
Managing Vibration Training Safety by Using Knee Flexion Angle and Rating Perceived Exertion

 ,
,
Abstract
:1. Introduction
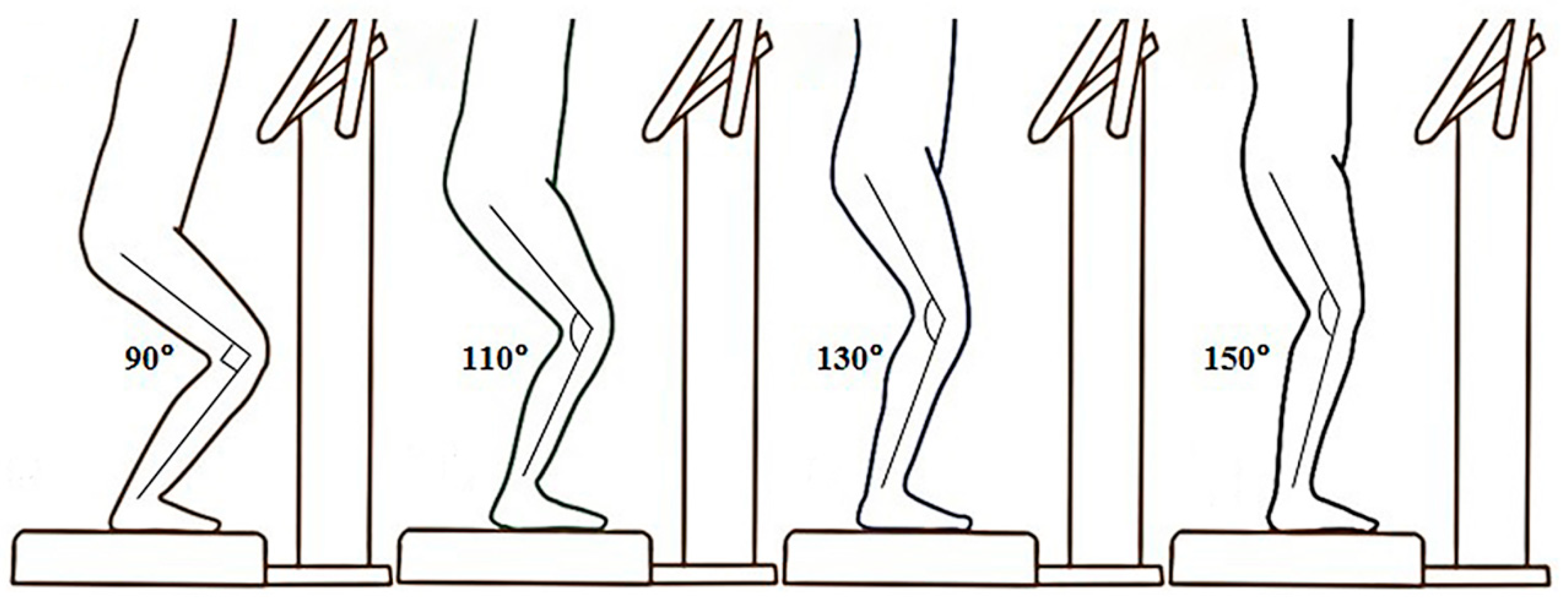
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Costantino, C.; Bertuletti, S.; Romiti, D. Efficacy of whole-body vibration board training on strength in athletes after anterior cruciate ligament reconstruction: A randomized controlled study. Clin. J. Sport Med. 2018, 28, 339–349. [Google Scholar] [CrossRef]
- Yang, W.W.; Chou, L.W.; Chen, W.H.; Shiang, T.Y.; Liu, C. Dual-frequency whole body vibration enhances vertical jumping and change-of-direction ability in rugby players. J. Sport Health Sci. 2017, 6, 346–351. [Google Scholar] [CrossRef] [Green Version]
- Pamukoff, D.N.; Montgomery, M.M.; Choe, K.H.; Moffit, T.J.; Vakula, M.N. Effect of Whole-Body Vibration on Sagittal Plane Running Mechanics in Individuals With Anterior Cruciate Ligament Reconstruction: A Randomized Crossover Trial. Arch. Phys. Med. Rehabil. 2018, 99, 973–980. [Google Scholar] [CrossRef]
- Zafar, H.; Alghadir, A.; Anwer, S.; Al-Eisa, E. Therapeutic effects of whole-body vibration training in knee osteoarthritis: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2015, 96, 1525–1532. [Google Scholar] [CrossRef]
- Luo, J.; McNamara, B.; Moran, K. The use of vibration training to enhance muscle strength and power. Sports Med. 2005, 35, 23–41. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Liu, C.; Chuang, L.R.; Chung, P.H.; Shiang, T.Y. Chronic effects of whole-body vibration on jumping performance and body balance using different frequencies and amplitudes with identical acceleration load. J. Sci. Med. Sport 2014, 17, 107–112. [Google Scholar] [CrossRef]
- Cardinale, M.; Bosco, C. The use of vibration as an exercise intervention. Exerc. Sport Sci. Rev. 2003, 31, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Savage, R.; Billing, D.; Furnell, A.; Netto, K.; Aisbett, B. Whole-body vibration and occupational physical performance: A review. Int. Arch. Occup. Environ. Health 2016, 89, 181–197. [Google Scholar] [CrossRef] [PubMed]
- Guglielmino, C.; Musumeci, G. Early elbow osteoarthritis in competitive enduro motorcyclist. Scand. J. Med. Sci. Sports 2020, 30, 1287–1290. [Google Scholar] [CrossRef] [PubMed]
- Musumeci, G.; Loreto, C.; Leonardi, R.; Castorina, S.; Giunta, S.; Carnazza, M.L.; Trovato, F.M.; Pichler, K.; Weinberg, A.M. The effects of physical activity on apoptosis and lubricin expression in articular cartilage in rats with glucocorticoid-induced osteoporosis. J. Bone Miner. Metab. 2013, 31, 274–284. [Google Scholar] [CrossRef]
- Ishitake, T.; Ando, H.; Miyazaki, Y.; Matoba, F. Changes of visual performance induced by exposure to whole-body vibration. Kurume Med. J. 1998, 45, 59–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, J.-G.; Zhang, L.-l.; Agresti, M.; Yan, Y.; LoGiudice, J.; Sanger, J.R.; Matloub, H.S.; Pritchard, K.A., Jr.; Jaradeh, S.S.; Havlik, R. Cumulative brain injury from motor vehicle-induced whole-body vibration and prevention by human Apolipoprotein AI molecule mimetic (4F) peptide (an Apo AI mimetic). J. Stroke Cerebrovasc. Dis. 2015, 24, 2759–2773. [Google Scholar] [CrossRef] [Green Version]
- Amir, I.; Young, E.; Belloso, A. Self-limiting benign paroxysmal positional vertigo following use of whole-body vibration training plate. J. Laryngol. Otol. 2010, 124, 796–798. [Google Scholar] [CrossRef]
