


Dependence of Skin-Electrode Contact Impedance on Material and Skin Hydration


Abstract
:1. Introduction
2. Materials and Methods
2.1. Electrode Material
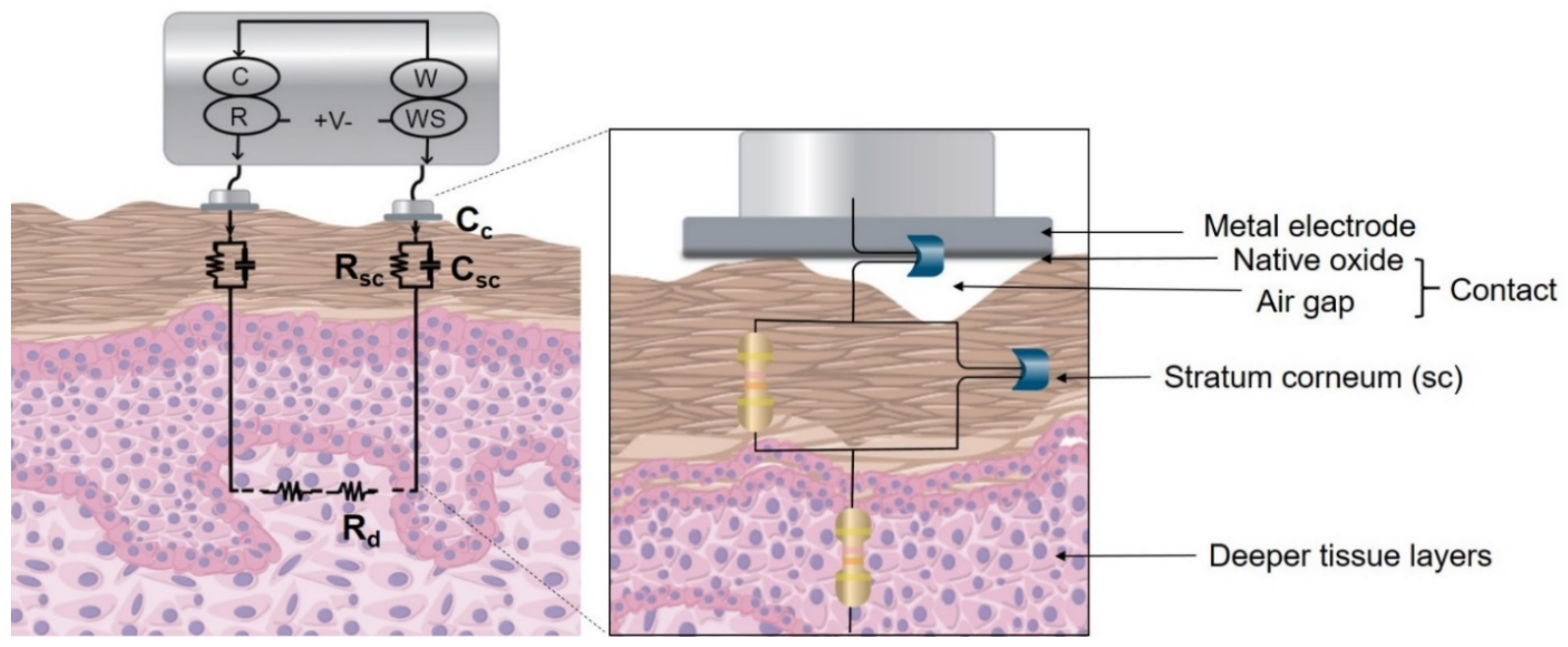
2.2. Skin-Electrode Impedance Equivalent Model for Dry Electrodes
2.2.1. Impedance Measurements on Phantom
2.2.2. Development of Model
2.3. Normative Subject Testing
2.3.1. In Vivo Skin-Impedance Measurements
2.3.2. Electrocardiogram Acquisition
2.3.3. Signal Processing and Analysis
3. Results
3.1. Electrode Material Characterization
3.2. Skin-Electrode Contact Impedance Model Parameters
3.3. Normative Subject Testing
3.3.1. In Vivo Skin-Electrode Contact Impedance
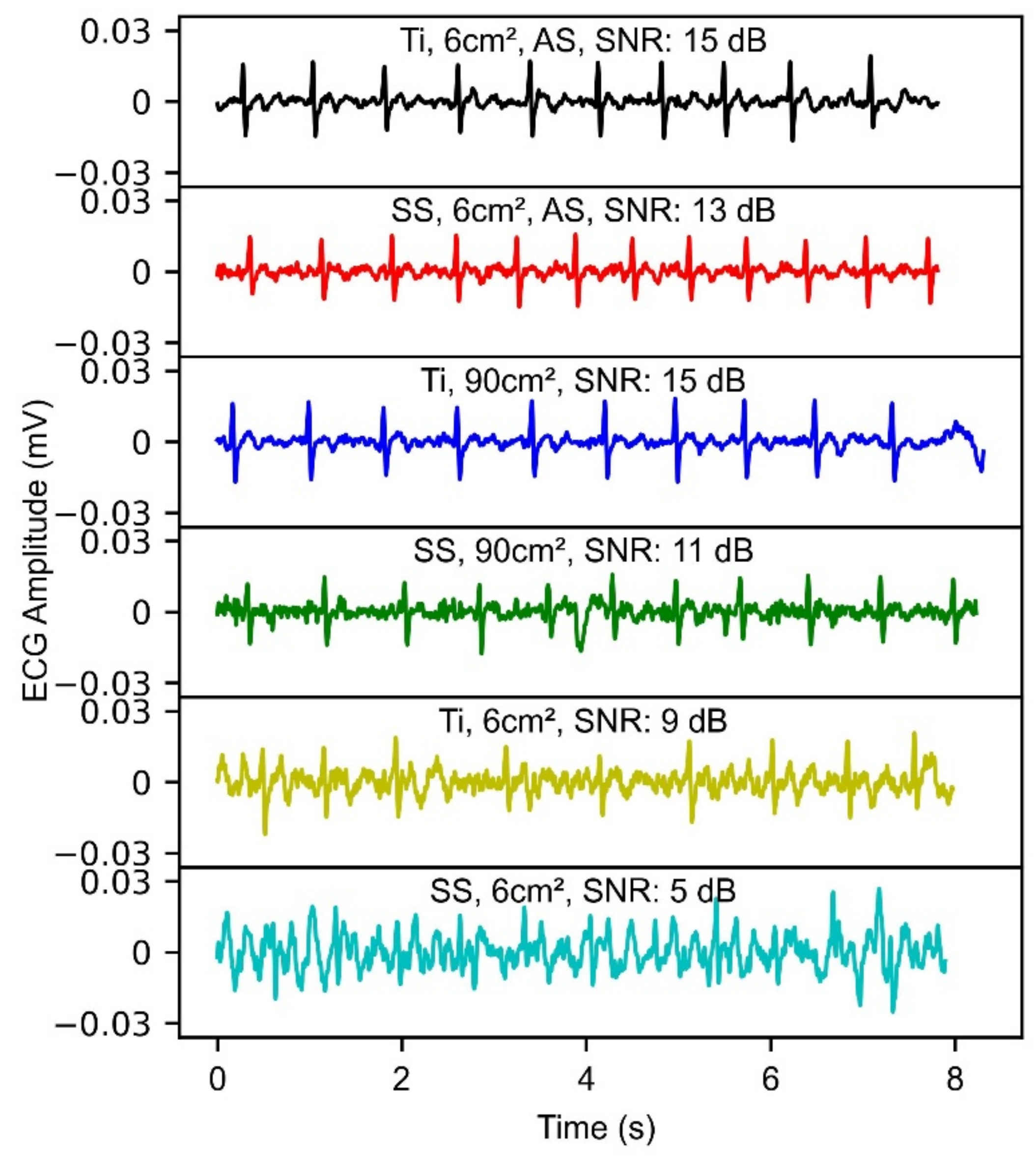
3.3.2. ECG Demonstration
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Steinhubl, S.R.; Waalen, J.; Edwards, A.M.; Ariniello, L.M.; Mehta, R.R.; Ebner, G.S.; Carter, C.; Baca-Motes, K.; Felicione, E.; Sarich, T.; et al. Effect of a Home-Based Wearable Continuous ECG Monitoring Patch on Detection of Undiagnosed Atrial Fibrillation. JAMA 2018, 320, 146–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serhani, M.A.; El Kassabi, H.T.; Ismail, H.; Navaz, A.N. ECG Monitoring Systems: Review, Architecture, Processes, and Key Challenges. Sensors 2020, 20, 1796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geddes, L.A. Historical evolution of circuit models for the electrode-electrolyte interface. Ann. Biomed. Eng. 1997, 25, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-H.; De Beeck, M.O.; Vanderheyden, L.; Carrette, E.; Mihajlović, V.; Vanstreels, K.; Grundlehner, B.; Gadeyne, S.; Boon, P.; Van Hoof, C. Soft, Comfortable Polymer Dry Electrodes for High Quality ECG and EEG Recording. Sensors 2014, 14, 23758–23780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huigen, E.; Peper, A.; Grimbergen, C.A. Investigation into the origin of the noise of surface electrodes. Med. Biol. Eng. Comput. 2002, 40, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Murphy, B.; Scheid, B.; Hendricks, Q.; Apollo, N.; Litt, B.; Vitale, F. Time Evolution of the Skin–Electrode Interface Impedance under Different Skin Treatments. Sensors 2021, 21, 5210. [Google Scholar] [CrossRef] [PubMed]
