
Non-Contact Monitoring and Classification of Breathing Pattern for the Supervision of People Infected by COVID-19




Abstract
:1. Introduction
2. Related Work
3. Proposed System
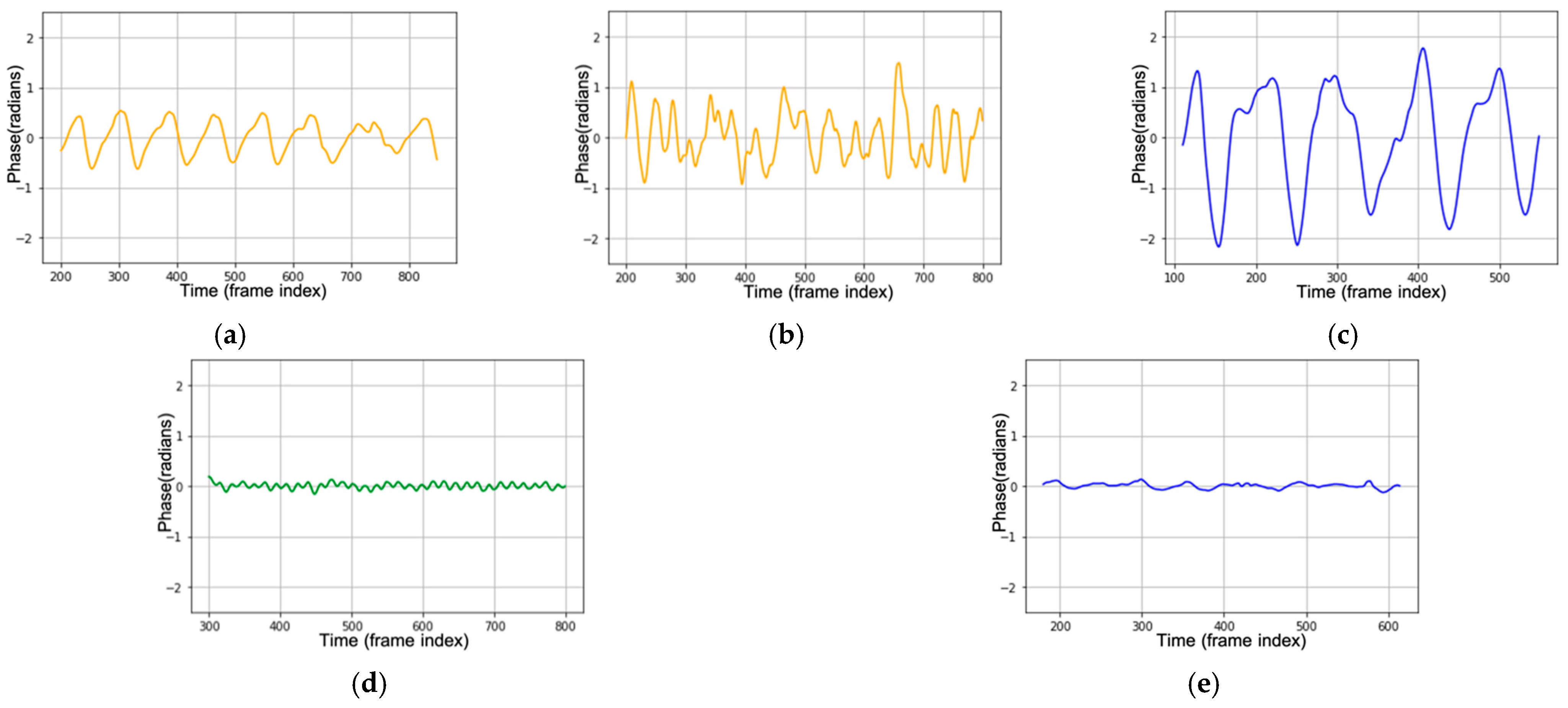
- Class 1—normal breathing: normal breathing has a constant breathing waveform and similar pattern during the time, shown in Figure 1a.
- Class 2—deep and quick breathing: deep and quick breathing has a large amplitude with a high frequency (high respiration rate), shown in Figure 1d.
- Class 3—deep breathing: deep breathing has a large amplitude with a normal respiration rate, shown in Figure 1c.
- Class 4—quick breathing: quick breathing has a small amplitude (short breath) with high frequency (high respiration rate), shown in Figure 1d.
- Class 5—holding the breath: the breathing waveform is almost disappeared, and the amplitudes are close to zero, shown in Figure 1e.
3.1. FMCW Module
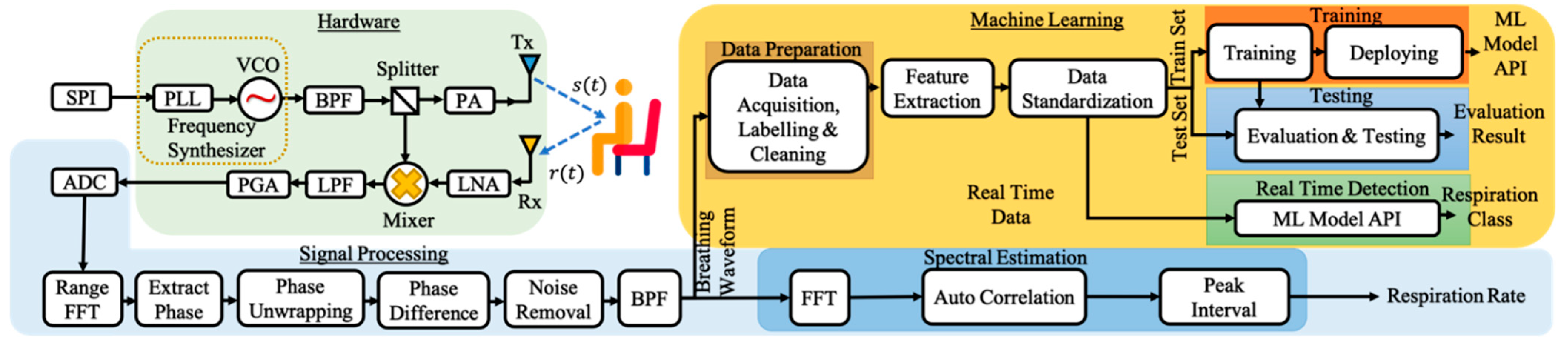
3.1.1. Signal Processing in Hardware
- The process begins when the user instructs the microcontroller unit (MCU).
- The instruction is transmitted through a serial peripheral interface (SPI), serial communication for short-distance communication.
- FMCW uses a continuous signal that has modulated frequency. Thus, we need a frequency synthesizer that generates the modulated frequency signal.
- A phase-locked loop (PLL) is a feedback control system that compares the phase of two input signals in a frequency synthesizer. It produces an error signal proportional to the difference between their steps.
- The error signal is then passed through the low-pass filter (LPF) and is used to drive the voltage control oscillator (VCO).
