Assessment of Scapulothoracic, Glenohumeral, and Elbow Motion in Adhesive Capsulitis by Means of Inertial Sensor Technology: A Within-Session, Intra-Operator and Inter-Operator Reliability and Agreement Study

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
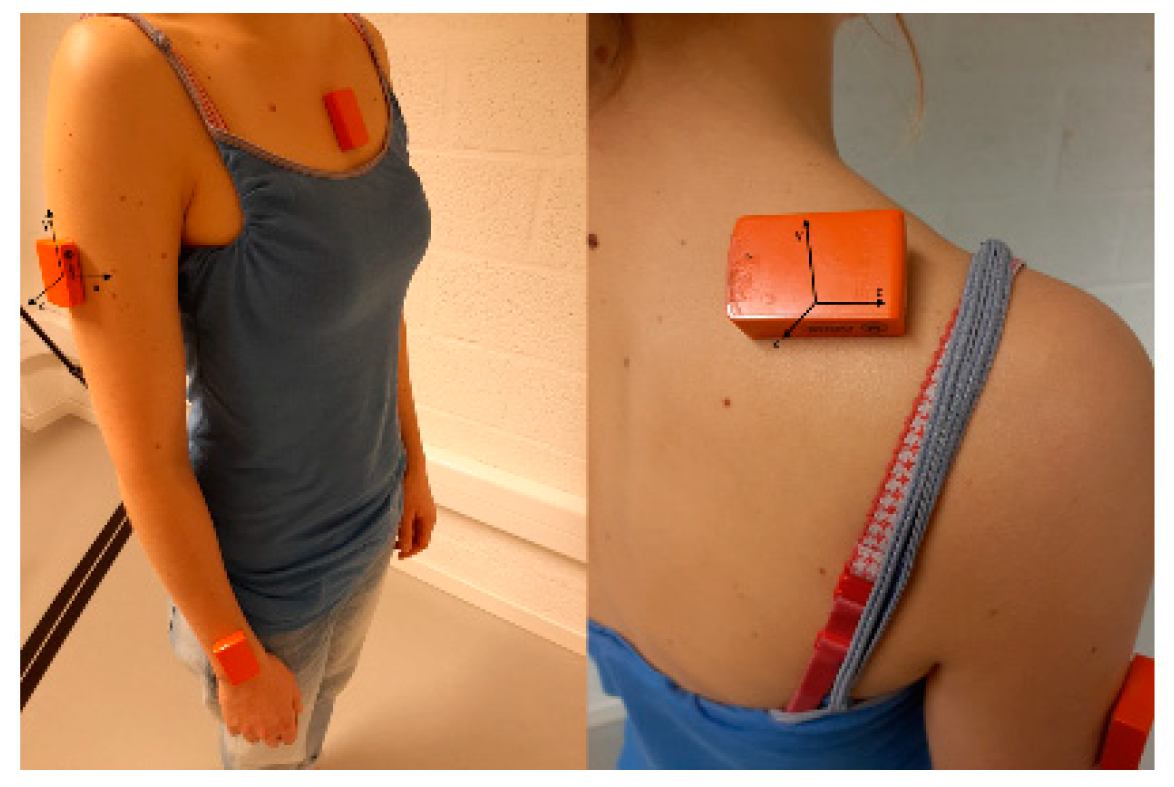
2.2.1. Instrumentation
2.2.2. Motion Analysis Protocol for AC
2.2.3. Data Collection Procedure
2.3. Data Analysis
2.4. Statistical Analysis with Regard to Within-Session, Intra-Operator and Inter-Operator Reliability, and Agreement Assessment
3. Results
3.1. Participants
3.2. Reliability and Agreement
3.2.1. Analytical Glenohumeral External Rotation
3.2.2. Combing Hair
3.2.3. Grasping the Seatbelt
3.2.4. Placing a Cup on an Overhead Shelf
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Le, H.V.; Lee, S.J.; Nazarian, A.; Rodriguez, E.K. Adhesive capsulitis of the shoulder: Review of pathophysiology and current clinical treatments. Shoulder Elb. 2017, 9, 75–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neviaser, A.S.; Neviaser, R.J. Adhesive capsulitis of the shoulder. J. Am. Acad. Orthop. Surg. 2011, 19, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Kelley, M.J.; Shaffer, M.A.; Kuhn, J.E.; Michener, L.A.; Seitz, A.L.; Uhl, T.L.; Godges, J.J.; McClure, P.W. Shoulder pain and mobility deficits: Adhesive capsulitis. J. Orthop. Sports Phys. Ther. 2013, 43, A1–A31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zuckerman, J.D.; Rokito, A. Frozen shoulder: A consensus definition. J. Shoulder Elb. Surg. 2011, 20, 322–325. [Google Scholar] [CrossRef] [PubMed]
- Fayad, F.; Roby-Brami, A.; Gautheron, V.; Lefevre-Colau, M.M.; Hanneton, S.; Fermanian, J.; Poiraudeau, S.; Revel, M. Relationship of glenohumeral elevation and 3-dimensional scapular kinematics with disability in patients with shoulder disorders. J. Rehabil. Med. 2008, 40, 456–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fayad, F.; Roby-Brami, A.; Yazbeck, C.; Hanneton, S.; Lefevre-Colau, M.M.; Gautheron, V.; Poiraudeau, S.; Revel, M. Three-dimensional scapular kinematics and scapulohumeral rhythm in patients with glenohumeral osteoarthritis or frozen shoulder. J. Biomech. 2008, 41, 326–332. [Google Scholar] [CrossRef]
- Hand, C.; Clipsham, K.; Rees, J.L.; Carr, A.J. Long-term outcome of frozen shoulder. J. Shoulder Elb. Surg. 2008, 17, 231–236. [Google Scholar] [CrossRef]
