
Kinematic Assessment to Measure Change in Impairment during Active and Active-Assisted Type of Robotic Rehabilitation for Patients with Stroke


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Outcome Measure
2.3.1. Clinical Assessment
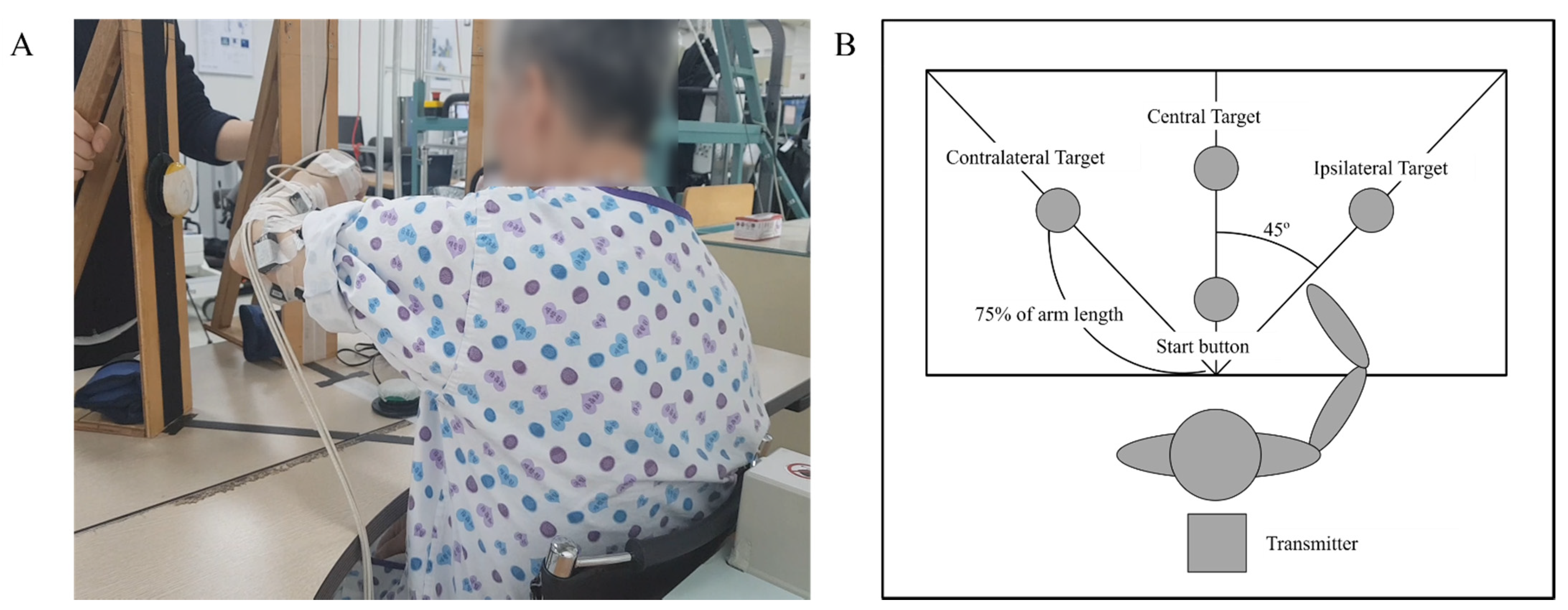
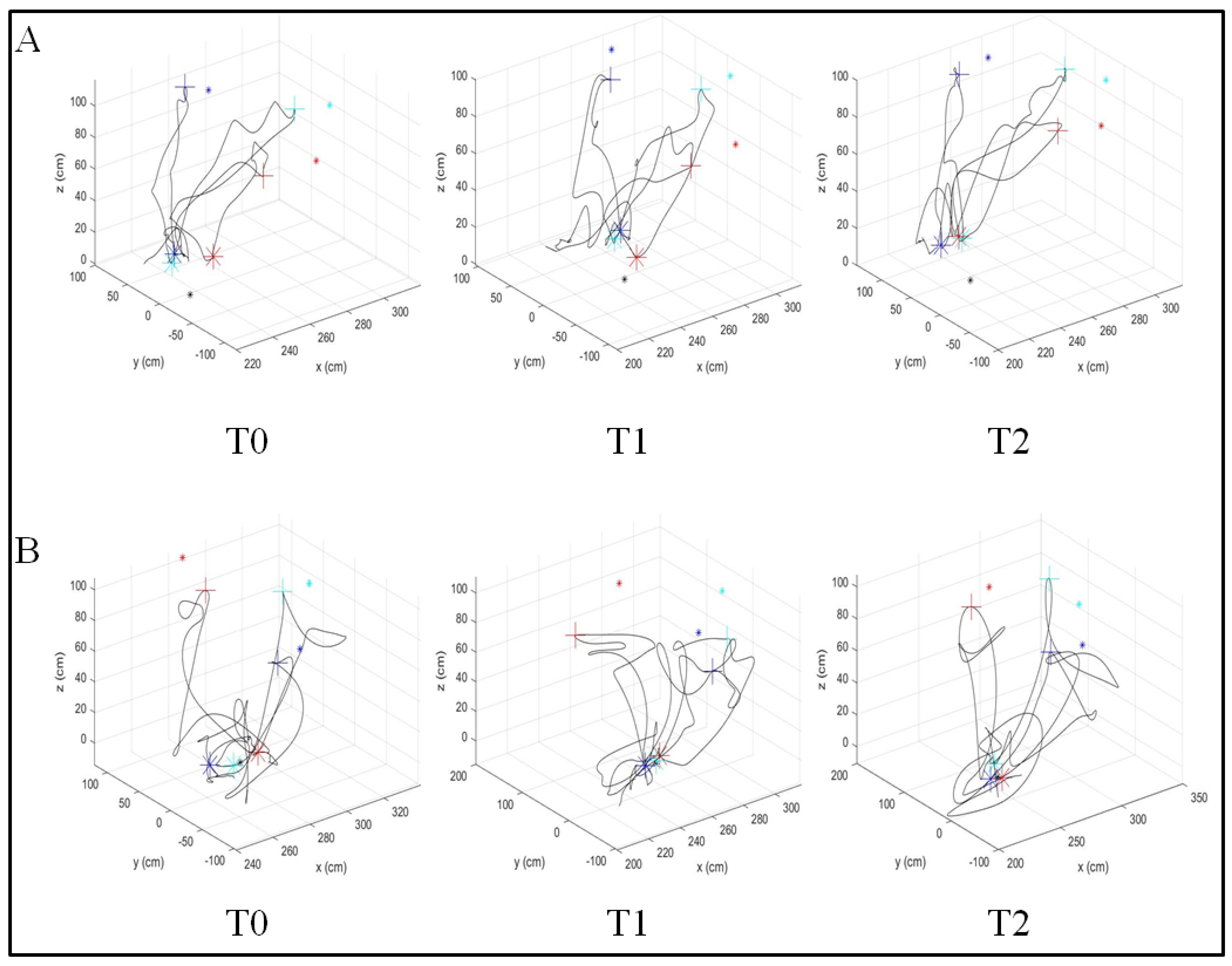
2.3.2. Kinematic Assessment
2.4. Data Analysis
3. Results
3.1. Comparison of Clinical Assessment
3.2. Comparison of Kinematic Assessment
3.3. Regression Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kwakkel, G.; Kollen, B.J.; Van Der Grond, J.; Prevo, A.J. Probability of Regaining Dexterity in the Flaccid Upper Limb. Stroke 2003, 34, 2181–2186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klamroth-Marganska, V.; Blanco, J.; Campen, K.; Curt, A.; Dietz, V.; Ettlin, T.; Felder, M.; Fellinghauer, B.; Guidali, M.; Kollmar, A.; et al. Three-dimensional, task-specific robot therapy of the arm after stroke: A multicentre, parallel-group randomised trial. Lancet Neurol. 2014, 13, 159–166. [Google Scholar] [CrossRef]
- Lo, A.C.; Guarino, P.D.; Richards, L.G.; Haselkorn, J.K.; Wittenberg, G.F.; Federman, D.G.; Ringer, R.J.; Wagner, T.; Krebs, H.I.; Volpe, B.; et al. Robot-Assisted Therapy for Long-Term Upper-Limb Impairment after Stroke. N. Engl. J. Med. 2010, 362, 1772–1783. [Google Scholar] [CrossRef] [Green Version]
- Babaiasl, M.; Mahdioun, S.H.; Jaryani, P.; Yazdani, M. A review of technological and clinical aspects of robot-aided rehabilitation of upper-extremity after stroke. Disabil. Rehabil. Assist. Technol. 2015, 11, 1–18. [Google Scholar] [CrossRef]
- Aprile, I.; Cruciani, A.; Germanotta, M.; Gower, V.; Pecchioli, C.; Cattaneo, D.; Vannetti, F.; Padua, L.; Gramatica, F. Upper Limb Robotics in Rehabilitation: An Approach to Select the Devices, Based on Rehabilitation Aims, and Their Evaluation in a Feasibility Study. Appl. Sci. 2019, 9, 3920. [Google Scholar] [CrossRef] [Green Version]
- Kwakkel, G.; Kollen, B.J.; Krebs, H.I. Effects of Robot-Assisted Therapy on Upper Limb Recovery After Stroke: A Systematic Review. Neurorehabilit. Neural Repair 2007, 22, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Mehrholz, J.; Pohl, M.; Platz, T.; Kugler, J.; Elsner, B. Electromechanical and robot-assisted arm training for improving activities of daily living, arm function, and arm muscle strength after stroke. Cochrane Database Syst. Rev. 2015, 11, CD006876. [Google Scholar] [CrossRef]
