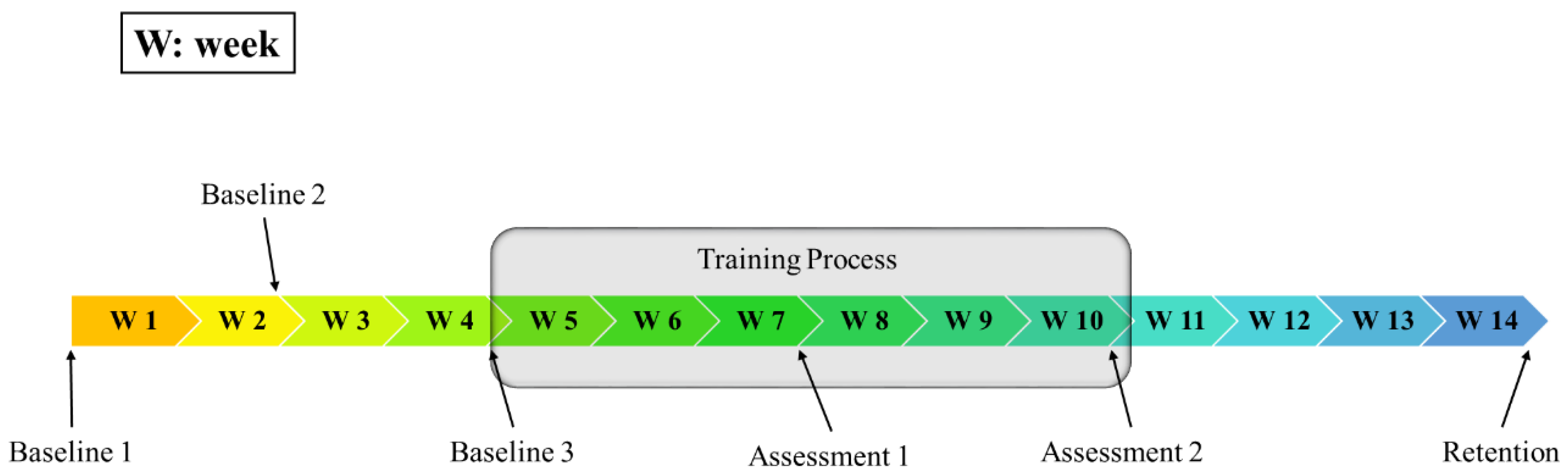
2.2. Participation Protocol
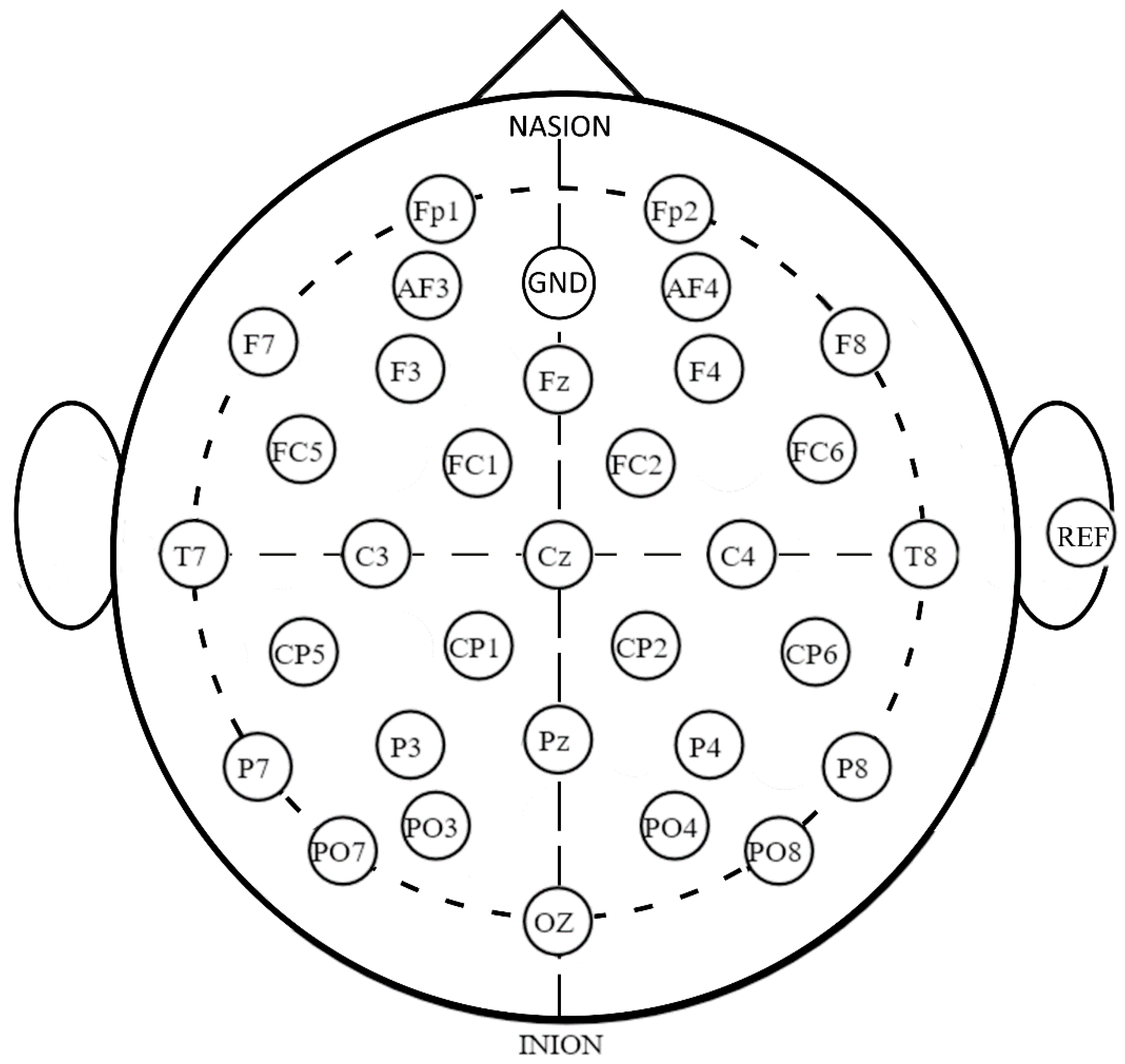
2.3. EEG Data Acquisition
2.4. Data Pre-Processing
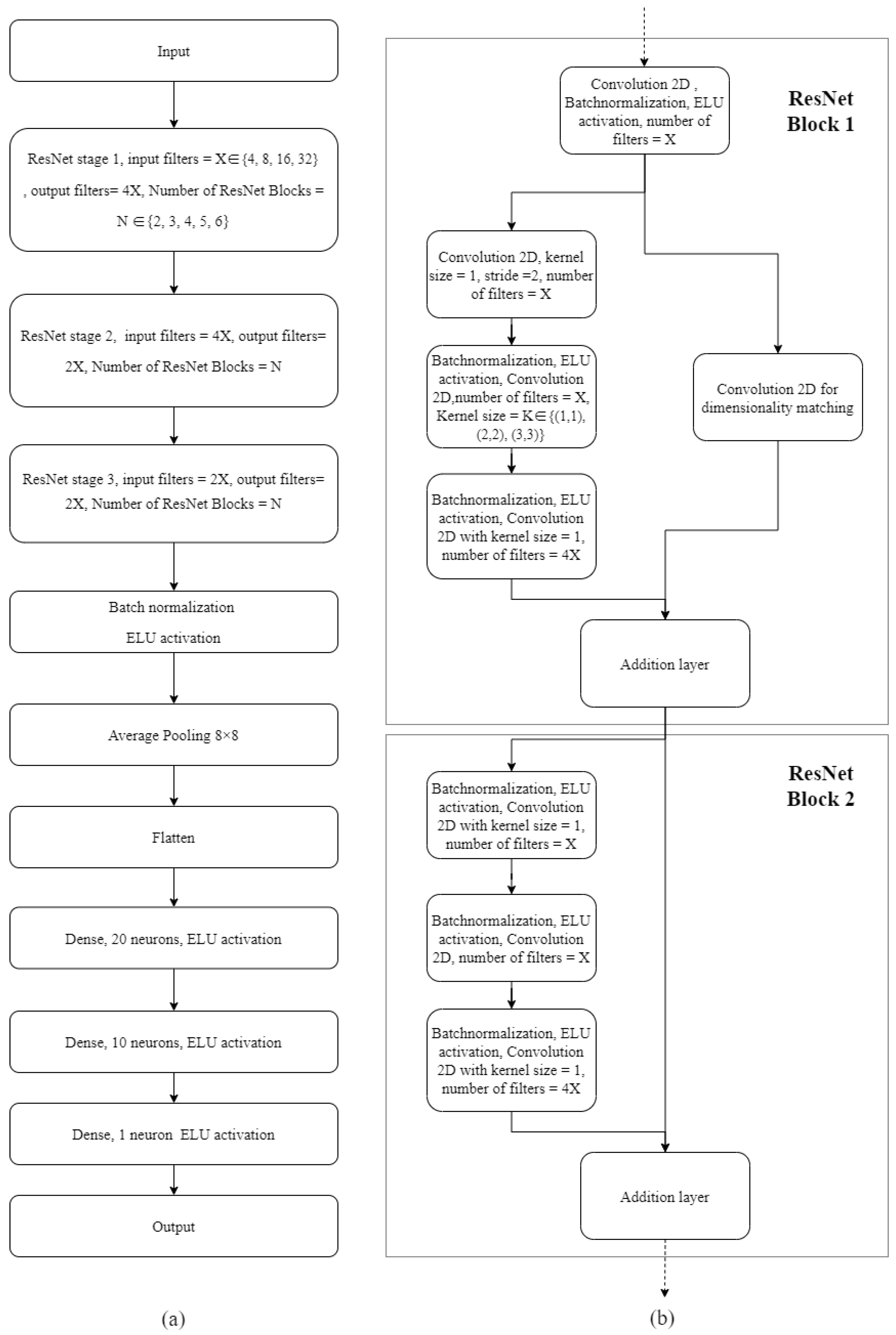
2.5. Neural Network Model Configuration, Hyperparameter Optimization and Testing
2.6. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. ANN Model Training and Hyperparameter Optimization
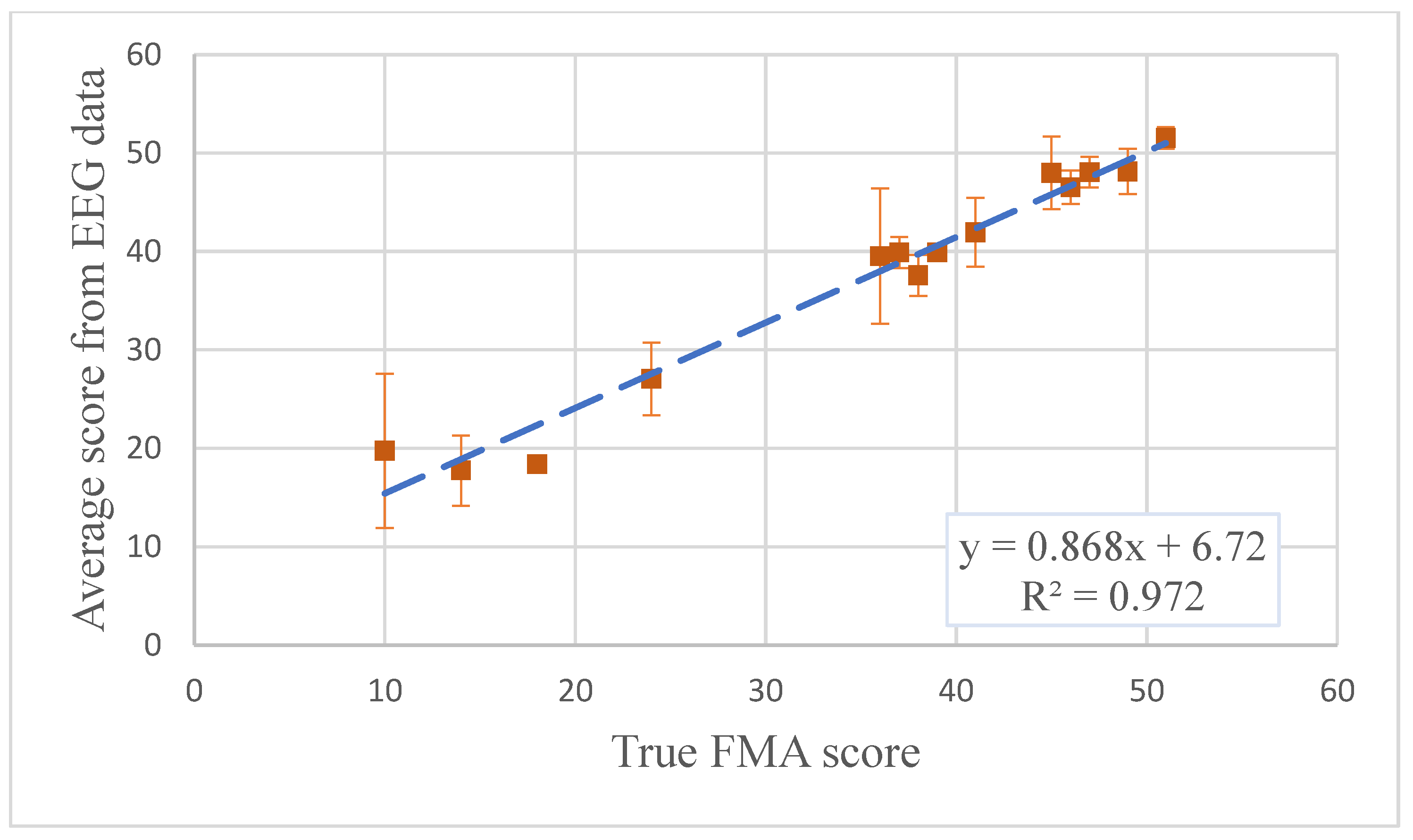
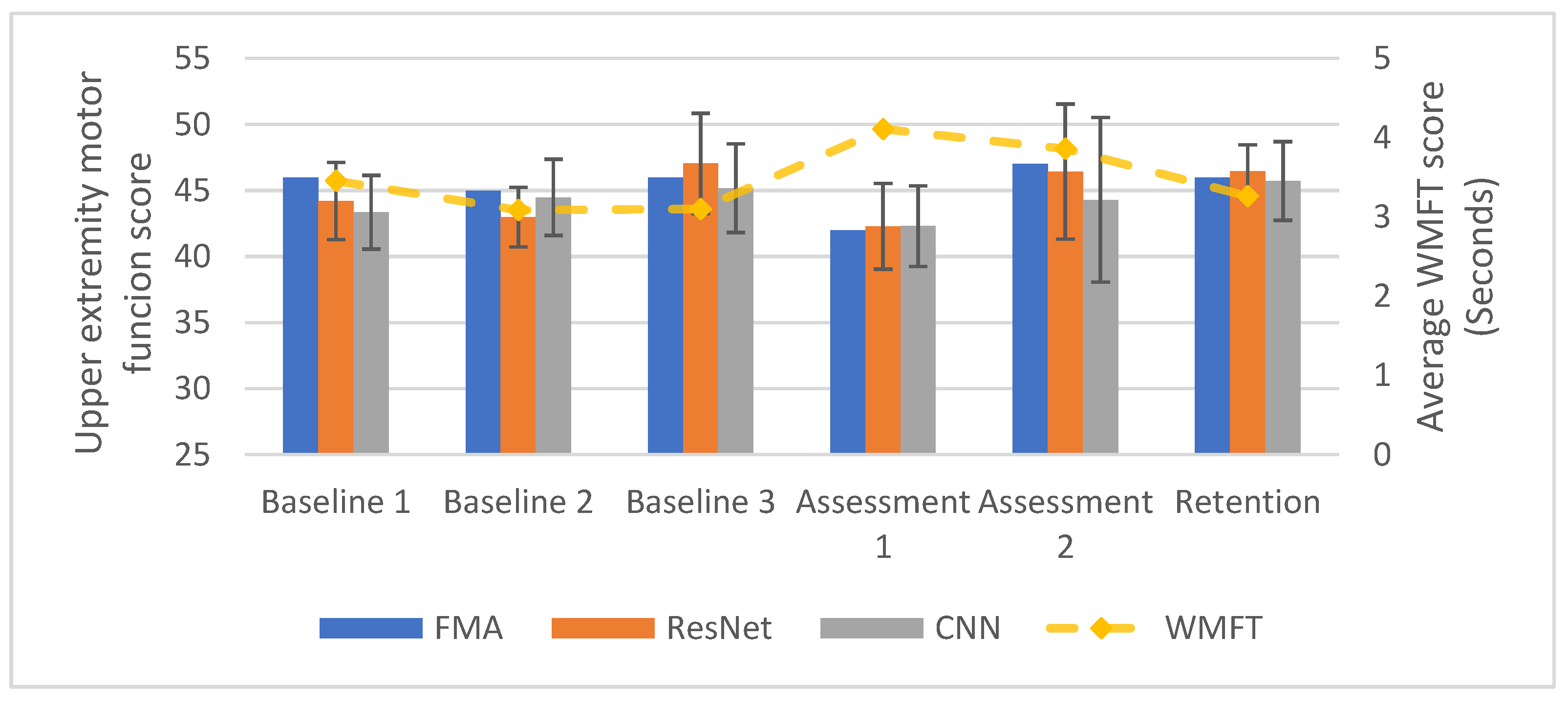
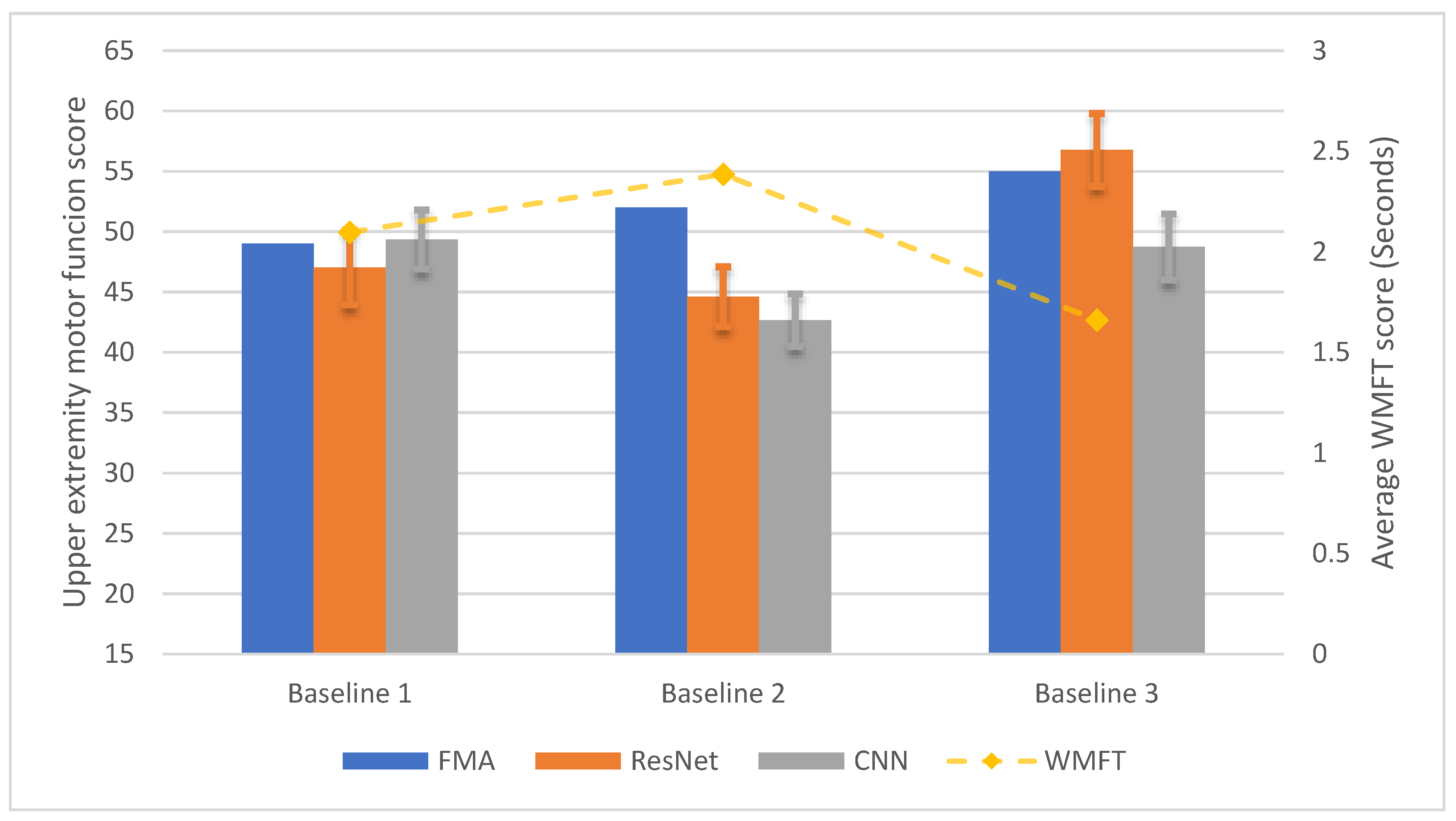
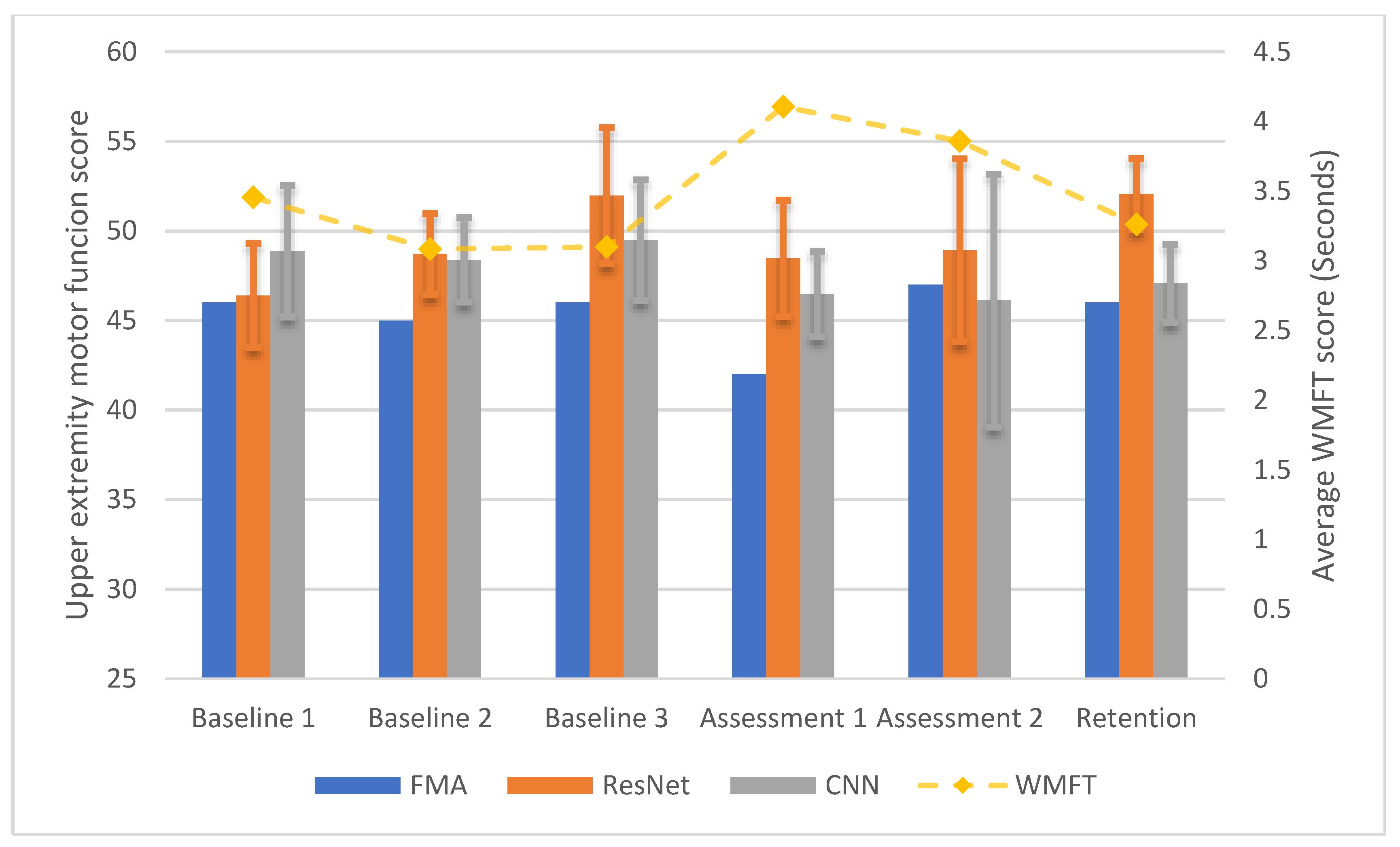
3.3. Longitudinal Within-Participant Test Result and Prediction
3.4. Longitudinal Cross-Participant Test Result and Prediction
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar] [CrossRef] [PubMed]