- Manske, R.C.; Prohaska, D. Diagnosis and management of adhesive capsulitis. Curr. Rev. Musculoskelet. Med. 2008, 1, 180–189. [Google Scholar] [CrossRef] [Green Version]
- Struyf, F.; Meeus, M. Current evidence on physical therapy in patients with adhesive capsulitis: What are we missing? Clin. Rheumatol. 2014, 33, 593–600. [Google Scholar] [CrossRef]
- Ertzgaard, P.; Öhberg, F.; Gerdle, B.; Grip, H. A new way of assessing arm function in activity using kinematic Exposure Variation Analysis and portable inertial sensors—A validity study. Man. Ther. 2016, 21, 241–249. [Google Scholar] [CrossRef]
- De Baets, L.; van der Straaten, R.; Matheve, T.; Timmermans, A. Shoulder assessment according to the international classification of functioning by means of inertial sensor technologies: A systematic review. Gait Posture 2017, 57, 278–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weir, J.P. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J. Strength Cond. Res. 2005, 19, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Poitras, I.; Dupuis, F.; Bielmann, M.; Campeau-Lecours, A.; Mercier, C.; Bouyer, L.J.; Roy, J.-S. Validity and Reliability of Wearable Sensors for Joint Angle Estimation: A Systematic Review. Sensors 2019, 19, 1555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parel, I.; Cutti, A.G.; Fiumana, G.; Porcellini, G.; Verni, G.; Accardo, A.P. Ambulatory measurement of the scapulohumeral rhythm: Intra- and inter-operator agreement of a protocol based on inertial and magnetic sensors. Gait Posture 2012, 35, 636–640. [Google Scholar] [CrossRef]
- Parel, I.; Cutti, A.G.; Kraszewski, A.; Verni, G.; Hillstrom, H.; Kontaxis, A. Intra-protocol repeatability and inter-protocol agreement for the analysis of scapulo-humeral coordination. Med. Biol. Eng. Comput. 2014, 52, 271–282. [Google Scholar] [CrossRef]
- Van den Noort, J.C.; Wiertsema, S.H.; Hekman, K.M.; Schonhuth, C.P.; Dekker, J.; Harlaar, J. Measurement of scapular dyskinesis using wireless inertial and magnetic sensors: Importance of scapula calibration. J. Biomech. 2015, 48, 3460–3468. [Google Scholar] [CrossRef]
- Bouvier, B.; Duprey, S.; Claudon, L.; Dumas, R.; Savescu, A. Upper Limb Kinematics Using Inertial and Magnetic Sensors: Comparison of Sensor-to-Segment Calibrations. Sensors 2015, 15, 18813–18833. [Google Scholar] [CrossRef]