- Rech, K.D.; Salazar, A.P.; Marchese, R.; Schifino, G.; Cimolin, V.; Pagnussat, A.S. Fugl-Meyer Assessment Scores Are Related With Kinematic Measures in People with Chronic Hemiparesis after Stroke. J. Stroke Cerebrovasc. Dis. 2020, 29, 104463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brihmat, N.; Loubinoux, I.; Castel-Lacanal, E.; Marque, P.; Gasq, D. Kinematic parameters obtained with the ArmeoSpring for upper-limb assessment after stroke: A reliability and learning effect study for guiding parameter use. J. Neuroeng. Rehabil. 2020, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Cheng, H.; Zhang, J.; Yang, S.; Cai, S. Robot-Assisted Therapy for Upper Extremity Motor Impairment After Stroke: A Systematic Review and Meta-Analysis. Phys. Ther. 2021, 101, pzab010. [Google Scholar] [CrossRef] [PubMed]
- Chien, W.; Chong, Y.; Tse, M.; Chien, C.; Cheng, H. Robot-assisted therapy for upper-limb rehabilitation in subacute stroke patients: A systematic review and meta-analysis. Brain Behav. 2020, 10, e01742. [Google Scholar] [CrossRef] [PubMed]
- Gijbels, D.; Lamers, I.; Kerkhofs, L.; Alders, G.; Knippenberg, E.; Feys, P. The Armeo Spring as training tool to improve upper limb functionality in multiple sclerosis: A pilot study. J. Neuroeng. Rehabil. 2011, 8, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lo, H.S.; Xie, S.Q. Exoskeleton robots for upper-limb rehabilitation: State of the art and future prospects. Med. Eng. Phys. 2012, 34, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Luna, C.O.; Rahman, M.H.; Saad, M.; Archambault, P.S.; Ferrer, S.B. Admittance-Based Upper Limb Robotic Active and Active-Assistive Movements. Int. J. Adv. Robot. Syst. 2015, 12, 117. [Google Scholar] [CrossRef]
- Park, J.H.; Park, G.; Kim, H.Y.; Lee, J.-Y.; Ham, Y.; Hwang, D.; Kwon, S.; Shin, J.-H. A comparison of the effects and usability of two exoskeletal robots with and without robotic actuation for upper extremity rehabilitation among patients with stroke: A single-blinded randomised controlled pilot study. J. Neuroeng. Rehabil. 2020, 17, 137. [Google Scholar] [CrossRef]
- Tran, V.D.; Dario, P.; Mazzoleni, S. Kinematic measures for upper limb robot-assisted therapy following stroke and correlations with clinical outcome measures: A review. Med Eng. Phys. 2018, 53, 13–31. [Google Scholar] [CrossRef] [PubMed]
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. The post-stroke hemiplegic patient. 1. A method for evaluation of physical performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar]
- Duret, C.; Courtial, O.; Grosmaire, A.G. Kinematic measures for upper limb motor assessment during robot-mediated training in patients with severe sub-acute stroke. Restor. Neurol. Neurosci. 2016, 34, 237–245. [Google Scholar] [CrossRef]
- Schwarz, A.; Kanzler, C.M.; Lambercy, O.; Luft, A.R.; Veerbeek, J. Systematic Review on Kinematic Assessments of Upper Limb Movements After Stroke. Stroke 2019, 50, 718–727. [Google Scholar] [CrossRef]
