All the subjects succeeded during trials, and no cases of misunderstanding of the AGoRA Smart Walker behavior were reported. In this work, the sample size is considered small; however, studies with walkers have been conducted with similar sample sizes [
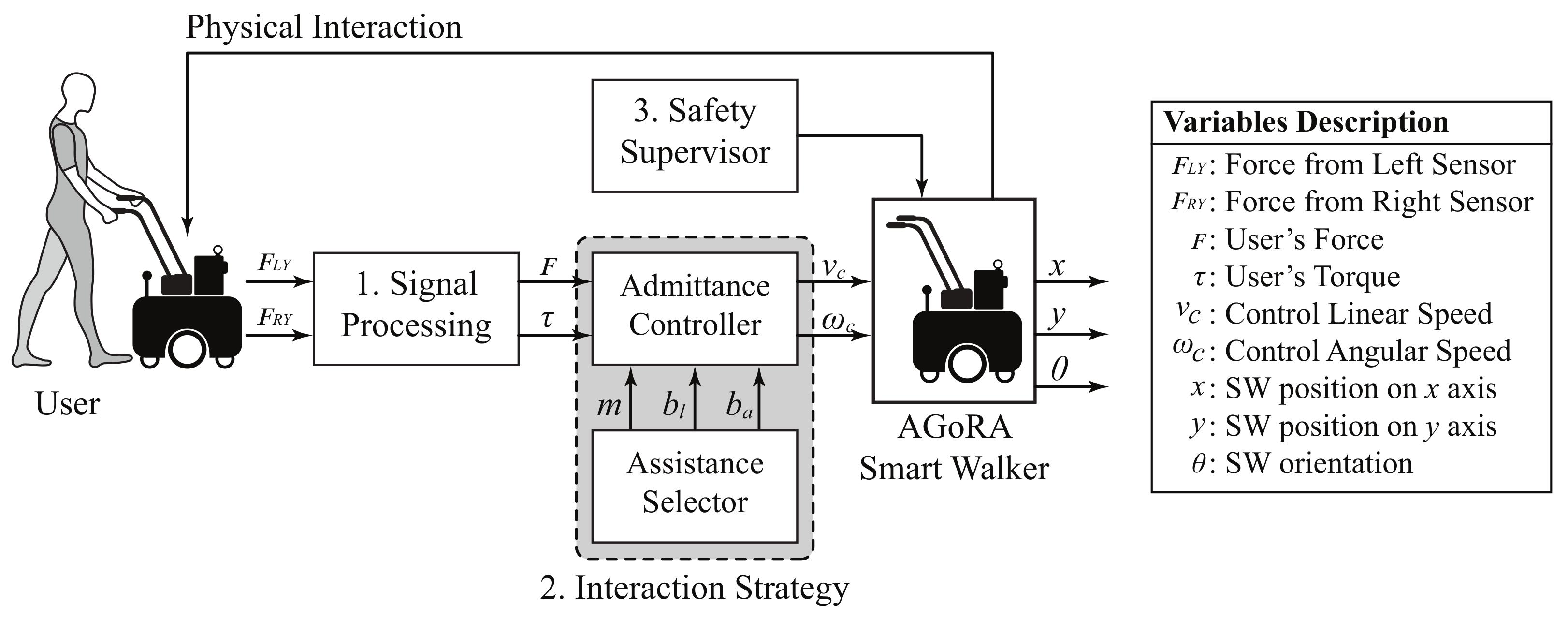
14]. On the one hand, regarding the interaction strategies, the users were entirely in control of the walker’s movements in all of them. For the assistive (AM) and resistive (RM) modes, an admittance controller was used to generate angular and linear speeds by taking the force and torque exerted by the users on the device. For the passive mode (PM), the walker’s speed controller and brakes were disabled, and it was meant to be operated as a conventional four-wheeled walker. Thus, under the PM, the user only had to push the device to make it move. Moreover, in terms of users’ safety, the supervisor was only active for the AM and RM, given that it was designed to override the speed controller when hazardous situations are detected. Thus, although the safety supervisor was disabled for the PM, no collisions occurred during trials.
