4.1. Meal Detection and Estimation Performance
In this section, we report the results on the performance of the framework in detecting and estimating the unannounced meals in the simulation scenario. The performance is reported on each mealtime and for the snacks.
Table 1 shows the meal detection performance of the meals and snacks at different mealtimes. The average breakfast meal size is of moderate size (70 ± 7 g). The method obtains a precision 86 ± 7% and a recall 90 ± 5%. In terms of detection time these meals are flagged at 38 ± 13 min. The lunch meals are the largest size considered in this study at 100 ± 10 g. At lunchtime, the proposed method detects lunch with 98 ± 2% precision and 97 ± 3% recall. This detection is completed in 37 ± 15 min. Finally, for dinner, the average size during this mealtime is 80 ± 7 g which can also be considered moderate-sized. For this proposed method, we detect dinner meals at 94 ± 5% precision and 89 ± 4% recall. The snacks ingested after lunch are of a relatively smaller size at 30 ± 3 g. Although the precision is high at 97 ± 5%, the recall is relatively low at 24 ± 15%. In addition, the detection time is 41 ± 23 min. The observation is made that the recall and detection time performance is dependent on the size of the meal, where small meals (snacks) show the worst performance and large meals (lunch) show the best performance, with moderately sized meals (breakfast and dinner) showing intermediate performance. On the other hand, we notice that the performance in terms of precision is consistently high (86–98%) across different meal sizes.
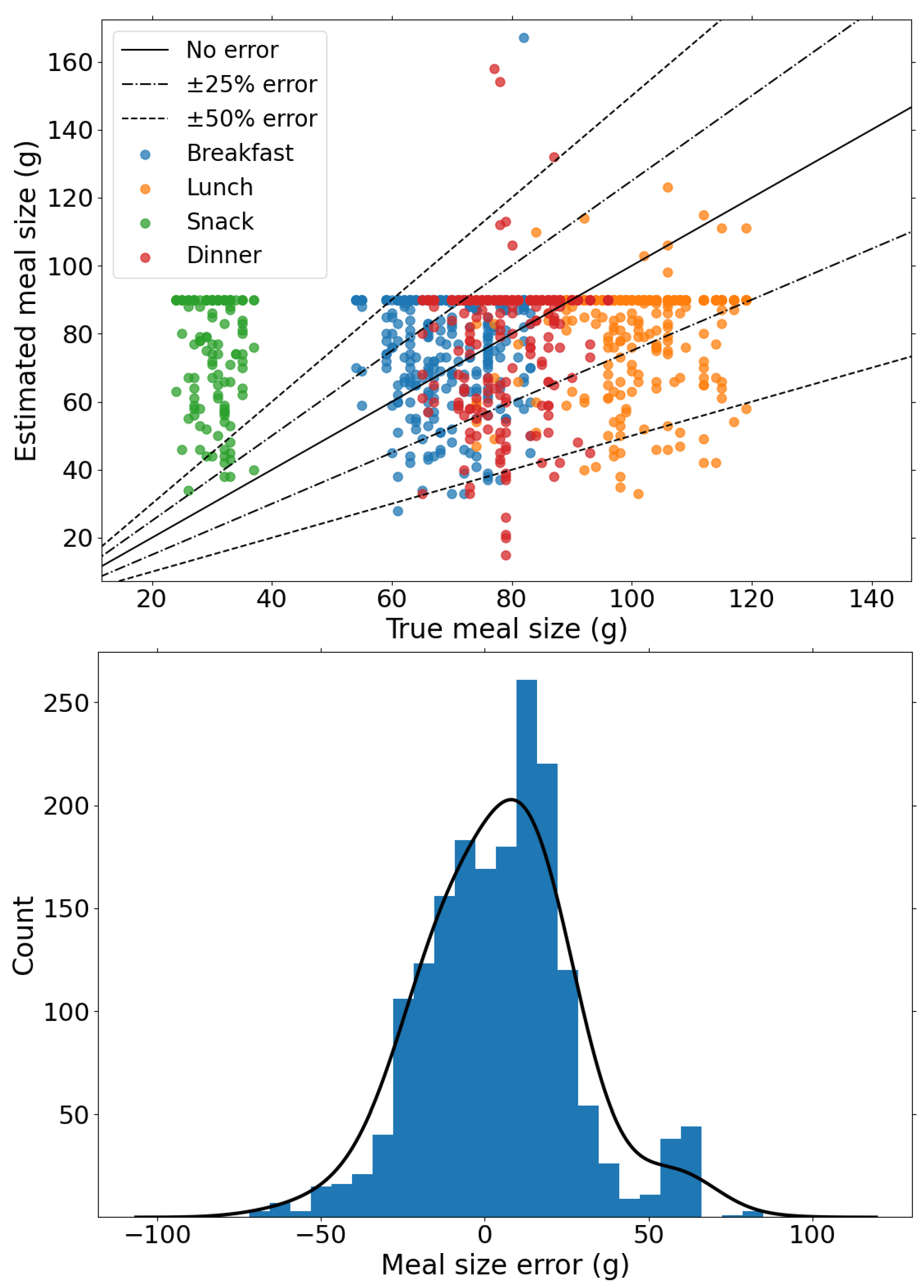
Following the evaluation of the meal detection performance, we analyse the performance of the proposed method on meal estimation.
