
Noninvasive Measurement of Tongue Pressure and Its Correlation with Swallowing and Respiration


Abstract
1. Introduction
2. Materials and Method
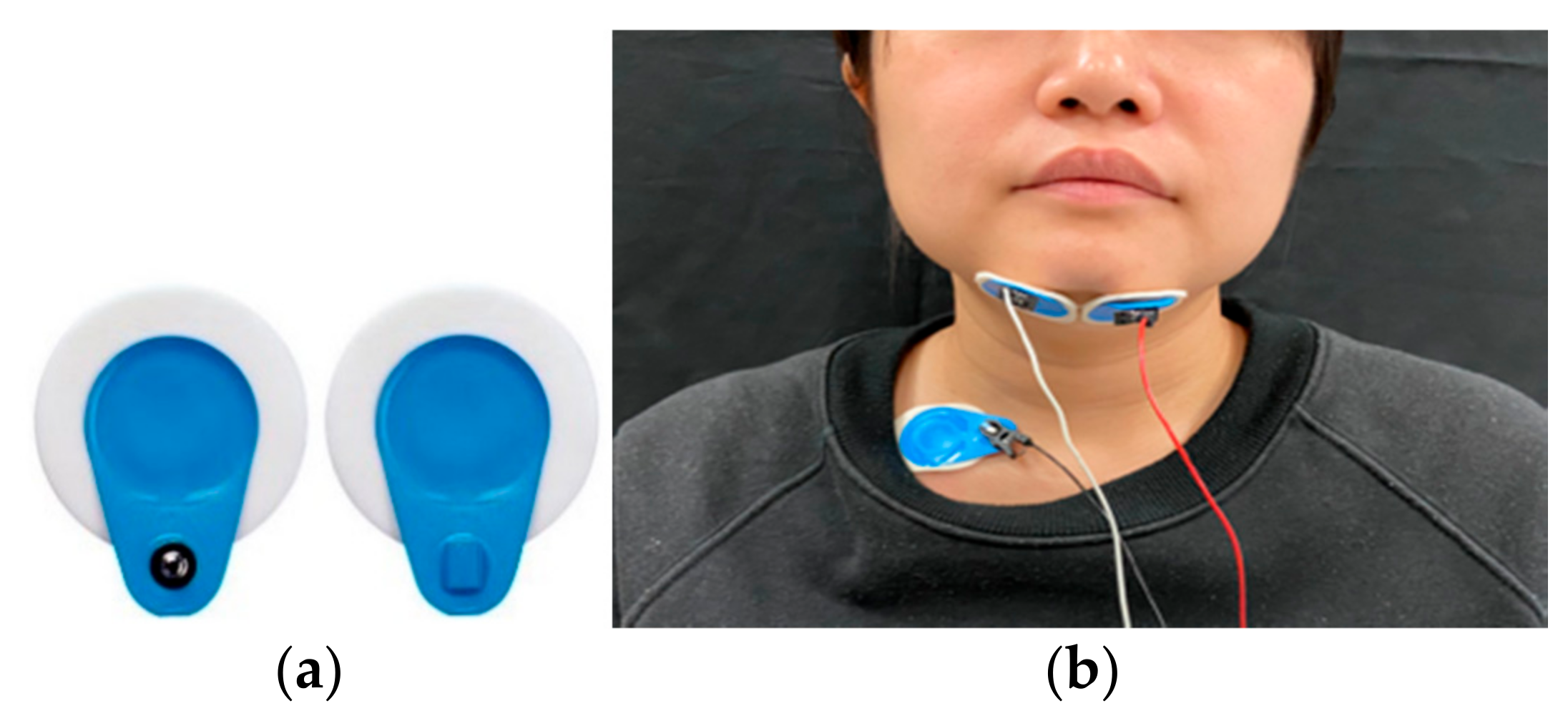
2.1. Sensors
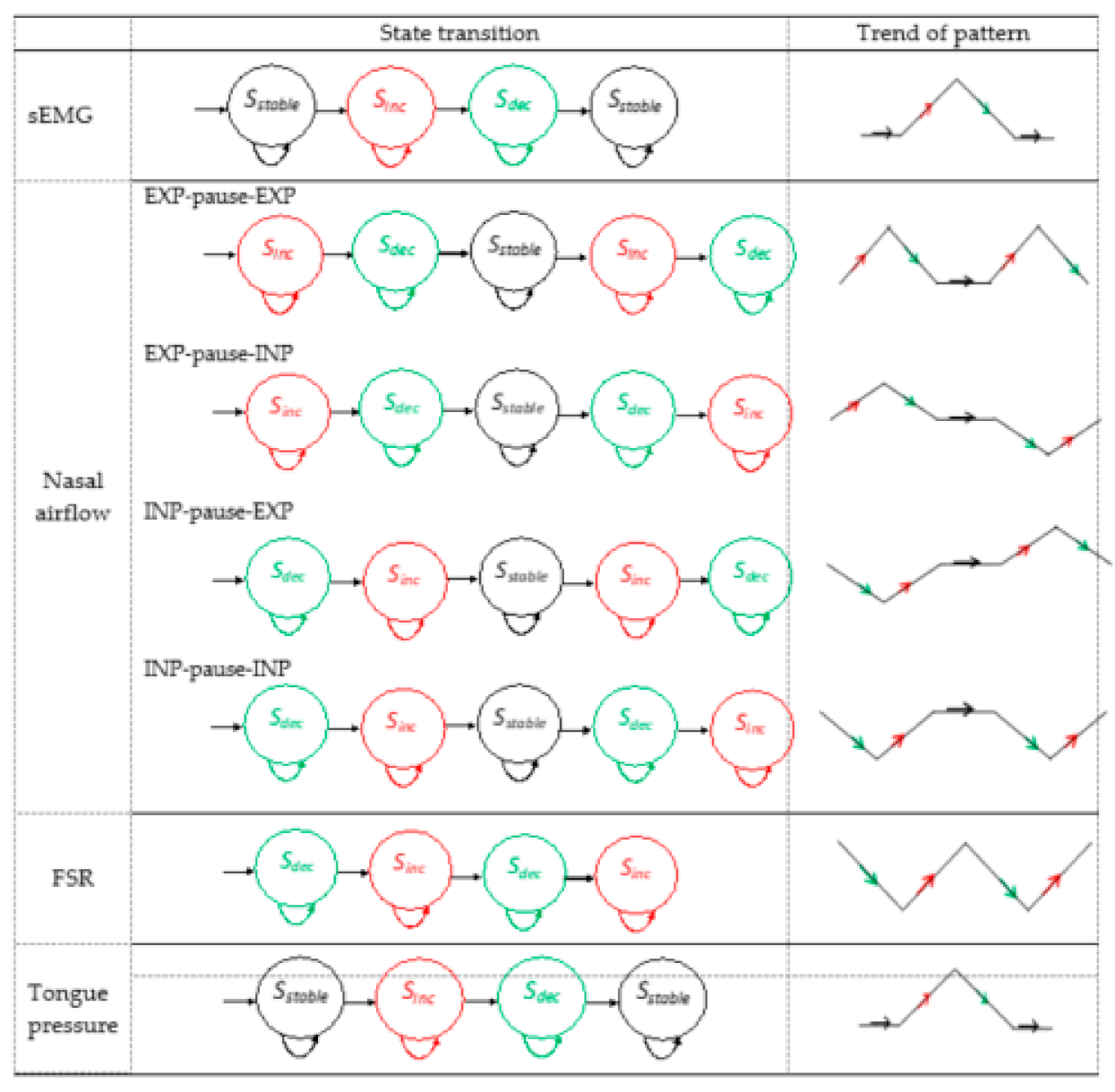
2.2. Multisensor Analytic Swallowing Model
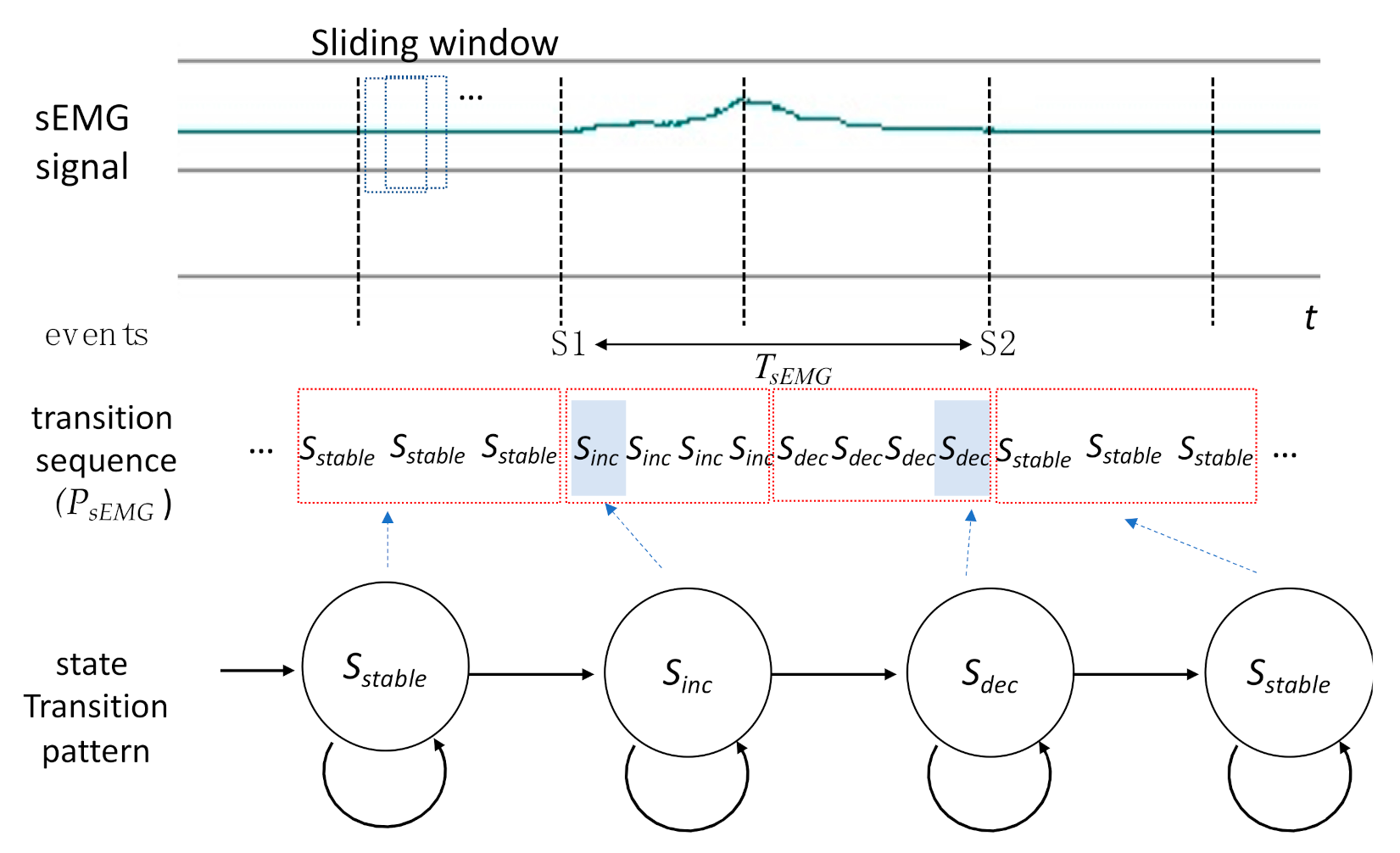
2.3. Pattern Autodetection
2.4. Participants
3. Experimental Results
3.1. Verification of the Autodetection Program
3.2. Results of sEMG
3.3. Results of Nasal Airflow
3.4. Results of FSR
3.5. Results of Tongue Pressure
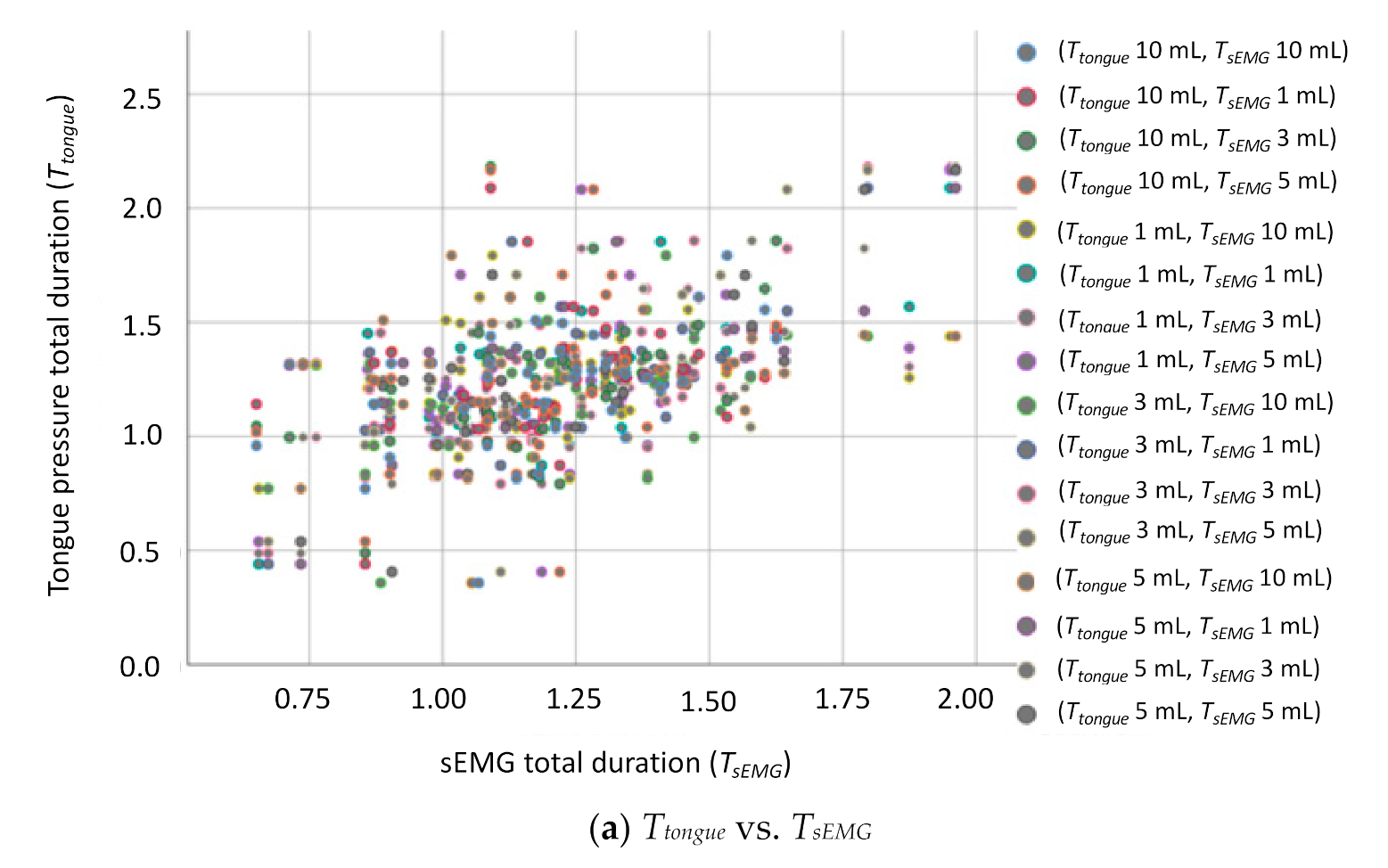
3.6. Correlations between Tongue Pressure and the Other Sensors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gil, C.G.; Desuter, G. Neurolaryngological disorders and deglutition. In Neurolaryngology; Sittel, C., Guntinas-Lichius, O., Eds.; Springer: Cham, Switzerland, 2018. [Google Scholar] [CrossRef]
- Bozorgi, C.; Holleufer, C.; Wendin, K. Saliva secretion and swallowing—The impact of different types of food and drink on subsequent intake. Nutrients 2020, 12, 256. [Google Scholar] [CrossRef] [PubMed]