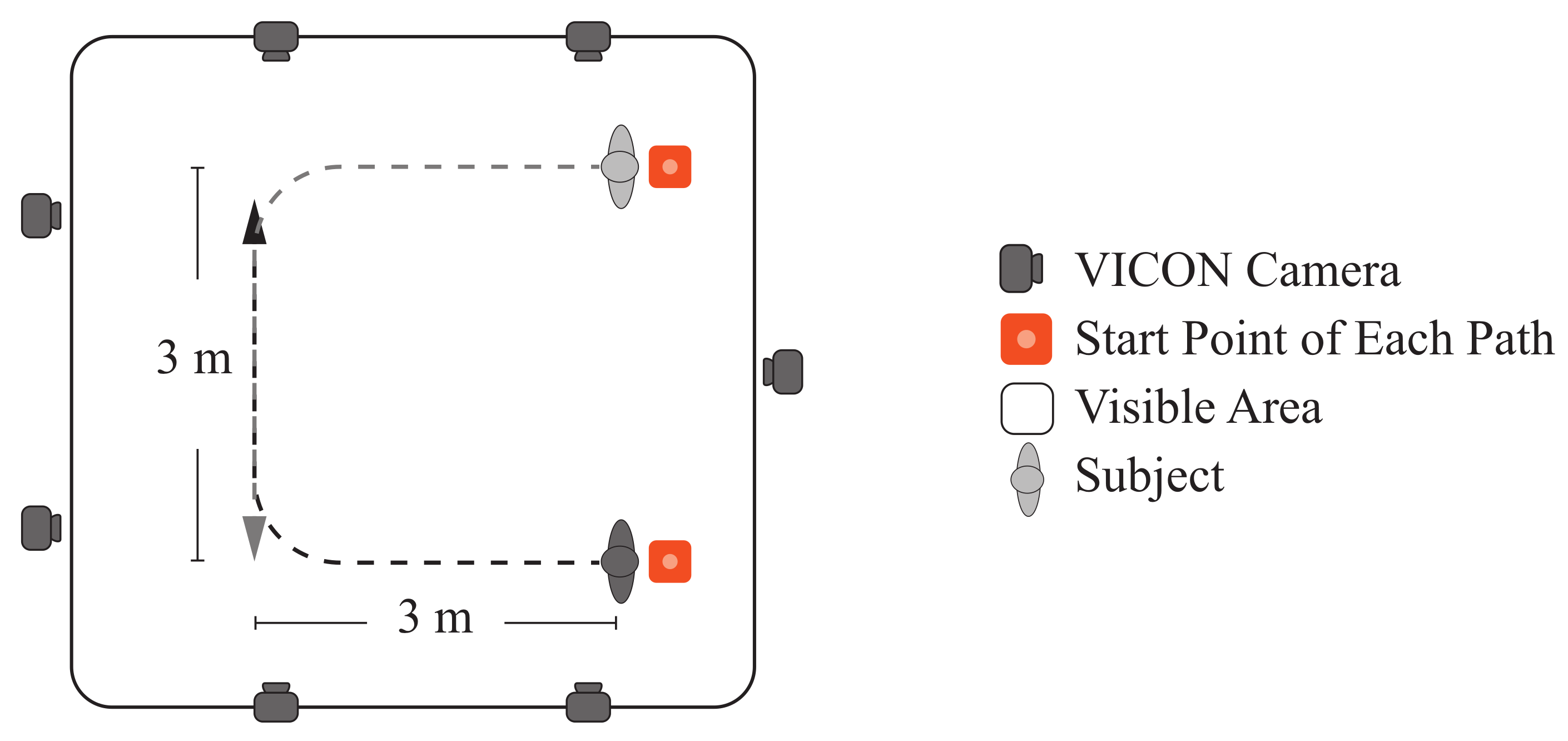
On the other hand, according to the results presented in the previous section, several effects on the physical interaction and kinematics of the users were obtained. Notably, changes in the virtual stiffness programmed in the device (i.e., assistance level) significantly impact users’ performance during trials. Moreover, despite the limited test area (i.e., paths’ area of 3 × 3 m
2), it was sufficient to attain a stable gait. As reported in the literature, between 3.5 and 5.2 steps are required to achieve a steady-state gait [
45]. According to our results, the average number of walking cycles (i.e., two consecutive steps) was around 6.7 to 9.3 cycles, ensuring enough space for the users’ gait to stabilize. Besides, the turning radius in the curves was wide enough to prevent users from having to reduce their speed.
