
An Analysis of Respiration with the Smart Sensor SENSIRIB in Patients Undergoing Thoracic Surgery



Abstract
:1. Introduction
2. Materials and Methods
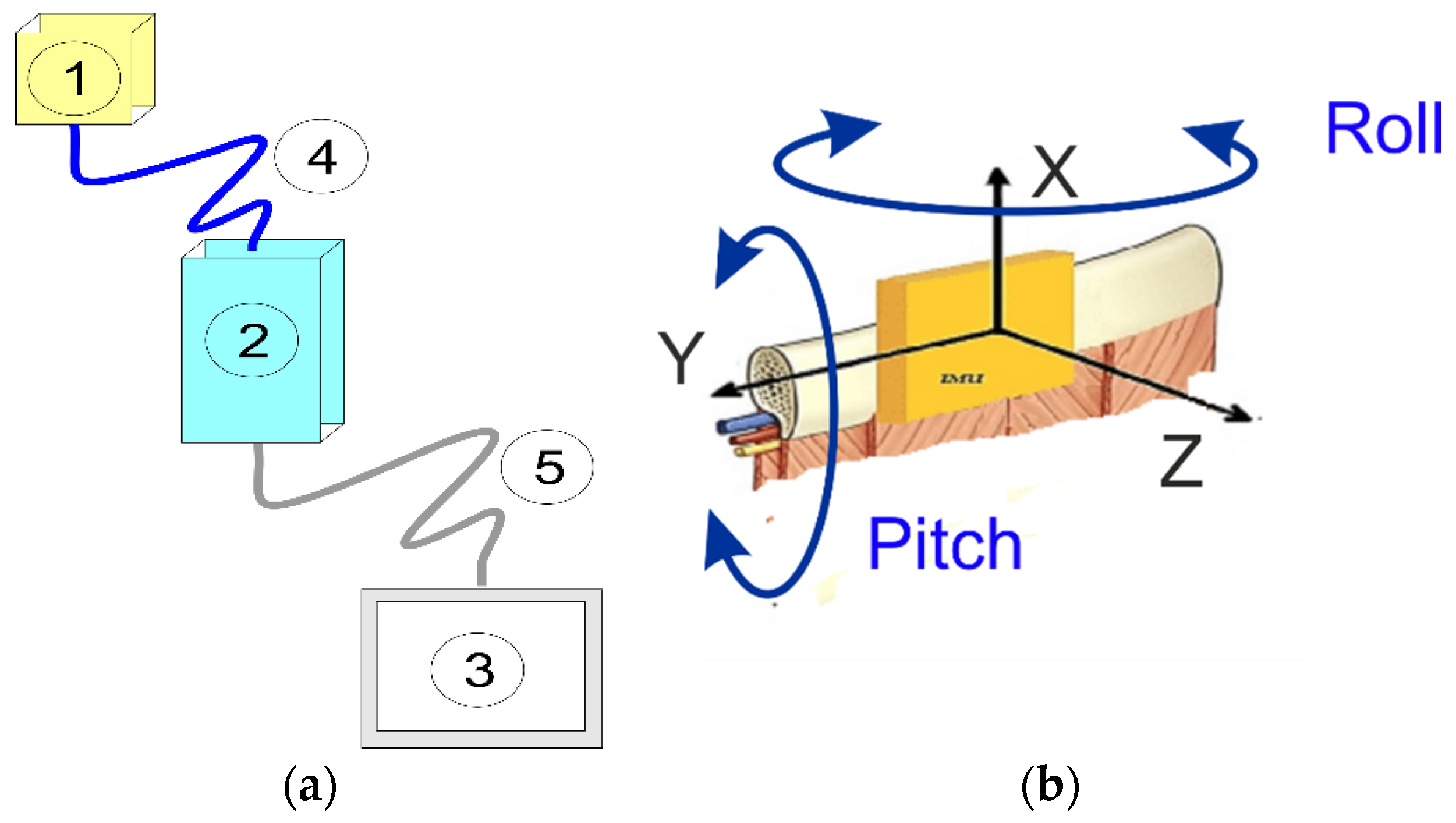
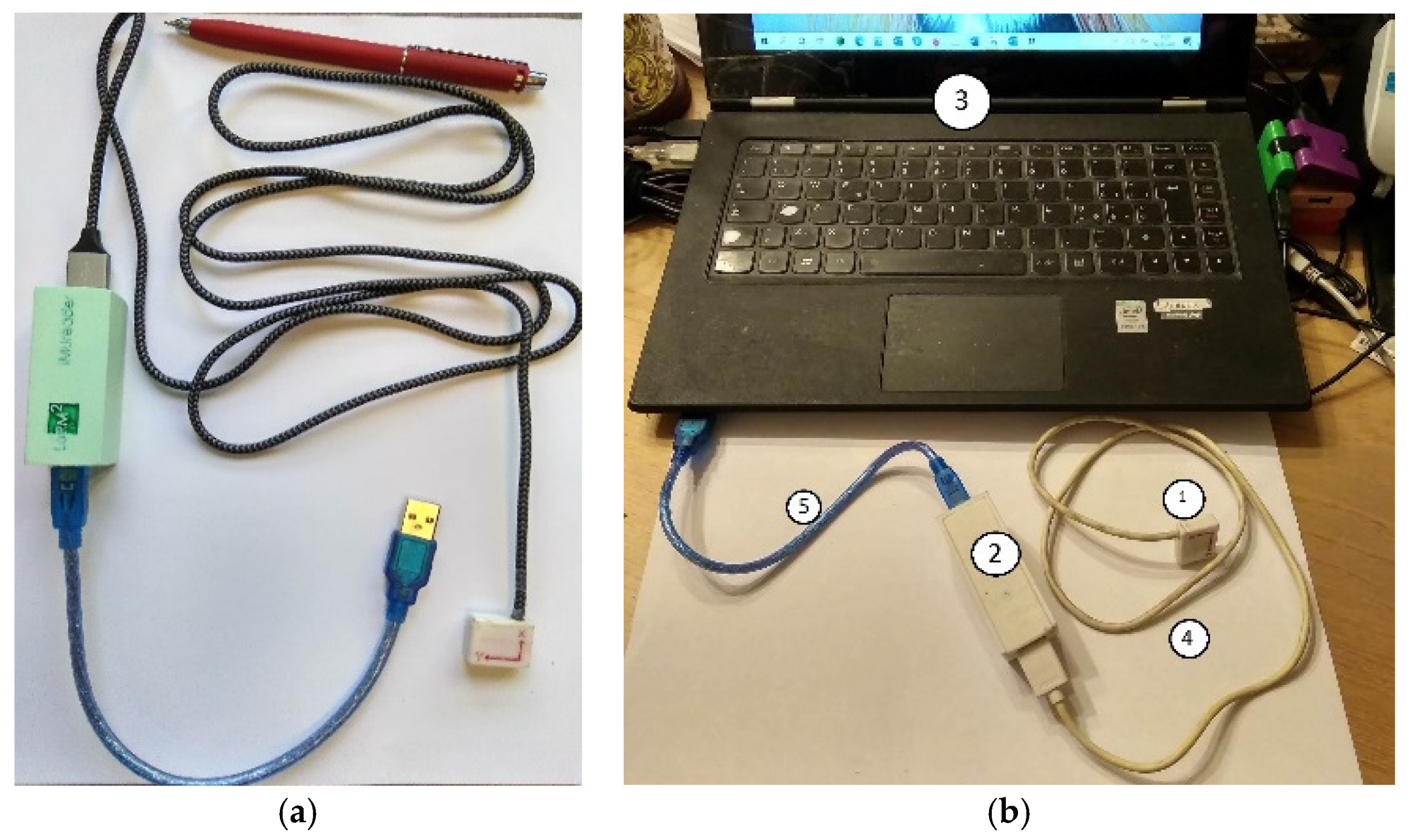
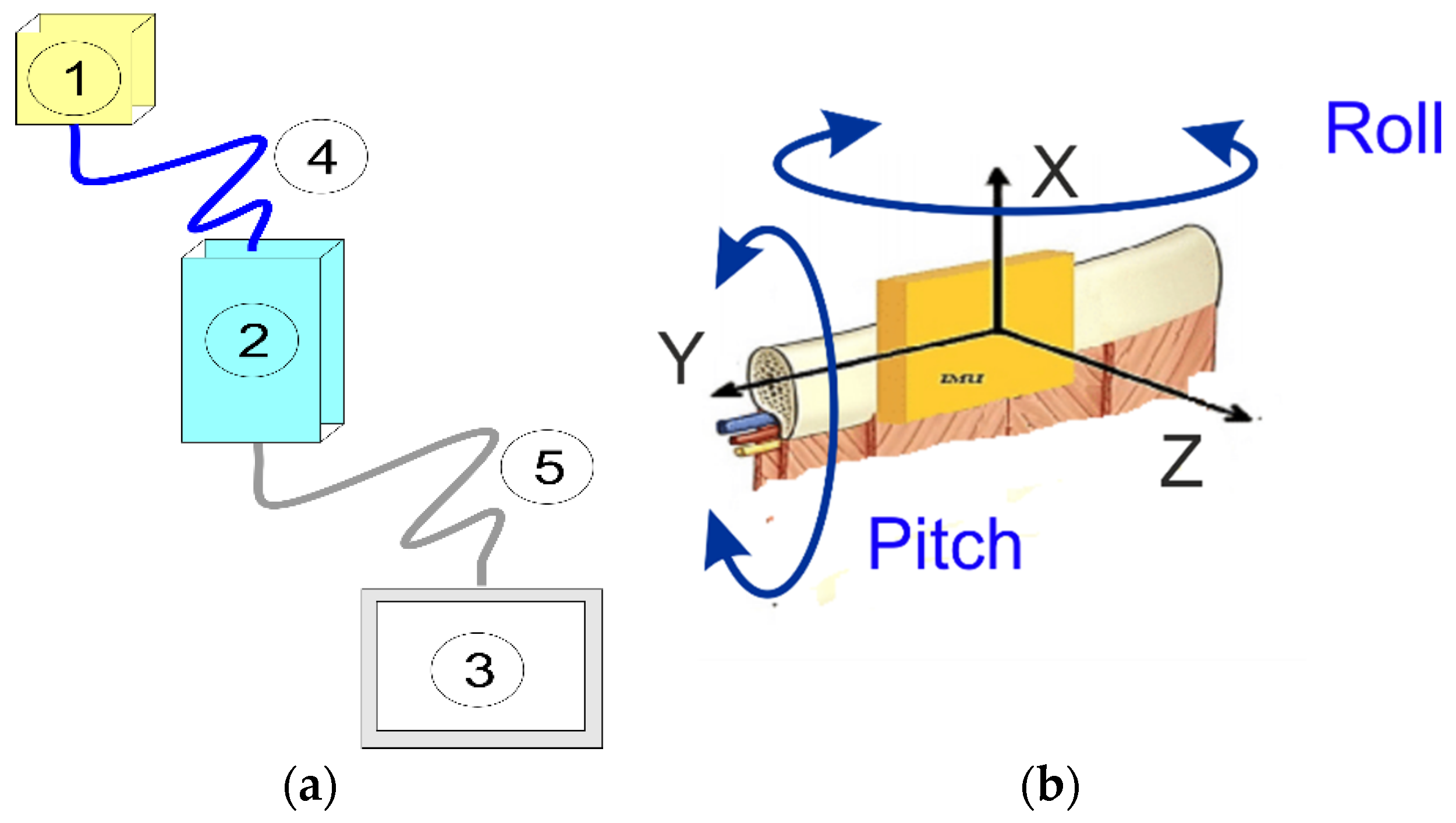
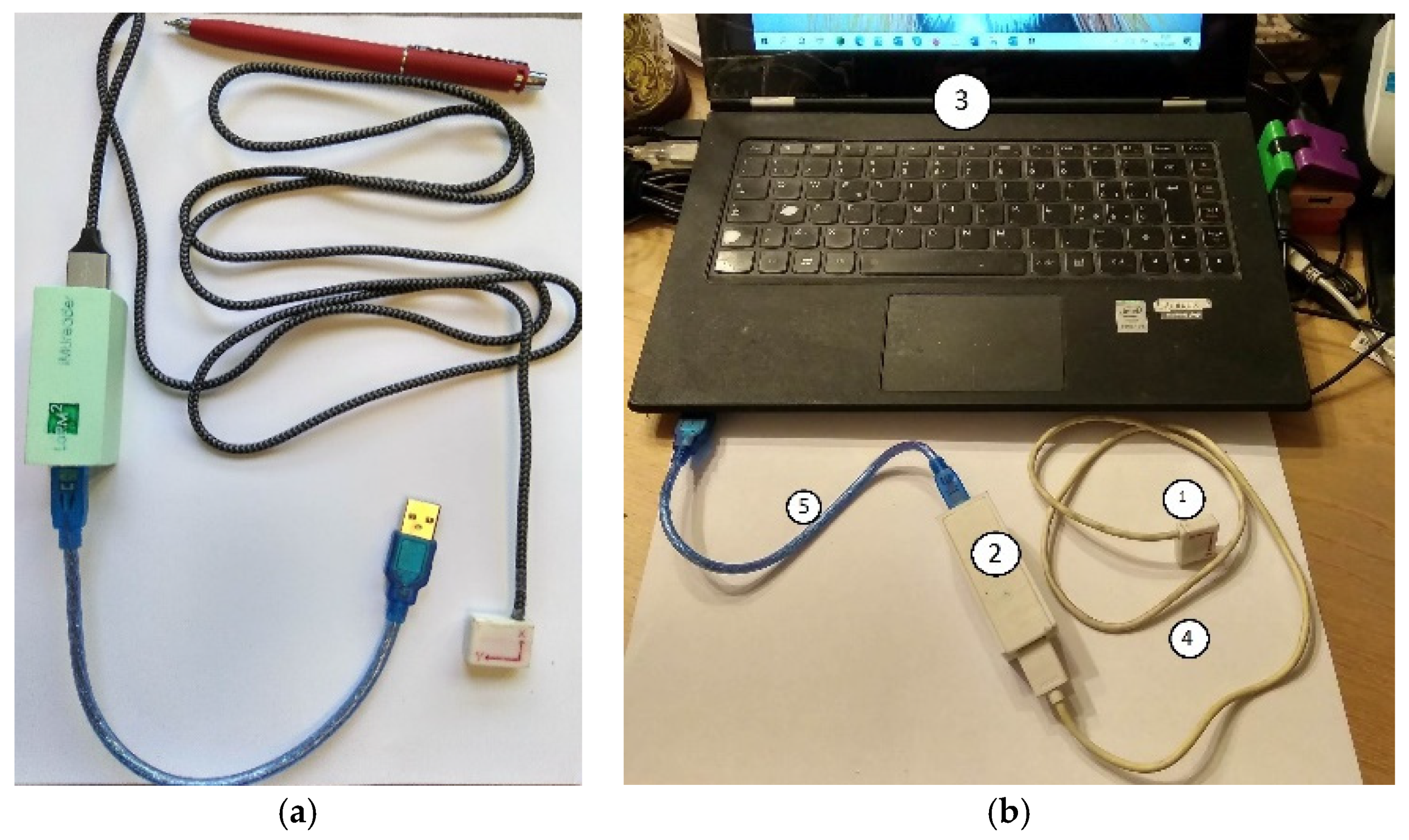
2.1. Device Description
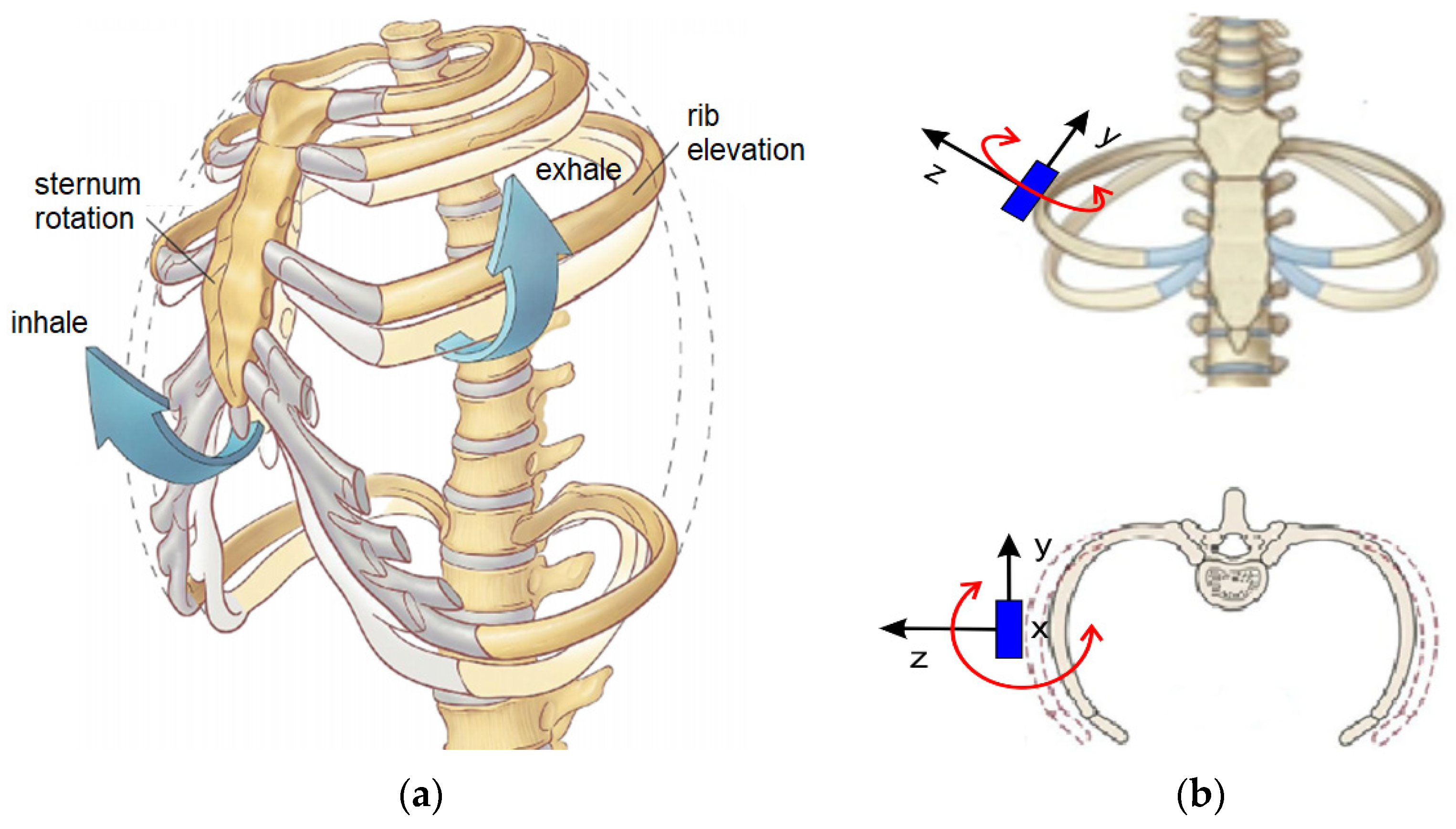
2.2. Biomechanics of Respiration
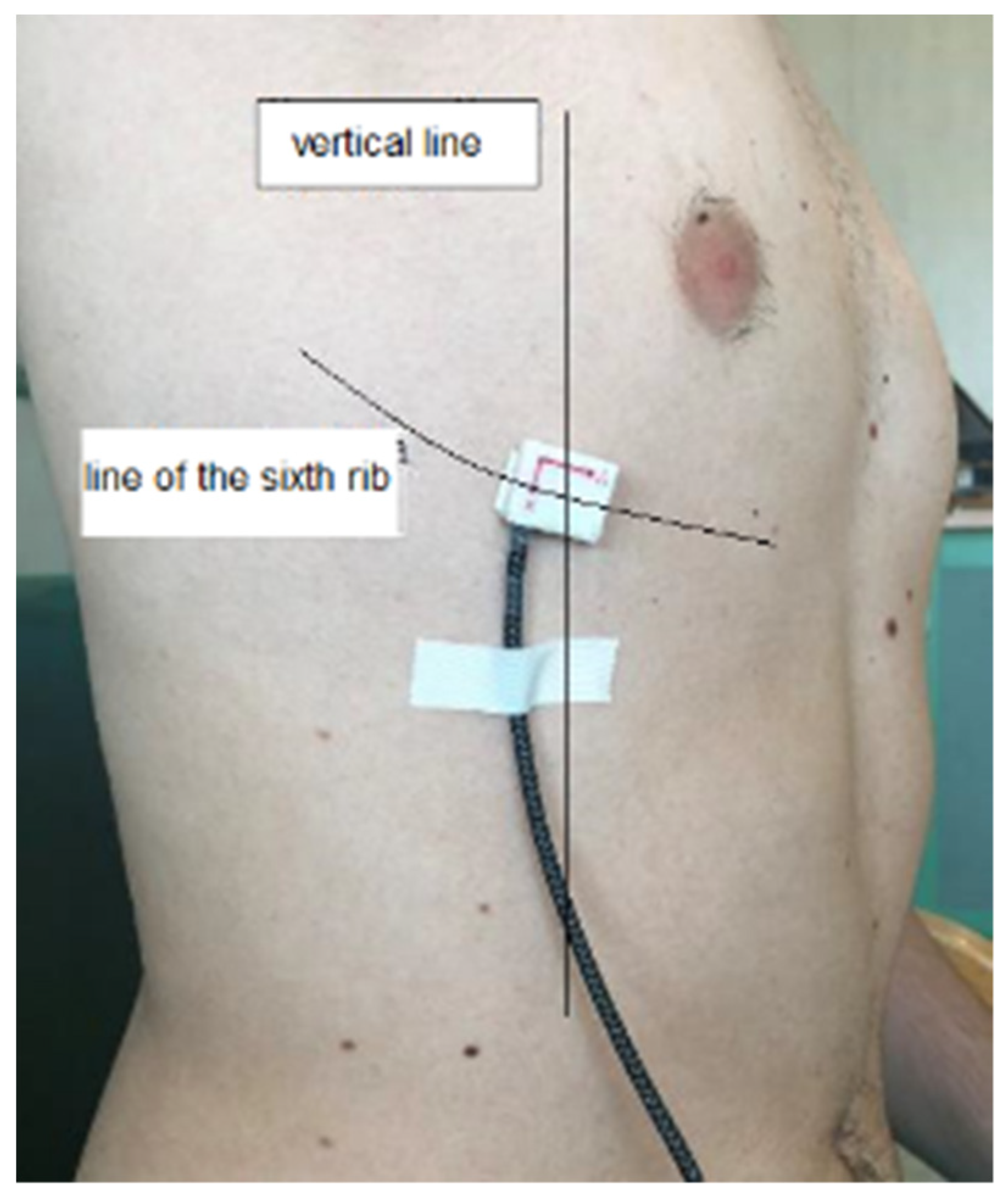
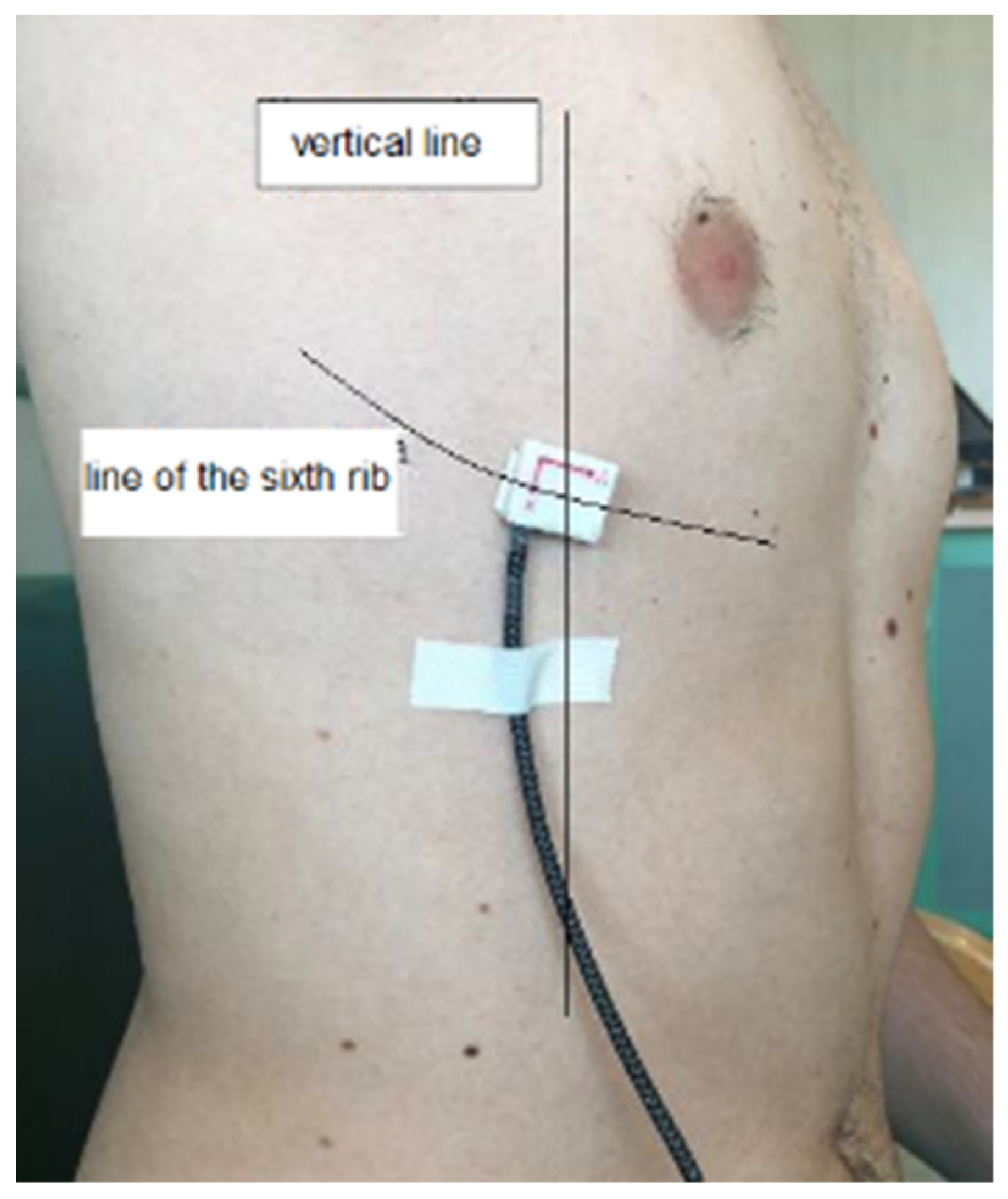
2.3. Measurement Strategy
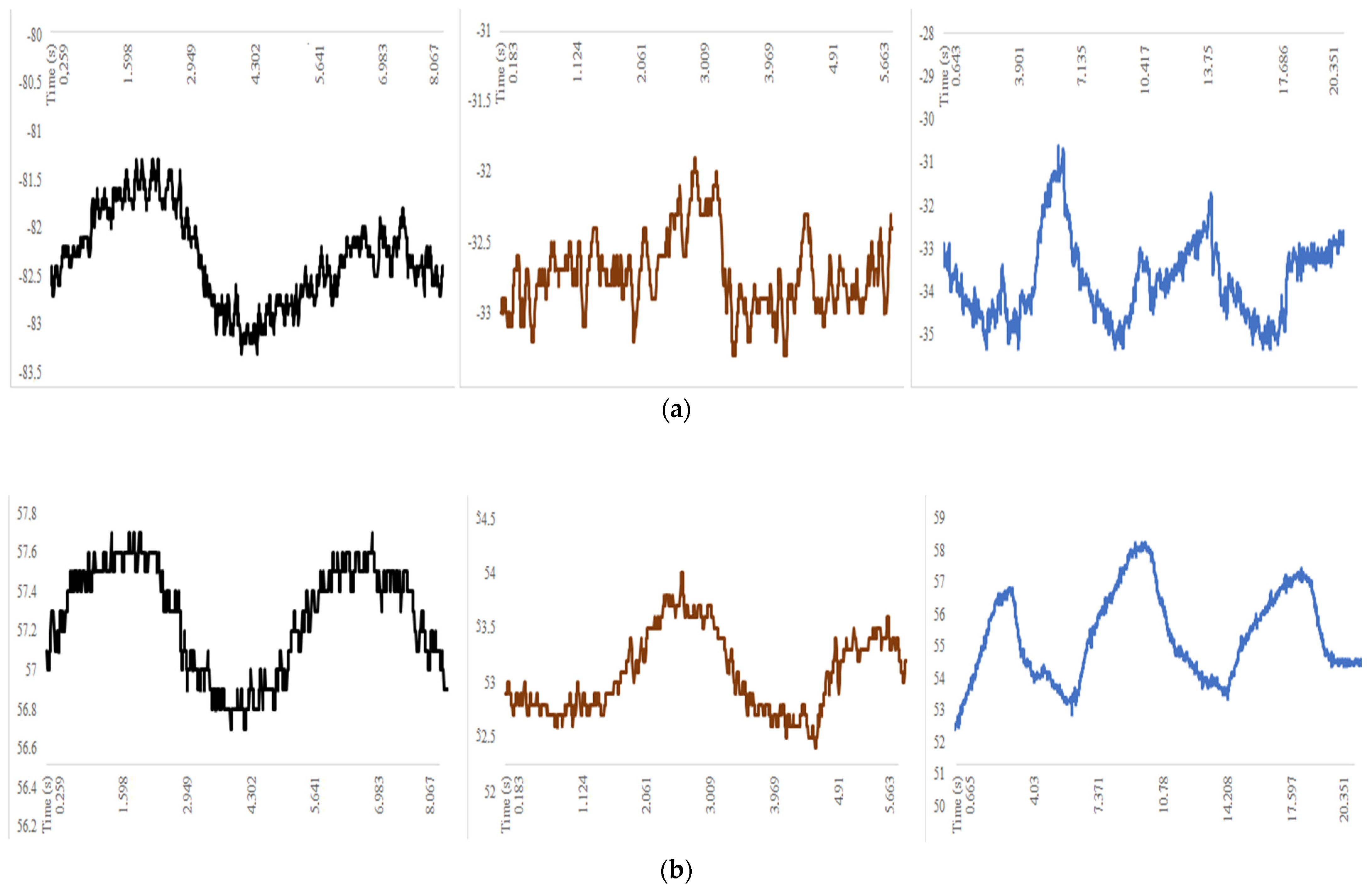
2.4. Data Storage and Analysis
3. Results
3.1. Results in the Post-Operative Functional Assessment
3.2. Results in the Complication Prediction
3.3. Respiratory Rate Monitoring
4. Discussion
4.1. Post-Operative Functional Assessment