- The VCO produces the output frequency. VCO increases the frequency by increasing the voltage.
- Bandpass filter (BPF) is then used to filter the signal. The signal is passed through a BPF so that only the main frequency is used and the harmonic frequency is ignored.
- The splitter is used to split the signal for the mixer and the transmitter.
- A power amplifier (PA) amplifies the signal before being transmitted by the transmitter antenna (Tx).
- Tx emits a modulated signal towards the object. The object will reflect the signal, and the receiver will receive the reflection.
- The signal received by the receiver will have a difference in frequency compared to the signal emitted by the transmitter. This difference describes the time for the signal to travel from the transmitter to the object. The object distance is obtained from the traveling time.
- As the received signal is very weak, we use a low noise amplifier (LNA) that amplifies the received signal .
- The mixer will mix the transmitted signal and received signal .
- We only need the signal with low frequency; we pass the signal through LPF to obtain the low-frequency signal and remove the high-frequency signal.
- PGA is a programmable gain amplifier that can control the gain.
- Finally, the data is transmitted to the MCU.
- The analog-to-digital converter (ADC) will convert the analog signal to the digital signal.
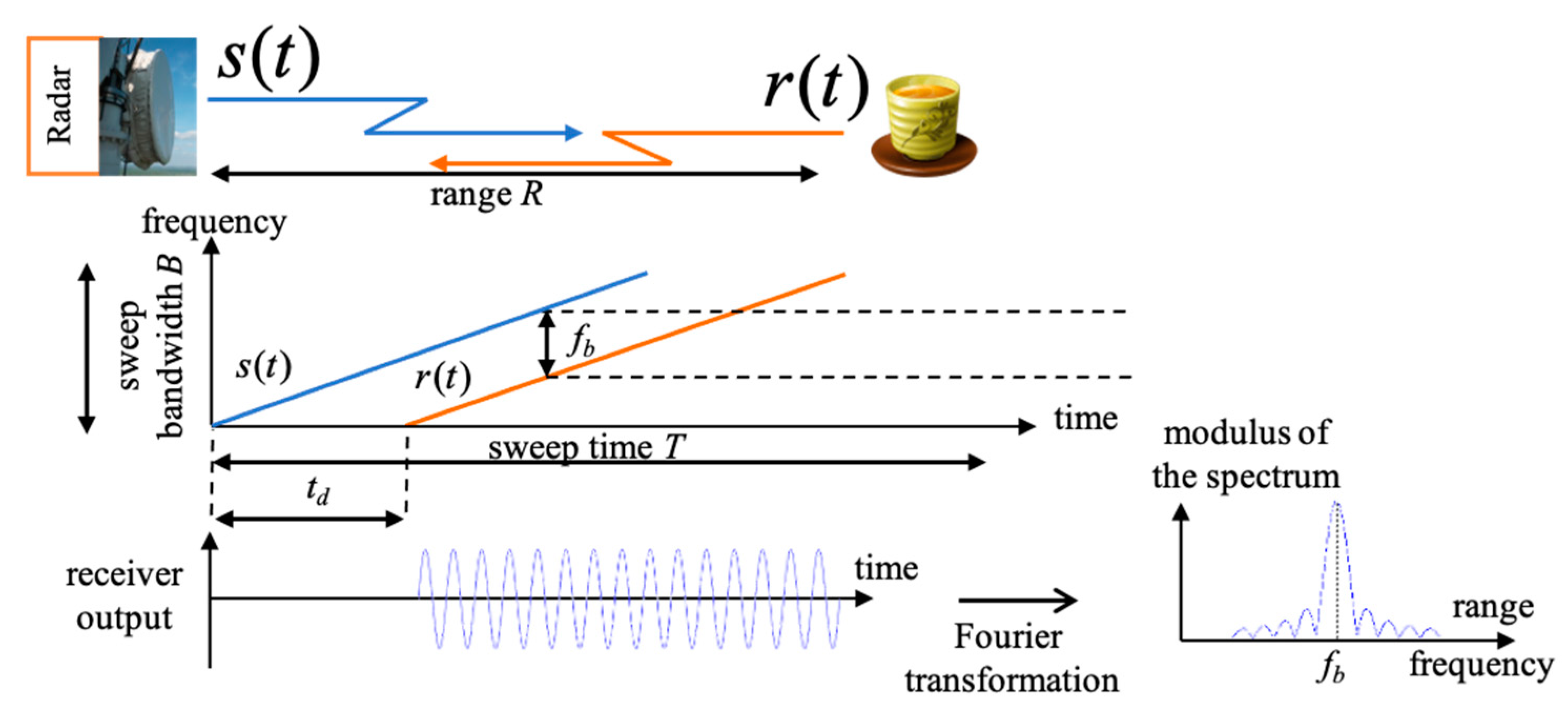
3.1.2. FMCW Signal Model
3.2. Signal Processing Module
3.2.1. Range FFT
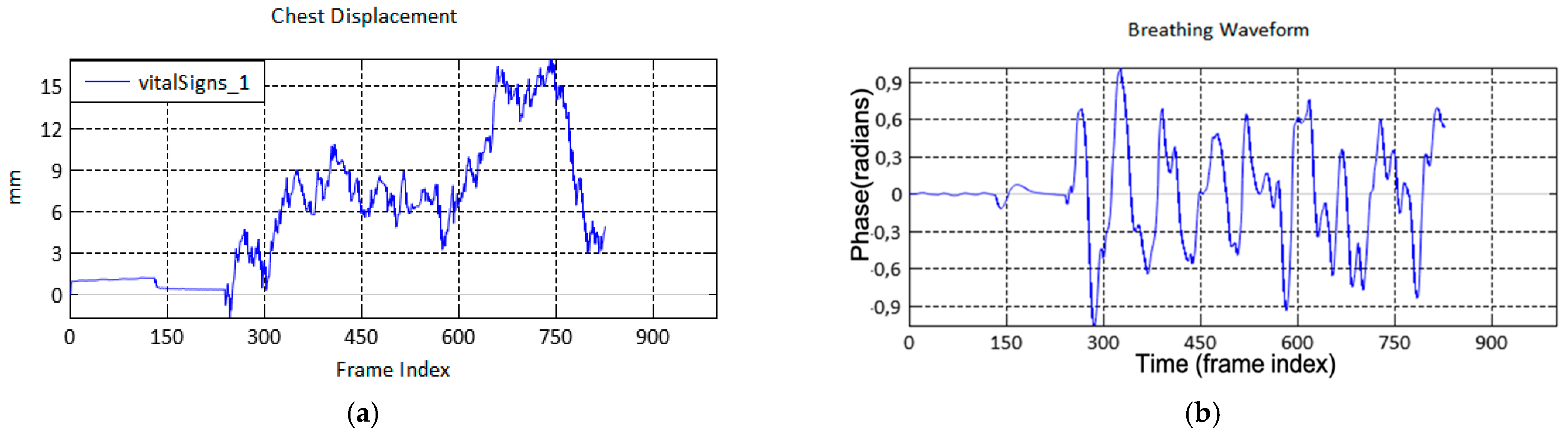
3.2.2. Extraction and Unwrapping
3.2.3. Noise Removal
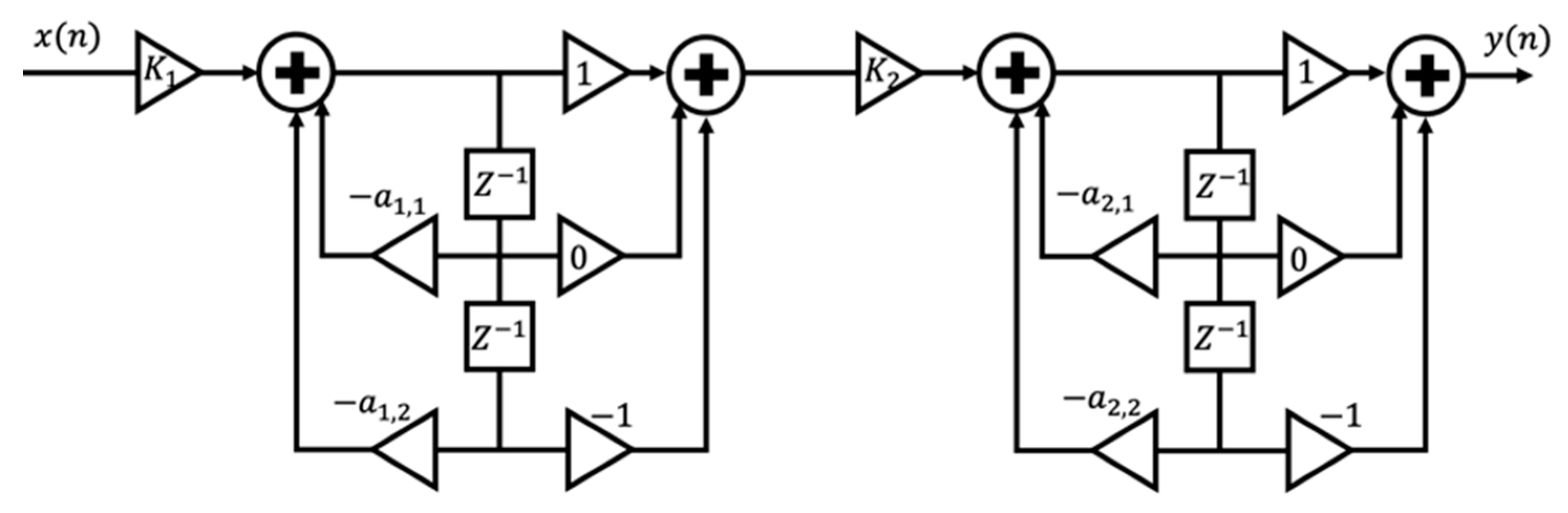
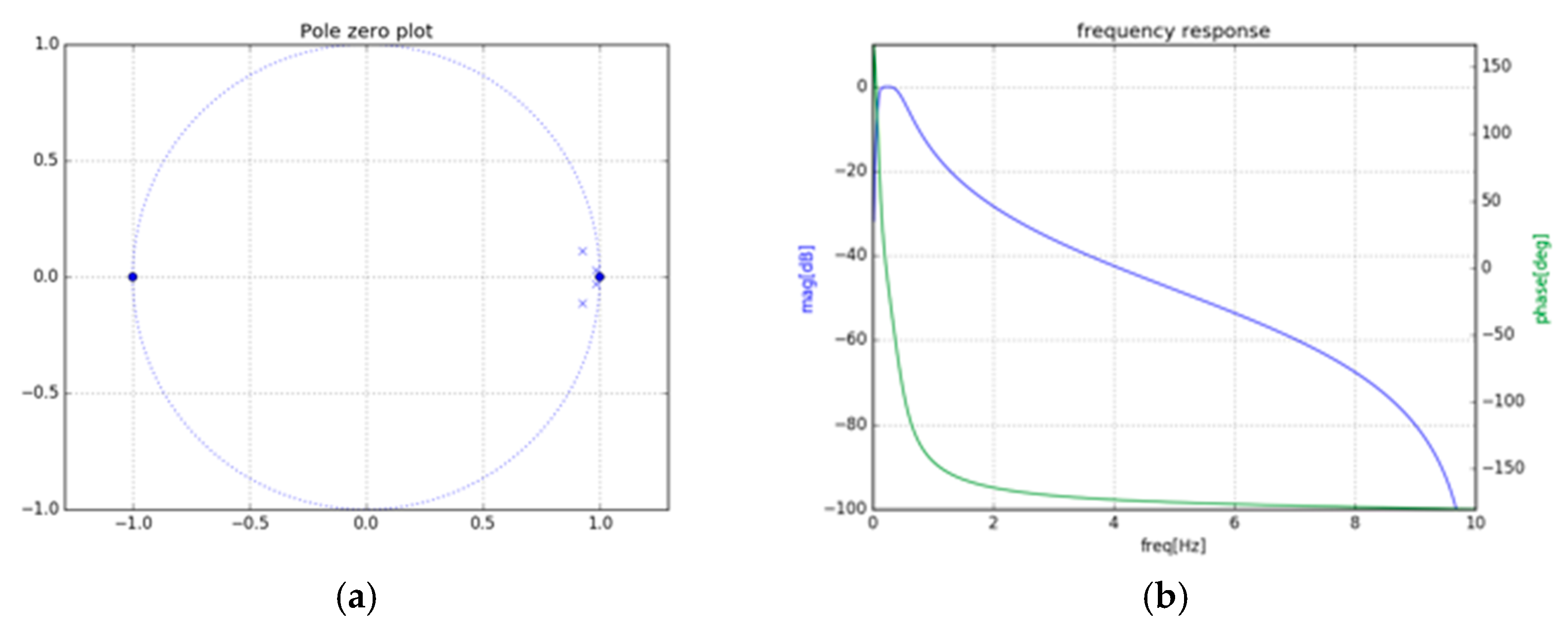
3.2.4. IIR BPF Using Cascaded Bi-Quad
3.2.5. Respiration Rate
3.3. Machine Learning (Classification Method) Module
3.3.1. Pre-Processing
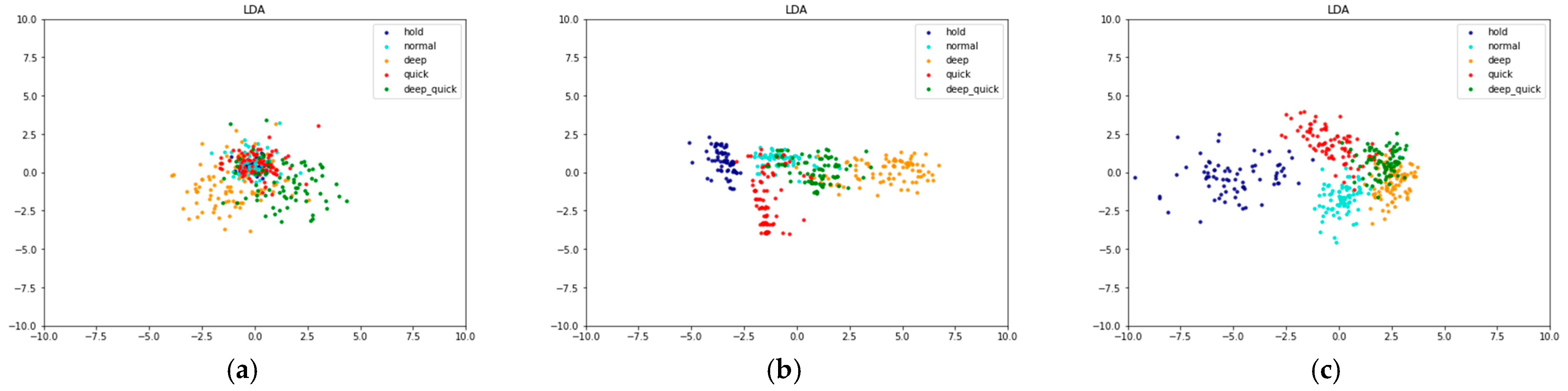
3.3.2. MFCC Feature Extraction
- Frame Blocking
- 2.