4.1. Physical Interaction Results
Regarding the physical interaction between the users and the SW, four indicators were measured. On the one hand, the user’s mean force exerted was estimated during trials for each assistance mode. As reported in
Table 3, more significant efforts were required from the user to handle the device during the resistive mode (RM). In contrast, the assistive mode (AM) allowed the most effortless interaction, as the mean exerted force by the users was lower than in passive mode (PM) and RM. This outcome indicated that the proposed impedance configurations permitted to have the expected behavior for assisting the subject. Moreover, by analyzing the posthoc tests results presented in
Table 4, it can be seen that this indicator exhibited significant differences for all the pairwise comparisons (
). These results might suggest that the proposed assistance levels allowed us to provide completely different dynamic responses on the AGoRA Smart Walker. In the same manner, the peak force values exhibited similar behavior. This indicator measures the initial contact between the user and the SW, and it estimates how difficult it is to start walking with the device. In this case, the highest value was also registered for the RM and the lowest value was obtained with the AM.
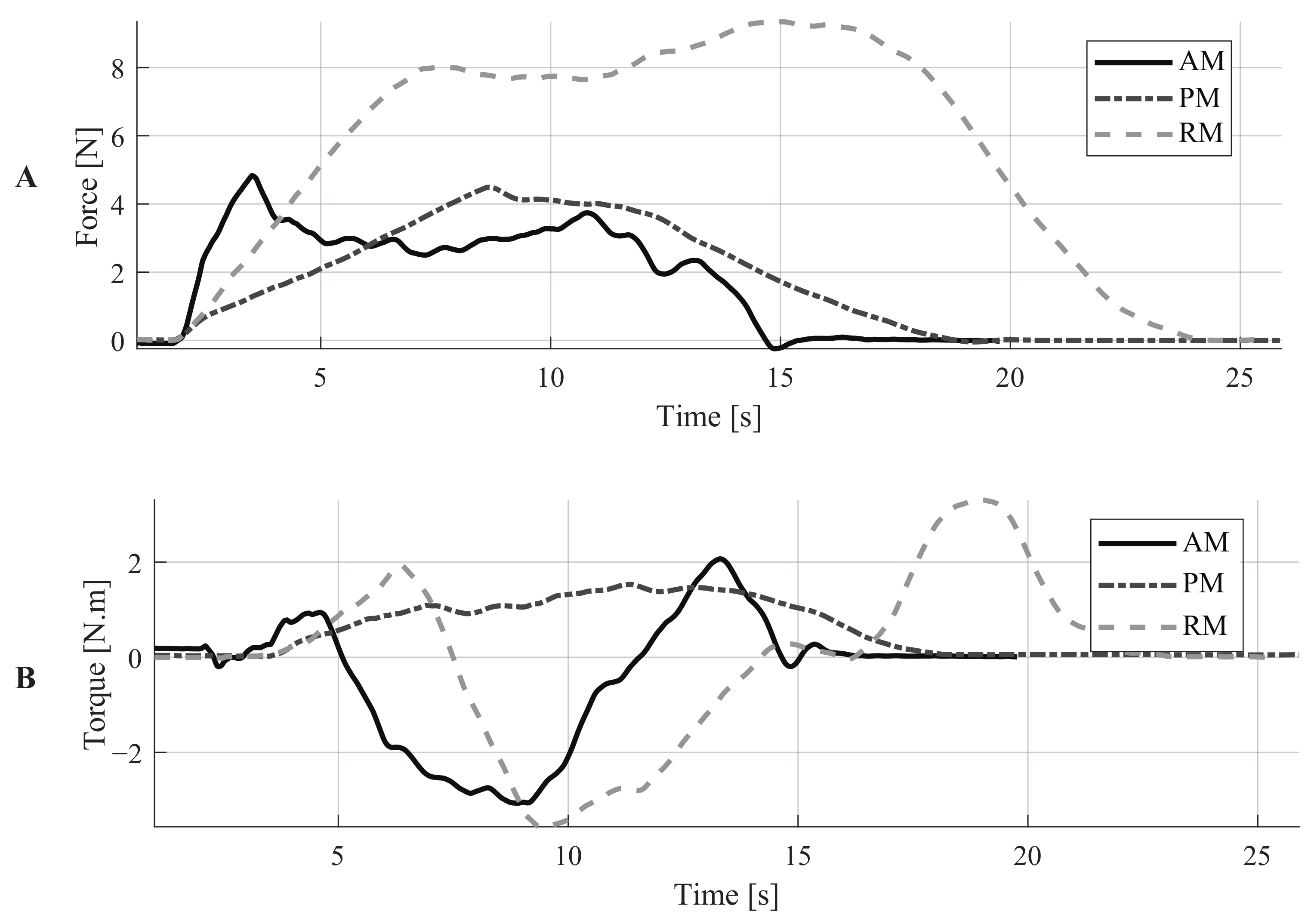
An illustration of these parameters can be found in
Figure 5A, where the force signals of a representative subject are shown. These signals describe an interesting outcome related to the initial force required to move the device. Comparing the AM and the PM, the peak force is higher with the AM. However, the required force to keep the device moving is lower for the AM than for the PM. The admittance controller explains this outcome as it models the walker as a dynamic mass-damping system. In this way, it is possible to make the smart walker feel more lightweight with the virtual mass. Moreover, the damper prevents the propagation of the natural oscillations of gait to the walker [
19,
46]. The combined effect of these elements induces inertia that must be overcome by the user to start walking. However, these elements also ensure that the walker’s movement can be maintained with less effort compared to the PM. In a real application, this behavior makes the AGoRA walker suitable for providing stability to users and assisting users’ gait without requiring as much effort as in the PM.
On the other hand, the mean and peak torque values were also estimated. Regarding the mean torque, significant differences were found for all the assistance levels. Moreover, by analyzing the magnitudes of this parameter, the highest mean torque values were obtained with the RM and the lowest ones with the PM. These results confirm the fact that the SW was virtually more challenging to handle with RM. Regarding the peak torque parameter, similar results were obtained. Significant differences were found for all the assistance levels. The highest values were obtained with the RM and the lowest ones with PM. Moreover, it can also be noted that the standard deviation values were higher with the RM, for both mean and peak torque parameters. This suggests that how users maneuvered the SW was more variable with this level of assistance.