- Schiefer, C.; Kraus, T.; Ellegast, R.P.; Ochsmann, E. A technical support tool for joint range of motion determination in functional diagnostics—An inter-rater study. J. Occup. Med. Toxicol. 2015, 10, 16. [Google Scholar] [CrossRef] [Green Version]
- Cutti, A.G.; Giovanardi, A.; Rocchi, L.; Davalli, A.; Sacchetti, R. Ambulatory measurement of shoulder and elbow kinematics through inertial and magnetic sensors. Med. Biol. Eng. Comput. 2008, 46, 169–178. [Google Scholar] [CrossRef]
- Shumway-Cook, A.; Woollacott, M.H. Motor Control: Translating Research into Clinical Practice, 4th ed.; Lippincott Williams And Wilkins: Philadelphia, PA, USA, 2017; p. 656. [Google Scholar]
- Walmsley, S.; Osmotherly, P.G.; Rivett, D.A. Movement and pain patterns in early stage primary/idiopathic adhesive capsulitis: A factor analysis. Physiotherapy 2014, 100, 336–343. [Google Scholar] [CrossRef]
- Wu, G.; van der Helm, F.C.; Veeger, H.E.; Makhsous, M.; Van Roy, P.; Anglin, C.; Nagels, J.; Karduna, A.R.; McQuade, K.; Wang, X.; et al. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion--Part II: Shoulder, elbow, wrist and hand. J. Biomech. 2005, 38, 981–992. [Google Scholar] [CrossRef] [PubMed]
- Shrout, P.E. Measurement reliability and agreement in psychiatry. Stat. Methods Med. Res. 1998, 7, 301–317. [Google Scholar] [CrossRef] [PubMed]
- Magermans, D.J.; Chadwick, E.K.; Veeger, H.E.; van der Helm, F.C. Requirements for upper extremity motions during activities of daily living. Clin. Biomech. 2005, 20, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Van Andel, C.J.; Wolterbeek, N.; Doorenbosch, C.A.; Veeger, D.H.; Harlaar, J. Complete 3D kinematics of upper extremity functional tasks. Gait Posture 2008, 27, 120–127. [Google Scholar] [CrossRef]
- Van den Noort, J.C.; Wiertsema, S.H.; Hekman, K.M.; Schonhuth, C.P.; Dekker, J.; Harlaar, J. Reliability and precision of 3D wireless measurement of scapular kinematics. Med. Biol. Eng. Comput. 2014, 52, 921–931. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Task | Explanation |
|---|---|
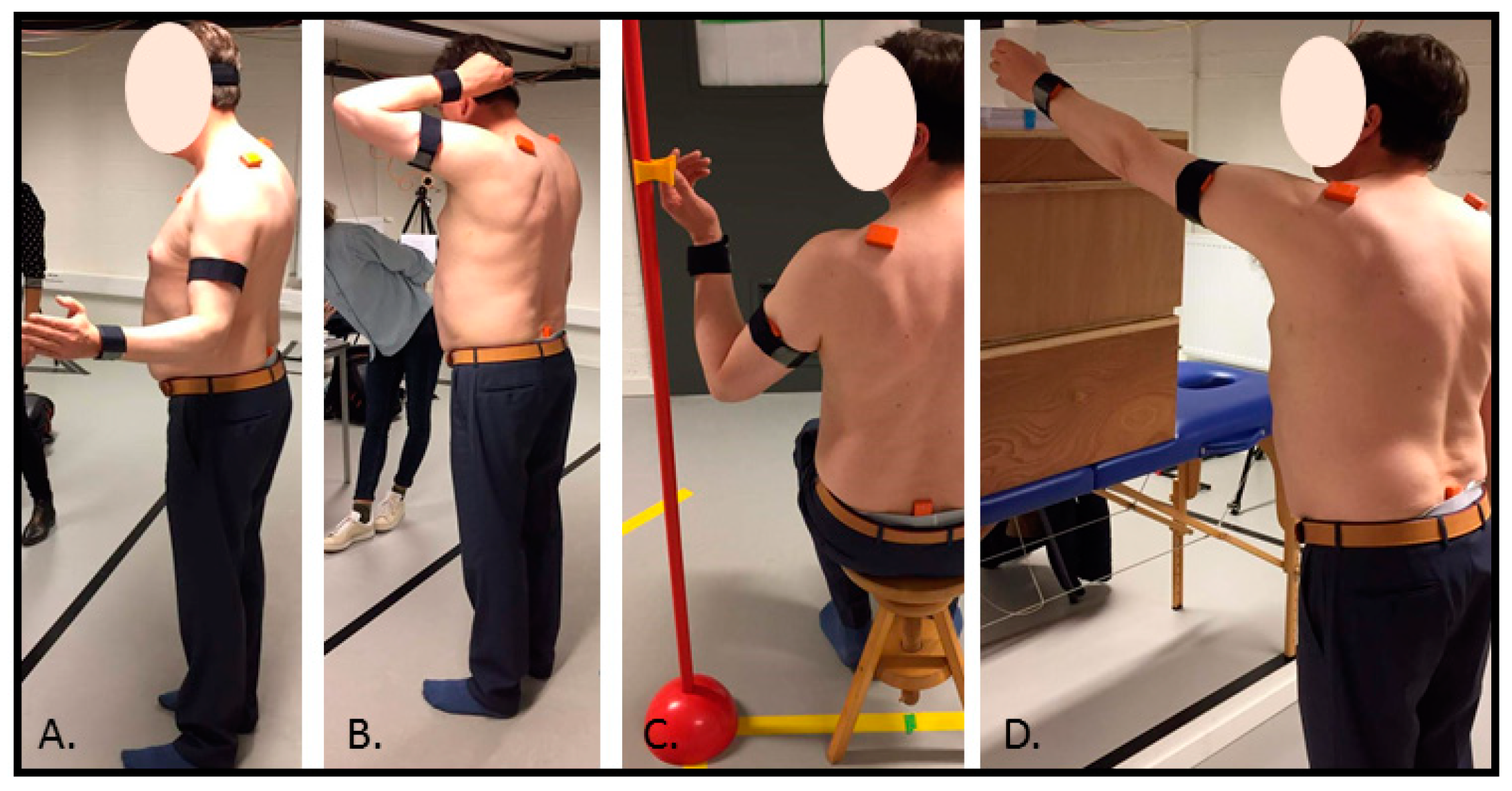
| Analytical GH external rotation | This task started with the test person in standing position, feet at hip width, and the tested arm in a 90° elbow flexion, with the upper arm alongside the body. The person was asked to externally rotate the humerus in the glenohumeral (GH) joint by moving the lower arm outwards. The person was asked not to move the scapula or the thorax. The end position was held for two seconds before going back to the start position. |