- Kwah, L.K.; Diong, J. National Institutes of Health Stroke Scale (NIHSS). J. Physiother. 2014, 60, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keith, R.; Granger, C.; Hamilton, B.; Sherwin, F. The functional independence measure: A new tool for rehabilitation. Adv. Clin. Rehabil. 1987, 1, 6–18. [Google Scholar]
- Pfurtscheller, G.; Lopes Da Silva, F.H. Event-related EEG/MEG synchronization and desynchronization: Basic principles. Clin. Neurophysiol. 1999, 110, 1842–1857. [Google Scholar] [CrossRef]
- Neuper, C.; Pfurtscheller, G. Event-related dynamics of cortical rhythms: Frequency-specific features and functional correlates. Int. J. Psychophysiol. 2001, 43, 41–58. [Google Scholar] [CrossRef]
- Anastasi, A.A.; Falzon, O.; Camilleri, K.; Vella, M.; Muscat, R. Brain Symmetry Index in Healthy and Stroke Patients for Assessment and Prognosis. Stroke Res. Treat. 2017, 2017, 1–9. [Google Scholar] [CrossRef]
- Leon-Carrion, J.; Martin-Rodriguez, J.F.; Damas-Lopez, J.; Barroso y Martin, J.M.; Dominguez-Morales, M.R. Delta-alpha ratio correlates with level of recovery after neurorehabilitation in patients with acquired brain injury. Clin. Neurophysiol. 2009, 120, 1039–1045. [Google Scholar] [CrossRef] [PubMed]
- Kawano, T.; Hattori, N.; Uno, Y.; Kitajo, K.; Hatakenaka, M.; Yagura, H.; Fujimoto, H.; Yoshioka, T.; Nagasako, M.; Otomune, H.; et al. Large-Scale Phase Synchrony Reflects Clinical Status after Stroke: An EEG Study. Neurorehabil. Neural Repair 2017, 31, 561–570. [Google Scholar] [CrossRef] [Green Version]
