
Optical Coherence Tomography for Patients with Developmental Disabilities: A Preliminary Study


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Material and Methods
2.1. Participant Recruitment and Consent
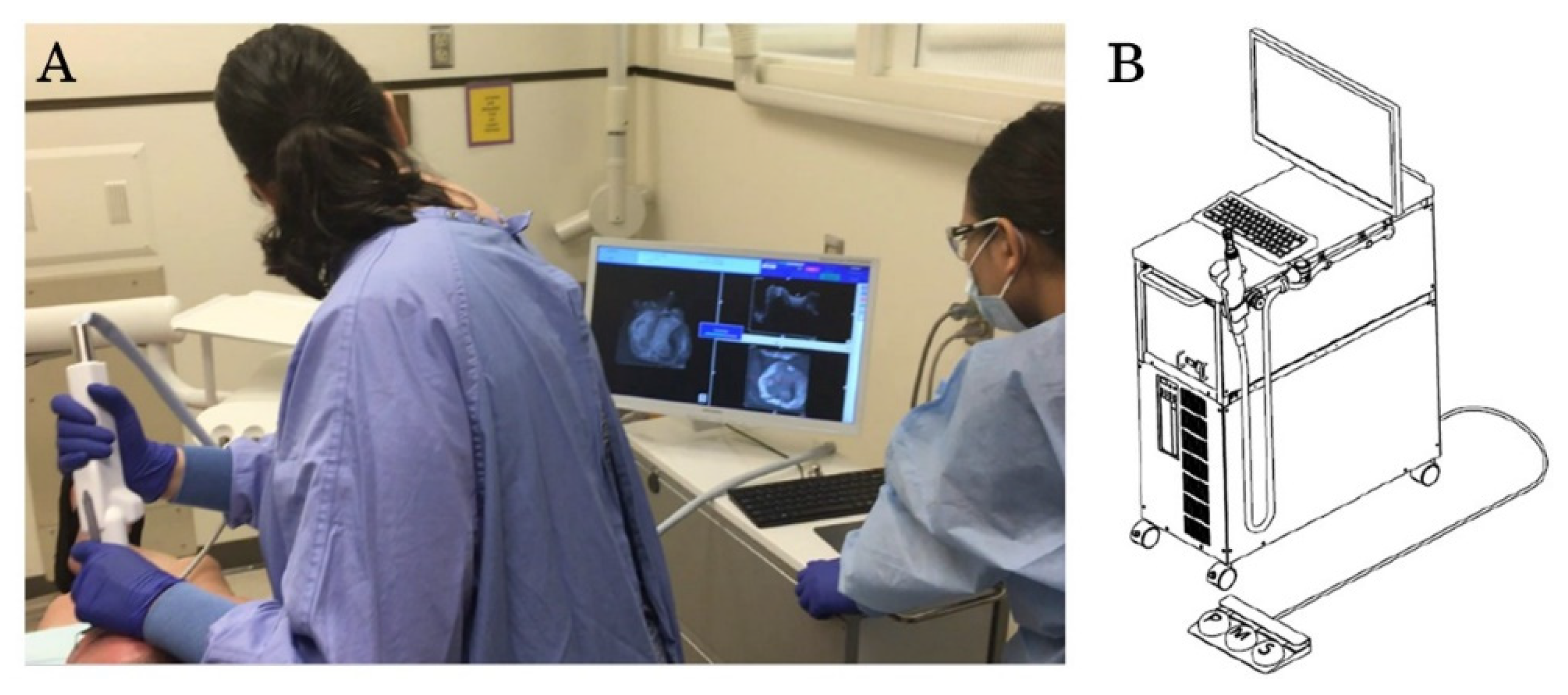
2.2. OCT Imaging Process
2.3. Data Collection and Analysis
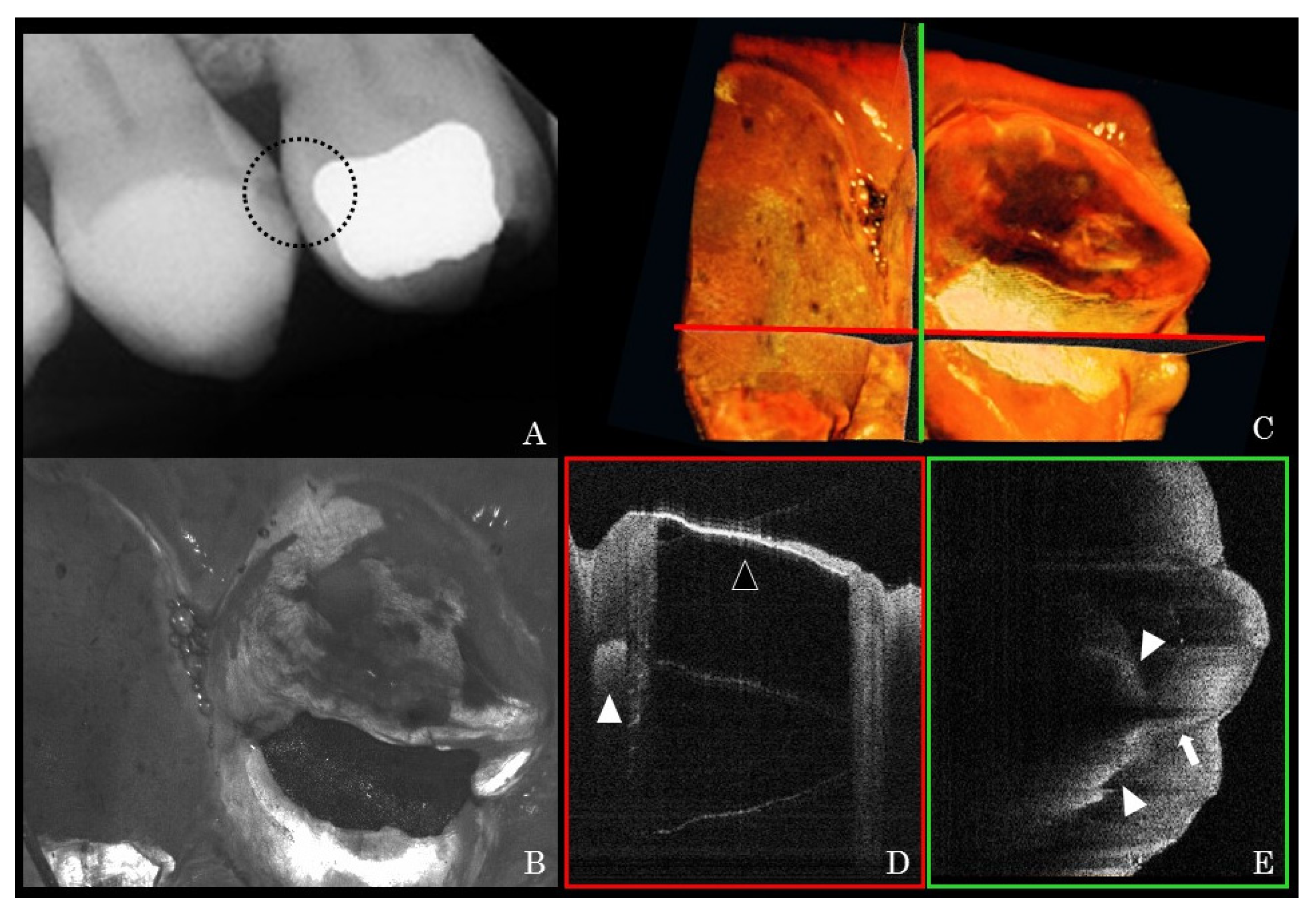
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Martin, M.D.; Kinoshita-Byrne, J.; Getz, T. Dental fear in a special needs clinic population of persons with disabilities. Spéc. Care Dent. 2002, 22, 99–102. [Google Scholar] [CrossRef]
- Gordon, S.M.; Dionne, R.A.; Snyder, J. Dental fear and anxiety as a barrier to accessing oral health care among patients with special health care needs. Spéc. Care Dent. 1998, 18, 88–92. [Google Scholar] [CrossRef]
- Leal TA, C.; Silva, A.M.; Nogueira, B.R.; Prado Júnior, R.R.; Ferreira, M.C.; Mendes, R.F. Physiologic and behavioural signs during a dental appointment in children and teenagers with Cerebral Palsy: A comparative cross-sectional study. Eur. Arch. Paediatr Dent. 2021, 22, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Stein, L.I.; Polido, J.C.; Mailloux, Z.; Coleman, G.G.; Cermak, S.A. Oral care and sensory sensitivities in children with autism spectrum disorders. Spéc. Care Dent. 2011, 31, 102–110. [Google Scholar] [CrossRef]
- Salmasi, A.; Harrison, R.; Brondani, M.A. They stole her teeth! An exploration of adults with developmental disability experiences with dental care. Spéc. Care Dent. 2015, 35, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Nelson, L.P.; Getzin, A.; Graham, D.; Zhou, J.; Wagle, E.M.; McQuiston, J.; McLaughlin, S.; Govind, A.; Sadof, M.; Huntington, N.L. Unmet dental needs and barriers to care for children with significant special health care needs. Pediatr. Dent. 2011, 33, 29–36. [Google Scholar]
