
Deep Convolutional Neural Network-Based Hemiplegic Gait Detection Using an Inertial Sensor Located Freely in a Pocket


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Acquisition System
2.2. Experimental Protocol
- The test subject randomly put the measurement system in the pocket of a jacket and waited at the starting point.
- When the start signal was given after the PC application and measurement system were connected, the test subject walked along the 20-m-long corridor at their usual walking speed.
- After walking 20 m, the subject turned around and waited.
- When the start signal was given, the subject returned along the 20-m-long corridor.
- The subject waited at the starting point.
- We ended the experiment by terminating the application and saving the measurement data.
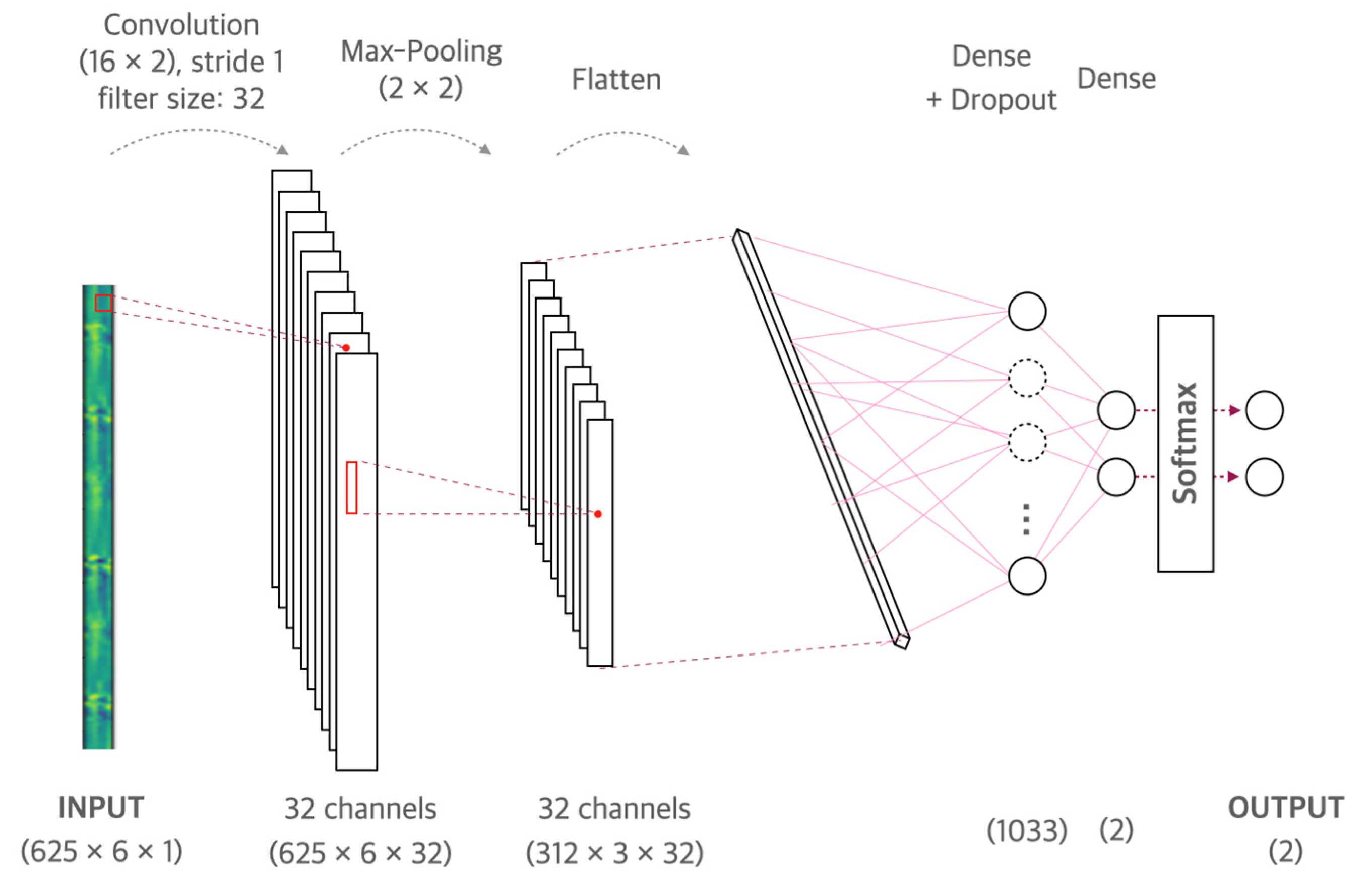
2.3. Machine Learning Model
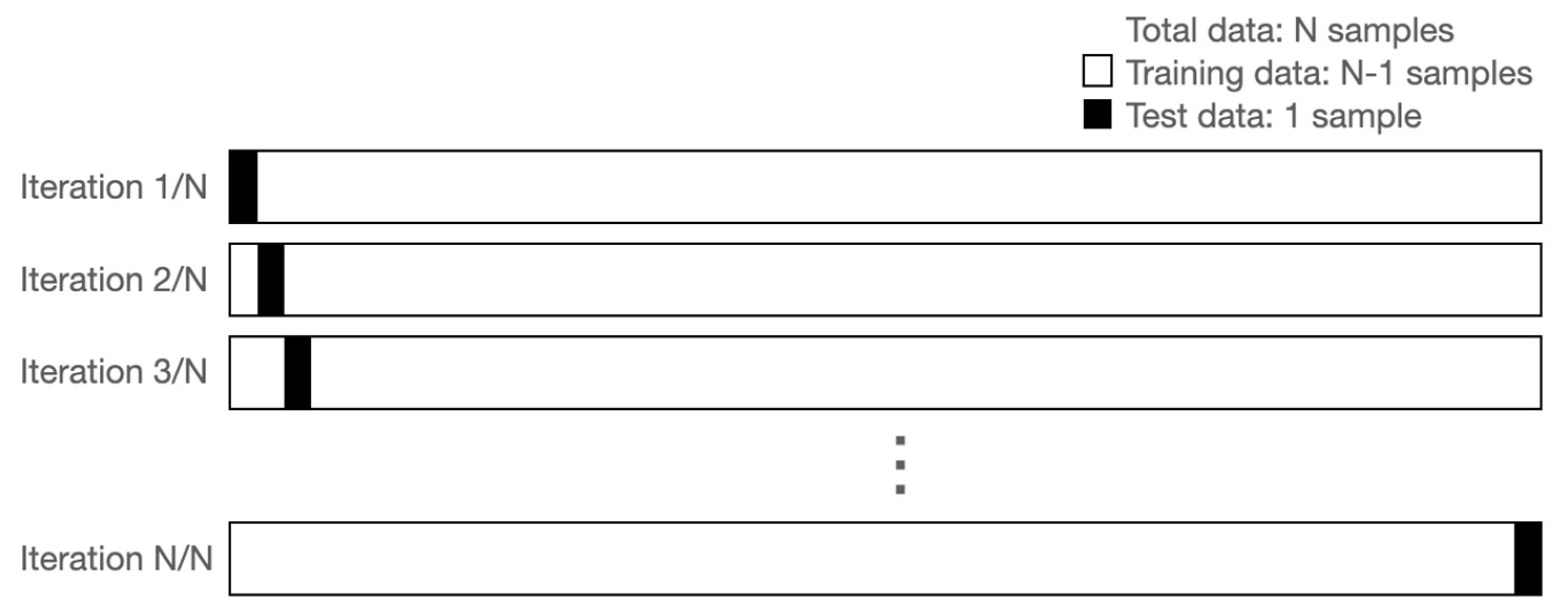
2.4. Leave-One-Out Cross Validation
2.5. Statistical Analysis
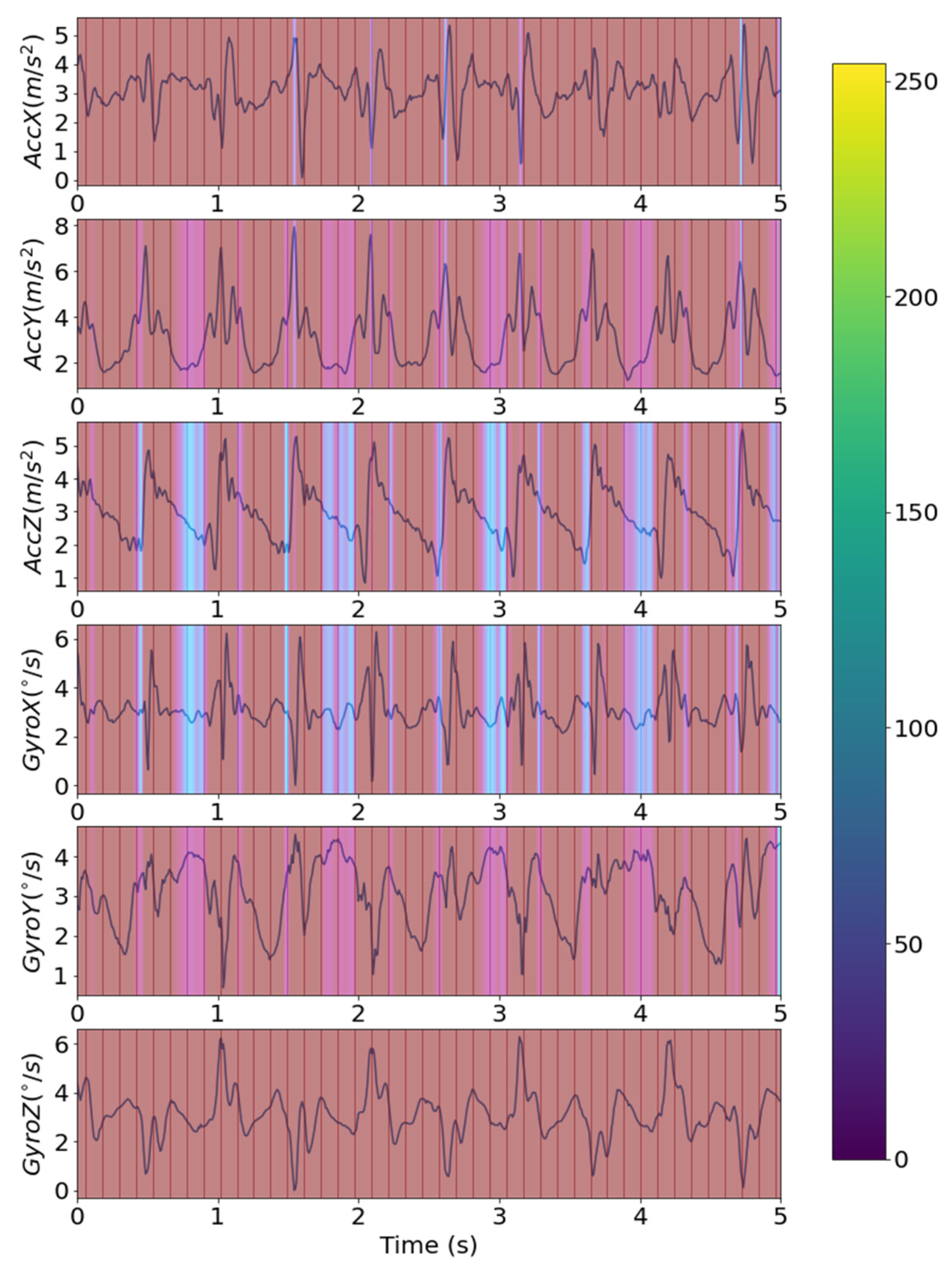
2.6. Grad-Cam
2.7. Uncertainty
3. Results
3.1. Dataset
3.2. CNN Model
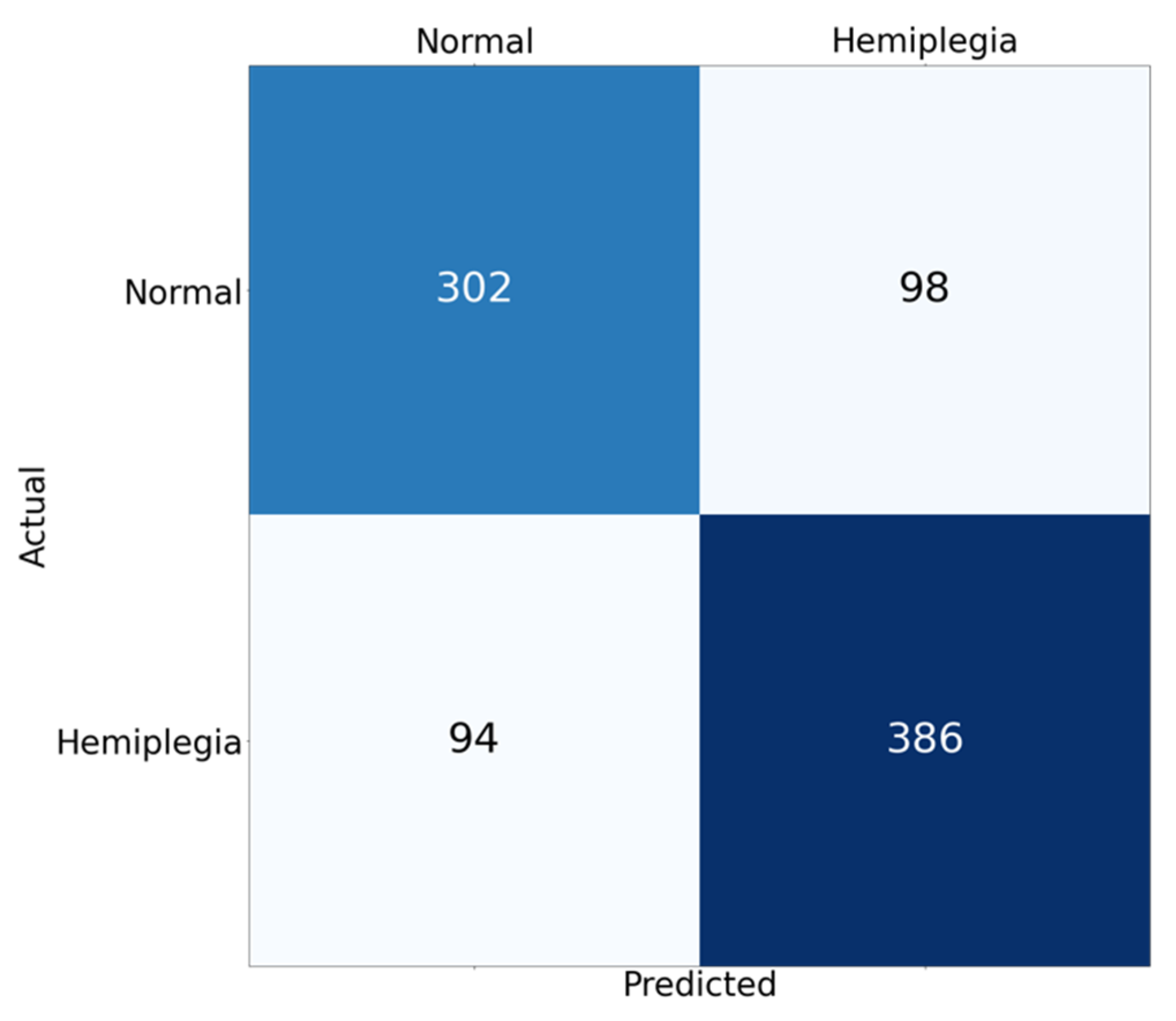
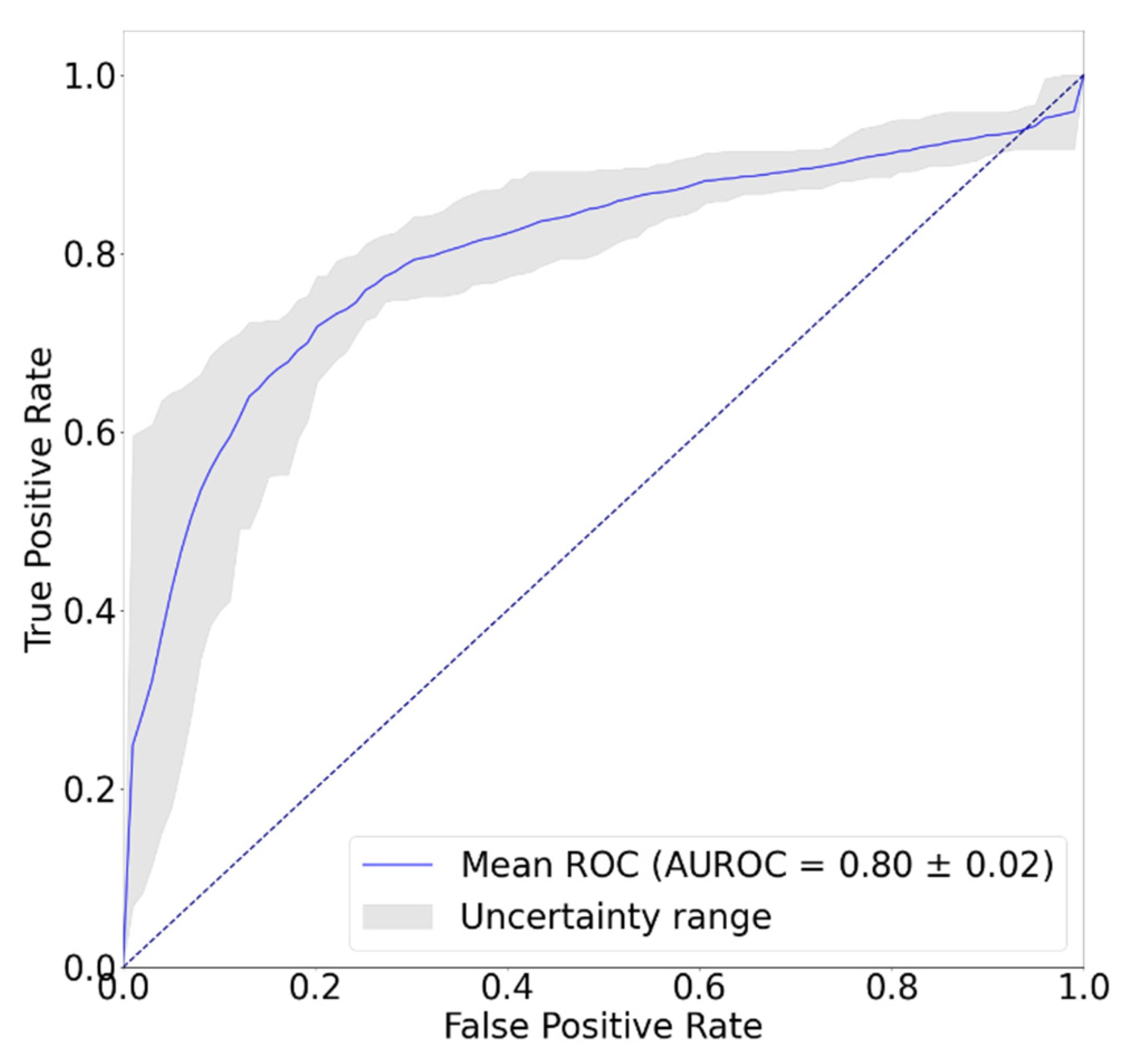
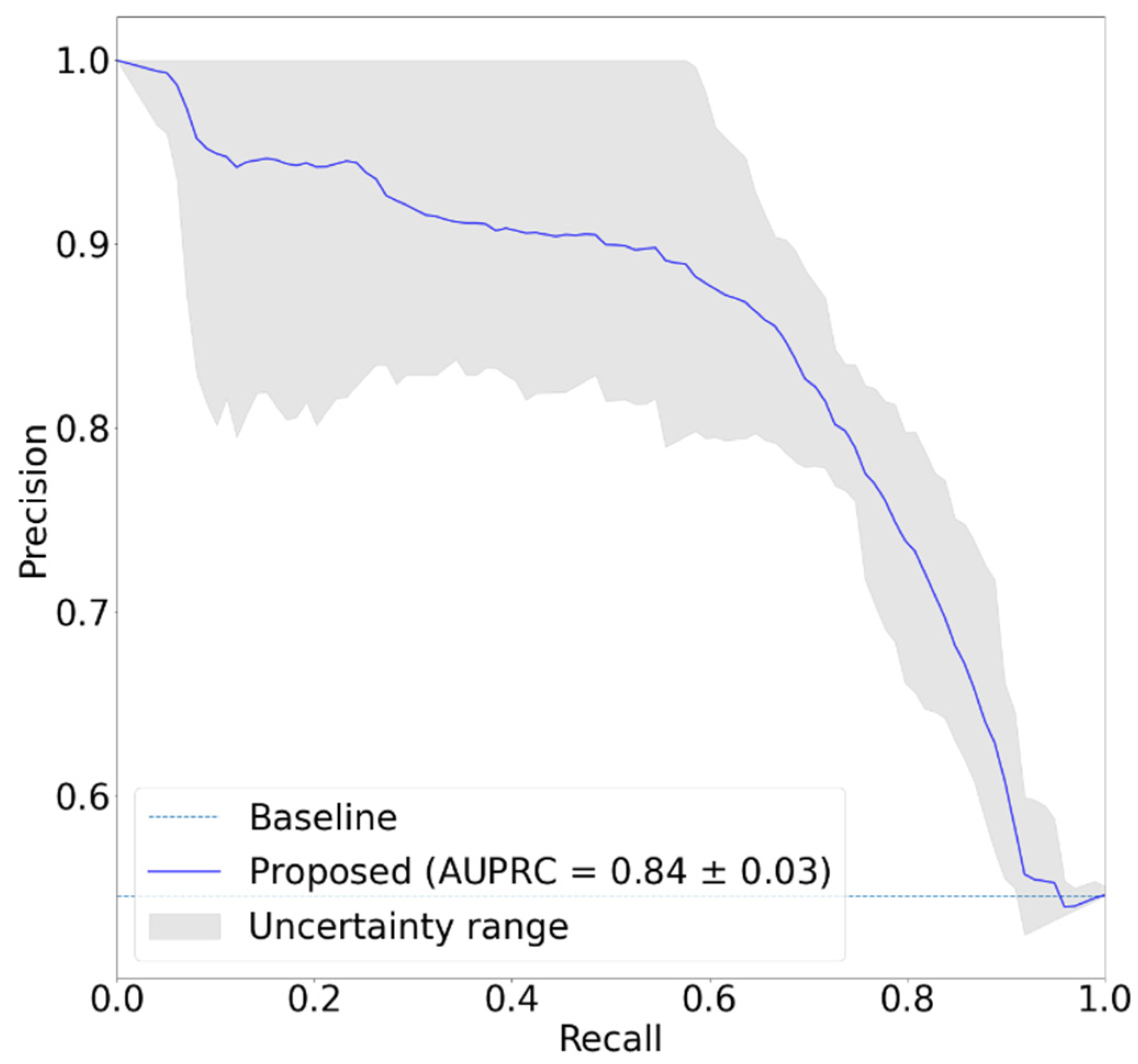
3.3. Classification Results
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Aminian, K.; Rezakhanlou, K.; De Andres, E.; Fritsch, C.; Leyvraz, P.-F.; Robert, P. Temporal feature estimation during walking using miniature accelerometers: An analysis of gait improvement after hip arthroplasty. Med. Biol. Eng. Comput. 