Feasibility of Social-Network-Based eHealth Intervention on the Improvement of Healthy Habits among Children

 ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
- Access to the social network: add friends, comment on different walls, give like to publications, create events and get points in the reward system (bieneSTARS).
- Personalized notifications: the application sends personalized notifications and advice about nutrition and physical activity. This is accomplished by using push notifications available on phones, tables and web browsers, as well as sending emails.
2.3. Measurements
2.3.1. Sociodemographic and Anthropometric Variables
2.3.2. Healthy Nutrition
2.3.3. Physical Activity
2.4. Data Collection
3. Results
3.1. Descriptive Study
Homogeneity of the Control and Intervention Groups
- Interactions: number of sessions initiated in the application throughout the intervention.
- Friends requests: number of friend requests sent, accepted and rejected.
- Posts: number of posts published by users.
- Likes: number of likes received in the different publications.
- Events: number of events created by users.
- Acquired Reward Points: number of reward points acquired through the “bieneSTARS” reward system.
3.2. Statistical Analysis
3.2.1. Individual Study of Intervention and Control Group Results
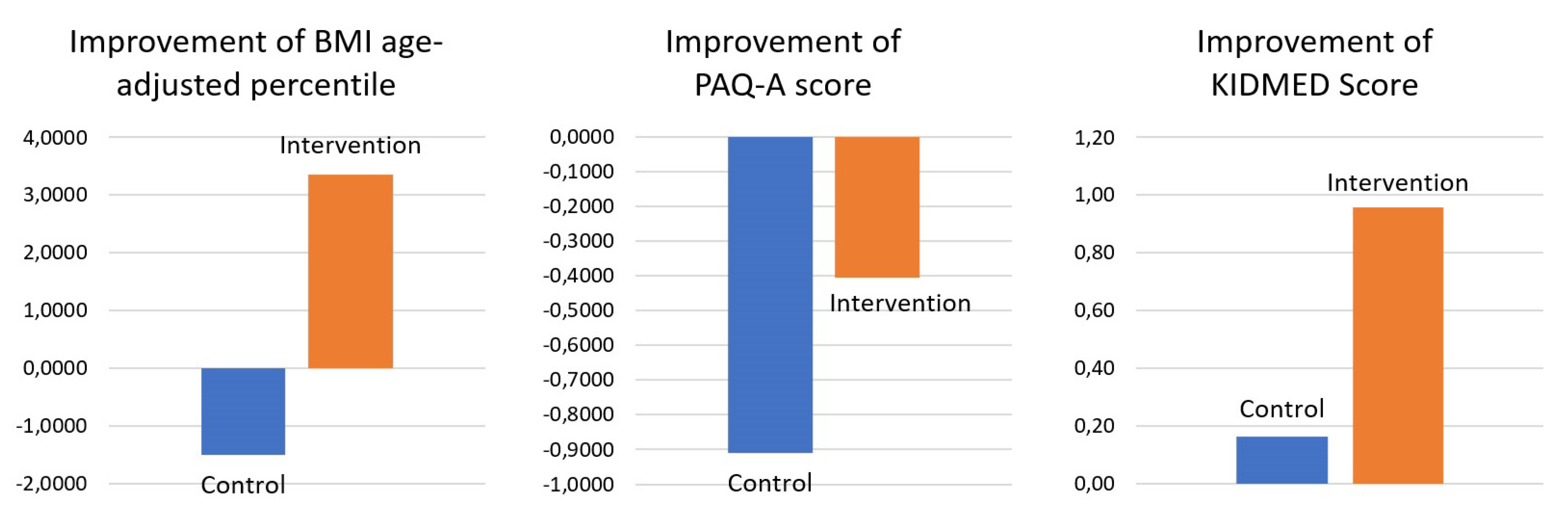
3.2.2. Difference between the Intervention and Control Groups
4. Discussion and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body Mass Index |
| CSE | Compulsory Secondary Education |
| ENSE | National Health Survey |
| F | Female |
| M | Male |
| PAQ-A | Physical Activity Questionnaire for Adolescents |
| RRG | Recognized Research Groups |
| WHO | World Health Organization |
References
- World Health Organization. Taking Action on Childhood Obesity; Technical Report. 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/274792/WHO-NMH-PND-ECHO-18.1-eng.pdf?ua=1 (accessed on 4 March 2020).
