
Improved Individualized Patient-Oriented Depth-of-Hypnosis Measurement Based on Bispectral Index



Abstract
:1. Introduction
2. Propofol Pharmacokinetic and Pharmacodynamic Modeling
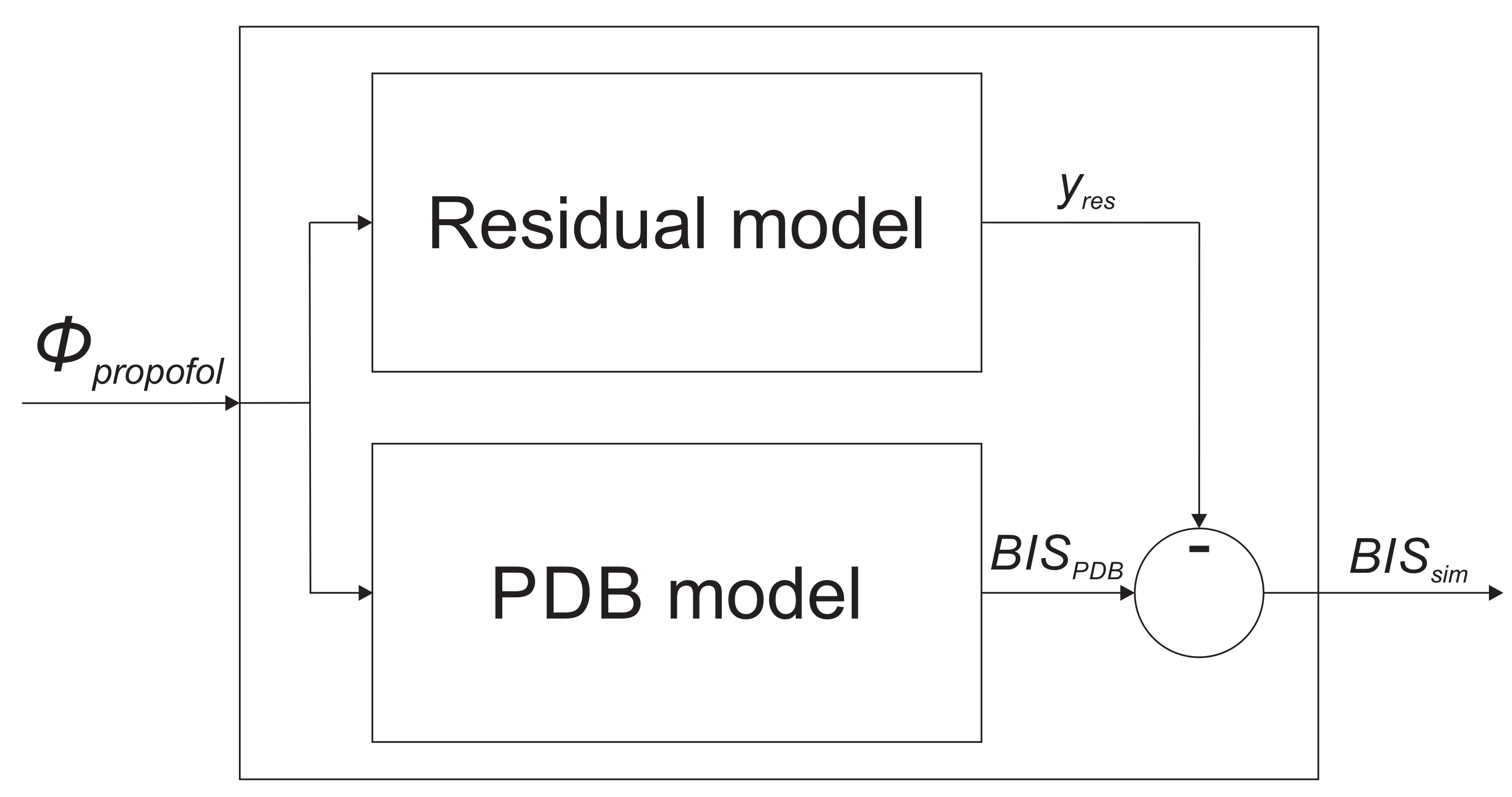
3. Residual Model Introduction—Improvement