- Ljungberg, J.; Neely, G.; Lundström, R. Cognitive performance and subjective experience during combined exposures to whole-body vibration and noise. Int. Arch. Occup. Environ. Health 2004, 77, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Carlsöö, S. The effect of vibration on the skeleton, joints and muscles: A review of the literature. Appl. Ergon. 1982, 13, 251–258. [Google Scholar] [CrossRef]
- Kiiski, J.; Heinonen, A.; Järvinen, T.L.; Kannus, P.; Sievänen, H. Transmission of vertical whole body vibration to the human body. J. Bone Miner. Res. 2008, 23, 1318–1325. [Google Scholar] [CrossRef] [Green Version]
- International Organization for Standardization (ISO). Mechanical Vibration and Shock: Evaluation of Human Exposure to Whole-Body Vibration. In Part 1: Mechanical Vibration and Shock. Evaluation of Human Exposure to Whole-Body Vibration. General Requirements; International Organization for Standardization: Geneva, Switzerland, 1997. [Google Scholar]
- Muir, J.; Kiel, D.P.; Rubin, C.T. Safety and severity of accelerations delivered from whole body vibration exercise devices to standing adults. J. Sci. Med. Sport 2013, 16, 526–531. [Google Scholar] [CrossRef] [Green Version]
- Perchthaler, D.; Horstmann, T.; Grau, S. Variations in neuromuscular activity of thigh muscles during whole-body vibration in consideration of different biomechanical variables. J. Sports Sci. Med. 2013, 12, 439–446. [Google Scholar]
- Ritzmann, R.; Gollhofer, A.; Kramer, A. The influence of vibration type, frequency, body position and additional load on the neuromuscular activity during whole body vibration. Eur. J. Appl. Physiol. 2013, 113, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Munera, M.; Bertucci, W.; Duc, S.; Chiementin, X. Transmission of whole body vibration to the lower body in static and dynamic half-squat exercises. Sports Biomech. 2016, 15, 409–428. [Google Scholar] [CrossRef]
- Lienhard, K.; Vienneau, J.; Friesenbichler, B.; Nigg, S.; Meste, O.; Nigg, B.M.; Colson, S.S. The effect of whole-body vibration on muscle activity in active and inactive subjects. Int. J. Sports Med. 2015, 36, 585–591. [Google Scholar] [CrossRef]
- Avelar, N.C.; Ribeiro, V.G.; Mezencio, B.; Fonseca, S.F.; Tossige-Gomes, R.; da Costa, S.J.; Szmuchrowski, L.; Gripp, F.; Coimbra, C.C.; Lacerda, A.C. Influence of the knee flexion on muscle activation and transmissibility during whole body vibration. J. Electromyogr. Kinesiol. 2013, 23, 844–850. [Google Scholar] [CrossRef]
- Cochrane, D.J.; Loram, I.D.; Stannard, S.R.; Rittweger, J. Changes in joint angle, muscle-tendon complex length, muscle contractile tissue displacement, and modulation of EMG activity during acute whole-body vibration. Muscle Nerve 2009, 40, 420–429. [Google Scholar] [CrossRef] [PubMed]
- Nawayseh, N. Transmission of vibration from a vibrating plate to the head of standing people. Sports Biomech. 2019, 18, 482–500. [Google Scholar] [CrossRef]
- Caryn, R.C.; Hazell, T.J.; Dickey, J.P. Transmission of acceleration from a synchronous vibration exercise platform to the head. Int. J. Sports Med. 2014, 35, 330–338. [Google Scholar] [CrossRef] [Green Version]
- Tankisheva, E.; Jonkers, I.; Boonen, S.; Delecluse, C.; van Lenthe, G.H.; Druyts, H.L.; Spaepen, P.; Verschueren, S.M. Transmission of whole-body vibration and its effect on muscle activation. J. Strength Cond. Res. 2013, 27, 2533–2541. [Google Scholar] [CrossRef]