- Ertekin, C. Physiological and pathological aspects of oropharyngeal swallowing. Mov. Disord. 2002, 17, S86–S89. [Google Scholar] [CrossRef] [PubMed]
- Sagawa, K.; Furuya, H.; Ohara, Y.; Yoshida, M.; Hirano, H.; Iijima, K.; Kikutani, T. Tongue function is important for masticatory performance in the healthy elderly: A cross-sectional survey of community-dwelling elderly. J. Prosthodont. Res. 2019, 63, 31–34. [Google Scholar] [CrossRef] [PubMed]
- Youmans, S.R.; Stierwalt, J.A.G. Measures of tongue function related to normal swallowing. Dysphagia 2006, 21, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Hori, K.; Taniguchi, H.; Hayashi, H.; Magara, J.; Minagi, Y.; Li, Q.; Ono, T.; Inoue, M. Role of tongue pressure production in oropharyngeal swallow biomechanics. Physiol. Rep. 2013, 1, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Hori, K.; Minagi, Y.; Uehara, F.; Salazar, S.E.; Ishihara, S.; Nakauma, M.; Funami, T.; Ikebe, K.; Maeda, Y.; et al. Coordination of tongue pressure production, hyoid movement, and suprahyoid muscle activity during squeezing of gels. Arch. Oral Biol. 2020, 111, 104631. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, H.-S.; Yun, D.H.; Chon, J.; Han, Y.J.; Yoo, S.D.; Kim, D.H.; Lee, S.A.; Joo, H.I.; Park, J.-S.; et al. The relationship between tongue pressure and oral dysphagia in stroke patients. Ann. Rehabil. Med. 2016, 40, 620–628. [Google Scholar] [CrossRef]
- Park, J.-S.; Kim, H.-J.; Oh, D.-H. Effect of tongue strength training using the Iowa Oral Performance Instrument in stroke patients with dysphagia. J. Phys. Ther. Sci. 2015, 27, 3631–3634. [Google Scholar] [CrossRef]
- Yano, J.; Yamamoto-Shimizu, S.; Yokoyama, T.; Kumakura, I.; Hanayama, K.; Tsubahara, A. Effects of tongue-strengthening exercise on the geniohyoid muscle in young healthy adults. Dysphagia 2020, 35, 110–116. [Google Scholar] [CrossRef]