- Nordin, N.; Xie, S.Q.; Wuensche, B. Assessment of movement quality in robot- assisted upper limb rehabilitation after stroke: A review. J. Neuroeng. Rehabil. 2014, 11, 137. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.H.; Park, G.; Cho, D.Y.; Kim, H.Y.; Lee, J.-Y.; Kim, S.; Park, S.-B.; Shin, J.-H. Comparisons between end-effector and exoskeleton rehabilitation robots regarding upper extremity function among chronic stroke patients with moderate-to-severe upper limb impairment. Sci. Rep. 2020, 10, 1806–1808. [Google Scholar] [CrossRef] [PubMed]
- Bertani, R.; Melegari, C.; Maria, C.; Bramanti, A.; Bramanti, P.; Calabrò, R.S. Effects of robot-assisted upper limb rehabilitation in stroke patients: A systematic review with meta-analysis. Neurol. Sci. 2017, 38, 1561–1569. [Google Scholar] [CrossRef] [PubMed]
- Ryf, C.; Weymann, A. The neutral zero method–A principle of measuring joint function. Injury 1995, 26, 1–11. [Google Scholar] [CrossRef]
- Sivan, M.; O’Connor, R.; Makower, S.; Levesley, M.; Bhakta, B. Systematic review of outcome measures used in the evaluation of robot-assisted upper limb exercise in stroke. J. Rehabil. Med. 2011, 43, 181–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gladstone, D.; Danells, C.J.; Black, S. The Fugl-Meyer Assessment of Motor Recovery after Stroke: A Critical Review of Its Measurement Properties. Neurorehabilit. Neural Repair 2002, 16, 232–240. [Google Scholar] [CrossRef]
- Lang, C.E.; Wagner, J.M.; Bastian, A.J.; Hu, Q.; Edwards, D.F.; Sahrmann, S.A.; Dromerick, A.W. Deficits in grasp versus reach during acute hemiparesis. Exp. Brain Res. 2005, 166, 126–136. [Google Scholar] [CrossRef]
- Osu, R.; Ota, K.; Fujiwara, T.; Otaka, Y.; Kawato, M.; Liu, M. Quantifying the quality of hand movement in stroke patients through three-dimensional curvature. J. Neuroeng. Rehabil. 2011, 8, 62. [Google Scholar] [CrossRef] [Green Version]
- Colombo, R.; Pisano, F.; Micera, S.; Mazzone, A.; Delconte, C.; Carrozza, M.; Dario, P.; Minuco, G. Assessing Mechanisms of Recovery During Robot-Aided Neurorehabilitation of the Upper Limb. Neurorehabilit. Neural Repair 2008, 22, 50–63. [Google Scholar] [CrossRef] [PubMed]
- Vergaro, E.; Casadio, M.; Squeri, V.; Giannoni, P.; Morasso, P.; Sanguineti, V. Self-adaptive robot training of stroke survivors for continuous tracking movements. J. Neuroeng. Rehabil. 2010, 7, 13. [Google Scholar] [CrossRef] [Green Version]
- Balasubramanian, S.; Melendez-Calderon, A.; Roby-Brami, A.; Burdet, E. On the analysis of movement smoothness. J. Neuroeng. Rehabil. 2015, 12, 112. [Google Scholar] [CrossRef]