Similar studies to this work have been reported by [
30,
31,
47]. Specifically, ref. [
47] implemented several motion control algorithms based on impulse force information. Moreover, this study evaluated the comfortableness of such control strategies. This study concluded that users prefer to interact with devices that provide good maneuverability, require small forces to move, and ensure safety [
47]. Although this study analyzed multiple sets of control parameters, no resistive mode was evaluated. Moreover, no kinematic information was reported. Regarding the work presented by [
31], the effects of multiple assistive and resistive forces were addressed. The authors reported using foot-switches for gait analysis purposes, finding that cadence, stride length, and double support phase were affected [
31]. This study did not measure the interaction force with users, and thus the movement of the device was not based on users’ intention (i.e., which might lead to hazardous situations). Moreover, applying constant assistive or resistive forces could hinder the implementation in real scenarios. Finally, a dynamic modulation strategy for an admittance controller was proposed by [
30]. In this study, the parameters of the controller were modified to guide users through the desired path. Although this controller is suitable for assisted navigation purposes, the effects on users’ kinematics were not reported.
4.2. Kinematic and Additional Results
Using the information captured by the motion analysis system, several indicators of users’ lower-limb kinematics were estimated (See
Table 5).
On the one hand, the users’ and SW’s speeds were registered for all the assistance levels. Regarding the users’ speed, the RM induced the lowest values (
m/s), mainly because with this configuration the SW opposed the users’ intentions to move. The highest speed values (
m/s) were reached under the unassisted mode (UM). Particularly, the users reduced their walking speed to
,
, and
of their unassisted speed, with the AM, PM, and RM, respectively. Moreover, statistical tests suggested significant differences for all pairwise comparisons of the users’ speed (See
Table 6). This outcome suggests that each assistance level could provide a completely different walking behavior of users. Furthermore, the gait speeds obtained in this work are slightly different from those from the literature evidence. Particularly, several studies report walking speeds ranging from 0.9 to 1.25 m/s [
28,
31]. Thus, the AGoRA Smart Walker allows slower speeds than the average unassisted walking speed [
48]. However, the AGoRA Walker is a rehabilitation device aimed at being used in clinical scenarios, where medical staff often require slower and controlled speeds to correct inappropriate gait patterns [
48].