- Fukuoka, T.; Ono, T.; Hori, K.; Wada, Y.; Uchiyama, Y.; Kasama, S.; Yoshikawa, H.; Domen, K. Tongue pressure measurement and videofluoroscopic study of swallowing in patients with Parkinson’s disease. Dysphagia 2019, 34, 80–88. [Google Scholar] [CrossRef]
- Logemann, J.A. Manual for the Videofluorographic Study of Swallowing, 2nd ed.; PRO-ED: Austin, TX, USA, 1993; pp. 157–162. [Google Scholar]
- Palmer, J.B.; Kuhlemeier, K.V.; Tippett, D.C.; Lynch, C. A protocol for the videofluorographic swallowing study. Dysphagia 1993, 8, 209–214. [Google Scholar] [CrossRef]
- Hiss, S.G.; Postma, G.N. Fiberoptic endoscopic evaluation of swallowing. Laryngoscope 2003, 113. [Google Scholar] [CrossRef]
- Li, Q.; Minagi, Y.; Ono, T.; Chen, Y.; Hori, K.; Fujiwara, S.; Maeda, Y. The biomechanical coordination during oropharyngeal swallowing: An evaluation with a non-invasive sensing system. Sci. Rep. 2017, 7, 15165. [Google Scholar] [CrossRef]
- Li, Q.; Hori, K.; Minagi, Y.; Ono, T.; Chen, Y.J.; Kondo, J.; Fujiwara, S.; Tamine, K.; Hayashi, H.; Inoue, M.; et al. Development of a system to monitor laryngeal movement during swallowing using a bend sensor. PLoS ONE 2013, 8, e70850. [Google Scholar] [CrossRef] [PubMed]
- Shieh, W.-Y.; Wang, C.-M.; Cheng, H.-Y.K.; Wang, C.-H. Using wearable and non-invasive sensors to measure swallowing function: Detection, verification, and clinical application. Sensors 2019, 19, 2624. [Google Scholar] [CrossRef]
- Shieh, W.-Y.; Wang, C.-M.; Chang, C.-S. Development of a portable non-invasive swallowing and respiration assessment device. Sensors 2015, 15, 12428–12453. [Google Scholar] [CrossRef]
- Wang, C.-M.; Shieh, W.-Y.; Weng, Y.-H.; Hsu, Y.-H.; Wu, Y.-R. Non-invasive assessment determine the swallowing and respiration dysfunction in early Parkinson’s disease. Parkinsonism Relat. Disord. 2017, 42, 22–27. [Google Scholar] [CrossRef]
- Ejendibia, P.; Baridam, B.B. String Searching with DFA-based Algorithm. Int. J. Appl. Inf. Syst. 2015, 9, 1–6. [Google Scholar] [CrossRef]
- LabVIEW. Available online: http://www.ni.com/ (accessed on 22 February 2021).