- Culmer, P.R.; Levesley, M.C.; Mon-Williams, M.; Williams, J.H. A new tool for assessing human movement: The Kinematic Assessment Tool. J. Neurosci. Methods 2009, 184, 184–192. [Google Scholar] [CrossRef]
- Field, A. A bluffer’s guide to sphericity. Br. Psychol. Soc. Math. Stat. Comput. Sect. Newsletter 1998, 6, 13–22. [Google Scholar]
- Tukey, J.W. Exploratory Data Analysis; Addison-Wesley: Boston, MA, USA, 1977; Volume 2. [Google Scholar]
- Hocking, R.R. A Biometrics Invited Paper. The Analysis and Selection of Variables in Linear Regression. Biometrics 1976, 32, 1–49. [Google Scholar] [CrossRef]
- Pila, O.; Duret, C.; Gracies, J.-M.; Francisco, G.E.; Bayle, N.; Hutin, E. Evolution of upper limb kinematics four years after subacute robot-assisted rehabilitation in stroke patients. Int. J. Neurosci. 2018, 128, 1030–1039. [Google Scholar] [CrossRef] [PubMed]
- Trombly, C.A.; Wu, C.-Y. Effect of Rehabilitation Tasks on Organization of Movement After Stroke. Am. J. Occup. Ther. 1999, 53, 333–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reyes-Guzmán, A.D.L.; Gil-Agudo, A.; Peñasco-Martín, B.; Solís-Mozos, M.; Del Ama-Espinosa, A.; Pérez-Rizo, E. Kinematic analysis of the daily activity of drinking from a glass in a population with cervical spinal cord injury. J. Neuroeng. Rehabil. 2010, 7, 41–52. [Google Scholar] [CrossRef] [Green Version]
- Reyes-Guzmán, A.D.L.; Dimbwadyo-Terrer, I.; Trincado-Alonso, F.; Monasterio-Huelin, F.; Torricelli, D.; Gil-Agudo, A. Quantitative assessment based on kinematic measures of functional impairments during upper extremity movements: A review. Clin. Biomech. 2014, 29, 719–727. [Google Scholar] [CrossRef] [Green Version]
- van Dokkum, L.; Hauret, I.; Mottet, D.; Froger, J.; Métrot, J.; Laffont, I. The Contribution of Kinematics in the Assessment of Upper Limb Motor Recovery Early After Stroke. Neurorehabilit. Neural Repair 2014, 28, 4–12. [Google Scholar] [CrossRef]
- Hussain, N.; Sunnerhagen, K.S.; Murphy, M.A. End-point kinematics using virtual reality explaining upper limb impairment and activity capacity in stroke. J. Neuroeng. Rehabil. 2019, 16, 82. [Google Scholar] [CrossRef]
- Park, M.; Ko, M.-H.; Oh, S.-W.; Lee, J.-Y.; Ham, Y.; Yi, H.; Choi, Y.; Ha, D.; Shin, J.-H. Effects of virtual reality-based planar motion exercises on upper extremity function, range of motion, and health-related quality of life: A multicenter, single-blinded, randomized, controlled pilot study. J. Neuroeng. Rehabil. 2019, 16, 122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rohrer, B.; Fasoli, S.; Krebs, H.I.; Hughes, R.; Volpe, B.; Frontera, W.R.; Stein, J.; Hogan, N. Movement Smoothness Changes during Stroke Recovery. J. Neurosci. 2002, 22, 8297–8304. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Kinematic Features | Abbreviation | Unit | Description | Characteristic |