- Lobodzinski, S.M. ECG Instrumentation: Application and Design. In Comprehensive Electrocardiology; Macfarlane, P.W., van Oosterom, A., Pahlm, O., Kligfield, P., Janse, M., Camm, J., Eds.; Springer: London, UK, 2010; pp. 427–480. [Google Scholar] [CrossRef]
- Geddes, L.A.; Baker, L.E. Principles of Applied Biomedical Instrumentation, 3rd ed.; John Wiley & Sons: New York, NY, USA, 1989. [Google Scholar] [CrossRef]
- Birgersson, U.; Åberg, P.; Nicander, I.; Ollmar, S.; Birgersson, E. Non-invasive bioimpedance of intact skin: Mathematical modeling and experiments. Physiol. Meas. 2010, 32, 1–18. [Google Scholar] [CrossRef]
- Schmidt, R.N.; Lisy, F.J.; Skebe, G.G.; Prince, T.S. Dry Physiological Recording Electrode. U.S. Patent 6,785,569, 31 August 2004. [Google Scholar]
- Albulbul, A. Evaluating Major Electrode Types for Idle Biological Signal Measurements for Modern Medical Technology. Bioengineering 2016, 3, 20. [Google Scholar] [CrossRef]
- Chlaihawi, A.A.; Narakathu, B.B.; Emamian, S.; Bazuin, B.J.; Atashbar, M.Z. Development of printed and flexible dry ECG electrodes. Sens. Bio-Sens. Res. 2018, 20, 9–15. [Google Scholar] [CrossRef]
- An, X.; Tangsirinaruenart, O.; Stylios, G.K. Investigating the performance of dry textile electrodes for wearable end-uses. J. Text. Inst. 2018, 110, 151–158. [Google Scholar] [CrossRef]
- Meziane, N.; Yang, S.; Shokoueinejad, M.; Webster, J.G.; Attari, M.; Eren, H. Simultaneous comparison of 1 gel with 4 dry electrode types for electrocardiography. Physiol. Meas. 2015, 36, 513–529. [Google Scholar] [CrossRef] [PubMed]
- Anusha, A.S.; Preejith, S.P.; Akl, T.J.; Joseph, J.; Sivaprakasam, M. Dry Electrode Optimization for Wrist-based Electrodermal Activity Monitoring. In Proceedings of the 2018 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Rome, Italy, 11–13 June 2018. [Google Scholar] [CrossRef]