Figure 4 shows the comparison of the estimated meal size and the actual meal sizes and shows the distribution of estimation errors in meals. First, we note that carbohydrate estimation is performed in relation to the median glucose level trajectory which have varying errors and thus can lead to under- and overestimation of meals. In total, 80% of the estimated CHO have a estimation error within 25 g, whereas only 6% of detected CHO is larger than 50 g, of which snacks represent the majority. The distribution of the estimation errors, shown in
Figure 4, shows that the proposed method is slightly biased towards overestimation with an average error 18 ± 15 g. This justifies applying the weight to the mealtime insulin bolus for the insulin delivery strategy to mitigate postprandial hyperglycaemia without significantly increasing hypoglycaemia risk.
4.2. Closed-Loop Glucose Control
In this section, we report results of the performance of the BiAP controller with different configurations. The different configurations used in this study are described below:
BiAP-NMA: In this configuration, meals are not announced prior to the selected mealtimes for bolus priming. The controller is therefore only able to respond to the postprandial glucose excursion through feedback from the CGM signal. Since there is no external input from the user for meal announcement this is a fully closed-loop configuration.
BiAP-MD: This is a fully closed-loop configuration that corresponds to the BiAP controller with the meal detection and estimation module incorporated. In this configuration, the insulin bolus is delivered as explained in the closed-loop insulin delivery.
BiAP-MA: This hybrid closed-loop configuration corresponds to the controller with meal announcement included. Meal announcement involves the individual estimating the meal size and input this in the controller in order to deliver a preprandial insulin bolus. The behaviour of the individual is modelled as earlier described to account for carbohydrate misestimation, missed boluses and late boluses.
The performance of the controllers in enabling tight glycaemic control is reported in
Table 2. BiAP-MD and BiAP-NMA are the two closed-loop controllers that are described as fully closed-loop. A comparison of the performance between these two controllers reveals that the meal detection and estimation algorithm improves the control of postprandial hyperglycaemia. This is evident from the significant reduction in time spent in hyperglycaemia (
TAR = −4.2%,
) and lower risk of hyperglycaemia (
HBGI = −0.8%,
). Overall, BiAP-MD reports a significantly lower mean glucose level (−4.4 mg/dL,
) than the BiAP-NMA controller and provides relatively tighter glycaemic control (