- Crary, M.A.; Carnaby-Mann, G.D.; Groher, M.E. Initial psychometric assessment of a functional oral intake scale for dysphagia in stroke patients. Arch. Phys. Med. Rehabil. 2005, 86, 1516–1520. [Google Scholar] [CrossRef]
- Ketel, E.C.; Aguayo-Mendoza, M.G.; Wijk, R.A.; Graaf, C.; Piqueras-Fiszman, B.; Stieger, M. Age, gender, ethnicity and eating capability influence oral processing behaviour of liquid, semi-solid and solid foods differently. Food Res. Int. 2019, 119, 143–151. [Google Scholar] [CrossRef]
- Yano, J.; Aoyagi, Y.; Ono, T.; Hori, K.; Yamaguchi, W.; Fujiwara, S.; Kumakura, I.; Minagi, S.; Tsubahara, S. Sequential coordination between lingual and pharyngeal pressures produced during dry swallowing. BioMed Res. Int. 2014, 2014. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sayaca, C.; Serel-Arslan, S.; Sayaca, N.; Demir, N.; Somay, G.; Kaya, D.; Karaduman, A. Is the proprioceptive neuromuscular facilitation technique superior to Shaker exercises in swallowing rehabilitation? Eur. Arch. Otorhinolaryngol. 2020, 277, 497–504. [Google Scholar] [CrossRef]
- Yoshikawa, M.; Yoshida, M.; Tsuga, K.; Akagawa, Y.; Groher, M.E. Comparison of three types of tongue pressure measurement devices. Dysphagia 2011, 26, 232–237. [Google Scholar] [CrossRef] [PubMed]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Signals | Events | Definition |
|---|---|---|
| sEMG | S1 | Submental muscles begin to move |
| S2 | Submental muscles stop moving and return to their resting state | |
| Nasal airflow | N1 | Nasal cavity begins to stop respiration |
| N2 | Nasal cavity restarts respiration | |
| Thyroid cartilage | C1 | Thyroid cartilage begins to move |
| C2 | Thyroid cartilage moves to its highest position | |
| C3 | Thyroid cartilage returns to its original position | |
| Tongue pressure | T1 | Tongue begins to squeeze |
| T2 | Tongue squeezing ends | |
| TP | Tongue pressure peaks |
| Parameters | Definition | Value |
|---|---|---|
| TsEMG | Surface electromyography (sEMG) onset time | S1–S2 |
| TNAir | Nasal airflow pause duration | N1–N2 |
| TTC1 | Thyroid cartilage first phase duration | C1–C2 |
| TTC2 | Thyroid cartilage second phase duration | C2–C3 |
| T TC1+ TC1 | Thyroid cartilage total excursion time | C1–C3 |
| Ttongue Ptongue | Tongue pressure onset duration Tongue pressure peak value | T1–T2 Peak at TP |
| Group | Age | Age | Male | Female |
|---|---|---|---|---|
| Range (Years) | Mean ± SD (Years) | |||
| Young | 20–39 | 26.6 ± 4.47 | 10 | 10 |
| Old | 39–62 | 48.6 ± 5.56 | 9 | 10 |
| Signal | 1 mL | 3 mL | 5 mL | 10 mL | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Manual (sec) ± SD | Auto (sec) ± SD | Bias ± 2SD | Error (%) | Manual (sec) ± SD | Auto (sec) ± SD | Bias ± 2SD | Error (%) | Manual (sec) ± SD | Auto (sec) ± SD | Bias ± 2SD | Error (%) | Manual (sec) ± SD | Auto (sec) ± SD | Bias ± 2SD | Error (%) | |
| sEMG | 1.27 ± 0.02 | 1.26 ± 0.06 | −0.01 ± 0.12 | 0.79 | 1.39 ± 0.04 | 1.40 ± 0.08 | 0.01 ± 0.15 | 0.72 | 1.34 ± 0.11 | 1.35 ± 0.03 | 0.01 ± 0.21 | 0.75 | 1.33 ± 0.07 | 1.34 ± 0.12 | 0.01 ± 0.24 | 0.75 |