4.2. Post-Operative Complications
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Bommart, S.; Berthet, J.P.; Durand, G.; Ghaye, B.; Pujol, J.L.; Marty-Ané, C.; Kovacsik, H. Normal postoperative appearances of lung cancer. Diagn. Interv. Imaging 2016, 97, 1025–1035. [Google Scholar] [CrossRef] [PubMed]
- Nonaka, M.; Kadokura, M.; Yamamoto, S.; Kataoka, D.; Iyano, K.; Kushihashi, T.; Kawada, T.; Takaba, T. Analysis of the anatomic changes in the thoracic cage after a lung resection using magnetic resonance imaging. Surg. Today 2000, 30, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Sengul, A.T.; Sahin, B.; Celenk, C.; Basoglu, A. Postoperative lung volume change depending on the resected lobe. Thorac. Cardiovasc. Surg. 2013, 61, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J., Jr. Benefits of aggressive perioperative management in patients undergoing thoracotomy. Chest 1995, 107 (Suppl. 6), 312S–315S. [Google Scholar] [CrossRef] [PubMed]
- Massard, G.; Wihlm, J.M. Postoperative atelectasis. Chest Surg. Clin. N. Am. 1998, 8, 503–528. [Google Scholar]
- Peroni, D.G.; Boner, A.L. Atelectasis: Mechanisms, diagnosis and management. Paediatr. Respir. Rev. 2000, 1, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Folke, M.; Cernerud, L.; Ekström, M.; Hök, B. Critical review of non-invasive respiratory monitoring in medical care. Med. Biol. Eng. Comput. 2003, 41, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Krehel, M.; Schmid, M.; Rossi, R.M.; Boesel, L.F.; Bona, G.L.; Scherer, L.J. An optical fibre-based sensor for