of the Population-Data-Based Model
4. Identification of the Residual Dynamic Model
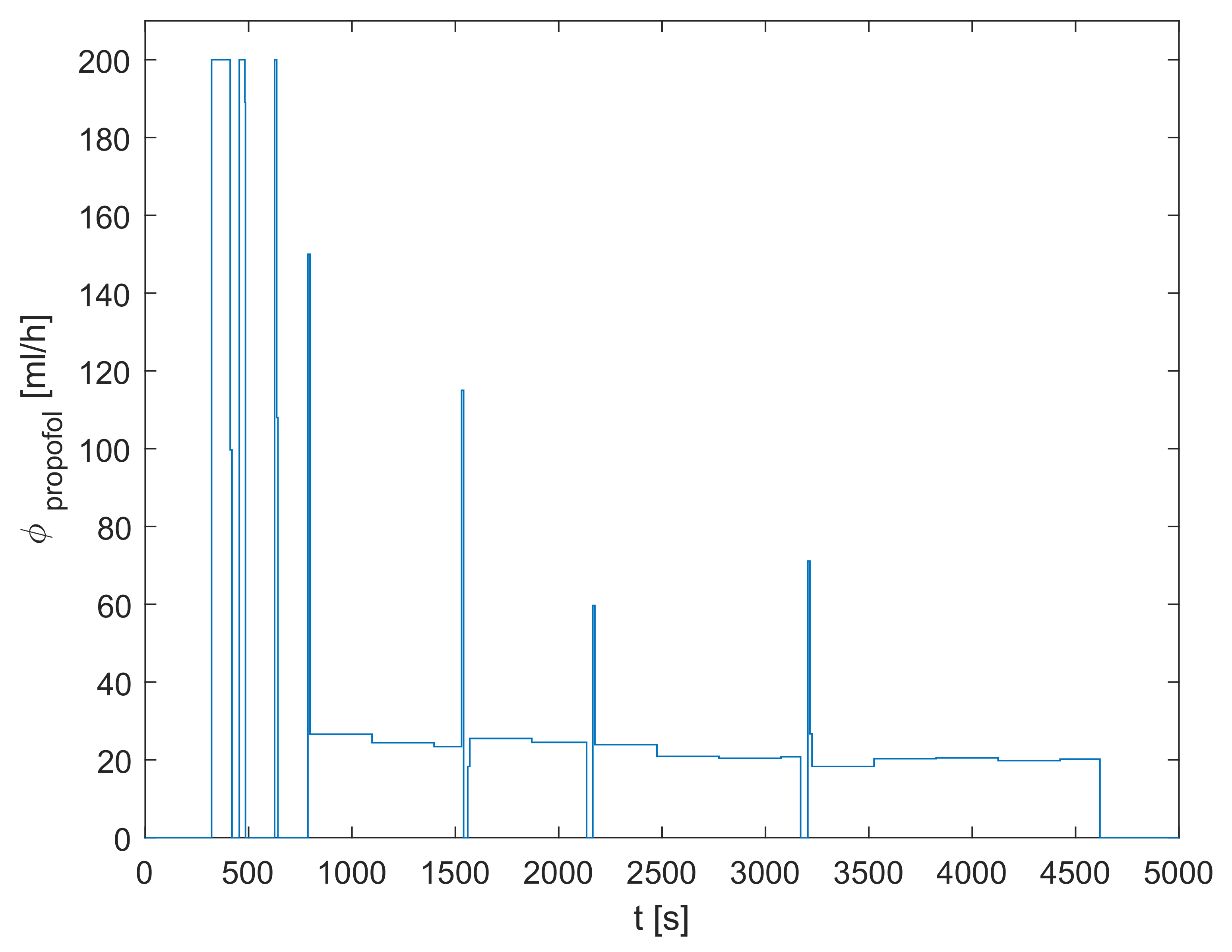