| Combing hair | This task started with the test person in standing position, feet at hip width, and the arms alongside the body. In the tested hand, the person held a comb. The person was asked to imitate combing hair, starting from the front of the head. The task ended when the comb was on the back of the head, with the hand palm facing the occiput. The person was asked to hold this end position for 2 s and to return afterwards to the start position. |
| Grasping a seatbelt | This task started with the test person in sitting position on a chair without back support, feet at hip width, knees in a 90° flexion, and hands placed on the thighs. A seatbelt was placed at a standardized distance from the midpoint of the chair (distance between belt and midpoint chair was 110% from the interacromial distance), with a marker at eye level. The person was asked to grab the seatbelt with the ipsilateral thumb and index finger at height of the marker and to hold that position for two second before going back to the start position. |
| Placing a cup on an overhead shelf | This task started with the test person in standing position, feet at hip width, and arms alongside the body. The person held a cup in the tested hand. The height of the shelf and the distance from the standing position to the shelf was adjusted according to the participant’s height (at 93% of the participant’s height) and arm length (distance acromion to the base of the third metacarpal, distance at 115% of arm length), respectively. The task ended when the cup was placed on a marked spot on the shelf. The participant held the arm for 2 s on the endpoint before coming back to the start position. |
| Analytical Ext Rot | Seatbelt | Comb Hair | Cup | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | SEMw | %SEMw | Mean (SD) | SEMw | %SEMw | Mean (SD) | SEMw | %SEMw | Mean (SD) | SEMw | %SEMw | |
| Scapulothoracic | ||||||||||||
| Med-Lat rotation | / | / | / | −6.7 (5.2) | 1.3 | 19.5 | −9.0 (6.9) | 1.2 | 13.0 | −9.5 (5.6) | 1.0 | 10.1 |
| Pro-retraction | 2.4 (2.7) | 0.4 | 17.8 | 3.8 (4.1) | 1.6 | 43.7 | 6.9 (7.3) | 1.1 | 16.1 | −9.0 (7.6) | 2.0 | 21.7 |
| Tilting | / | / | / | −15.5 (9.0) | 1.2 | 7.5 | −25.7 (5.7) | 2.3 | 9.1 | −19.4 (10.4) | 1.9 | 9.8 |