- Windowing
- 3.
- Fast Fourier Transform (FFT)
- 4.
- Mel-frequency Wrapping (MFW)
- 5.
- Discrete Cosine Transform (DCT)
- 6.
- Cepstral Liftering
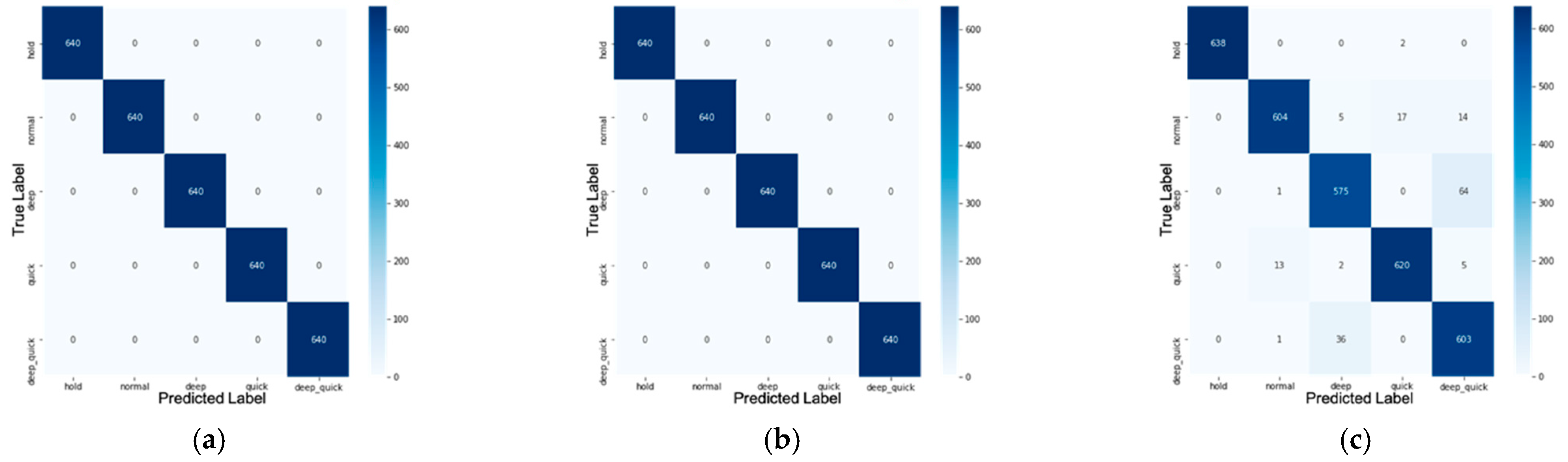
3.3.3. Classification Using XGBoost Classifier
4. Experimental and Analysis Results
4.1. Experimental Setup
4.2. Data Collection and Labelling
4.3. Experiment and Analysis Results
- The mean is the average value of the population.
- The median or middle value is a measure of data centering. If the data is sorted, the observed value is in the middle.
- Maximum describes a greater value than or equal to all values in data.
- Variance presents a square of the average distance between each quantity and mean.
- Standard deviation is used to measure the amount of variation or dispersion of data. The standard deviation describes how far the sample deviates from the mean.
- Absolute deviation represents the absolute difference between each data point and the average. This explains the variability of the data set.
- Kurtosis defines the degree of “tailedness” of a distribution.
- Skewness is known as a measure of slope, which is a number that can indicate whether the curve shape is slanted or not.
- n estimators: [200 300 400], n estimators represent the number of sequential trees modelled in XGBoost.
- Max depth: [3 4 5], max depth means the maximum number of terminal nodes in a tree.