- Kawano, T.; Hattori, N.; Uno, Y.; Hatakenaka, M.; Yagura, H.; Fujimoto, H.; Yoshioka, T.; Nagasako, M.; Otomune, H.; Kitajo, K.; et al. Electroencephalographic Phase Synchrony Index as a Biomarker of Poststroke Motor Impairment and Recovery. Neurorehabil. Neural Repair 2020, 34, 711–722. [Google Scholar] [CrossRef]
- Zhang, X.; D’Arcy, R.; Menon, C. Scoring upper-extremity motor function from EEG with artificial neural networks: A preliminary study. J. Neural Eng. 2019, 16, 036013. [Google Scholar] [CrossRef]
- Riahi, N.; Vakorin, V.A.; Menon, C. Estimating Fugl-Meyer Upper Extremity Motor Score from Functional-Connectivity Measures. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 860–868. [Google Scholar] [CrossRef] [PubMed]
- Liyanage, S.R.; Guan, C.; Zhang, H.; Ang, K.K.; Xu, J.; Lee, T.H. Dynamically weighted ensemble classification for non-stationary EEG processing. J. Neural Eng. 2013, 10, 036007. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, A.; Raza, H.; Meena, Y.K.; Dutta, A.; Prasad, G. Online Covariate Shift Detection based Adaptive Brain-Computer Interface to Trigger Hand Exoskeleton Feedback for Neuro-Rehabilitation. IEEE Trans. Cogn. Dev. Syst. 2017, XX, 1–11. [Google Scholar] [CrossRef] [Green Version]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Identity Mappings in Deep Residual Networks. Eur. Conf. Comput. Vis. 2016, 630–645. [Google Scholar] [CrossRef] [Green Version]
- Orand, A.; Aksoy, E.E.; Miyasaka, H.; Levy, C.; Zhang, X.; Menon, C. Bilateral tactile feedback-enabled training for stroke survivors using microsoft kinecttm. Sens. Switz. 2019, 19, 3474. [Google Scholar] [CrossRef] [Green Version]