- Hsieh, K.; Scott, H.M.; Murthy, S. Associated Risk Factors for Depression and Anxiety in Adults with Intellectual and Developmental Disabilities: Five-Year Follow Up. Am. J. Intellect. Dev. Disabil. 2020, 125, 49–63. [Google Scholar] [CrossRef] [PubMed]
- Klingberg, G.; Broberg, A.G. Dental fear/anxiety and dental behaviour management problems in children and adolescents: A review of prevalence and concomitant psychological factors. Int. J. Paediatr. Dent. 2007, 17, 391–406. [Google Scholar] [CrossRef]
- Ozdemir, S.; Parlakyıldız Gokce, A.; Unver, T. Simulation of three intraoral radiographic techniques in pediatric dental patients: Subjective comfort assessment using the VAS and Wong-Baker FACES Pain Raiting Scale. BMC Oral Health. 2020, 20, 33. [Google Scholar] [CrossRef]
- Pitts, N.B.; Hamood, S.S.; Longbottom, C.; Rimmer, P.A. The use of bitewing positioning devices in children’s dentistry. Dentomaxillofac. Radiol. 1991, 20, 121–126. [Google Scholar] [CrossRef]
- Ghanei, M.; Arnrup, K.; Robertson, A. Procedural pain in routine dental care for children: A part of the Swedish BITA study. Eur. Arch. Paediatr. Dent. 2018, 19, 365–372. [Google Scholar] [CrossRef] [Green Version]
- Novaes, T.; Matos, R.; Raggio, D.; Imparato, J.; Braga, M.; Mendes, F. Influence of the Discomfort Reported by Children on the Performance of Approximal Caries Detection Methods. Caries Res. 2010, 44, 465–471. [Google Scholar] [CrossRef]