1999, 37, 686–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishiguchi, S.; Yamada, M.; Nagai, K.; Mori, S.; Kajiwara, Y.; Sonoda, T.; Yoshimura, K.; Yoshitomi, H.; Ito, H.; Okamoto, K. Reliability and validity of gait analysis by android-based smartphone. Telemed. E-Health 2012, 18, 292–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thang, H.M.; Viet, V.Q.; Thuc, N.D.; Choi, D. Gait identification using accelerometer on mobile phone. In Proceedings of the 2012 International Conference on Control, Automation and Information Sciences (ICCAIS), Ho Chi Minh City, Vietnam, 26–29 November 2012; pp. 344–348. [Google Scholar]
- Lee, J.-A.; Cho, S.-H.; Lee, J.-W.; Lee, K.-H.; Yang, H.-K. Wearable accelerometer system for measuring the temporal parameters of gait. In Proceedings of the 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 22–26 August 2007; pp. 483–486. [Google Scholar]
- Bugané, F.; Benedetti, M.; Casadio, G.; Attala, S.; Biagi, F.; Manca, M.; Leardini, A. Estimation of spatial-temporal gait parameters in level walking based on a single accelerometer: Validation on normal subjects by standard gait analysis. Comput. Methods Programs Biomed. 2012, 108, 129–137. [Google Scholar] [CrossRef]
- Hartmann, A.; Luzi, S.; Murer, K.; de Bie, R.A.; de Bruin, E.D. Concurrent validity of a trunk tri-axial accelerometer system for gait analysis in older adults. Gait Posture 2009, 29, 444–448. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Park, S.; Shin, H. Detection of hemiplegic walking using a wearable inertia sensing device. Sensors 2018, 18, 1736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mizuike, C.; Ohgi, S.; Morita, S. Analysis of stroke patient walking dynamics using a tri-axial accelerometer. Gait Posture 2009, 30, 60–64. [Google Scholar] [CrossRef]
- Moore, S.A.; Hickey, A.; Lord, S.; Del Din, S.; Godfrey, A.; Rochester, L. Comprehensive measurement of stroke gait characteristics with a single accelerometer in the laboratory and community: A feasibility, validity and reliability study. J. Neuroeng. Rehabil. 2017, 14, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Lee, J.S.; Kwak, J.; Shin, H. Design of the wearable device for hemiplegic gait detection using an accelerometer and a gyroscope. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju, Korea, 11–15 July 2017; pp. 1409–1412. [Google Scholar]
- Sekine, M.; Abe, Y.; Sekimoto, M.; Higashi, Y.; Fujimoto, T.; Tamura, T.; Fukui, Y. Assessment of gait parameter in hemiplegic patients by accelerometry. In Proceedings of the 22nd Annual International Conference of the IEEE Engineering in Medicine and Biology Society (Cat. No. 00CH37143), Chicago, IL, USA, 23–28 July 2000; pp. 1879–1882. [Google Scholar]
- Rastegari, E.; Azizian, S.; Ali, H. Machine learning and similarity network approaches to support automatic classification of parkinson’s diseases using accelerometer-based gait analysis. In Proceedings of the 52nd Hawaii International Conference on System Sciences, Maui, HI, USA, 8–11 January 2019. [Google Scholar]