- Peng, S.; Xu, K.; Chen, W. Comparison of Active Electrode Materials for Non-Contact ECG Measurement. Sensors 2019, 19, 3585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, G.; Wang, S.; Duan, Y.Y. Towards conductive-gel-free electrodes: Understanding the wet electrode, semi-dry electrode and dry electrode-skin interface impedance using electrochemical impedance spectroscopy fitting. Sens. Actuators B Chem. 2018, 277, 250–260. [Google Scholar] [CrossRef]
- Conn, N.J.; Schwarz, K.Q.; A Borkholder, D. Nontraditional Electrocardiogram and Algorithms for Inconspicuous In-Home Monitoring: Comparative Study. JMIR mHealth uHealth 2018, 6, e120. [Google Scholar] [CrossRef] [PubMed]
- Goyal, K.; Borkholder, D.A.; Day, S.W. A biomimetic skin phantom for characterizing wearable electrodes in the low-frequency regime. Sens. Actuators A Phys. 2022, 340, 113513. [Google Scholar] [CrossRef]
- Revilla, R.I.; Wouters, B.; Andreatta, F.; Lanzutti, A.; Fedrizzi, L.; De Graeve, I. EIS comparative study and critical Equivalent Electrical Circuit (EEC) analysis of the native oxide layer of additive manufactured and wrought 316L stainless steel. Corros. Sci. 2020, 167, 108480. [Google Scholar] [CrossRef]
- Bishop, H.; Rivière, J.; Coad, J. Auger spectroscopy of titanium. Surf. Sci. 1971, 24, 1–17. [Google Scholar] [CrossRef]
- Taji, B.; Chan, A.D.C.; Shirmohammadi, S. Effect of Pressure on Skin-Electrode Impedance in Wearable Biomedical Measurement Devices. IEEE Trans. Instrum. Meas. 2018, 67, 1900–1912. [Google Scholar] [CrossRef]
- Hsu, C.H.; Mansfeld, F. Technical Note: Concerning the Conversion of the Constant Phase Element Parameter Y0into a Capacitance. Corrosion 2001, 57, 747–748. [Google Scholar] [CrossRef]
- Cochran, W.G. The χ2 Test of Goodness of Fit. Ann. Math. Stat. 1952, 23, 315–345. [Google Scholar] [CrossRef]
- Equivalent Circuit Modeling Using the Gamry Electrochemical Impedance Spectroscopy Software. Available online: https://www.gamry.com/application-notes/EIS/equivalent-circuit-modeling-using-the-gamry-eis300-electrochemical-impedance-spectroscopy-software/ (accessed on 6 September 2022).