| Nasal | 0.70 ± 0.13 | 0.72 ± 0.05 | 0.02 ± 0.26 | 2.86 | 0.67 ± 0.16 | 0.72 ± 0.12 | 0.05 ± 0.31 | 7.46 | 0.80 ± 0.05 | 0.79 ± 0.03 | −0.01 ± 0.10 | 1.25 | 0.84 ± 0.15 | 0.88 ± 0.13 | 0.04 ± 0.30 | 4.76 |
| FSR | 1.17 ± 0.16 | 1.22 ± 0.22 | 0.05 ± 0.44 | 4.27 | 1.21 ± 0.15 | 1.25 ± 0.11 | 0.04 ± 0.30 | 3.31 | 1.11 ± 0.13 | 1.10 ± 0.12 | −0.01 ± 0.25 | 0.90 | 1.30 ± 0.19 | 1.34 ± 0.08 | 0.04 ± 0.38 | 3.08 |
| Tongue | 1.51 ± 0.03 | 1.54 ± 0.03 | 0.03 ± 0.06 | 1.99 | 1.32 ± 0.06 | 1.34 ± 0.02 | 0.02 ± 0.12 | 1.52 | 1.43 ± 0.21 | 1.44 ± 0.11 | 0.01 ± 0.41 | 0.70 | 1.48 ± 0.11 | 1.50 ± 0.07 | 0.02 ± 0.22 | 1.35 |
| Factor | Type | Mean | SD | p |
|---|---|---|---|---|
| Sex | Male | 1.28 | 0.32 | 0.671 |
| Female | 1.21 | 0.28 | ||
| Age | Young | 1.1 | 0.21 | 0.047 * |
| Old | 1.38 | 0.83 | ||
| Volume | 1 mL | 1.22 | 0.30 | 0.665 |
| 3 mL | 1.25 | 0.26 | ||
| 5 mL | 1.27 | 0.35 | ||
| 10 mL | 1.23 | 0.29 | ||
| Gender * Age | – | – | – | 0.738 |
| Gender * Volume | – | – | – | 0.468 |
| Age * Volume | – | – | – | 0.007 * |
| Gender * Age * Volume | – | – | – | 0.802 |
| Factor | Type | Mean | SD | p |
|---|---|---|---|---|
| Sex | Male | 0.59 | 0.14 | 0.017 * |
| Female | 0.56 | 0.13 | ||
| Age | Young | 0.58 | 0.16 | 0.172 |
| Old | 0.57 | 0.10 | ||
| Volume | 1 mL | 0.56 | 0.17 | 0.002 * |
| 3 mL | 0.56 | 0.13 | ||
| 5 mL | 0.57 | 0.11 | ||
| 10 mL | 0.63 | 0.14 | ||
| Gender * Age | – | – | – | 0.371 |
| Gender * Volume | – | – | – | 0.171 |
| Age * Volume | – | – | – | 0.513 |
| Gender * Age * Volume | – | – | – | 0.260 |
| Factor | Type | Mean | SD | p |
|---|---|---|---|---|
| Sex | Male | 1.17 | 0.18 | 0.011 * |
| Female | 1.14 | 0.19 | ||
| Age | Young | 1.13 | 0.17 | 0.001 * |
| Old | 1.18 | 0.19 | ||
| Volume | 1 mL | 1.09 | 0.20 | 0.001 * |
| 3 mL | 1.15 | 0.17 | ||
| 5 mL | 1.18 | 0.19 | ||
| 10 mL | 1.23 | 0.19 | ||
| Gender * Age | – | – | – | 0.685 |
| Gender * Volume | – | – | – | 0.428 |
| Age * Volume | – | – | – | 0.102 |
| Gender * Age * Volume | – | – | – | 0.816 |
| Factor | Type | Mean | SD | p |
|---|---|---|---|---|
| Sex | Male | 0.57 | 0.13 | 0.297 |
| Female | 0.60 | 0.13 | ||
| Age | Young | 0.59 | 0.12 | 0.327 |
| Old | 0.58 | 0.15 | ||
| Volume | 1 mL | 0.56 | 0.15 | 0.390 |
| 3 mL | 0.60 | 0.12 | ||
| 5 mL | 0.59 | 0.14 | ||
| 10 mL | 0.61 | 0.14 | ||
| Gender * Age | – | – | – | 0.588 |
| Gender * Volume | – | – | – | 0.653 |
| Age * Volume | – | – | – | 0.462 |
| Gender * Age * Volume | – | – | – | 0.941 |
| Factor | Type | Mean | SD | p |
|---|---|---|---|---|
| Sex | Male | 0.59 | 0.12 | 0.001 * |
| Female | 0.54 | 0.09 | ||
| Age | Young | 0.53 | 0.10 | 0.002 * |
| Old | 0.59 | 0.11 | ||
| Volume | 1 mL | 0.51 | 0.11 | 0.001 * |
| 3 mL | 0.55 | 0.11 | ||
| 5 mL | 0.58 | 0.13 | ||
| 10 mL | 0.63 | 0.10 | ||
| Gender * Age | – | – | – | 0.401 |
| Gender * Volume | – | – | – | 0.051 |
| Age * Volume | – | – | – | 0.071 |