4.1. Identification Signals
4.2. Residual Dynamic Model Structure
4.3. Parameter Estimation
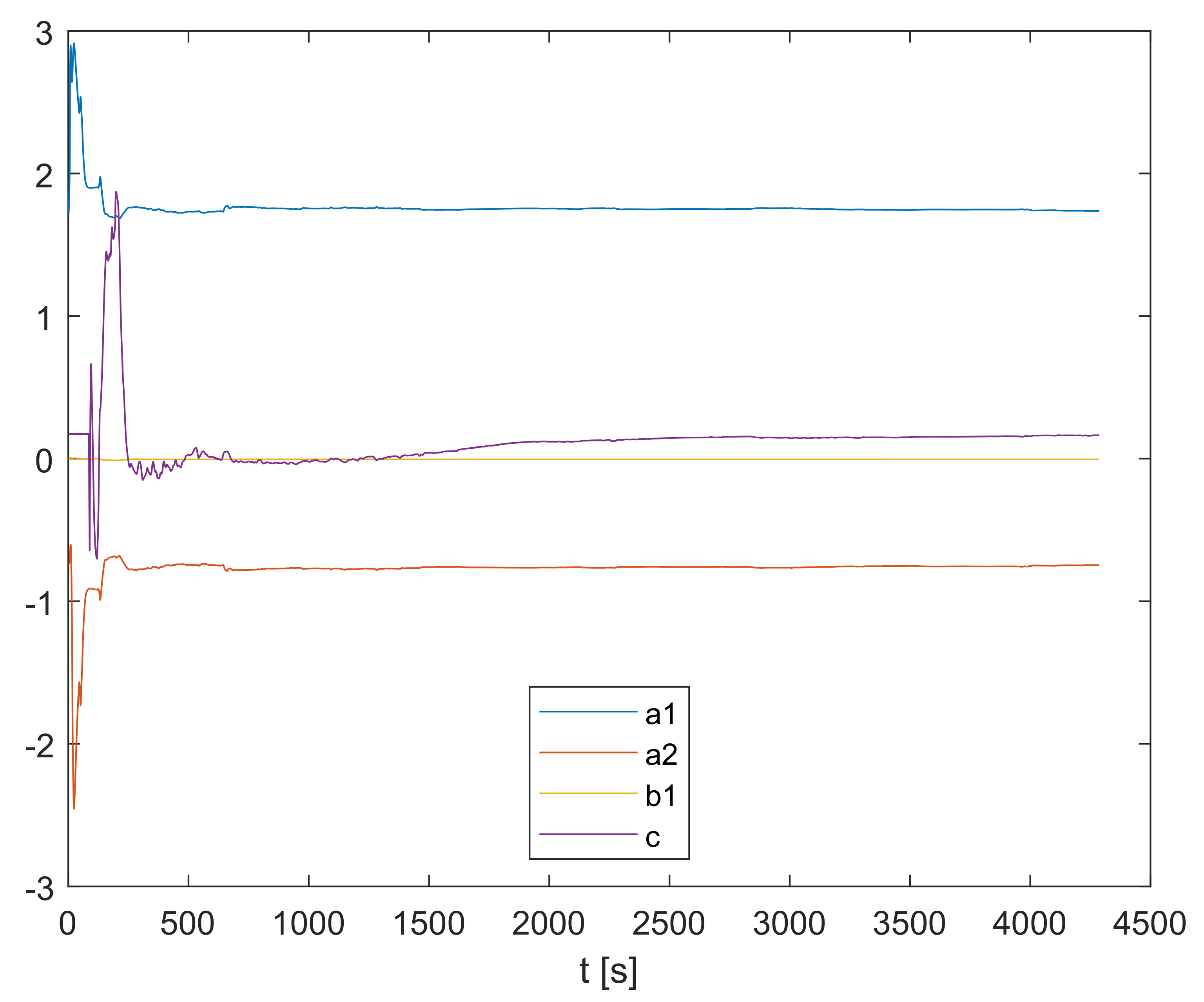