- Farman, A.; Horsley, B.; Warr, E.; Ianke, J.; Hood, H. Outcomes of digital X-ray mini-panel examinations for patients having mental retardation and developmental disability. Dentomaxillofac. Radiol. 2003, 32, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, A. The use of lateral oblique radiographs in dental treatment planning for patients with special needs. J. Disabil. Oral. Health. 2016, 17, 154–158. [Google Scholar]
- Peltier, B. Psychological treatment of fearful and phobic special needs patients. Spéc. Care Dent. 2009, 29, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Wilson, N.J.; Lin, Z.; Villarosa, A.; Lewis, P.; Philip, P.; Sumar, B.; George, A. Countering the poor oral health of people with intellectual and developmental disability: A scoping literature review. BMC Public Health 2019, 19, 1530. [Google Scholar] [CrossRef]
- Glassman, P.; Caputo, A.; Dougherty, N.; Lyons, R.; Messieha, Z.; Miller, C.; Peltier, B.; Romer, M. Special Care Dentistry Association consensus statement on sedation, anesthesia, and alternative techniques for people with special needs. Spéc. Care Dent. 2009, 29, 2–8. [Google Scholar] [CrossRef]
- Waldman, H.B.; Perlman, S.P. Ensuring oral health for older individuals with intellectual and developmental disabilities. J. Clin. Nurs. 2012, 21, 909–913. [Google Scholar] [CrossRef]
- Chen, H.-Y.; Yang, H.; Chi, H.-J. Physiologic and behavioral effects of papoose board on anxiety in dental patients with special needs. J. Formos. Med. Assoc. 2014, 113, 94–101. [Google Scholar] [CrossRef] [Green Version]
- Americans with Disabilities Act: Title II Regulations 217. Available online: https://www.ada.gov/ada_title_II.htm (accessed on 15 November 2020).