Regarding the SW motion, the linear speed showed similar behavior to users’ speed, where the lowest values were obtained with the RM (See
Table 5). This parameter also exhibited significant differences between all the assistance levels. The SW’s angular speed exhibited similar behavior. Significant differences were obtained for all pairwise comparisons (See
Table 6). These outcomes also support the fact that each assistance level provides completely different walking behaviors for the users.
On the other hand, gait parameters such as cadence, cycle duration, and the number of cycles were also calculated. The differences between all the assistance levels were found to be statistically significant for these parameters (See
Table 6). Regarding cadence, literature evidence suggests that the users’ cadence in this study was nearly
of the average cadence during unassisted walking in healthy adults [
49]. This discrepancy might be supported by the fact that this work’s experimental environment was considerably smaller to reach average gait speeds, and thus average cadences [
31]. The lowest cadence was obtained with the RM, and this outcome is supported by the most prolonged gait cycles also obtained with the RM (See
Table 5). The RM induced more step cycles, thus it can be deduced that shorter steps were obtained under the RM.
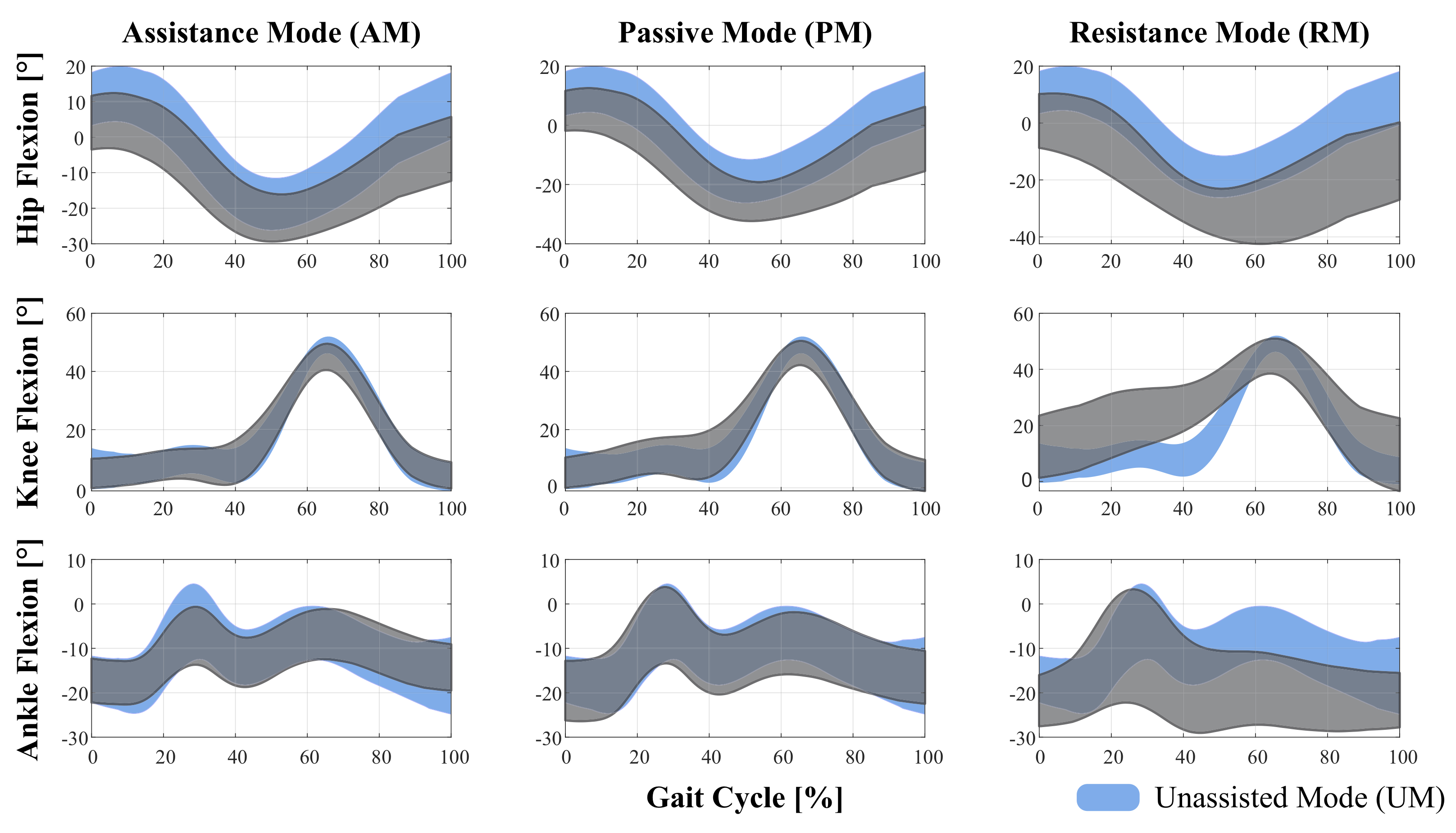
In terms of the effects of the assistance levels on the lower-limb kinematics chain, the range of motion (ROM) was calculated for hip, knee, and ankle joints in the sagittal plane (See
Table 5). Moreover, a comparison of such flexion angles with the unassisted mode is shown in
Figure 6. Regarding hip joint, significant differences were found for nearly all pairwise comparisons (See
Table 6). Particularly, no differences were found for AM vs. PM and PM vs. UM comparisons. Reductions of
, and
of the unassisted ROM were obtained for the AM and PM, respectively. However, an increase of
was obtained for the RM. This result might suggest that when the device opposes the users’ movement intention, they compensate their motion with slower and wider walking patterns, to exert a higher impulse force (i.e., higher forces along the