|---|---|---|---|---|
| Max Speed | MaxSp | mm/s | the fastest speed in each speed profile during each movement the higher values are related to a faster movement | Movement Speed |
| Mean Speed | MeanSp | mm/s | the average of the motion speeds of each speed profile during each movement the higher values are related to a faster movement | |
| Hand Path Ratio | HPR | dimensionless | the ratio between the actual distance to the desired distance in a single movement between the starting point and the target point [26,27] the higher values are related to a longer hand trajectory during the movement. | Movement Efficiency |
| Movement Deviation | MD | mm | the mean absolute value of the vertical distance from the theoretical path to each point on the real path [28] ※ the lower values indicate that the real path is similar to the desired path | Movement Accuracy |
| Target Error | TEr | mm | the minimum distance from the index finger to the target location at the end of the movement as intended by the subject [26] ※ the lower values indicate that the target has been reached | |
| Ration between Mean and Maximum Speed | RMMS | % | the ratio of the mean to the maximum speed the value of a healthy subject should be close to one | Movement Smoothness |
| Mean Arrest Period Ratio | MAPR | % | the ratio of the movement time in which the hand stopped to the total movement time. The arrested hand was defined to have less than 20% of the average speed during each movement [29] the lower values are related to a more continuous movement | |
| SPARC | SPARC | dimensionless | the amplitude and Fourier magnitude spectrum from the velocity profile of the hand movement [30] the lower values indicate that there is more sub-movement in the movement | |
| Time to Peak Speed | TPeakSp | s | the time from the start of the movement to the maximum speed during the movement [31] the lower values indicate that the maximum speed of movement is reached faster | Movement Control Strategy |
| Demographic Data and Clinical Characteristics | ACT Group (n = 7) | ACAS Group (n = 8) |
|---|---|---|
| Age | 51.11 ± 14.85 | 53.60 ± 11.23 |
| Time after stroke onset (months) | 9.38 ± 5.79 | 9.60 ± 5.79 |
| Stroke type (infarction/hemorrhage) | 3/4 | 3/5 |
| Hemiplegic side, right | 4 | 4 |
| Sex, male | 6 | 6 |
| FMA-prox | 22.71 ± 5.94 | 21.00 ± 4.96 |
| FMA-UE | 31.29 ± 10.00 | 28.63 ± 11.44 |
| Variable | ACT Group (n = 7) | ACAS Group (n = 8) | Time | Time × Group | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T0 | T1 | T2 | F | p-Value | F | p-Value | |