- Learning rate: [0.1, 0.01, 0.001], the learning rate is the learning parameters that control the change value in estimating the prediction. A smaller value causes a stronger model with specific characteristics of the tree. However, lower values will require a larger number of trees to model all relations and do a lot of computation.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Spinelli, A.; Pellino, G. COVID-19 pandemic: Perspectives on an unfolding crisis. Br. J. Surg. 2020, 107, 785–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, Y.Y.; Ma, Y.T.; Zhang, J.Y.; Xie, X. COVID-19 and the cardiovascular system. Nat. Rev. Cardiol. 2020, 17, 259–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singhal, T. A review of coronavirus disease-2019 (COVID-19). Indian J. Pediatrics 2020, 87, 281–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, D.; Tang, Z.; Wang, S.; Hui, H.; Gong, L.; Lu, Y.; Xue, Z.; Liao, H.; Chen, F.; Yang, F.; et al. The role of imaging in the detection and management of COVID-19: A review. IEEE Rev. Biomed. Eng. 2020, 14, 16–29. [Google Scholar] [CrossRef]
- Cai, J.; Sun, W.; Huang, J.; Gamber, M.; Wu, J.; He, G. Indirect virus transmission in cluster of COVID-19 cases, Wenzhou, China, 2020. Emerg. Infect. Dis. 2020, 26, 1343–1345. [Google Scholar] [CrossRef] [PubMed]
- Jones, N.R.; Qureshi, Z.U.; Temple, R.J.; Larwood, J.P.; Greenhalgh, T.; Bourouiba, L. Two metres or one: What is the evidence for physical distancing in covid-19? BMJ 2020, 370, m3223. [Google Scholar] [CrossRef]
- Salathé, M.; Althaus, C.L.; Neher, R.; Stringhini, S.; Hodcroft, E.; Fellay, J.; Zwahlen, M.; Senti, G.; Battegay, M.; Wilder-Smith, A.; et al. COVID-19 epidemic in Switzerland: On the importance of testing, contact tracing and isolation. Swiss Med Wkly. 2020, 150, w20225. [Google Scholar] [CrossRef]
- Lewnard, J.A.; Lo, N.C. Scientific and ethical basis for social-distancing interventions against COVID-19. Lancet Infect. Dis. 2020, 20, 631–633. [Google Scholar] [CrossRef] [Green Version]
- Pan, L.; Mu, M.; Yang, P.; Sun, Y.; Wang, R.; Yan, J.; Li, P.; Hu, B.; Wang, J.; Hu, C.; et al. Clinical characteristics of COVID-19 patients with digestive symptoms in Hubei, China: A descriptive, cross-sectional, multicenter study. Am. J. Gastroenterol. 2020, 115. [Google Scholar] [CrossRef] [PubMed]
- Su, W.-C.; Juan, P.-H.; Chian, D.-M.; Horng, T.-S.J.; Wen, C.-K.; Wang, F.-K. 2-D Self-Injection-Locked Doppler Radar for Locating Multiple People and Monitoring Their Vital Signs. IEEE Trans. Microw. Theory Tech. 2021, 69, 1016–1026. [Google Scholar] [CrossRef]
- Poyiadji, N.; Shahin, G.; Noujaim, D.; Stone, M.; Patel, S.; Griffith, B. COVID-19—Associated acute hemorrhagic necrotizing encephalopathy: CT and MRI features. Radiology 2020, 296, E119–E120. [Google Scholar] [CrossRef] [Green Version]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Wang, Y.; Hu, M.; Li, Q.; Zhang, X.P.; Zhai, G.; Yao, N. Abnormal respiratory patterns classifier may contribute to large-scale screening of people infected with COVID-19 in an accurate and unobtrusive manner. arXiv 2020, arXiv:2002.05534. [Google Scholar]
- Massaroni, C.; Lo Presti, D.; Formica, D.; Silvestri, S.; Schena, E. Non-Contact Monitoring of Breathing Pattern and Respiratory Rate via RGB Signal Measurement. Sensors 2019, 19, 2758. [Google Scholar] [CrossRef] [Green Version]
- Cretikos, M.A.; Bellomo, R.; Hillman, K.; Chen, J.; Finfer, S.; Flabouris, A. Respiratory rate: The neglected vital sign. Med J. Aust. 2008, 188, 657–659. [Google Scholar] [CrossRef]
- Hellewell, J.; Abbott, S.; Gimma, A.; Bosse, N.I.; Jarvis, C.I.; Russell, T.W.; Munday, J.D.; Kucharski, A.J.; Edmunds, W.J.; Sun, F.; et al. Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. Lancet Glob. Health 2020, 8, 488–496. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Kim, B.-H.; Park, J.-K.; Yook, J.-G. A Novel Vital-Sign Sensing Algorithm for Multiple Subjects Based on 24-GHz FMCW Doppler Radar. Remote Sens. 2019, 11, 1237. [Google Scholar] [CrossRef] [Green Version]
- Jin, F.; Zhang, R.; Sengupta, A.; Cao, S.; Hariri, S.; Agarwal, N.K.; Agarwal, S.K. Multiple Patients Behavior Detection in Real-time using mmWave Radar and Deep CNNs. In Proceedings of the 2019 IEEE Radar Conference (RadarConf), Boston, MA, USA, 22–26 April 2019. [Google Scholar]
- Cardillo, E.; Caddemi, A. Radar Range-Breathing Separation for the Automatic Detection of Humans in Cluttered Environments. IEEE Sens. J. 2020. [Google Scholar] [CrossRef]
- Cardillo, E.; Li, C.; Caddemi, A. Vital Sign Detection and Radar Self-Motion Cancellation Through Clutter Identification. IEEE Trans. Microw. Theory Tech. 2021, 69, 1932–1942. [Google Scholar] [CrossRef]
- Miao, D.; Zhao, H.; Hong, H.; Zhu, X.; Li, C. Doppler radar-based human breathing patterns classification using Support Vector Machine. In Proceedings of the 2017 IEEE Radar Conference (RadarConf), Seattle, WA, USA, 8–12 May 2017. [Google Scholar]
- Ji, S.; Wen, H.; Wu, J.; Zhang, Z.; Zhao, K. Systematic Heartbeat Monitoring using a FMCW mm-Wave Radar. In Proceedings of the 2021 IEEE International Conference on Consumer Electronics and Computer Engineering (ICCECE), Guangzhou, China, 15–17 January 2021. [Google Scholar]
- Al-Naji, A.; Gibson, K.; Lee, S.-H.; Chahl, J. Monitoring of Cardiorespiratory Signal: Principles of Remote Measurements and Review of Methods. IEEE Access 2017, 5, 15776–15790. [Google Scholar] [CrossRef]
- Harford, M.; Catherall, J.; Gerry, S.; Young, J.D.; Watkinson, P. Availability and performance of image-based, non-contact methods of monitoring heart rate, blood pressure, respiratory rate, and oxygen saturation: A systematic review. Physiol. Meas. 2019, 40, 06TR01. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Laurentius, T.; Bollheimer, C.; Leonhardt, S.; Hoog Antink, C. Noncontact Monitoring of Heart Rate and Heart Rate Variability in Geriatric Patients Using Photoplethysmography Imaging. IEEE J. Biomed. Health Inform. 2020, 1. [Google Scholar] [CrossRef]