respiratory monitoring. Sensors 2014, 14, 13088–13101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciocchetti, M.; Massaroni, C.; Saccomandi, P.; Caponero, M.A.; Polimadei, A.; Formica, D.; Schena, E. Smart Textile Based on Fiber Bragg Grating Sensors for Respiratory Monitoring: Design and Preliminary Trials. Biosensors 2015, 5, 602–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ono, T.; Takegawa, H.; Ageishi, T.; Takashina, M.; Numasaki, H.; Matsumoto, M.; Teshima, T. Respiratory monitoring with an acceleration sensor. Phys. Med. Biol. 2011, 56, 6279–6289. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Chen, B.; Zhou, J.; Lv, Z. A Low-Power and Portable Biomedical Device for Respiratory Monitoring with a Stable Power Source. Sensors 2015, 15, 19618–19632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beyer, B.; Van Sint Jan, S.; Chèze, L.; Sholukha, V.; Feipel, V. Relationship between costovertebral joint kinematics and lung volume in supine humans. Respir. Physiol. Neurobiol. 2016, 232, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Kondo, T.; Kobayashi, I.; Taguchi, Y.; Hayama, N.; Tajiri, S.; Yanagimachi, N. An analysis of the chest wall motions using the dynamic MRI in healthy elder subjects. Tokai J. Exp. Clin. Med. 2005, 30, 15–20. [Google Scholar] [PubMed]
- Ceccarelli, M. Portable Device for Measuring the Movement of Human Ribs. Italy Patent Pending No. 102,021,000,005,726, 13 March 2021. [Google Scholar]