| Glenohumeral | ||||||||||||
| Abd-adduction | / | / | / | −44.3 (14.1) | 2.4 | 5.5 | −69.3 (29.8) | 4.7 | 6.8 | −50.7 (21.6) | 4.3 | 8.4 |
| In-external rotation | 15.1 (6.0) | 2.3 | 15.5 | 60.6 (20.5) | 3.9 | 6.4 | 54.0 (27.0) | 3.7 | 6.8 | 34.2 (23.4) | 5.5 | 16.1 |
| Flexion-extension | / | / | / | −18.9 (14.0) | 4.4 | 23.3 | −54.2 (8.8) | 2.9 | 5.4 | −55.8 (10.9) | 1.0 | 1.8 |
| Elbow | ||||||||||||
| Flexion-extension | / | / | / | −50.0 (17.2) | 4.5 | 9.0 | −143.8 (11.0) | 2.7 | 1.9 | −5.4 (4.5) | 1.6 | 30.6 |
| Intra-Operator Agreement | Inter-Operator Agreement | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | SEM | %SEM | MDC | %MDC | Meandiff | SDdiff | LOA | Mean (SD) | SEM | %SEM | MDC | %MDC | Meandiff | SDdiff | LOA | |
| Analytical Glenohumeral External Rotation | ||||||||||||||||
| Scapulothoracic | ||||||||||||||||
| Pro-retraction | 2.7 (2.8) | 1.0 | 36.0 | 2.7 | 99.7 | −0.6 | 1.2 | 1.7, −3.0 | 3.1 (3.0) | 1.5 | 49.2 | 4.3 | 136.4 | −0.2 | 1.7 | 3.3, −3.7 |
| Glenohumeral | ||||||||||||||||
| Int-external rotation | 15.7 (6.3) | 1.8 | 11.7 | 5.1 | 32.5 | −1.1 | 4.8 | 8.4, −10.7 | 16.6 (6.5) | 4.6 | 27.5 | 12.7 | 76.3 | −0.8 | 8.4 | 16.1, −17.7 |
| Combing Hair | ||||||||||||||||
| Scapulothoracic | ||||||||||||||||
| Med-lat rotation | −9.5 (7.2) | 2.9 | 30.4 | 8.0 | 84.4 | 1.0 | 3.4 | 7.9, −5.9 | −9.8 (7.0) | 0.9 | 9.6 | 2.6 | 26.5 | −0.4 | 1.7 | 3.0, −3.9 |
| Pro-retraction | 5.3 (6.4) | 3.6 | 68.1 | 10.1 | 188.8 | 3.1 | 4.6 | 12.2, −6.0 | 4.4 (5.2) | 1.8 | 40.8 | 5.0 | 113.1 | −1.2 | 3.0 | 4.7, −7.2 |
| Tilting | −25.2 (5.2) | 3.6 | 14.3 | 10.0 | 39.5 | −1.1 | 4.1 | 7.2, −9.4 | −24.2 (5.0) | 6.6 | 27.2 | 18.3 | 75.5 | −0.9 | 7.1 | 13.3, −15.1 |
| Glenohumeral | ||||||||||||||||
| Abd-adduction | −71.7 (29.5) | 9.5 | 13.2 | 26.3 | 36.7 | 5.6 | 12.6 | 30.8, −19.5 | −78.3 (26.3) | 19.1 | 24.5 | 53.1 | 67.8 | 2.3 | 22.1 | 46.5, −41.9 |
| Int-external rotation | 54.7 (27.4) | 16.5 | 30.1 | 45.6 | 83.3 | −2.1 | 19.1 | 36.1, −40.3 | 60.4 (27.0) | 27.8 | 46.0 | 77.0 | 127.5 | −5.6 | 33.2 | 60.9, −72.1 |
| Flexion-extension | −53.0 (9.1) | 5.0 | 9.4 | 13.8 | 26 | −2.3 | 6.2 | 10.0, −14.7 | −54.6 (10.1) | 6.4 | 11.7 | 17.6 | 32.3 | 5.4 | 8.0 | 21.4, −10.6 |
| Elbow | ||||||||||||||||
| Flexion-extension | −144.2 (12.3) | 7.1 | 4.9 | 19.7 | 13.6 | 0.7 | 7.8 | 16.3, −14.8 | 142.2 (15.0) | 4.3 | 11.8 | 11.8 | 8.3 | −4.7 | 12.5 | 20.2, −29.7 |