- Abdulhay, E.; Arunkumar, N.; Narasimhan, K.; Vellaiappan, E.; Venkatraman, V. Gait and tremor investigation using machine learning techniques for the diagnosis of Parkinson disease. Future Gener. Comput. Syst. 2018, 83, 366–373. [Google Scholar] [CrossRef]
- Chung, P.-C.; Hsu, Y.-L.; Wang, C.-Y.; Lin, C.-W.; Wang, J.-S.; Pai, M.-C. Gait analysis for patients with Alzheimer’s disease using a triaxial accelerometer. In Proceedings of the 2012 IEEE International Symposium on Circuits and Systems (ISCAS), Seoul, Korea, 20–23 May 2012; pp. 1323–1326. [Google Scholar]
- Henriksen, M.; Lund, H.; Moe-Nilssen, R.; Bliddal, H.; Danneskiod-Samsøe, B. Test–retest reliability of trunk accelerometric gait analysis. Gait Posture 2004, 19, 288–297. [Google Scholar] [CrossRef]
- Rispens, S.M.; Pijnappels, M.; van Schooten, K.S.; Beek, P.J.; Daffertshofer, A.; van Dieën, J.H. Consistency of gait characteristics as determined from acceleration data collected at different trunk locations. Gait Posture 2014, 40, 187–192. [Google Scholar] [CrossRef] [Green Version]
- LeMoyne, R.; Mastroianni, T. Implementation of Machine Learning Classification Regarding Hemiplegic Gait Using an Assortment of Machine Learning Algorithms with Quantification from Conformal Wearable and Wireless Inertial Sensor System. J. Biomed. Sci. Eng. 2021, 14, 415–425. [Google Scholar] [CrossRef]