- Ricciardi, D.; Cavallari, I.; Creta, A.; Di Giovanni, G.; Calabrese, V.; Di Belardino, N.; Mega, S.; Colaiori, I.; Ragni, L.; Proscia, C.; et al. Impact of the high-frequency cutoff of bandpass filtering on ECG quality and clinical interpretation: A comparison between 40Hz and 150Hz cutoff in a surgical preoperative adult outpatient population. J. Electrocardiol. 2016, 49, 691–695. [Google Scholar] [CrossRef] [PubMed]
- Thakor, N.; Webster, J.G.; Tompkins, W.J. Optimal QRS detector. Med. Biol. Eng. Comput. 1983, 21, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Mark, R.G.; Clifford, G.D. Robust heart rate estimation from multiple asynchronous noisy sources using signal quality indices and a Kalman filter. Physiol. Meas. 2007, 29, 15–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castro, I.D.; Varon, C.; Torfs, T.; Van Huffel, S.; Puers, R.; Van Hoof, C. Evaluation of a Multichannel Non-Contact ECG System and Signal Quality Algorithms for Sleep Apnea Detection and Monitoring. Sensors 2018, 18, 577. [Google Scholar] [CrossRef] [Green Version]
- Welch, P.D. The use of fast Fourier transform for the estimation of power spectra: A method based on time averaging over short, modified periodograms. IEEE Trans. Audio Electroacoust. 1967, 15, 70–73. [Google Scholar] [CrossRef] [Green Version]
- Makowski, D.; Pham, T.; Lau, Z.J.; Brammer, J.C.; Lespinasse, F.; Pham, H.; Schölzel, C.; Chen, S.H.A. NeuroKit2: A Python toolbox for neurophysiological signal processing. Behav. Res. Methods 2021, 53, 1689–1696. [Google Scholar] [CrossRef]
- Pei, W.; Zhang, H.; Wang, Y.; Guo, X.; Xing, X.; Huang, Y.; Xie, Y.; Yang, X.; Chen, H. Skin-Potential Variation Insensitive Dry Electrodes for ECG Recording. IEEE Trans. Biomed. Eng. 2016, 64, 463–470. [Google Scholar] [CrossRef]
- He, T.; Clifford, G.; Tarassenko, L. Application of independent component analysis in removing artefacts from the electrocardiogram. Neural Comput. Appl. 2005, 15, 105–116. [Google Scholar] [CrossRef]
- Helmenstine, M. Table of Electrical Resistivity and Conductivity. 2019. Available online: https://www.thoughtco.com/table-of-electrical-resistivity-conductivity-608499 (accessed on 6 September 2022).