| FMA-UE | 31.30 ± 10.00 | 34.10 ± 11.60 | 35.30 ± 9.00 | 24.70 ± 3.10 | 27.40 ± 4.80 | 27.70 ± 2.10 | 4.383 | 0.025 | 0.094 | 0.907 |
| FMA-prox | 22.70 ± 5.90 | 24.30 ± 6.80 | 26.00 ± 6.00 | 19.40 ± 2.40 | 21.00 ± 3.00 | 22.30 ± 1.90 | 8.475 | 0.003 | 0.055 | 0.921 |
| MaxSp (mm/s) | 3.55 ± 1.60 | 3.85 ± 1.92 | 3.59 ± 1.50 | 2.94 ± 1.03 | 3.51 ± 0.87 | 4.25 ± 1.07 †,‡ | 9.369 | 0.001 | 9.163 | 0.001 |
| MeanSp (mm/s) | 1.13 ± 0.60 | 1.41 ± 0.78 | 1.46 ± 0.63 † | 1.06 ± 0.51 | 1.21 ± 0.34 | 1.62 ± 0.46 †,‡ | 33.842 | <0.001 | 5.516 | 0.022 |
| HPR | 0.92 ± 0.23 | 0.89 ± 0.25 | 0.95 ± 0.16 | 0.93 ± 0.15 | 0.87 ± 0.13 | 0.88 ± 0.10 | 0.916 | 0.407 | 0.646 | 0.521 |
| MD (mm) | 81.61 ± 7.20 | 76.84 ± 20.69 | 71.29 ± 19.46 | 80.80 ± 21.96 | 77.61 ± 11.91 | 76.43 ± 13.58 | 1.956 | 0.188 | 0.741 | 0.499 |
| TEr (mm) | 30.72 ± 14.83 | 29.56 ± 18.21 | 30.89 ± 20.59 | 37.22 ± 12.77 | 33.14 ± 10.70 | 28.42 ± 7.30 | 1.1013 | 0.364 | 1.120 | 0.343 |
| RMMS (%) | 0.31 ± 0.05 | 0.35 ± 0.08 | 0.41 ± 0.08 †,‡ | 0.36 ± 0.06 | 0.36 ± 0.06 | 0.39 ± 0.04 | 7.793 | 0.004 | 2.340 | 0.128 |
| MAPR (%) | 0.10 ± 0.06 | 0.10 ± 0.07 | 0.09 ± 0.07 | 0.08 ± 0.04 | 0.07 ± 0.04 | 0.07 ± 0.04 | 0.721 | 0.475 | 0.440 | 0.615 |
| SPARC | −8.57 ± 1.01 | −8.63 ± 1.88 | −7.26 ± 1.06 † | −9.91 ± 2.21 | −8.84 ± 1.87 | −7.91 ± 1.70 †,‡ | 15.177 | 0.001 | 0.371 | 0.699 |
| TPeakSp (s) | 0.60 ± 0.22 | 0.60 ± 0.23 | 0.53 ± 0.23 | 0.67 ± 0.25 | 0.59 ± 0.21 | 0.50 ± 0.16 ‡ | 2.125 | 0.154 | 0.398 | 0.630 |
| ACT Group (n = 7) | ACAS Group (n = 8) | |||||
|---|---|---|---|---|---|---|
| Independent Variables | Unstandardized B | Adjusted R2 | p-Value | Unstandardized B | Adjusted R2 | p-Value |
| MaxSp | 3.664 | 0.337 | <0.001 | 3.278 | 0.173 | <0.001 |
| MeanSp | 8.232 | 0.290 | <0.001 | 0.638 | −0.005 | 0.721 |
| HPR | −21.655 | 0.166 | <0.001 | −7.203 | 0.008 | 0.119 |
| MD | 0.008 | −0.006 | 0.800 | 0.016 | −0.004 | 0.612 |
| TEr | −0.494 | 0.522 | <0.001 | −0.538 | 0.364 | <0.001 |
| RMMS | 12.629 | 0.011 | 0.104 | −39.030 | 0.134 | <0.001 |
| MAPR | 22.386 | 0.058 | 0.002 | 59.103 | 0.228 | <0.001 |
| SPARC | 0.430 | 0.008 | 0.136 | 0.066 | −0.006 | 0.832 |
| TPeakSp | −6.459 | 0.058 | 0.002 | −10.652 | 0.123 | <0.001 |
| ACT Group (n = 7) | ACAS Group (n = 8) | |||||
|---|---|---|---|---|---|---|
| Independent Variables | Unstandardized B | Adjusted R2 | p-Value | Unstandardized B | Adjusted R2 | p-Value |
| MaxSp | 2.486 | 0.495 | <0.001 | 1.106 | 0.124 | <0.001 |
| MeanSp | 6.126 | 0.514 | <0.001 | −0.039 | −0.006 | 0.956 |
| HPR | −12.488 | 0.176 | <0.001 | −2.099 | 0.002 | 0.247 |