- Kebe, M.; Gadhafi, R.; Mohammad, B.; Sanduleanu, M.; Saleh, H.; Al-Qutayri, M. Human Vital Signs Detection Methods and Potential Using Radars: A Review. Sensors 2020, 20, 1454. [Google Scholar] [CrossRef] [Green Version]
- Fioranelli, F.; Le Kernec, J.; Shah, S.A. Radar for Health Care: Recognizing Human Activities and Monitoring Vital Signs. IEEE Potentials 2019, 38, 16–23. [Google Scholar] [CrossRef] [Green Version]
- Wang, P.; Boufounos, P.; Mansour, H.; Orlik, P.V. Slow-Time MIMO-FMCW Automotive Radar Detection with Imperfect Waveform Separation. In Proceedings of the ICASSP 2020-2020 IEEE International Conference on Acoustics, Speech and Signal. Processing (ICASSP), Barcelona, Spain, 4–8 May 2020. [Google Scholar]
- Tang, L.; Meng, H.; Chen, X.; Zhang, J.; Lv, L.; Liu, K. A Novel 3D Imaging Method of FMCW MIMO-SAR. In Proceedings of the 2018 China International SAR Symposium (CISS), Shanghai, China, 10–12 October 2018. [Google Scholar]
- Wang, Y.; Wang, W.; Zhou, M.; Ren, A.; Tian, Z. Remote Monitoring of Human Vital Signs Based on 77-GHz mm-Wave FMCW Radar. Sensors 2020, 20, 2999. [Google Scholar] [CrossRef] [PubMed]
- Su, W.-C.; Tang, M.-C.; Arif, R.E.; Horng, T.-S.; Wang, F.-K. Stepped-Frequency Continuous-Wave Radar With Self-Injection-Locking Technology for Monitoring Multiple Human Vital Signs. IEEE Trans. Microw. Theory Tech. 2019, 67, 5396–5405. [Google Scholar] [CrossRef]
- Lee, Y.S.; Pathirana, P.N.; Caelli, T.; Evans, R. Doppler radar in respiratory monitoring: Detection and analysis. In Proceedings of the 2013 International Conference on Control. Automation and Information Sciences (ICCAIS), Nha Trang, Vietnam, 25–28 November 2013. [Google Scholar]
- Zito, D.; Pepe, D.; Mincica, M.; Zito, F.; Tognetti, A.; Lanata, A.; De Rossi, D. SoC CMOS UWB Pulse Radar Sensor for Contactless Respiratory Rate Monitoring. IEEE Trans. Biomed. Circuits Syst. 2011, 5, 503–510. [Google Scholar] [CrossRef]
- Chen, T.; Guestrin, C. XGBoost. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016. [Google Scholar]
- Parui, S.; Roshan Bajiya, A.K.; Samanta, D.; Chakravorty, N. Emotion Recognition from EEG Signal using XGBoost Algorithm. In Proceedings of the 2019 IEEE 16th India Council International Conference (INDICON), Rajkot, India, 13–15 December 2019. [Google Scholar]
- Sharma, D.; Ali, I. A modified MFCC feature extraction technique for robust speaker recognition. In Proceedings of the 2015 International Conference on Advances in Computing, Communications and Informatics (ICACCI), Kochi, India, 10–13 August 2015. [Google Scholar]
- Wang, X.Y. The Improved MFCC Speech Feature Extraction Method and its Application. Adv. Mater. Res. 2013, 756, 4059–4062. [Google Scholar] [CrossRef]
- Kiyokawa, H.; Greenberg, M.; Shirota, K.; Pasterkamp, H. Auditory Detection of Simulated Crackles in Breath Sounds. Chest 2001, 119, 1886–1892. [Google Scholar] [CrossRef] [Green Version]
- Casalino, G.; Castellano, G.; Zaza, G. A mHealth solution for contact-less self-monitoring of blood oxygen saturation. In Proceedings of the 2020 IEEE Symposium on Computers and Communications (ISCC), Rennes, France, 7–10 July 2020. [Google Scholar]
- Abdelnasser, H.; Harras, K.A.; Youssef, M. UbiBreathe. In Proceedings of the 16th ACM International Symposium on Mobile Ad Hoc Networking and Computing, Hangzhou, China, 22–25 June 2015. [Google Scholar]
- Liu, X.; Cao, J.; Tang, S.; Wen, J.; Guo, P. Contactless Respiration Monitoring Via Off-the-Shelf WiFi Devices. IEEE Trans. Mob. Comput. 2016, 15, 2466–2479. [Google Scholar] [CrossRef]
- Wang, X.; Yang, C.; Mao, S. PhaseBeat: Exploiting CSI Phase Data for Vital Sign Monitoring with Commodity WiFi Devices. In Proceedings of the 2017 IEEE 37th International Conference on Distributed Computing Systems (ICDCS), Atlanta, GA, USA, 5–8 June 2017. [Google Scholar]
- Rahman, A.; Lubecke, V.M.; Boric-Lubecke, O.; Prins, J.H.; Sakamoto, T. Doppler Radar Techniques for Accurate Respiration Characterization and Subject Identification. IEEE J. Emerg. Sel. Top. Circuits Syst. 2018, 8, 350–359. [Google Scholar] [CrossRef]
- Ahmad, A.; Roh, J.C.; Wang, D.; Dubey, A. Vital signs monitoring of multiple people using a FMCW millimeter-wave sensor. In Proceedings of the 2018 IEEE Radar Conference (RadarConf18), Oklahoma City, OK, USA, 23–27 April 2018. [Google Scholar]
- Hu, W.; Zhao, Z.; Wang, Y.; Zhang, H.; Lin, F. Noncontact Accurate Measurement of Cardiopulmonary Activity Using a Compact Quadrature Doppler Radar Sensor. IEEE Trans. Biomed. Eng. 2014, 61, 725–735. [Google Scholar] [CrossRef]
- Dell’Aversano, A.; Natale, A.; Buonanno, A.; Solimene, R. Through the Wall Breathing Detection by Means of a Doppler Radar and MUSIC Algorithm. IEEE Sens. Lett. 2017, 1, 1–4. [Google Scholar] [CrossRef]
- van Loon, K.; Breteler, M.J.; van Wolfwinkel, L.; Rheineck Leyssius, A.T.; Kossen, S.; Kalkman, C.J.; van Zaane, B.; Peelen, L.M. Wireless non-invasive continuous respiratory monitoring with FMCW radar: A clinical validation study. J. Clin. Monit. Comput. 2015, 30, 797–805. [Google Scholar] [CrossRef] [Green Version]
- He, M.; Nian, Y.; Gong, Y. Novel signal processing method for vital sign monitoring using FMCW radar. Biomed. Signal Process. Control 2017, 33, 335–345. [Google Scholar] [CrossRef]
- Prat, A.; Blanch, S.; Aguasca, A.; Romeu, J.; Broquetas, A. Collimated Beam FMCW Radar for Vital Sign Patient Monitoring. IEEE Trans. Antennas Propag. 2019, 67, 5073–5080. [Google Scholar] [CrossRef] [Green Version]
- Taylor, W.; Abbasi, Q.H.; Dashtipour, K.; Ansari, S.; Shah, S.A.; Khalid, A.; Imran, M.A. A Review of the State of the Art in Non-Contact Sensing for COVID-19. Sensors 2020, 20, 5665. [Google Scholar] [CrossRef] [PubMed]
- AL-Khalidi, F.Q.; Saatchi, R.; Burke, D.; Elphick, H.; Tan, S. Respiration rate monitoring methods: A review. Pediatric Pulmonol. 2011, 46, 523–529. [Google Scholar] [CrossRef] [Green Version]