- Christou, V.; Arjmand, A.; Dimopoulos, D.; Varvarousis, D.; Tzallas, A.T.; Gogos, C.; Tsipouras, M.G.; Ploumis, A.; Giannakeas, N. Neural Network-Based approach for Hemiplegia Detection via Accelerometer Signals. In Proceedings of the 2021 6th South-East Europe Design Automation, Computer Engineering, Computer Networks and Social Media Conference (SEEDA-CECNSM), Preveza, Greece, 24–26 September 2021; pp. 1–5. [Google Scholar]
- Lemoyne, R.; Mastroianni, T. Implementation of a smartphone as a wearable and wireless gyroscope platform for machine learning classification of hemiplegic gait through a multilayer perceptron neural network. In Proceedings of the 2018 17th IEEE International Conference on Machine Learning and Applications (ICMLA), Orlando, FL, USA, 17–20 December 2018; pp. 946–950. [Google Scholar]
- Buckley, C.; Micó-Amigo, M.E.; Dunne-Willows, M.; Godfrey, A.; Hickey, A.; Lord, S.; Rochester, L.; Del Din, S.; Moore, S.A. Gait asymmetry post-stroke: Determining valid and reliable methods using a single accelerometer located on the trunk. Sensors 2020, 20, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakatsuchi, T.; Ikebuchi, M.; Nishikawa, T.; Sugahara, T.; Nakajima, S.; Morimoto, M.; Nakamura, H. Analysis of Gait in Stroke Patients with Hemiplegia Using a Wearable Accelerometer. Osaka City Med. J. 2020, 66, 31–37. [Google Scholar]
- Pandit, T.; Nahane, H.; Lade, D.; Rao, V. Abnormal Gait Detection by Classifying Inertial Sensor Data using Transfer Learning. In Proceedings of the 2019 18th IEEE International Conference On Machine Learning And Applications (ICMLA), Boca Raton, FL, USA, 16–19 December 2019; pp. 1444–1447. [Google Scholar]