TIR = +3.9%,
). Finally, this is accomplished without a statistically significant increase in time spent in hypoglycaemia (
TBR = +0.1%,
) or risk of hypoglycaemia (
LBGI = +0.1,
).
A further comparison is made between the BiAP-MA and BiAP-MD controller. The first observation is that BiAP-MA has lower mean blood glucose level (−6.8 mg/dL,
) than BiAP-MD. In addition, we see significant improvement in tight glycaemic control with BiAP-MA over the proposed BiAP-MD controller: increased time in range (+6.9% mg/dL,
), reduced time spent in hyperglycaemia (−7%,
), and reduced associated risk of hyperglycaemia (−1.1,
). This difference in performance highlights the advantage of the individual pre-bolusing for meals over automatic meal detection and estimation. The accumulation of errors in meal announcements may lead to an increase in time spent in hypoglycaemia (+0.1%,
) and associated risk of hypoglycaemia (+0.1%,
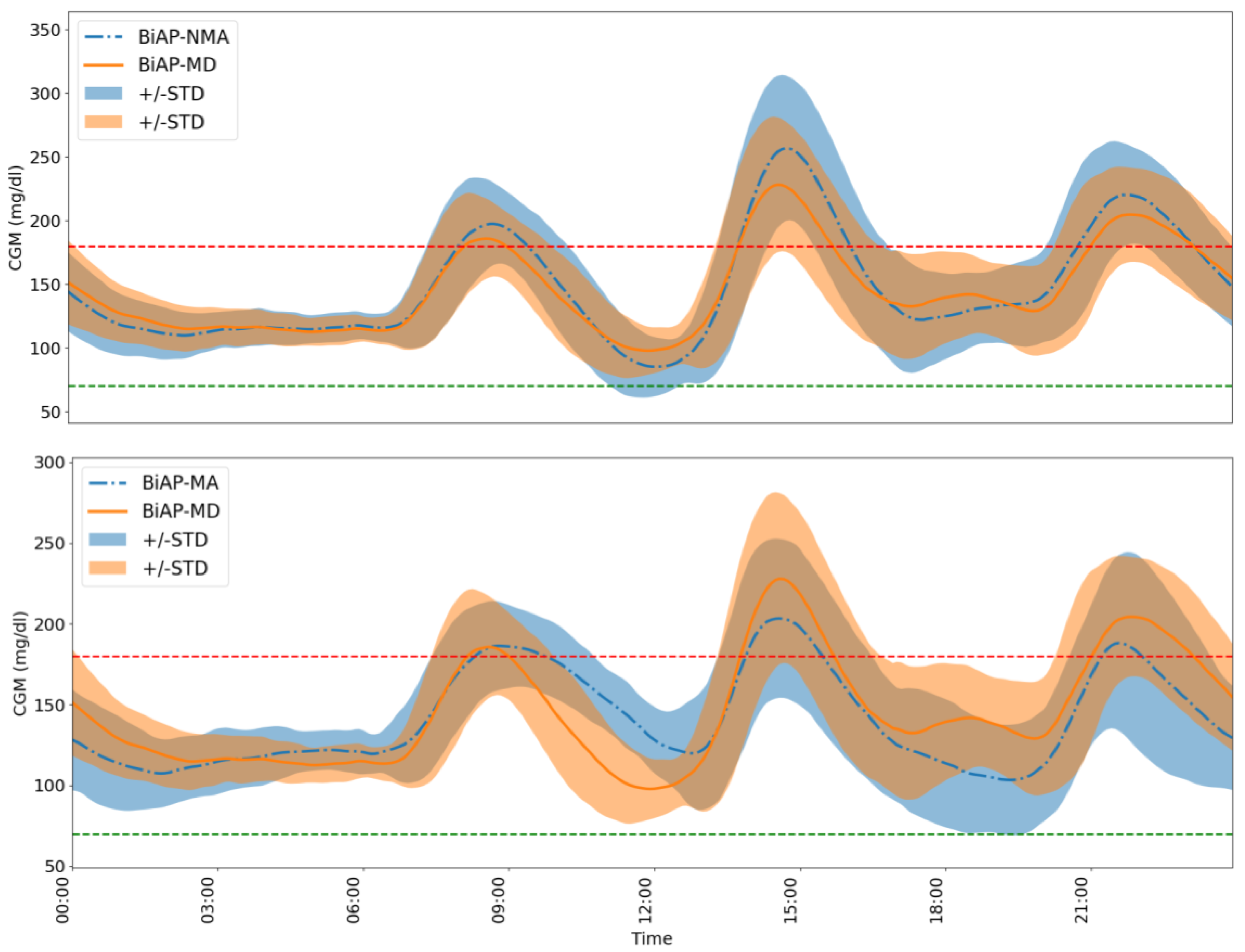
), however, these are not observed to be statistically significant. The difference in 24 h glucose profiles of an individual using the BiAP controller with the different configurations over the 2-month period is highlighted in
Figure 5.
An analysis of the CVGA plots on the population level as shown in
Figure 6 reveals a difference in the quality of glycaemic control for the different configurations. The first comparison we consider is between the fully closed-loop BiAP controllers (BiAP-NMA and BiAP-MD). The general numerical assessment shows that both configurations demonstrate a similar performance with 90% in Zone A+B and 10% in Lower D zone. In detail, however, the observation seen in
Table 2 BiAP-MD exhibits tighter glycaemic control than BiAP-NMA is further buttressed in this plot. In total, 10% of BiAP-MD markers were observed in the Upper B zone which is an improvement in comparison to 20% of BiAP-NMA markers, therefore displaying a lesser tendency towards benign control deviations into hyperglycaemia.
On the other hand, for the second comparison we consider quality of glycaemic control between BiAP-MA (hybrid closed-loop configuration) and BiAP-MD (fully closed-loop configuration). BiAP-MA shows marginally worse quality control with 80% of the population in Zone A+B compared to BiAP-MD with 90% in Zone A+B. As seen in
Table 2 earlier, BiAP-MA provides tighter glycaemic control that BiAP-MD, however, this can is more likely to lead to more instances of hypoglycaemia particularly when meals are overestimated and delayed. This would explain the higher instance of individuals from the population in Lower D zone and therefore a failure to deal with hypoglycaemia during control.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}