5. Online Recursive Parameter Estimation
6. Model Validation Based on Real Clinical Data
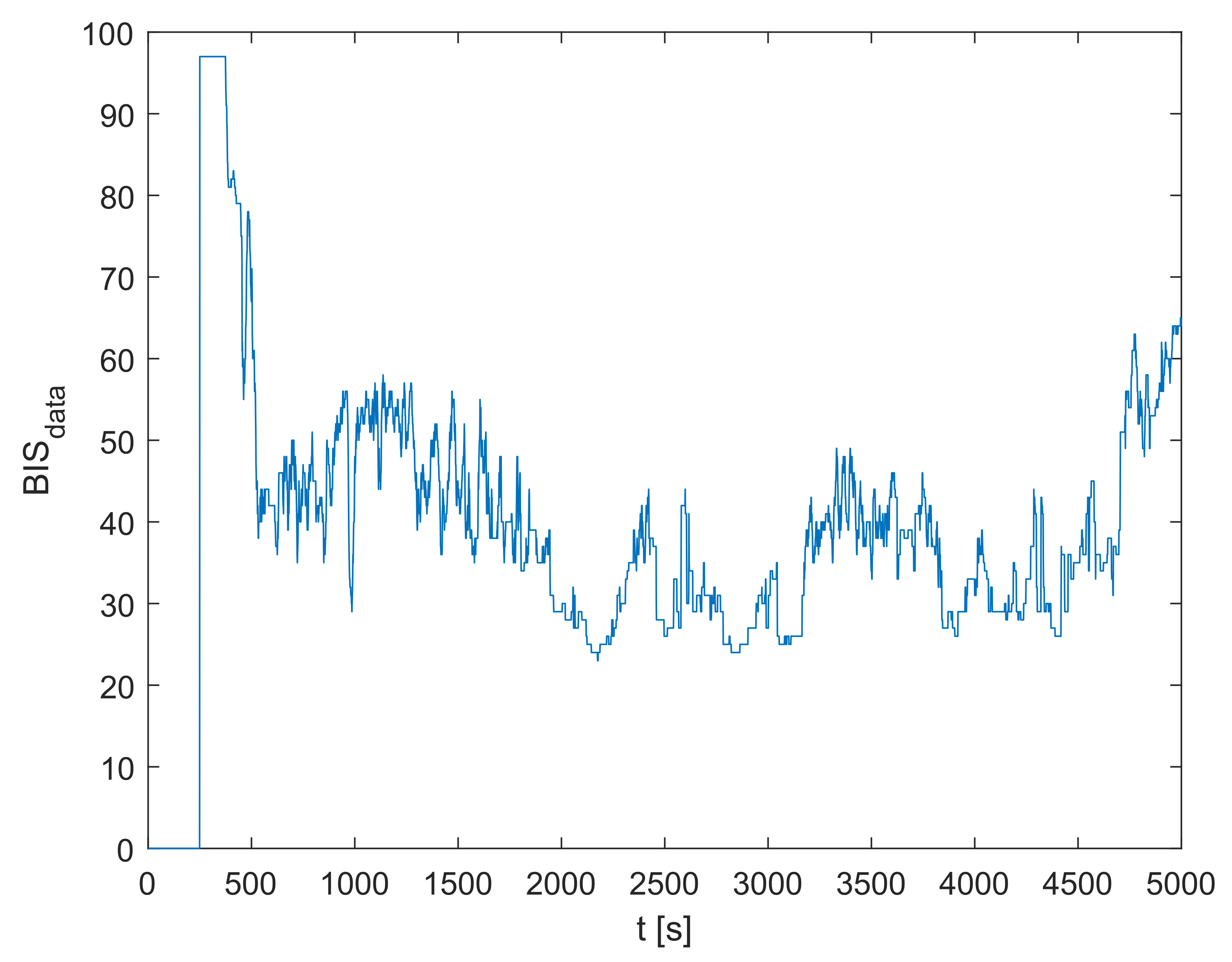