- Langevoort, J.; Sutherland, I.; Hanekamp, L.; Gellings, P. On the oxide formation on stainless steels AISI 304 and incoloy 800H investigated with XPS. Appl. Surf. Sci. 1987, 28, 167–179. [Google Scholar] [CrossRef] [Green Version]
- Lausmaa, J. Surface spectroscopic characterization of titanium implant materials. J. Electron. Spectrosc. Relat. Phenom. 1996, 81, 343–361. [Google Scholar] [CrossRef]
- Li, G.; Wang, S.; Duan, Y.Y. Towards gel-free electrodes: A systematic study of electrode-skin impedance. Sens. Actuators B Chem. 2017, 241, 1244–1255. [Google Scholar] [CrossRef]
- Ferrari, L.M.; Ismailov, U.; Greco, F.; Ismailova, E. Capacitive Coupling of Conducting Polymer Tattoo Electrodes with the Skin. Adv. Mater. Interfaces 2021, 8, 2100352. [Google Scholar] [CrossRef]
- Björklund, S.; Ruzgas, T.; Nowacka, A.; Dahi, I.; Topgaard, D.; Sparr, E.; Engblom, J. Skin Membrane Electrical Impedance Properties under the Influence of a Varying Water Gradient. Biophys. J. 2013, 104, 2639–2650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, B.B.; Mulcahey, P.J.; Driscoll, N.; Richardson, A.G.; Robbins, G.T.; Apollo, N.V.; Maleski, K.; Lucas, T.H.; Gogotsi, Y.; Dillingham, T.; et al. A Gel-Free Ti3C2Tx-Based Electrode Array for High-Density, High-Resolution Surface Electromyography. Adv. Mater. Technol. 2020, 5, 2000325. [Google Scholar] [CrossRef]
- FDA-2019-D-1649; Cutaneous Electrodes for Recording Purposes—Performance Criteria for Safety and Performance Based Pathway. U.S. Food and Drug Administration: Silver Spring, MD, USA, 2019.
- Kappenman, E.S.; Luck, S.J. The effects of electrode impedance on data quality and statistical significance in ERP recordings. Psychophysiology 2010, 47, 888–904. [Google Scholar] [CrossRef] [Green Version]
- Chi, Y.M.; Jung, T.-P.; Cauwenberghs, G. Dry-Contact and Noncontact Biopotential Electrodes: Methodological Review. IEEE Rev. Biomed. Eng. 2010, 3, 106–119. [Google Scholar] [CrossRef] [Green Version]
- Boxley, C.J.; White, H.S.; Gardner, C.E.; Macpherson, J.V. Nanoscale Imaging of the Electronic Conductivity of the Native Oxide Film on Titanium Using Conducting Atomic Force Microscopy. J. Phys. Chem. B 2003, 107, 9677–9680. [Google Scholar] [CrossRef]
- Rosenkranz, A.; Reinert, L.; Gachot, C.; Aboufadl, H.; Grandthyll, S.; Jacobs, K.; Müller, F.; Mücklich, F. Oxide Formation, Morphology, and Nanohardness of Laser-Patterned Steel Surfaces. Adv. Eng. Mater. 2015, 17, 1234–1242. [Google Scholar] [CrossRef]
- Balanis, C.A. Advanced Engineerig Electromagnetics; John Wiley & Sons: Hoboken, NJ, USA, 2012. [Google Scholar]
- Löberg, J.; Holmberg, J.P.; Mattisson, I.; Arvidsson, A.; Ahlberg, E. Electronic Properties of TiO2 Nanoparticles Films and the Effect on Apatite-Forming Ability. Int. J. Dent. 2013, 2013, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Qiu, Y.; Thomas, S.; Gupta, R.; Gengenbach, T.; Jones, R.; Birbilis, N. A Surface Study of the Native Oxide upon a Compositionally Complex Alloy. Corrosion 2018, 74, 1312–1317. [Google Scholar] [CrossRef]
- Bergey, G.E.; Squires, R.D.; Sipple, W.C. Electrocardiogram Recording with Pasteless Electrodes. IEEE Trans. Biomed. Eng. 1971, BME-18, 206–211. [Google Scholar] [CrossRef]