- NCD Risk Factor Collaboration. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- Ministerio de Sanidad Consumo y Bienestar Social. Encuesta Nacional de Salud; España 2017—Determinantes de Salud. 2017. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/encuestaNacional/encuesta2017.htm (accessed on 4 March 2020).
- Daniels, S.R. The Consequences of Childhood Overweight and Obesity. Future Child. 2006, 16, 47–67. [Google Scholar] [CrossRef] [PubMed]
- Ul-Haq, Z.; MacKay, D.F.; Fenwick, E.; Pell, J.P. Meta-analysis of the association between body mass index and health-related quality of life among children and adolescents, assessed using the pediatric quality of life inventory index. J. Pediatr. 2013, 162, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.J. Self-Esteem and Health-Related Quality of Life in Childhood Obesity. In Childhood Obesity; Goran, M.I., Ed.; Taylor & Francis: Oxfordshire, UK, 2016; pp. 235–262. [Google Scholar]
- Strauss, R.S.; Pollack, H.A. Social Marginalization of Overweight Children. Arch. Pediatr. Adolesc. Med. 2003, 157, 746. [Google Scholar] [CrossRef]
- Loveman, E.; Colquitt, J.L.; Mead, E.; Johnson, R.E.; Fraser, H.; Olajide, J.; Murphy, M.; Malley, O.C.; Azevedo, L.B.; Ells, L.J.; et al. Diet, physical activity and behavioural interventions for the treatment of overweight or obese adolescents aged 12 to 17 years. Cochrane 2017, 2016, CD012105. [Google Scholar] [CrossRef]
- O’Hara, L.; Gregg, J. The war on obesity: A social determinant of health. Health Promot. J. Aust. 2006, 17, 260–263. [Google Scholar] [CrossRef]
- Brown, T.; Moore, T.H.; Hooper, L.; Gao, Y.; Zayegh, A.; Ijaz, S.; Elwenspoek, M.; Foxen, S.C.; Magee, L.; O’Malley, C.; et al. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2019, CD001871. [Google Scholar] [CrossRef]
- Tong, H.L.; Coiera, E.; Tong, W.; Wang, Y.; Quiroz, J.C.; Martin, P.; Laranjo, L. Efficacy of a mobile social networking intervention in promoting physical activity: Quasi-experimental study. J. Med. Internet Res. 2019, 21, 1–15. [Google Scholar] [CrossRef]
- Byrne, J.L.; Cameron Wild, T.; Maximova, K.; Browne, N.E.; Holt, N.L.; Cave, A.J.; Martz, P.; Ellendt, C.; Ball, G.D. A brief eHealth tool delivered in primary care to help parents prevent childhood obesity: A randomized controlled trial. Pediatr. Obes. 2018, 13, 659–667. [Google Scholar] [CrossRef]
- Lau, Y.; Chee, D.G.H.; Chow, X.P.; Cheng, L.J.; Wong, S.N. Personalised eHealth interventions in adults with overweight and obesity: A systematic review and meta-analysis of randomised controlled trials. Prev. Med. 2020, 132, 106001. [Google Scholar] [CrossRef]
- Thompson, D.; Baranowski, T.; Cullen, K.; Watson, K.; Liu, Y.; Canada, A.; Bhatt, R.; Zakeri, I. Food, fun, and fitness internet program for girls: Pilot evaluation of an e-Health youth obesity prevention program examining predictors of obesity. Prev. Med. 2008, 47, 494–497. [Google Scholar] [CrossRef] [PubMed]