- Zhang, W.; Smuck, M.; Legault, C.; Ith, M.A.; Muaremi, A.; Aminian, K. Gait symmetry assessment with a low back 3D accelerometer in post-stroke patients. Sensors 2018, 18, 3322. [Google Scholar] [CrossRef] [Green Version]
- LeMoyne, R.; Mastroianni, T. Wearable and wireless gait analysis platforms: Smartphones and portable media devices. In Wireless MEMS Networks and Applications; Elsevier: Amsterdam, The Netherlands, 2017; pp. 129–152. [Google Scholar]
- Iso, T.; Yamazaki, K. Gait analyzer based on a cell phone with a single three-axis accelerometer. In Proceedings of the 8th Conference on Human-Computer Interaction with Mobile Devices and Services, Helsinki, Finland, 12–15 September 2006; pp. 141–144. [Google Scholar]
- Zhang, S.; Poon, S.K.; Vuong, K.; Sneddon, A.; Loy, C.T. A deep learning-based approach for gait analysis in Huntington disease. In MEDINFO 2019: Health and Wellbeing e-Networks for All; IOS Press: Amsterdam, The Netherlands, 2019; pp. 477–481. [Google Scholar]
- Moro, M.; Marchesi, G.; Odone, F.; Casadio, M. Markerless gait analysis in stroke survivors based on computer vision and deep learning: A pilot study. In Proceedings of the 35th Annual ACM Symposium on Applied Computing, New York, NY, USA, 30 March–3 April 2020; pp. 2097–2104. [Google Scholar]
- Horst, F.; Lapuschkin, S.; Samek, W.; Müller, K.-R.; Schöllhorn, W.I. Explaining the unique nature of individual gait patterns with deep learning. Sci. Rep. 2019, 9, 2391. [Google Scholar] [CrossRef] [Green Version]