- Americans with Disabilities Act: Title III Regulations 267. Available online: https://www.ada.gov/ada_title_III.htm (accessed on 15 November 2020).
- ADA Access to Medical Care for Individuals with Mobility Disabilities. Available online: https://www.ada.gov/medcare_mobility_ta/medcare_ta.htm (accessed on 15 November 2020).
- Washington Administrative Code WAC 246-225A-020. Available online: https://app.leg.wa.gov/wac/default.aspx?cite=246-225A-020 (accessed on 15 November 2020).
- Radiation Control Law, Health and Safety Code. Available online: https://www.vmb.ca.gov/laws_regs/rad_laws.pdf (accessed on 15 November 2020).
- Chauhan, V.; Wilkins, R.C. A comprehensive review of the literature on the biological effects from dental X-ray exposures. Int. J. Radiat. Biol. 2019, 95, 107–119. [Google Scholar] [CrossRef] [Green Version]
- McGiff, T.J.; Danforth, R.A.; Herschaft, E.E. Maintaining Radiation Exposures as Low As Reasonably Achievable (ALARA) for Dental Personnel Operating Portable Hand-Held X-ray Equipment. Health Phys. 2012, 103, S179–S185. [Google Scholar] [CrossRef]
- Mupparapu, M.; Nadeau, C. Oral and Maxillofacial Imaging. Dent. Clin. N. Am. 2016, 60, 1–37. [Google Scholar] [CrossRef]
- Gomez, J.L. Detection and diagnosis of the early caries lesion. BMC Oral Health 2015, 15, S3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimada, Y.; Sadr, A.; Sumi, Y.; Tagami, J. Application of Optical Coherence Tomography (OCT) for Diagnosis of Caries, Cracks, and Defects of Restorations. Curr. Oral Health Rep. 2015, 2, 73–80. [Google Scholar] [CrossRef] [Green Version]
- Ueno, T.; Shimada, Y.; Matin, K.; Zhou, Y.; Wada, I.; Sadr, A.; Sumi, Y.; Tagami, J. Optical analysis of enamel and dentin caries in relation to mineral density using swept-source optical coherence tomography. J. Med. Imaging 2016, 3, 035507. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, J.; Espigares, J.; Takagaki, T.; Shimada, Y.; Tagami, J.; Numata, T.; Chan, D.; Sadr, A. Real-time in-depth imaging of gap formation in bulk-fill resin composites. Dent. Mater. 2019, 35, 585–596. [Google Scholar] [CrossRef]
- Fried, D.; Featherstone, J.D.; Darling, C.L.; Jones, R.S.; Ngaotheppitak, P.; Bühler, C.M. Early Caries Imaging and Monitoring with Near-Infrared Light. Dent. Clin. N. Am. 2005, 49, 771–793. [Google Scholar] [CrossRef] [PubMed]
- Luong, M.N.; Shimada, Y.; Araki, K.; Yoshiyama, M.; Tagami, J.; Sadr, A. Diagnosis of Occlusal Caries with Dynamic Slicing of 3D Optical Coherence Tomography Images. Sensors 2020, 20, 1659. [Google Scholar] [CrossRef] [Green Version]
- Shimada, Y.; Nakagawa, H.; Sadr, A.; Wada, I.; Nakajima, M.; Nikaido, T.; Otsuki, M.; Tagami, J.; Sumi, Y. Noninvasive cross-sectional imaging of proximal caries using swept-source optical coherence tomography (SS-OCT) in vivo. J. Biophotonics 2014, 7, 506–513. [Google Scholar] [CrossRef]
- Nakagawa, H.; Sadr, A.; Shimada, Y.; Tagami, J.; Sumi, Y. Validation of swept source optical coherence tomography (SS-OCT) for the diagnosis of smooth surface caries in vitro. J. Dent. 2013, 41, 80–89. [Google Scholar] [CrossRef]
- Kitasako, Y.; Sadr, A.; Shimada, Y.; Ikeda, M.; Sumi, Y.; Tagami, J. Remineralization capacity of carious and non-carious white spot lesions: Clinical evaluation using ICDAS and SS-OCT. Clin. Oral Investig. 2019, 23, 863–872. [Google Scholar] [CrossRef] [PubMed]