- Wakeling, J.M.; Nigg, B.M.; Rozitis, A.I. Muscle activity damps the soft tissue resonance that occurs in response to pulsed and continuous vibrations. J. Appl. Physiol. 2002, 93, 1093–1103. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.C.; Rymer, W.Z. Damping in reflexively active and areflexive lengthening muscle evaluated with inertial loads. J. Neurophysiol. 1998, 80, 3369–3372. [Google Scholar] [CrossRef] [PubMed]
- Burke, D.; Hagbarth, K.E.; Löfstedt, L.; Wallin, B.G. The responses of human muscle spindle endings to vibration of non-contracting muscles. J. Physiol. 1976, 261, 673–693. [Google Scholar] [CrossRef] [PubMed]
- Cristi, C.; Collado, P.S.; Marquez, S.; Garatachea, N.; Cuevas, M.J. Whole-body vibration training increases physical fitness measures without alteration of inflammatory markers in older adults. Eur. J. Sport Sci. 2014, 14, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Marin, P.J.; Santos-Lozano, A.; Santin-Medeiros, F.; Delecluse, C.; Garatachea, N. A comparison of training intensity between whole-body vibration and conventional squat exercise. J. Electromyogr. Kinesiol. 2011, 21, 616–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertucci, W.; Arfaoui, A.; Duc, S.; Letellier, T.; Brikci, A. Effect of whole body vibration in energy expenditure and perceived exertion during intense squat exercise. Acta Bioeng. Biomech. 2015, 17, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Paddan, G.; Griffin, M. The transmission of translational seat vibration to the head--I. vertical seat vibration. J. Biomech. 1988, 21, 191–197. [Google Scholar] [CrossRef]
- Borg, G. Borg’s Perceived Exertion and Pain Scales; Human Kinetics: Champaign, IL, USA, 1998. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 1988. [Google Scholar]
- Sonza, A.; Volkel, N.; Zaro, M.A.; Achaval, M.; Hennig, E.M. A whole body vibration perception map and associated acceleration loads at the lower leg, hip and head. Med. Eng. Phys. 2015, 37, 642–649. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Knee Angle Condition | 90 Degrees | 110 Degrees | 130 Degrees | 150 Degrees | F Value |
|---|---|---|---|---|---|
| Head transmissibility | 0.46 ± 0.12 | 0.32 ± 0.08 | 0.47 ± 0.07 | 0.76 ± 0.14 | 43.93 1 |
| Knee transmissibility | 1.86 ± 0.51 | 1.61 ± 0.51 | 1.38 ± 0.41 | 1.47 ± 0.33 | 6.77 1 |
| Rating of perceived exertion | 2.8 ± 1.0 | 2.3 ± 0.9 | 3.1 ± 1.1 | 4.3 ± 1.6 | 13.84 1 |
| Transmissibility | RPE | |||
|---|---|---|---|---|
| 90 Degrees | 110 Degrees | 130 Degrees | 150 Degrees | |
| Head | 0.145 | 0.069 | −0.136 | 0.508 1 |
| Knee | 0.025 | −0.129 | 0.040 | 0.127 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chuang, L.-R.; Yang, W.-W.; Chang, P.-L.; Chen, V.C.-F.; Liu, C.; Shiang, T.-Y. Managing Vibration Training Safety by Using Knee Flexion Angle and Rating Perceived Exertion. Sensors 2021, 21, 1158. https://doi.org/10.3390/s21041158
Chuang L-R, Yang W-W, Chang P-L, Chen VC-F, Liu C, Shiang T-Y. Managing Vibration Training Safety by Using Knee Flexion Angle and Rating Perceived Exertion. Sensors. 2021; 21(4):1158. https://doi.org/10.3390/s21041158
Chicago/Turabian StyleChuang, Long-Ren, Wen-Wen Yang, Po-Ling Chang, Vincent Chiun-Fan Chen, Chiang Liu, and Tzyy-Yuang Shiang. 2021. "Managing Vibration Training Safety by Using Knee Flexion Angle and Rating Perceived Exertion" Sensors 21, no. 4: 1158. https://doi.org/10.3390/s21041158