y-axis, see
Table 3). Furthermore, by analyzing the hip flexion curves presented in
Figure 6, it can be noted that for all assistance levels a reduction of the initial flexion angle occurred in comparison to the UM. Such reduction could be caused by compensation on the trunk inclination angle during walker-assisted gait (See
Figure 6).
Regarding the knee joint, the ROM was smaller than the UM for all the assistance levels provided by the SW. As described in
Table 6, significant differences were found between each assistance mode and UM, whilst no significant differences were found for AM vs. PM. Regarding the ankle joint, the PM and RM induced increases in the range of motion of this joint (See
Table 5). This result also supports the fact that, when users interact with the SW, they tilt the trunk and lower limbs to generate greater impulse forces on the device (See
Figure 6). In this sense, it can be noted that the ankle flexion was higher with the RM (
°). These results suggest that RM is the level of assistance that most affected the users’ gait pattern.
In addition to the above, to better understand the behavior of users’ trunk kinematics, the trunk’s angle was estimated along the sagittal plane for all the assistance levels. Specifically, this angle was calculated using the ground plane as a reference, so that a person completely standing would have a 90° angle. Significant differences were found between the assistance levels. Regarding the outcomes of pairwise comparisons, significant differences were found between all modes compared to the RM. Moreover, increases of , , in trunk’s angle were found for AM, PM, and UM, compared to the RM. This outcome suggests that users tilted the most during the resistive behavior of the Smart Walker.
An additional parameter related to the trial duration was also calculated. As expected, the RM’s trials were the longest ones, and the UM trials were the shortest ones (See
Table 5). Moreover, significant differences were found for all pairwise comparisons, supporting the fact that each assistance level provides a completely different interaction with the SW (See
Table 6).