- Asare, M.; Danquah, S.A. The relationship between physical activity, sedentary behaviour and mental health in Ghanaian adolescents. Child Adolesc. Psychiatry Ment. Health 2015, 9, 11. [Google Scholar] [CrossRef] [PubMed]
- Tucker, L.B.; McKay, H.A.; Ward, L.M.; Houghton, K.M.; Rosenberg, A.M.; Feldman, D.E.; Oen, K.; Roth, J.; Stringer, E.; Baxter-Jones, A.; et al. A21: Physical Activity in Children with Juvenile Idiopathic Arthritis (JIA): The LEAP (Linking Exercise, Activity, and Pathophysiology in Childhood Arthritis) Study. Arthritis Rheumatol. 2014, 66, S33–S34. [Google Scholar] [CrossRef]
- Grao-Cruces, A.; Nuviala, A.; Fernández-Martínez, A.; Porcel-Gálvez, A.M.; Moral-García, J.E.; Martínez-López, E.J. Adherencia a la dieta mediterránea en adolescentes rurales y urbanos del sur de España, satisfacción con la vida, antropometría y actividades físicas y sedentarias. Nutr. Hosp. 2013, 28, 1129–1135. [Google Scholar] [CrossRef]
- Mistretta, A.; Marventano, S.; Antoci, M.; Cagnetti, A.; Giogianni, G.; Nolfo, F.; Rametta, S.; Pecora, G.; Marranzano, M. Mediterranean diet adherence and body composition among Southern Italian adolescents. Obes. Res. Clin. Pract. 2017, 11, 215–226. [Google Scholar] [CrossRef]
- Benítez-Andrades, J.A.; Martínez-Martínez, M.; García-Rodríguez, I.; Fernández-San-Juan, C.; Marqués-Sánchez, P. A responsive web application for the alteration of healthy habits in the child population. In Proceedings of the 13th International Joint Conference on Biomedical Engineering Systems and Technologies, Valleta, Malta, 24–26 February 2020; Cabitza, F., Fred, A., Gamboa, H., Eds.; Volume 5, HEALTHINF. pp. 321–328. [Google Scholar]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- World Health Organization. WHO AnthroPlus for Personal Computers Manual: Software for Assessing Growth of the World’s Children and Adolescents. 2009. Available online: https://www.who.int/growthref/tools/who_anthroplus_manual.pdf (accessed on 4 March 2020).
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef]
- Martínez-Gómez, D.; Martínez-de Haro, V.; Pozo, T.; Welk, G.J.; Villagra, A.; Calle, M.E.; Marcos, A.; Veiga, O.L. Reliability and validity of the PAQ-A questionnaire to assess physical activity in Spanish adolescents. Revista Española de Salud Publica 2009, 83, 427–439. [Google Scholar] [CrossRef]
- Chen, S.R.; Lee, Y.J.; Chiu, H.W.; Jeng, C. Impact of physical activity on heart rate variability in children with type 1 diabetes. Child’s Nerv. Syst. 2008, 24, 741–747. [Google Scholar] [CrossRef]
- Benítez, J.A.; Labra, J.E.; Quiroga, E.; Martín, V.; García, I.; Marqués-Sánchez, P.; Benavides, C. A Web-Based Tool for Automatic Data Collection, Curation, and Visualization of Complex Healthcare Survey Studies including Social Network Analysis. Comput. Math. Methods Med. 2017, 2017, 2579848. [Google Scholar] [CrossRef]
- Michie, S.; Ashford, S.; Sniehotta, F.F.; Dombrowski, S.U.; Bishop, A.; French, D.P. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: The CALO-RE taxonomy. Psychol. Health 2011, 26, 1479–1498. [Google Scholar] [CrossRef] [PubMed]