- Ceniccola, G.D.; Castro, M.G.; Piovacari, S.M.; Horie, L.M.; Corrêa, F.G.; Barrere, A.P.; Toledo, D.O. Current technologies in body composition assessment: Advantages and disadvantages. Nutrition 2019, 62, 25–31. [Google Scholar] [CrossRef]
- Wang, L.; Lin, Z.Q.; Wong, A. COVID-Net: A tailored deep convolutional neural network design for detection of COVID-19 cases from chest X-ray images. Sci. Rep. 2020, 10, 1–12. [Google Scholar]
- Nam, Y.; Kong, Y.; Reyes, B.; Reljin, N.; Chon, K.H. Monitoring of Heart and Breathing Rates Using Dual Cameras on a Smartphone. PLoS ONE 2016, 11, e0151013. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, A.; Vaughan, R. Deep Learning Radar Design for Breathing and Fall Detection. IEEE Sens. J. 2020, 20, 5072–5085. [Google Scholar] [CrossRef]
- Barthel, P.; Wensel, R.; Bauer, A.; Muller, A.; Wolf, P.; Ulm, K.; Huster, K.M.; Francis, D.P.; Malik, M.; Schmidt, G. Respiratory rate predicts outcome after acute myocardial infarction: A prospective cohort study. Eur. Heart J. 2012, 34, 1644–1650. [Google Scholar] [CrossRef] [PubMed]
- Silva, T.A.; Silva, L.F.; Muchaluat-Saade, D.C.; Conci, A. A Computational Method to Assist the Diagnosis of Breast Disease Using Dynamic Thermography. Sensors 2020, 20, 3866. [Google Scholar] [CrossRef]
- Lahiri, B.B.; Bagavathiappan, S.; Jayakumar, T.; Philip, J. Medical applications of infrared thermography: A review. Infrared Phys. Technol. 2012, 55, 221–235. [Google Scholar] [CrossRef]
- Qiu, H.; Wu, J.; Hong, L.; Luo, Y.; Song, Q.; Chen, D. Clinical and epidemiological features of 36 children with coronavirus disease 2019 (COVID-19) in Zhejiang, China: An observational cohort study. Lancet Infect. Dis. 2020, 20, 689–696. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Qi, T.; Liu, L.; Ling, Y.; Qian, Z.; Li, T.; Li, F.; Xu, Q.; Zhang, Y.; Xu, S.; et al. Clinical progression of patients with COVID-19 in Shanghai, China. J. Infect. 2020, 80, e1–e6. [Google Scholar] [CrossRef]
- Reddi, B.; Fletcher, N. Physics of ultrasound. Focused Intensive Care Ultrasound 2019, 9–16. [Google Scholar] [CrossRef]
- Genc, A.; Ryk, M.; Suwała, M.; Zurakowska, T.; Kosiak, W. Ultrasound imaging in the general practitioner’s office–A literature review. J. Ultrason. 2016, 16, 78. [Google Scholar] [CrossRef]
- Li, C.; Xiao, Y.; Lin, J. A 5GHz Double-Sideband Radar Sensor Chip in 0.18 μm CMOS for Non-Contact Vital Sign Detection. IEEE Microw. Wirel. Compon. Lett. 2008, 18, 494–496. [Google Scholar]
- Lee, Y.S.; Pathirana, P.N.; Steinfort, C.L.; Caelli, T. Monitoring and Analysis of Respiratory Patterns Using Microwave Doppler Radar. IEEE J. Transl. Eng. Health Med. 2014, 2, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Staderini, E.M. UWB radars in medicine. IEEE Aerosp. Electron. Syst. Mag. 2002, 17, 13–18. [Google Scholar] [CrossRef]
- Immoreev, I. Practical Application of Ultra-Wideband Radars. In Proceedings of the 2006 3rd International Conference on Ultrawideband and Ultrashort Impulse Signals, Sevastopol, Ukraine, 18–22 September 2006. [Google Scholar]
- Adib, F.; Mao, H.; Kabelac, Z.; Katabi, D.; Miller, R.C. Smart Homes that Monitor Breathing and Heart Rate. Proc. 33rd Annu. ACM Conf. Human Factors Comput. Syst. 2015, 837–846. [Google Scholar] [CrossRef]
- Schleicher, B.; Nasr, I.; Trasser, A.; Schumacher, H. IR-UWB Radar Demonstrator for Ultra-Fine Movement Detection and Vital-Sign Monitoring. IEEE Trans. Microw. Theory Tech. 2013, 61, 2076–2085. [Google Scholar] [CrossRef] [Green Version]
- Li, C.; Lubecke, V.M.; Boric-Lubecke, O.; Lin, J. A Review on Recent Advances in Doppler Radar Sensors for Noncontact Healthcare Monitoring. IEEE Trans. Microw. Theory Tech. 2013, 61, 2046–2060. [Google Scholar] [CrossRef]
- Droitcour, A.; Lubecke, V.; Jenshan, L.; Boric-Lubecke, O. A microwave radio for Doppler radar sensing of vital signs. In Proceedings of the 2001 IEEE MTT-S International Microwave Sympsoium Digest (Cat. No.01CH37157), Phoenix, AZ, USA, 20–24 May 2001. [Google Scholar]
- Muehlsteff, J.; Thijs, J.A.J.; Pinter, R. The use of a two channel Doppler radar sensor for the characterization of heart motion phases. In Proceedings of the 2006 International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August–3 September 2006. [Google Scholar]
- Pisa, S.; Pittella, E.; Piuzzi, E. A survey of radar systems for medical applications. IEEE Aerosp. Electron. Syst. Mag. 2016, 31, 64–81. [Google Scholar] [CrossRef]
- Tu, J.; Lin, J. Fast Acquisition of Heart Rate in Noncontact Vital Sign Radar Measurement Using Time-Window-Variation Technique. IEEE Trans. Instrum. Meas. 2016, 65, 112–122. [Google Scholar] [CrossRef]
- Hsieh, C.-H.; Chiu, Y.-F.; Shen, Y.-H.; Chu, T.-S.; Huang, Y.-H. A UWB Radar Signal Processing Platform for Real-Time Human Respiratory Feature Extraction Based on Four-Segment Linear Waveform Model. IEEE Trans. Biomed. Circuits Syst. 2016, 10, 219–230. [Google Scholar] [CrossRef]
- Wang, S.; Pohl, A.; Jaeschke, T.; Czaplik, M.; Köny, M.; Leonhardt, S.; Pohl, N. A novel ultra-wideband 80 GHz FMCW radar system for contactless monitoring of vital signs. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 4978–4981. [Google Scholar]
- Xiong, Y.; Peng, Z.; Gu, C.; Li, S.; Wang, D.; Zhang, W. Differential Enhancement Method for Robust and Accurate Heart Rate Monitoring via Microwave Vital Sign Sensing. IEEE Trans. Instrum. Meas. 2020, 69, 7108–7118. [Google Scholar] [CrossRef]
- Lum, L.C. Hyperventilation Syndromes in Medicine and Psychiatry: A Review. J. Royal Society Med. 1987, 80, 229–231. [Google Scholar] [CrossRef] [Green Version]
- Abnormal-Breathing-Patterns. Available online: https://media.lanecc.edu/users/driscolln/RT127/Softchalk/regulation_of_Breathing/regulation_of_Breathing4.html (accessed on 24 March 2021).
- Texas Instrument IWR1443. Available online: https://www.ti.com/product/IWR1443 (accessed on 24 March 2021).