| Grasping the Seatbelt | ||||||||||||||||
| Scapulothoracic | ||||||||||||||||
| Med-lat rotation | −6.7 (4.8) | 2.0 | 29.9 | 5.6 | 83.0 | 0.1 | 3.4 | 7.0, −6.8 | −6.7 (3.9) | 3.4 | 50.6 | 9.4 | 140.3 | −0.2 | 4.1 | 8.1, −8.5 |
| Pro-retraction | 3.0 (4.5) | 2.2 | 71.7 | 6.0 | 198.6 | 2.4 | 2.5 | 7.5, −2.7 | 2.8 (5.1) | 1.3 | 44.8 | 3.5 | 124.3 | −1.0 | 2.5 | 4.1, −6.07 |
| Tilting | −14.7 (7.5) | 5.1 | 34.7 | 14.1 | 96.1 | −1.5 | 6.1 | 10.7, −13.8 | −15.4 (6.0) | 3.8 | 24.5 | 10.5 | 68.0 | 2.9 | 4.3 | 11.5, −5.8 |
| Glenohumeral | ||||||||||||||||
| Abd-adduction | −47.8 (12.0) | 3.7 | 7.6 | 10.1 | 21.2 | 6.8 | 9.8 | 26.5, −12.8 | −50.8 (9.6) | 4.4 | 8.6 | 12.1 | 23.9 | −0.9 | −0.8 | 11.8, −13.3 |
| Int-external rotation | 61.3 (20.7) | 9.9 | 16.2 | 27.4 | 44.8 | −1.3 | 15.0 | 28.6, −31.4 | 58.0 (21.1) | 13.0 | 22.4 | 36.0 | 62.0 | 7.9 | 17.9 | 43.4, −27.7 |
| Flexion-extension | −17.0 (13.3) | 6.4 | 37.9 | 17.9 | 105.0 | −3.8 | 7.4 | 10.9, −18.6 | −19.0 (11.8) | 7.8 | 41.0 | 21.6 | 113.6 | 4.7 | 9.8 | 24.3, −14.9 |
| Elbow | ||||||||||||||||
| Flexion-extension | −49.8 (16.3) | 4.2 | 8.4 | 11.5 | 23.1 | −0.3 | 11.4 | 22.5, −23.0 | −50.6 (18.3) | 6.8 | 13.4 | 18.7 | 37.0 | 1.8 | 10.6 | 23.0, −19.4 |
| Placing a Cup on an Overhead Shelf | ||||||||||||||||
| Scapulothoracic | ||||||||||||||||
| Med-lat rotation | −9.7 (6.2) | 2.3 | 23.8 | 6.4 | 66.1 | 0.0 | 3.7 | 7.6, −7.0 | −9.9 (6.1) | 3.3 | 33.7 | 9.2 | 93.4 | 0.2 | 3.8 | 7.7, −7.3 |
| Pro-retraction | −10.1 (6.2) | 3.1 | 31.0 | 8.6 | 85.9 | 2.1 | 3.9 | 10.0, −5.8 | −10.5 (5.0) | 1.5 | 14.4 | 4.2 | 39.8 | −1.3 | 2.2 | 3.1, −5.7 |
| Tilting | −18.6 (9.0) | 4.3 | 22.9 | 11.8 | 63.6 | −1.6 | 5.9 | 10.2, −13.5 | −17.4 (7.5) | 3.2 | 18.5 | 8.9 | 51.3 | −0.7 | 3.8 | 6.9, −8.3 |
| Glenohumeral | ||||||||||||||||
| Abd-adduction | −52.3 (20.9) | 6.4 | 12.2 | 17.7 | 33.8 | 3.2 | 8.9 | 20.9, −14.6 | −53.6 (17.6) | 6.1 | 11.3 | 16.9 | 31.4 | −3.3 | 7.5 | 11.6, −18.3 |
| Int-external rotation | 35.4 (21.2) | 11.0 | 31.2 | 30.6 | 86.5 | −2.4 | 13.7 | 25.1, −29.8 | 36.9 (21.0) | 10.2 | 27.7 | 28.3 | 76.7 | −0.7 | 19.1 | 37.4, −38.8 |
| Flexion-extension | −53.8 (11.2) | 9.4 | 17.6 | 26.2 | 48.7 | −4.0 | 11.0 | 18.0, −26.1 | −56.4 (12.9) | 5.4 | 9.5 | 14.8 | 26.3 | 9.2 | 6.7 | 22.6, −4.2 |
| Elbow | ||||||||||||||||