- Champion, K.E.; Parmenter, B.; McGowan, C.; Spring, B.; Wafford, Q.E.; Gardner, L.A.; Thornton, L.; McBride, N.; Barrett, E.L.; Teesson, M.; et al. Effectiveness of school-based eHealth interventions to prevent multiple lifestyle risk behaviours among adolescents: A systematic review and meta-analysis. Lancet Digit. Health 2019, 1, e206–e221. [Google Scholar] [CrossRef]


{kind=link}
| Mean CG | Mean IG | SD CG | SD IG | p | |
|---|---|---|---|---|---|
| Gender | 0.53 | 0.58 | 0.51 | 0.50 | 0.411 |
| Age | 12.77 | 12.63 | 0.62 | 0.59 | 0.081 |
| BMI age-adjusted percentile | 57.12 | 49.68 | 29.15 | 30.4 | 0.067 |
| KIDMED score | 7.31 | 7.06 | 3.24 | 2.50 | 0.522 |
| PAQ-A score | 2.98 | 2.75 | 0.90 | 0.97 | 0.078 |
| Total | Average per User | Average per Day | |
|---|---|---|---|
| Interactions | 7696 | 58.75 | 80.17 |
| Friend requests | 1127 | 8.60 | 11.74 |
| Accepted friend requests | 181 | 1.38 | 1.89 |
| Rejected friend requests | 222 | 1.70 | 2.31 |
| Posts | 3722 | 28.41 | 38.77 |
| Likes | 4727 | 36.08 | 49.24 |
| Events | 107 | 0.82 | 1.12 |
| Acquired Reward Points (BieneSTARS) | 11215 | 85.61 | 116.82 |
| Mean Pre | Mean Post | Median Pre | Median Post | Z | p | ||
|---|---|---|---|---|---|---|---|
| BMI age-adjusted percentile ( >50 initial) | 77.59 | 72.85 | 77.65 | 71.40 | −5.394 | 0.000 | |
| IG | BMI age-adjusted percentile ( <50 initial) | 22.94 | 25.57 | 24.40 | 25.60 | −2.653 | 0.008 |
| PAQ-A Score | 2.75 | 2.35 | 2.90 | 2.84 | −0.666 | 0.505 | |
| KIDMED Score | 7.06 | 8.02 | 8.00 | 9.00 | −5.960 | 0.000 | |
| BMI age-adjusted percentile ( >50 initial) | 78.09 | 77.49 | 82.10 | 81.65 | −0.241 | 0.809 | |
| CG | BMI age-adjusted percentile ( <50 initial) | 26.53 | 24.33 | 27.30 | 21.60 | −2.421 | 0.015 |
| PAQ-A Score | 2.98 | 2.06 | 3.05 | 2.60 | −5.099 | 0.000 | |
| KIDMED Score | 7.31 | 7.47 | 8.00 | 8.00 | −0.482 | 0.630 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benítez-Andrades, J.A.; Arias, N.; García-Ordás, M.T.; Martínez-Martínez, M.; García-Rodríguez, I. Feasibility of Social-Network-Based eHealth Intervention on the Improvement of Healthy Habits among Children. Sensors 2020, 20, 1404. https://doi.org/10.3390/s20051404
Benítez-Andrades JA, Arias N, García-Ordás MT, Martínez-Martínez M, García-Rodríguez I. Feasibility of Social-Network-Based eHealth Intervention on the Improvement of Healthy Habits among Children. Sensors. 2020; 20(5):1404. https://doi.org/10.3390/s20051404
Chicago/Turabian StyleBenítez-Andrades, José Alberto, Natalia Arias, María Teresa García-Ordás, Marta Martínez-Martínez, and Isaías García-Rodríguez. 2020. "Feasibility of Social-Network-Based eHealth Intervention on the Improvement of Healthy Habits among Children" Sensors 20, no. 5: 1404. https://doi.org/10.3390/s20051404
APA StyleBenítez-Andrades, J. A., Arias, N., García-Ordás, M. T., Martínez-Martínez, M., & García-Rodríguez, I. (2020). Feasibility of Social-Network-Based eHealth Intervention on the Improvement of Healthy Habits among Children. Sensors, 20(5), 1404. https://doi.org/10.3390/s20051404