- Carson, N.; Leach, L.; Murphy, K.J. A re-examination of Montreal Cognitive Assessment (MoCA) cutoff scores. Int. J. Geriatr. Psychiatry 2017, 33, 379–388. [Google Scholar] [CrossRef]
- Stancák, A.; Pfurtscheller, G. Event-related desynchronisation of central beta-rhythms during brisk and slow self-paced finger movements of dominant and nondominant hand. Cogn. Brain Res. 1996, 4, 171–183. [Google Scholar] [CrossRef]
- Gao, L.; Wang, J.; Chen, L. Event-related desynchronization and synchronization quantification in motor-related EEG by Kolmogorov entropy. J. Neural Eng. 2013, 10, 036023. [Google Scholar] [CrossRef]
- Pfurtscheller, G.; Neuper, C. Simultaneous EEG 10 Hz desynchronization and 40 Hz synchronization during finger movements. Neuroreport 1992, 3, 1057–1060. [Google Scholar] [CrossRef]
- Pfurtscheller, G.; Brunner, C.; Schlögl, A.; Lopes da Silva, F.H. Mu rhythm (de)synchronization and EEG single-trial classification of different motor imagery tasks. Neuroimage 2006, 31, 153–159. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar] [CrossRef] [Green Version]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the Inception Architecture for Computer Vision. arXiv 2015, arXiv:1512.00567. [Google Scholar]
- Schirrmeister, R.T.; Springenberg, J.T.; Fiederer, L.D.J.; Glasstetter, M.; Eggensperger, K.; Tangermann, M.; Hutter, F.; Burgard, W.; Ball, T. Deep learning with convolutional neural networks for brain mapping and decoding of movement-related information from the human EEG. arXiv 2017, arXiv:1703.05051. [Google Scholar]
- Chollet, F. Keras. Github Repos. Available online: https://github.com/keras-team/keras (accessed on 25 September 2020).