| MD | 0.001 | −0.007 | 0.973 | −0.003 | −0.005 | 0.805 |
| TEr | −0.200 | 0.268 | <0.001 | −0.204 | 0.340 | <0.001 |
| RMMS | 12.345 | 0.046 | 0.004 | −13.161 | 0.098 | <0.001 |
| MAPR | 9.107 | 0.027 | 0.023 | 20.227 | 0.172 | <0.001 |
| SPARC | 0.226 | 0.006 | 0.164 | 0.111 | −0.001 | 0.834 |
| TPeakSp | −3.425 | 0.051 | 0.003 | −4.796 | 0.164 | <0.001 |
| ACT Group (n = 7) | ACAS Group (n = 8) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Kinematic Characteristic | Selected Variables | Unstandardized B | Adjusted R2 | p-Value | Kinematic Characteristic | Selected Variables | Unstandardized B | Adjusted R2 | p-Value |
| Speed | MaxSp | 2.384 | 0.648 | <0.001 | Speed | MaxSp | 1.107 | 0.599 | <0.001 |
| Efficiency | - | - | Efficiency | - | - | ||||
| Accuracy | TEr | −0.405 | Accuracy | TEr | −0.360 | ||||
| Smoothness | - | - | Smoothness | RMMS | −14.479 | ||||
| MAPR | 35.345 | ||||||||
| SPARC | −0.532 | ||||||||
| Control strategy | - | - | Control strategy | TPeakSp | −8.889 | ||||
| ACT Group (n = 7) | ACAS Group (n = 8) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Kinematic Characteristic | Selected Variables | Unstandardized B | Adjusted R2 | p-Value | Kinematic Characteristic | Selected Variables | Unstandardized B | Adjusted R2 | p-Value |
| Speed | MeanSp | 5.663 | 0.677 | <0.001 | Speed | - | - | 0.542 | <0.001 |
| Efficiency | HPR | −3.551 | Efficiency | - | - | ||||
| Accuracy | TEr | −0.073 | Accuracy | TEr | −0.127 | ||||
| Smoothness | MAPR | 12.874 | Smoothness | RMMS | −8.773 | ||||
| MAPR | 11.550 | ||||||||
| Control strategy | Control strategy | TPeakSp | −1.173 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, D.; Shin, J.-H.; Kwon, S. Kinematic Assessment to Measure Change in Impairment during Active and Active-Assisted Type of Robotic Rehabilitation for Patients with Stroke. Sensors 2021, 21, 7055. https://doi.org/10.3390/s21217055
Hwang D, Shin J-H, Kwon S. Kinematic Assessment to Measure Change in Impairment during Active and Active-Assisted Type of Robotic Rehabilitation for Patients with Stroke. Sensors. 2021; 21(21):7055. https://doi.org/10.3390/s21217055
Chicago/Turabian StyleHwang, Donghwan, Joon-Ho Shin, and Suncheol Kwon. 2021. "Kinematic Assessment to Measure Change in Impairment during Active and Active-Assisted Type of Robotic Rehabilitation for Patients with Stroke" Sensors 21, no. 21: 7055. https://doi.org/10.3390/s21217055
APA StyleHwang, D., Shin, J.-H., & Kwon, S. (2021). Kinematic Assessment to Measure Change in Impairment during Active and Active-Assisted Type of Robotic Rehabilitation for Patients with Stroke. Sensors, 21(21), 7055. https://doi.org/10.3390/s21217055