- Sugiura, M.; Kitasako, Y.; Sadr, A.; Shimada, Y.; Sumi, Y.; Tagami, J. White spot lesion remineralization by sugar-free chewing gum containing bio-available calcium and fluoride: A double-blind randomized controlled trial. J. Dent. 2016, 54, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Espigares, J.; Sadr, A.; Hamba, H.; Shimada, Y.; Otsuki, M.; Tagami, J.; Sumi, Y. Assessment of natural enamel lesions with optical coherence tomography in comparison with microfocus x-ray computed tomography. J. Med. Imaging 2015, 2, 14001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlsson, L. Caries Detection Methods Based on Changes in Optical Properties between Healthy and Carious Tissue. Int. J. Dent. 2010, 2010, 270729. [Google Scholar] [CrossRef] [Green Version]
- Zain, E.; Zakian, C.; Chew, H. Influence of the loci of non-cavitated fissure caries on its detection with optical coherence tomography. J. Dent. 2018, 71, 31–37. [Google Scholar] [CrossRef]
- Zaitsev, V.; Matveyev, A.L.; Matveev, L.A.; Gelikonov, G.V.; Baum, O.I.; Omelchenko, A.I.; Shabanov, D.V.; Sovetsky, A.A.; Yuzhakov, A.V.; Fedorov, A.A.; et al. Revealing structural modifications in thermomechanical reshaping of collagenous tissues using optical coherence elastography. J. Biophotonics 2019, 12, e201800250. [Google Scholar] [CrossRef]
- Van Hilsen, Z.; Jones, R.S. Comparing potential early caries assessment methods for teledentistry. BMC Oral Health 2013, 13, 16. [Google Scholar] [CrossRef] [Green Version]
- Reed, M.D.; Van Nostran, W. Assessing pain intensity with the visual analog scale: A plea for uniformity. J. Clin. Pharmacol. 2014, 54, 241–244. [Google Scholar] [CrossRef]
- Garra, G.; Singer, A.J.; Taira, B.; Chohan, J.; Cardoz, H.; Chisena, E.; Thode, H.C. Validation of the Wong-Baker FACES Pain Rating Scale in Pediatric Emergency Department Patients. Acad. Emerg. Med. 2010, 17, 50–54. [Google Scholar] [CrossRef]
- Finlay, W.M.L.; Lyons, E. Acquiescence in Interviews with People Who Have Mental Retardation. Ment. Retard. 2002, 40, 14–29. [Google Scholar] [CrossRef]
- Gabre, P.; Sjöquist, K. Experience and assessment of pain in individuals with cognitive impairments. Spéc. Care Dent. 2003, 22, 174–180. [Google Scholar] [CrossRef]
- Racine, N.M.; Riddell, R.R.P.; Khan, M.; Calic, M.; Taddio, A.; Tablon, P. Systematic Review: Predisposing, Precipitating, Perpetuating, and Present Factors Predicting Anticipatory Distress to Painful Medical Procedures in Children. J. Pediatr. Psychol. 2016, 41, 159–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gedney, J.J.; Logan, H.; Baron, R.S. Predictors of short-term and long-term memory of sensory and affective dimensions of pain. J. Pain 2003, 4, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Redelmeier, D.A.; Katz, J.; Kahneman, D. Memories of colonoscopy: A randomized trial. Pain 2003, 104, 187–194. [Google Scholar] [CrossRef] [Green Version]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Espinoza, K.; Hayashi, J.; Shimada, Y.; Tagami, J.; Sadr, A. Optical Coherence Tomography for Patients with Developmental Disabilities: A Preliminary Study. Sensors 2021, 21, 7940. https://doi.org/10.3390/s21237940
Espinoza K, Hayashi J, Shimada Y, Tagami J, Sadr A. Optical Coherence Tomography for Patients with Developmental Disabilities: A Preliminary Study. Sensors. 2021; 21(23):7940. https://doi.org/10.3390/s21237940
Chicago/Turabian StyleEspinoza, Kimberly, Juri Hayashi, Yasushi Shimada, Junji Tagami, and Alireza Sadr. 2021. "Optical Coherence Tomography for Patients with Developmental Disabilities: A Preliminary Study" Sensors 21, no. 23: 7940. https://doi.org/10.3390/s21237940