- Tensorflow. TensorFlow. Available online: https://medium.com/tensorflow/tensorflow-at-google-i-o-2018-b6612840f59d (accessed on 25 September 2020).
- Apache Spark. Apache SparkTM—Lightning-Fast Cluster Computing. Available online: http://spark.apache.org/ (accessed on 25 September 2020).
- Bergstra, J.; Bardenet, R.; Bengio, Y.; Kégl, B. Algorithms for Hyper-Parameter Optimization. In Proceedings of the 24th International Conference on Neural Information Processing Systems, Granada, Spain, 12 December 2011; pp. 2546–2554. [Google Scholar]
- Gladstone, D.J.; Danells, C.J.; Black, S.E. The Fugl-Meyer Assessment of Motor Recovery after Stroke: A Critical Review of Its Measurement Properties. Neurorehabil. Neural Repair 2002, 16, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Van Der Lee, J.H.; Beckerman, H.; Lankhorst, G.J.; Bouter, L.M. The responsiveness of the Action Research Arm test and the Fugl-Meyer Assessment scale in chronic stroke patients. J. Rehabil. Med. 2001, 33, 110–113. [Google Scholar] [CrossRef] [Green Version]
- Sanford, J.; Moreland, J.; Swanson, L.R.; Stratford, P.W.; Gowland, C. Reliability of the Fugl-Meyer assessment for testing motor performance in patients following stroke. Phys. Ther. 1993, 73, 447–454. [Google Scholar] [CrossRef]
- Hsueh, I.-P.; Hsu, M.-J.; Sheu, C.-F.; Lee, S.; Hsieh, C.-L.; Lin, J.-H. Psychometric Comparisons of 2 Versions of the Fugl-Meyer Motor Scale and 2 Versions of the Stroke Rehabilitation Assessment of Movement. Neurorehabil. Neural Repair 2008, 22, 737–744. [Google Scholar] [CrossRef]
- Hiragami, S.; Inoue, Y.; Harada, K. Minimal clinically important difference for the Fugl-Meyer assessment of the upper extremity in convalescent stroke patients with moderate to severe hemiparesis. J. Phys. Sci. 2019, 31, 917–921. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Layer Name | Parameters |
|---|---|
| Input Layer | Shape = (None, 270, 32, 2) |
| 2D Convolutional Layer 1 | Number of Filters ∈ {25, 50, 100}, Kernel Size ∈ {(2,2), (2,4), (2,6), … (10,8), (10,10)} |
| Max Pooling Layer 1 | Pooling Size = (2, 2) |
| 2D Convolutional Layer 2 | Number of Filters ∈ {25, 50, 100}, Kernel Size = (2, 2) |
| Max Pooling Layer 2 | Pooling Size = (2, 2) |
| Flatten Layer | N/A |
| Dense Layer 1 | Number of neurons = 100 |
| Dropout Layer | Dropout rate∈ {0 to 1 with 0.05 as step size} |
| Dense Layer 2 | Number of neurons = 25 |
| Dense Layer 3 | Number of neurons = 10 |
| Dense Layer 4 | Number of neurons = 5 |
| Output Layer | Number of neurons = 1 |
| ID | Age | Gender | Years after Stroke | Affected Side | MOCA | Handedness before Stroke |
|---|---|---|---|---|---|---|
| P1 | 65 | Male | 7 | Left | 27 | Right |
| P2 | 51 | Female | 7 | Right | 23 | Right |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, X.; D’Arcy, R.; Chen, L.; Xu, M.; Ming, D.; Menon, C. The Feasibility of Longitudinal Upper Extremity Motor Function Assessment Using EEG. Sensors 2020, 20, 5487. https://doi.org/10.3390/s20195487
Zhang X, D’Arcy R, Chen L, Xu M, Ming D, Menon C. The Feasibility of Longitudinal Upper Extremity Motor Function Assessment Using EEG. Sensors. 2020; 20(19):5487. https://doi.org/10.3390/s20195487
Chicago/Turabian StyleZhang, Xin, Ryan D’Arcy, Long Chen, Minpeng Xu, Dong Ming, and Carlo Menon. 2020. "The Feasibility of Longitudinal Upper Extremity Motor Function Assessment Using EEG" Sensors 20, no. 19: 5487. https://doi.org/10.3390/s20195487
APA StyleZhang, X., D’Arcy, R., Chen, L., Xu, M., Ming, D., & Menon, C. (2020). The Feasibility of Longitudinal Upper Extremity Motor Function Assessment Using EEG. Sensors, 20(19), 5487. https://doi.org/10.3390/s20195487