| Flexion-extension | −5.0 (4.0) | 4.3 | 86.2 | 11.8 | 238.8 | −0.3 | 6.2 | 12.2, −12.8 | −3.7 (4.3) | 4.9 | 131.3 | 13.6 | 363.8 | −1.5 | 6.6 | 11.8, −14.8 |
| Analytical Ext Rot | Seatbelt | Comb Hair | Cup | |
|---|---|---|---|---|
| ICCw (95% CI) | ||||
| Scapulothoracic | ||||
| Med-Lat rotation | / | 0.97 (0.92, 0.99) | 0.98 (0.94, 0.99) | 0.97 (0.93, 0.99) |
| Pro-Retraction | 0.89 (0.74, 0.97) | 0.92 (0.90, 0.98) | 0.97 (0.94, 0.99) | 0.96 (0.89, 0.99) |
| Tilting | / | 0.98 (0.95, 0.99) | 0.87 (0.72, 0.96) | 0.97 (0.93, 0.99) |
| Glenohumeral | ||||
| Abd-adduction | / | 0.98 (0.95, 0.99) | 0.98 (0.96, 0.99) | 0.97 (0.91, 0.99) |
| In-external rotation | 0.85 (0.65, 0.96) | 0.98 (0.95, 0.99) | 0.98 (0.96, 0.99) | 0.96 (0.89, 0.99) |
| Flexion-extension | / | 0.96 (0.91, 0.99) | 0.88 (0.71, 0.97) | 0.97 (0.91, 0.99) |
| Elbow | ||||
| Flexion-extension | / | 0.97 (0.92, 0.99) | 0.94 (0.85, 0.98) | 0.90 (0.76, 0.97) |
| Analytical Ext Rot | Seatbelt | Comb Hair | Cup | |
|---|---|---|---|---|
| ICCintra-operator (95% CI) | ||||
| Scapulothoracic | ||||
| Med-Lat rotation | / | 0.87 (0.46, 0.97) | 0.94 (0.78, 0.99) | 0.92 (0.66, 0.98) |
| Pro-Retraction | 0.95 (0.78, 0.99) | 0.82 (0.04, 0.93) | 0.81 (0.23, 0.95) | 0.87 (0.51, 0.97) |
| Tilting | / | 0.82 (0.29, 0.96) | 0.82 (0.31, 0.96) | 0.89 (0.56, 0.97) |
| Glenohumeral | ||||
| Abd-adduction | / | 0.73 (0.02, 0.93) | 0.95 (0.83, 0.99) | 0.95 (0.83, 0.99) |
| In-external rotation | 0.85 (0.35, 0.97) | 0.87 (0.46, 0.97) | 0.89 (0.50, 0.96) | 0.90 (0.59, 0.97) |
| Flexion-extension | / | 0.91 (0.63, 0.98) | 0.87 (0.51, 0.97) | 0.68 (0.00, 0.92) |
| Elbow | ||||
| Flexion-extension | / | 0.88 (0.50, 0.97) | 0.90 (0.60, 0.98) | 0.40 (0.00, 0.85) |
| ICCinter-operator (95% CI) | ||||
| Scapulothoracic | ||||
| Med-Lat rotation | / | 0.24 (0.00, 0.82) | 0.94 (0.75, 0.98) | 0.82 (0.23, 0.96) |
| Pro-Retraction | 0.83 (0.45, 0.96) | 0.91 (0.64, 0.98) | 0.83 (0.39, 0.96) | 0.86 (0.45, 0.97) |
| Tilting | / | 0.87 (0.50, 0.97) | 0.29 (0.00, 0.83) | 0.78 (0.18, 0.95) |
| Glenohumeral | ||||
| Abd-adduction | / | 0.74 (0.05, 0.88) | 0.80 (0.23, 0.96) | 0.93 (0.51, 0.97) |
| Int-external rotation | 0.38 (0.00, 0.87) | 0.84 (0.42, 0.96) | 0.73 (0.00, 0.94) | 0.87 (0.49, 0.97) |
| Flexion-extension | / | 0.74 (0.00, 0.95) | 0.83 (0.37, 0.96) | 0.84 (0.35, 0.96) |
| Elbow | ||||
| Flexion-extension | / | 0.85 (0.38, 0.96) | 0.79 (0.22, 0.95) | 0.84 (0.35, 0.96) |