| Gender * Age * Volume | – | – | – | 0.320 |
| Factor | Type | Mean | SD | p |
|---|---|---|---|---|
| Sex | Male | 1.30 | 0.27 | 0.038 * |
| Female | 1.21 | 0.32 | ||
| Age | Young | 1.16 | 0.27 | 0.036 * |
| Old | 1.38 | 0.28 | ||
| Volume | 1 mL | 1.27 | 0.28 | 0.420 |
| 3 mL | 1.26 | 0.31 | ||
| 5 mL | 1.29 | 0.36 | ||
| 10 mL | 1.22 | 0.27 | ||
| Gender * Age | – | – | – | 0.401 |
| Gender * Volume | – | – | – | 0.051 |
| Age * Volume | – | – | – | 0.071 |
| Gender * Age * Volume | – | – | – | 0.320 |
| Factor | Type | Mean | SD | p |
|---|---|---|---|---|
| Sex | Male | 0.11 | 0.04 | 0.012 * |
| Female | 0.13 | 0.04 | ||
| Age | Young | 0.14 | 0.03 | 0.016 * |
| Old | 0.11 | 0.04 | ||
| Volume | 1 mL | 0.13 | 0.04 | 0.288 |
| 3 mL | 0.12 | 0.04 | ||
| 5 mL | 0.12 | 0.04 | ||
| 10 mL | 0.12 | 0.04 | ||
| Gender * Age | – | – | – | 0.574 |
| Gender * Volume | – | – | – | 0.722 |
| Age * Volume | – | – | – | 0.692 |
| Gender * Age * Volume | – | – | – | 0.526 |
| Two Parameters | Water Volume | Pearson’s r | p |
|---|---|---|---|
| Ttongue vs. TsEMG | 1 mL | 0.611 | <0.01 ** |
| 3 mL | 0.671 | <0.01 ** | |
| 5 mL | 0.717 | <0.01 ** | |
| 10 mL | 0.532 | <0.01 ** | |
| Ttongue vs. TNAir | 1 mL | −0.001 | 0.993 |
| 3 mL | 0.272 | 0.094 | |
| 5 mL | 0.204 | 0.213 | |
| 10 mL | −0.019 | 0.908 | |
| Ttongue vs. TTC1+TC2 | 1 mL | 0.117 | 0.479 |
| 3 mL | 0.153 | 0.352 | |
| 5 mL | −0.026 | 0.877 | |
| 10 mL | 0.221 | 0.177 |
| Air Bulb Method | Sensor Sheet Methods | |
|---|---|---|
| Sensor number | 1 | 3–5 |
| Sensing area | bulb shape/length 3.0 cm/diameter 1.3 cm/thickness 0.5 cm | triangle/base 8.0 cm/height 8 cm/thickness 0.1 cm |
| Sensing position | between the tongue and the hard palate | attach on the hard palate |
| Attachment | without the use of glue | need to use the glue to fix the sheet |
| Sample rate | 1 KHz | 100 Hz |
| Measurement | tongue pressure, onset duration | tongue pressure, onset duration, pressure distribution |
| Material | soft rubber | conductive tactile sheet |
| Usage | disposable | reuse |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shieh, W.-Y.; Wang, C.-M.; Cheng, H.-Y.K.; Imbang, T.I. Noninvasive Measurement of Tongue Pressure and Its Correlation with Swallowing and Respiration. Sensors 2021, 21, 2603. https://doi.org/10.3390/s21082603
Shieh W-Y, Wang C-M, Cheng H-YK, Imbang TI. Noninvasive Measurement of Tongue Pressure and Its Correlation with Swallowing and Respiration. Sensors. 2021; 21(8):2603. https://doi.org/10.3390/s21082603
Chicago/Turabian StyleShieh, Wann-Yun, Chin-Man Wang, Hsin-Yi Kathy Cheng, and Titilianty Ignatia Imbang. 2021. "Noninvasive Measurement of Tongue Pressure and Its Correlation with Swallowing and Respiration" Sensors 21, no. 8: 2603. https://doi.org/10.3390/s21082603
APA StyleShieh, W.-Y., Wang, C.-M., Cheng, H.-Y. K., & Imbang, T. I. (2021). Noninvasive Measurement of Tongue Pressure and Its Correlation with Swallowing and Respiration. Sensors, 21(8), 2603. https://doi.org/10.3390/s21082603