- Brooker, G.M. Understanding millimetre wave FMCW radars. In Proceedings of the 1st International Conference on Sensing Technology, Palmerston North, New Zealand, 21–23 November 2005; pp. 152–157. [Google Scholar]
- Itoh, K. Analysis of the phase unwrapping problem. Appl. Opt. 1982, 21, 2470. [Google Scholar] [CrossRef]
- Trouve, E.; Nicolas, J.-M.; Maitre, H. Improving phase unwrapping techniques by the use of local frequency estimates. IEEE Trans. Geosci. Remote Sens. 1998, 36, 1963–1972. [Google Scholar] [CrossRef] [Green Version]
- Kranjec, J.; Beguš, S.; Geršak, G.; Drnovšek, J. Non-contact heart rate and heart rate variability measurements: A review. Biomed. Signal Process. Control 2014, 13, 102–112. [Google Scholar] [CrossRef]
- Smith, S.W. The Scientist and Engineer’s Guide to Digital Signal Processing; California Technical Pub.: San Diego, CA, USA, 1997. [Google Scholar]
- Robertson, N. Design IIR Bandpass Filters. Available online: https://www.dsprelated.com/showarticle/1128.php (accessed on 24 March 2021).
- Patel, K.; Prasad, R.K. Speech recognition and verification using MFCC & VQ. Int. J. Emerg. Sci. Eng. 2013, 1, 137–140. [Google Scholar]
- Mansour, A.H.; Salh, G.Z.A.; Mohammed, K.A. Voice Recognition using Dynamic Time Warping and Mel-Frequency Cepstral Coefficients Algorithms. Int. J. Comput. Appl. 2015, 116, 34–41. [Google Scholar] [CrossRef] [Green Version]
- Muda, L.; Begam, M.; Elamvazuthi, I. Voice recognition algorithms using mel frequency cepstral coefficient (MFCC) and dynamic time warping (DTW) techniques. arXiv 2010, arXiv:1003.4083. [Google Scholar]
- Gupta, D.; Bansal, P.; Choudhary, K. The state of the art of feature extraction techniques in speech recognition. Speech Lang. Process. Hum. Mach. Commun. 2018, 195–207. [Google Scholar] [CrossRef]
- Davis, S.T.E.V.E.N.B.; Mermelstein, P.A.U.L. Comparison of Parametric Representations for Monosyllabic Word Recognition in Continuously Spoken Sentences. Read. Speech Recognit. 1990, 28, 65–74. [Google Scholar]
- Brownlee, J. XGBoost for Regression. Available online: https://machinelearningmastery.com/xgboost-for-regression/ (accessed on 24 March 2021).
- Kasturi, S.N. LightGBM vs XGBOOST: Which Algorithm Win the Race!!! Available online: https://towardsdatascience.com/lightgbm-vs-xgboost-which-algorithm-win-the-race-1ff7dd4917d (accessed on 24 April 2021).
- Bentéjac, C.; Csörgő, A.; Martínez-Muñoz, G. A comparative analysis of gradient boosting algorithms. Artif. Intell. Rev. 2021, 54, 1937–1967. [Google Scholar] [CrossRef]
- Blei, D.M.; Ng, A.Y.; Jordan, M.I. Latent dirichlet allocation. J. Mach. Learn. Res. 2003, 3, 993–1022. [Google Scholar]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Starting Frequency | Bandwidth | Chirp Rate | Samples Per-Chirp | Chirps Per-Frame | Chirp Duration | Frame Duration | Range Resolution | Max Unambiguous Range |
|---|---|---|---|---|---|---|---|---|
| 77 GHz | 4 GHz | 2 MHz | 250 samples | 2 | 50 μs | 50 ms | 0.0375 | 9 m |
| Class | Training Samples | Testing Samples |
|---|---|---|
| Normal breathing | 640 | 160 |
| Deep and quick breathing | 640 | 160 |
| Deep breathing | 640 | 160 |
| Quick breathing | 640 | 160 |
| Holding the breath | 640 | 160 |
| Total | 3200 | 800 |
| Feature Extraction | Training Accuracy | Testing Accuracy |
|---|---|---|
| without feature extraction (raw data) | 100% | 82.125% |
| statistic | 100% | 81.375% |
| MFCC | 95% | 87.375% |
| True Positive (TP) | True Negative (TN) |
|---|---|
| Prediction: the system detects that the patient suffers from X disease Reality: the patient does not suffer from X disease |
| False-Positive (FP) | False-Negative (FN) |
| Prediction: the system does not detect that the patient suffers from X disease Reality: the patient does not suffer from X disease |
| Class. | Raw (without Feature Extraction) | With Statistic Feature Extraction | With MFCC Feature Extraction | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Precision | Recall | f1-Score | Precision | Recall | f1-Score | Precision | Recall | f1-Score | |
| Normal | 0.873 | 0.644 | 0.741 | 0.728 | 0.688 | 0.707 | 0.807 | 0.731 | 0.767 |
| Deep quick | 0.728 | 0.719 | 0.723 | 0.738 | 0.775 | 0.756 | 0.886 | 0.875 | 0.881 |
| Deep | 0.815 | 0.994 | 0.9 | 0.87 | 1 | 0.93 | 0.844 | 0.981 | 0.908 |
| Quick | 0.741 | 0.75 | 0.745 | 0.758 | 0.606 | 0.674 | 0.874 | 0.781 | 0.825 |
| Hold | 0.958 | 1 | 0.979 | 0.947 | 1 | 0.973 | 0.952 | 1 | 0.976 |
| Class | Real-Time Measurement | Breathing Rate | |
|---|---|---|---|
| Manual | Measured | ||
| Normal |  | 21 | 20.51 |
| Deep Quick |  | 23 | 23.44 |
| Deep |  | 17 | 17.58 |
| Quick |  | 22 | 23.51 |
| Hold |  | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Purnomo, A.T.; Lin, D.-B.; Adiprabowo, T.; Hendria, W.F. Non-Contact Monitoring and Classification of Breathing Pattern for the Supervision of People Infected by COVID-19. Sensors 2021, 21, 3172. https://doi.org/10.3390/s21093172
Purnomo AT, Lin D-B, Adiprabowo T, Hendria WF. Non-Contact Monitoring and Classification of Breathing Pattern for the Supervision of People Infected by COVID-19. Sensors. 2021; 21(9):3172. https://doi.org/10.3390/s21093172
Chicago/Turabian StylePurnomo, Ariana Tulus, Ding-Bing Lin, Tjahjo Adiprabowo, and Willy Fitra Hendria. 2021. "Non-Contact Monitoring and Classification of Breathing Pattern for the Supervision of People Infected by COVID-19" Sensors 21, no. 9: 3172. https://doi.org/10.3390/s21093172
APA StylePurnomo, A. T., Lin, D.-B., Adiprabowo, T., & Hendria, W. F. (2021). Non-Contact Monitoring and Classification of Breathing Pattern for the Supervision of People Infected by COVID-19. Sensors, 21(9), 3172. https://doi.org/10.3390/s21093172