- Ceccarelli, M.; Puglisi, L.; Mesiti, F.; Ambrogi, V. A device for experimental characterization of biomechanics of breathing and coughing. In Proceedings of the 26th ABCM International Congress of Mechanical Engineering, Florianópolis, SC, Brazil, 24 November 2021. [Google Scholar]
- Cretikos, M.A.; Bellomo, R.; Hillman, K.; Chen, J.; Finfer, S.; Flabouris, A. Respiratory rate: The neglected vital sign. Med. J. Aust. 2008, 188, 657–659. [Google Scholar] [CrossRef] [PubMed]
- Churpek, M.M.; Yuen, T.C.; Park, S.Y.; Meltzer, D.O.; Hall, J.B.; Edelson, D.P. Derivation of a cardiac arrest prediction model using ward vital signs. Crit. Care Med. 2012, 40, 2102–2108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicolò, A.; Massaroni, C.; Schena, E.; Sacchetti, M. The Importance of Respiratory Rate Monitoring: From Healthcare to Sport and Exercise. Sensors 2020, 20, 6396. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pre-Operation | Post-Operation | Non-Operated Site | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Acc. X (g) | Acc. Y (g) | Acc. Z (g) | Acc. X (g) | Acc. Y (g) | Acc. Z (g) | Acc. X (g) | Acc. Y (g) | Acc. Z (g) | ||
| Mean | −0.85 | 0.54 | 0.07 | Mean | −0.81 | −0.33 | 0.05 | −0.80 | 0.31 | 0.04 |
| SD | 0.00 | 0.00 | 0.01 | SD | 0.00 | 0.01 | 0.01 | 0.00 | 0.00 | 0.01 |
| Roll (deg) | Pitch (deg) | Roll (deg) | Pitch (deg) | Roll (deg) | Pitch (deg) | |||||
| Mean | 2.2 | 0.90 | Mean | 1.50 | 1.10 | 2.10 | 2.3 | |||
| SD | 2.04 | 0.58 | SD | 0.87 | 0.13 | 0.72 | 0.15 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ceccarelli, M.; Taje, R.; Papuc, P.E.; Ambrogi, V. An Analysis of Respiration with the Smart Sensor SENSIRIB in Patients Undergoing Thoracic Surgery. Sensors 2022, 22, 1561. https://doi.org/10.3390/s22041561
Ceccarelli M, Taje R, Papuc PE, Ambrogi V. An Analysis of Respiration with the Smart Sensor SENSIRIB in Patients Undergoing Thoracic Surgery. Sensors. 2022; 22(4):1561. https://doi.org/10.3390/s22041561
Chicago/Turabian StyleCeccarelli, Marco, Riccardo Taje, Paula Elena Papuc, and Vincenzo Ambrogi. 2022. "An Analysis of Respiration with the Smart Sensor SENSIRIB in Patients Undergoing Thoracic Surgery" Sensors 22, no. 4: 1561. https://doi.org/10.3390/s22041561
APA StyleCeccarelli, M., Taje, R., Papuc, P. E., & Ambrogi, V. (2022). An Analysis of Respiration with the Smart Sensor SENSIRIB in Patients Undergoing Thoracic Surgery. Sensors, 22(4), 1561. https://doi.org/10.3390/s22041561