| The analytical external rotation task is an appropriate task to assess ST pro-retraction and GH in-external rotation. However, thorough task explanation is essential. |
| The combing hair task is an appropriate task in the assessment of ST med-lateral rotation, GH flexion-extension, and elbow flexion-extension. This task is not appropriate for assessing ST pro-retraction and GH in-external rotation. |
| The grasping the seatbelt task is a suitable task for GH ab-adduction, GH in-external rotation, and elbow flexion-extension assessment. In contrast, grasping the seatbelt is not an option when ST pro-retraction, ST med-lateral rotation, or GH flexion-extension is assessed. |
| Placing a cup on an overhead shelf task is in general an appropriate task for all ST and GH joint rotations assessment. Only for elbow flexion-extension, this task does not suit. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Baets, L.; Vanbrabant, S.; Dierickx, C.; van der Straaten, R.; Timmermans, A. Assessment of Scapulothoracic, Glenohumeral, and Elbow Motion in Adhesive Capsulitis by Means of Inertial Sensor Technology: A Within-Session, Intra-Operator and Inter-Operator Reliability and Agreement Study. Sensors 2020, 20, 876. https://doi.org/10.3390/s20030876
De Baets L, Vanbrabant S, Dierickx C, van der Straaten R, Timmermans A. Assessment of Scapulothoracic, Glenohumeral, and Elbow Motion in Adhesive Capsulitis by Means of Inertial Sensor Technology: A Within-Session, Intra-Operator and Inter-Operator Reliability and Agreement Study. Sensors. 2020; 20(3):876. https://doi.org/10.3390/s20030876
Chicago/Turabian StyleDe Baets, Liesbet, Stefanie Vanbrabant, Carl Dierickx, Rob van der Straaten, and Annick Timmermans. 2020. "Assessment of Scapulothoracic, Glenohumeral, and Elbow Motion in Adhesive Capsulitis by Means of Inertial Sensor Technology: A Within-Session, Intra-Operator and Inter-Operator Reliability and Agreement Study" Sensors 20, no. 3: 876. https://doi.org/10.3390/s20030876
APA StyleDe Baets, L., Vanbrabant, S., Dierickx, C., van der Straaten, R., & Timmermans, A. (2020). Assessment of Scapulothoracic, Glenohumeral, and Elbow Motion in Adhesive Capsulitis by Means of Inertial Sensor Technology: A Within-Session, Intra-Operator and Inter-Operator Reliability and Agreement Study. Sensors, 20(3), 876. https://doi.org/10.3390/s20030876