In terms of safety provision during each of the assistance levels, several aspects are worth mentioning. In particular, Pervez et al., proposed a danger index to estimate user’s safety during mobility assistance [
50]. Even though this study does not calculate such indicators, it avoids most of the unsafe situations highlighted in Pervez et al., On the one hand, it is pointed out that for safe assistance there should not be any appreciable speed mismatch between the assistive robot and the user. All the assistance levels proposed in this work guarantee that the smart walker moves at the desired speed of the user. Even in the RM when the smart walker is harder to push, the speed of the user is adjusted to a slower velocity that matches the smart walker’s speed. Regarding obstacles management, the danger index formulation suggests that the robot should not be very close to obstacles nor collide with them. In this case, the safety supervisor maintains the smart walker away from obstacles, as it limits the speed of the walker when approaching an obstacle. This safety condition is not guaranteed in the passive mode, as the brakes and motors are completely disabled. Additionally, the danger index also considers vibrations and jerks. In these cases, the AGoRA smart walker uses an admittance controller that acts as a low pass filter, mitigating any vibrations or jerks.
Finally, although this work was performed on healthy subjects, it is expected that, when testing the assist levels on patients with gait limitations, similar behaviors in kinematic and physical parameters will be obtained. This means that, regardless of the gait condition, the RM will be harder to interact with, and thus patients will exhibit slower gait patterns and increased interaction forces. Moreover, as previously reported in the literature, it is expected that older adult patients or patients with gait dysfunctions will present slower gait patterns in all modes, and will have the less muscular capacity to exert forces on the device [
51,
52,
53].
4.3. Final Remarks and Future Works
One of the main findings of this study is related to the kinematic and interaction parameters during the resistive mode (RM). Although the RM opposes the user’s intention to move, it might induce muscular training during rehabilitation processes; the level of resistance could be configured to meet each user’s specific needs. This assistance level also induces slower gait patterns compared to the reported studies in the literature. However, these could be interpreted as a safety strategy, where slower gait patterns might help users to avoid collisions and stumbling during walking. Additionally, the force data gathered during the RM provided insights into possible applications of muscular training.
This study was carried out employing the AGoRA Smart Walker, which is mounted on a commercial robotic platform. This selection was made as the Human–Robot Interface of this assistive device was validated in a previous study with healthy subjects [
19]. Moreover, this platform can provide enough safety constraints to guarantee users natural and proper interaction.
One of the limitations of this study is that it lacks EMG information that supports these findings related to physical interaction under the RM. Moreover, it should also be noted that a limitation of this research is the sample size and the participation of only healthy subjects. However, this study is the first approach to the use of controllers with different levels of assistance in walker-assisted gait, and further analyses are required in populations with gait problems, such as older adults or patients with neurological conditions.
Regarding the behavior of the assistive (AM) and the passive modes (PM), they may be useful in patients with lower assistance requirements, as the device allows faster and less controlled movements. However, considering that, during the PM, no speed controller is active, hazardous situations might occur as neither safety supervisor is active. During this mode, the user is completely in control of the smart walker motion.
By comparing the AM and PM behavior, AM can be beneficial to users as it allows the dynamics of the device to be removed. Specifically, the AGoRA Walker is a device mounted on a heavy commercial robotic platform. Thus the implementation of the admittance controller facilitates the user’s interaction with the device. Specifically, the smart walker can be configured to render a lightweight (i.e., as the AM) or bulky device (i.e., as the RM) by setting small or large values on the virtual mass parameter of the admittance controller. It has been reported that these modifications could be suitable to assist activities of daily living, like walking up and down on-ramps using a smart walker [
13]. To validate the performance, safety, and effects of the interaction strategies, this study was conducted on a group of healthy subjects, before their deployment in a clinical setting. Moreover, as reported by several related works, the implementation of assistive and resistive strategies might be useful to provide guidance and gait re-training in clinical scenarios [
30,
31,
32]. In particular, the proposed strategies in this work can be easily adapted to cognitive interaction strategies (e.g., assisted navigation) where the smart walker modifies its virtual stiffness to provide feedback in path following, guidance, and navigation tasks.
In addition to the above, it is worth mentioning that the paradigm of multiple assistance levels is not exclusive to walker-assisted gait. In particular, these strategies can be easily implemented in other assistive devices such as exoskeletons or hybrid devices [
54,
55,
56]. Finally, future works will address the assessment of these interaction strategies in a clinical scenario with pathological patients or older people. In this work, the RM was configured according to the weight of the users. Therefore, future works will also address the development of a multivariate model to determine the correlation between the users’ weight and the ability to maneuver the SW. Future studies will also assess more complex walking tasks, including longer and more challenging paths and tasks.


 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}