- Alharthi, A.S.; Yunas, S.U.; Ozanyan, K.B. Deep learning for monitoring of human gait: A review. IEEE Sens. J. 2019, 19, 9575–9591. [Google Scholar] [CrossRef] [Green Version]
- Begg, R.; Kamruzzaman, J. A machine learning approach for automated recognition of movement patterns using basic, kinetic and kinematic gait data. J. Biomech. 2005, 38, 401–408. [Google Scholar] [CrossRef]
- Su, B.; Smith, C.; Gutierrez Farewik, E. Gait phase recognition using deep convolutional neural network with inertial measurement units. Biosensors 2020, 10, 109. [Google Scholar] [CrossRef]
- Pogorelc, B.; Bosnić, Z.; Gams, M. Automatic recognition of gait-related health problems in the elderly using machine learning. Multimed. Tools Appl. 2012, 58, 333–354. [Google Scholar] [CrossRef] [Green Version]
- Gao, J.; Gu, P.; Ren, Q.; Zhang, J.; Song, X. Abnormal gait recognition algorithm based on LSTM-CNN fusion network. IEEE Access 2019, 7, 163180–163190. [Google Scholar] [CrossRef]
- McGinnis, R.S.; Mahadevan, N.; Moon, Y.; Seagers, K.; Sheth, N.; Wright, J.A., Jr.; DiCristofaro, S.; Silva, I.; Jortberg, E.; Ceruolo, M. A machine learning approach for gait speed estimation using skin-mounted wearable sensors: From healthy controls to individuals with multiple sclerosis. PLoS ONE 2017, 12, e0178366. [Google Scholar] [CrossRef]
- Invensense, T. MPU-9250 Datasheet. Available online: https://invensense.tdk.com/download-pdf/mpu-9250-datasheet/ (accessed on 24 October 2021).