- Lopes, C.; Fiedler, P.; Rodrigues, M.S.; Borges, J.; Bertollo, M.; Alves, E.; Barradas, N.P.; Comani, S.; Haueisen, J.; Vaz, F. Me-Doped Ti–Me Intermetallic Thin Films Used for Dry Biopotential Electrodes: A Comparative Case Study. Sensors 2021, 21, 8143. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, L.M.; Ismailov, U.; Badier, J.-M.; Greco, F.; Ismailova, E. Conducting polymer tattoo electrodes in clinical electro- and magneto-encephalography. NPJ Flex. Electron. 2020, 4, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Heikenfeld, J.; Jajack, A.; Rogers, J.; Gutruf, P.; Tian, L.; Pan, T.; Li, R.; Khine, M.; Kim, J.; Wang, J.; et al. Wearable sensors: Modalities, challenges, and prospects. Lab Chip 2018, 18, 217–248. [Google Scholar] [CrossRef] [Green Version]
- Li, G.-L.; Wu, J.-T.; Xia, Y.-H.; He, Q.-G.; Jin, H.-G. Review of semi-dry electrodes for EEG recording. J. Neural Eng. 2020, 17, 051004. [Google Scholar] [CrossRef]
- Liu, J.; Lin, S.; Li, W.; Zhao, Y.; Liu, D.; He, Z.; Wang, D.; Lei, M.; Hong, B.; Wu, H. Ten-Hour Stable Noninvasive Brain-Computer Interface Realized by Semidry Hydrogel-Based Electrodes. Research 2022, 2022, 1–12. [Google Scholar] [CrossRef]
- Li, G.; Wang, S.; Li, M.; Duan, Y.Y. Towards real-life EEG applications: Novel superporous hydrogel-based semi-dry EEG electrodes enabling automatically ‘charge–discharge’ electrolyte. J. Neural Eng. 2021, 18, 046016. [Google Scholar] [CrossRef]
- Searle, A.; Kirkup, L. A direct comparison of wet, dry and insulating bioelectric recording electrodes. Physiol. Meas. 2000, 21, 271–283. [Google Scholar] [CrossRef]
- Park, J.-G.; Lee, S.-H.; Ryu, J.-S.; Hong, Y.-K.; Kim, T.-G.; Busnaina, A.A. Interfacial and Electrokinetic Characterization of IPA Solutions Related to Semiconductor Wafer Drying and Cleaning. J. Electrochem. Soc. 2006, 153, G811–G814. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, Y. Characteristics of skin admittance for dry electrodes and the measurement of skin moisturisation. Med. Biol. Eng. Comput. 1986, 24, 71–77. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Electrode Area | Rd (kΩ) | Rsc (MΩ) | Csc (nF) | Cc (µF) | Goodness of Fit |
|---|---|---|---|---|---|
| 4 cm2 | 1.77 | 1.62 | 151 | 0.68 | 0.017 |
| 9 cm2 | 1.75 | 0.70 | 391 | 1.34 | 0.044 |
| Electrode Material (Phantom Hydration Status) | Rd (kΩ cm2) | Rsc (MΩ cm2) | Csc (nF cm−2) | Cc (nF cm−2) | Goodness of Fit |
|---|---|---|---|---|---|
| Ti (dry) | 9.3 | 6.4 | 41 | 267 | 0.007 |
| SS (dry) | 9.3 | 6.4 | 41 | 114 | 0.031 |
| Ti (hydrated) | 9.3 | 3.0 | 190 | 420 | 0.042 |
| SS (hydrated) | 9.3 | 3.0 | 190 | 224 | 0.035 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goyal, K.; Borkholder, D.A.; Day, S.W. Dependence of Skin-Electrode Contact Impedance on Material and Skin Hydration. Sensors 2022, 22, 8510. https://doi.org/10.3390/s22218510
Goyal K, Borkholder DA, Day SW. Dependence of Skin-Electrode Contact Impedance on Material and Skin Hydration. Sensors. 2022; 22(21):8510. https://doi.org/10.3390/s22218510
Chicago/Turabian StyleGoyal, Krittika, David A. Borkholder, and Steven W. Day. 2022. "Dependence of Skin-Electrode Contact Impedance on Material and Skin Hydration" Sensors 22, no. 21: 8510. https://doi.org/10.3390/s22218510