- O’Shea, K.; Nash, R. An introduction to convolutional neural networks. arXiv 2015, arXiv:1511.08458. [Google Scholar]
- Lee, S.-M.; Yoon, S.M.; Cho, H. Human activity recognition from accelerometer data using Convolutional Neural Network. In Proceedings of the 2017 IEEE International Conference on Big Data and Smart Computing (Bigcomp), Jeju, Korea, 13–16 February 2017; pp. 131–134. [Google Scholar]
- Dehzangi, O.; Taherisadr, M.; ChangalVala, R. IMU-based gait recognition using convolutional neural networks and multi-sensor fusion. Sensors 2017, 17, 2735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gadaleta, M.; Rossi, M. Idnet: Smartphone-based gait recognition with convolutional neural networks. Pattern Recognit. 2018, 74, 25–37. [Google Scholar] [CrossRef] [Green Version]
- Kreuter, D.; Takahashi, H.; Omae, Y.; Akiduki, T.; Zhang, Z. Classification of human gait acceleration data using convolutional neural networks. Int. J. Innov. Comput. Inf. Control 2020, 16, 609–619. [Google Scholar]
- Tian, J. Adversarial vulnerability of deep neural network-based gait event detection: A comparative study using accelerometer-based data. Biomed. Signal Process. Control 2022, 73, 103429. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhou, S. Wearable device-based gait recognition using angle embedded gait dynamic images and a convolutional neural network. Sensors 2017, 17, 478. [Google Scholar] [CrossRef]
- Srivastava, N.; Hinton, G.; Krizhevsky, A.; Sutskever, I.; Salakhutdinov, R. Dropout: A simple way to prevent neural networks from overfitting. J. Mach. Learn. Res. 2014, 15, 1929–1958. [Google Scholar]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- Snoek, J.; Larochelle, H.; Adams, R.P. Practical bayesian optimization of machine learning algorithms. Adv. Neural Inf. Process. Syst. 2012, 25. [Google Scholar]
- Zhou, B.; Khosla, A.; Lapedriza, A.; Oliva, A.; Torralba, A. Learning deep features for discriminative localization. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2921–2929. [Google Scholar]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-cam: Visual explanations from deep networks via gradient-based localization. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 618–626. [Google Scholar]
- Gal, Y.; Ghahramani, Z. Dropout as a bayesian approximation: Representing model uncertainty in deep learning. In Proceedings of the 33rd International Conference on Machine Learning, New York, NY, USA, 19–24 June 2016; pp. 1050–1059. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters. | Normal (N = 21) | Hemiplegia (N = 21) |
|---|---|---|
| Age (years) | 53.0 ± 16.0 (range: 27–77) | 62.6 ± 9.2 (47–78) |
| Sex (M/F, N) | 11/10 | 13/8 |
| Height (cm) | 165.0 ± 7.6 (150–178) | 165.1 ± 11.0 (145–178) |
| Weight (kg) | 66.3 ± 9.9 (48–82) | 66.2 ± 14.6 (38–90) |
| Paralyzed side (N) | not applicable | Left (7), Right (11), Both (3) |
| Evaluation Metrics | Values |
|---|---|
| Accuracy | 0.78 |
| Precision | 0.80 |
| Recall | 0.80 |
| F1 score | 0.80 |
| AUROC | 0.80 |
| AUPRC | 0.84 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, H. Deep Convolutional Neural Network-Based Hemiplegic Gait Detection Using an Inertial Sensor Located Freely in a Pocket. Sensors 2022, 22, 1920. https://doi.org/10.3390/s22051920
Shin H. Deep Convolutional Neural Network-Based Hemiplegic Gait Detection Using an Inertial Sensor Located Freely in a Pocket. Sensors. 2022; 22(5):1920. https://doi.org/10.3390/s22051920
Chicago/Turabian StyleShin, Hangsik. 2022. "Deep Convolutional Neural Network-Based Hemiplegic Gait Detection Using an Inertial Sensor Located Freely in a Pocket" Sensors 22, no. 5: 1920. https://doi.org/10.3390/s22051920
APA StyleShin, H. (2022). Deep Convolutional Neural Network-Based Hemiplegic Gait Detection Using an Inertial Sensor Located Freely in a Pocket. Sensors, 22(5), 1920. https://doi.org/10.3390/s22051920