6.1. Recorded Signals
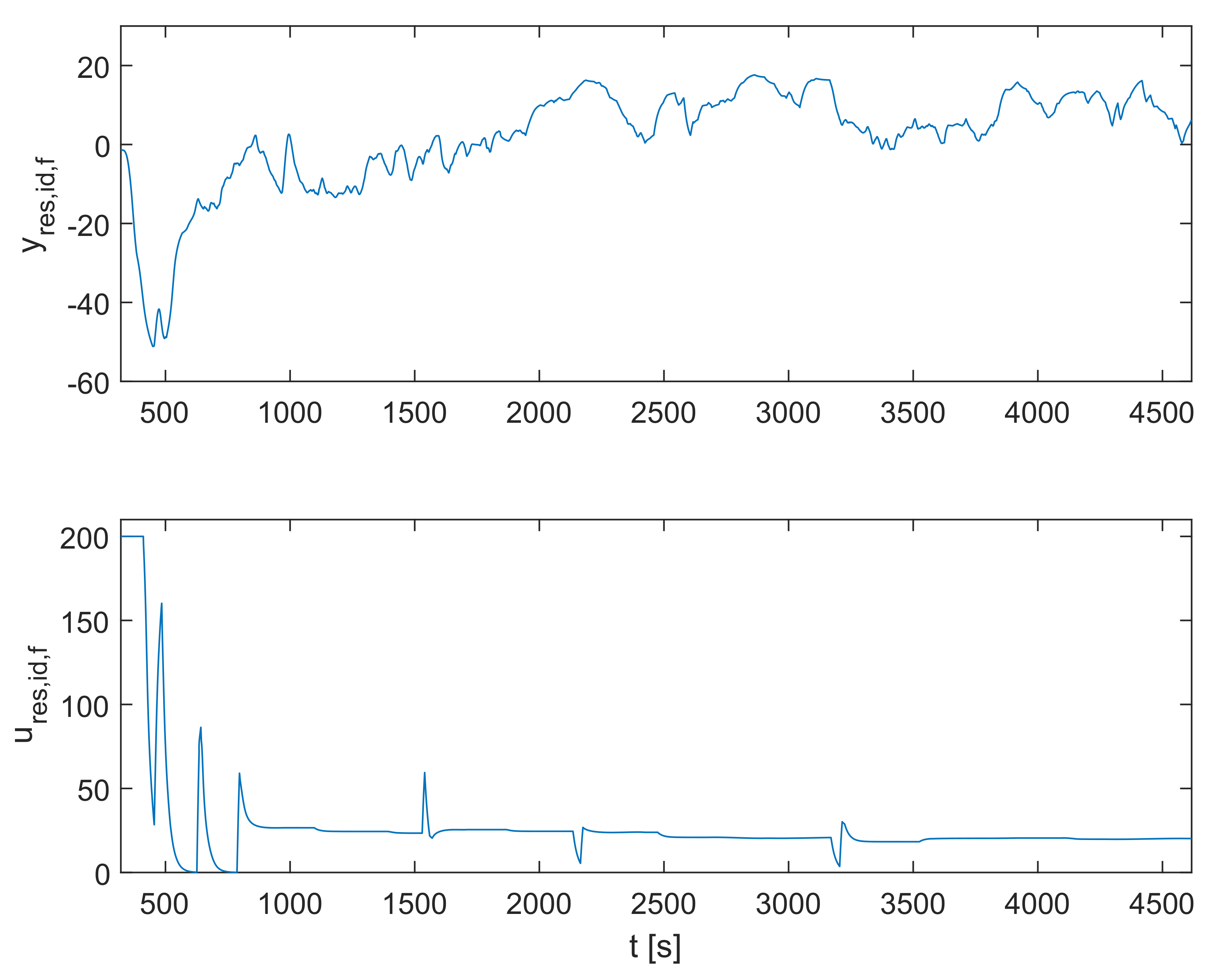
6.2. Identification Results
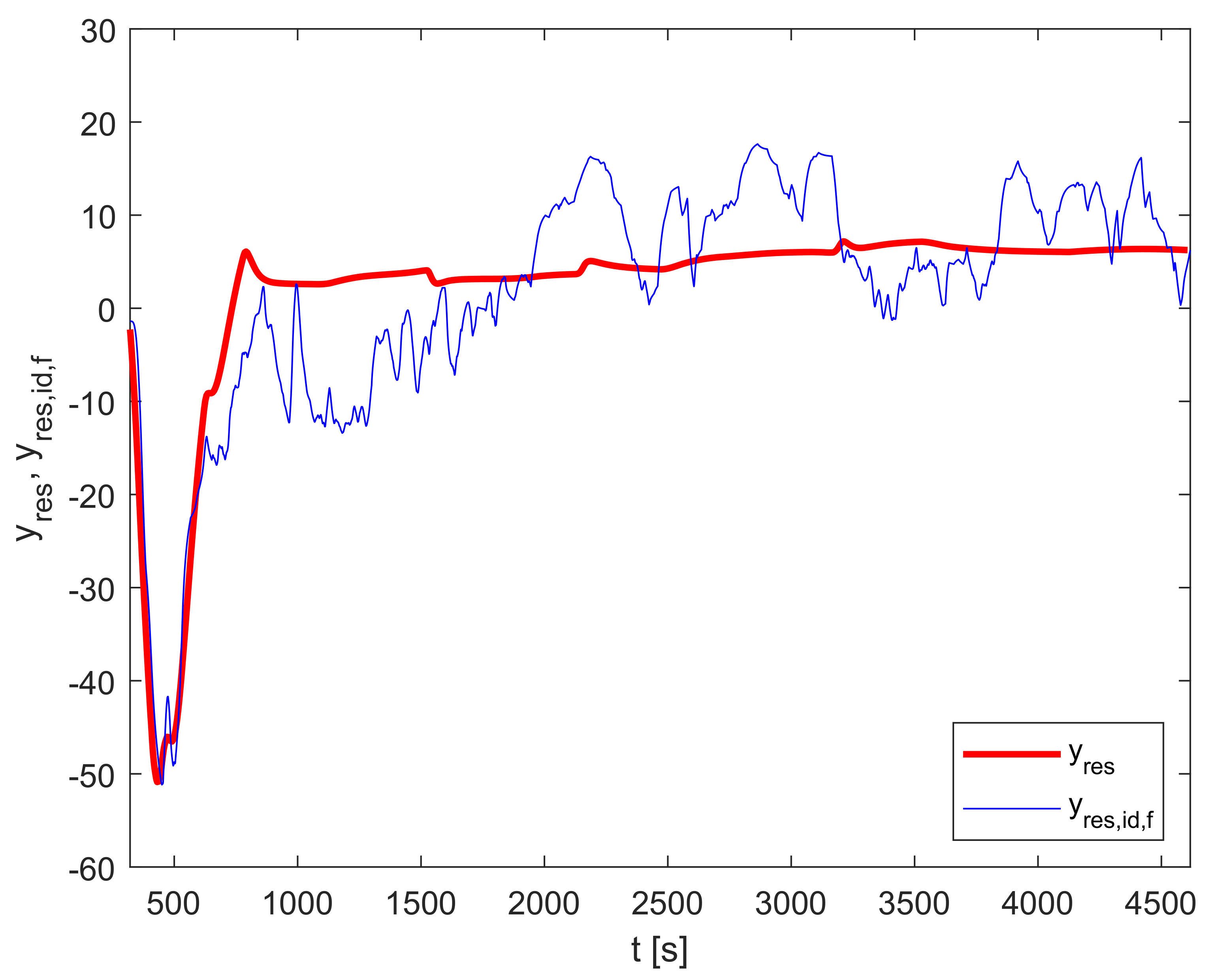
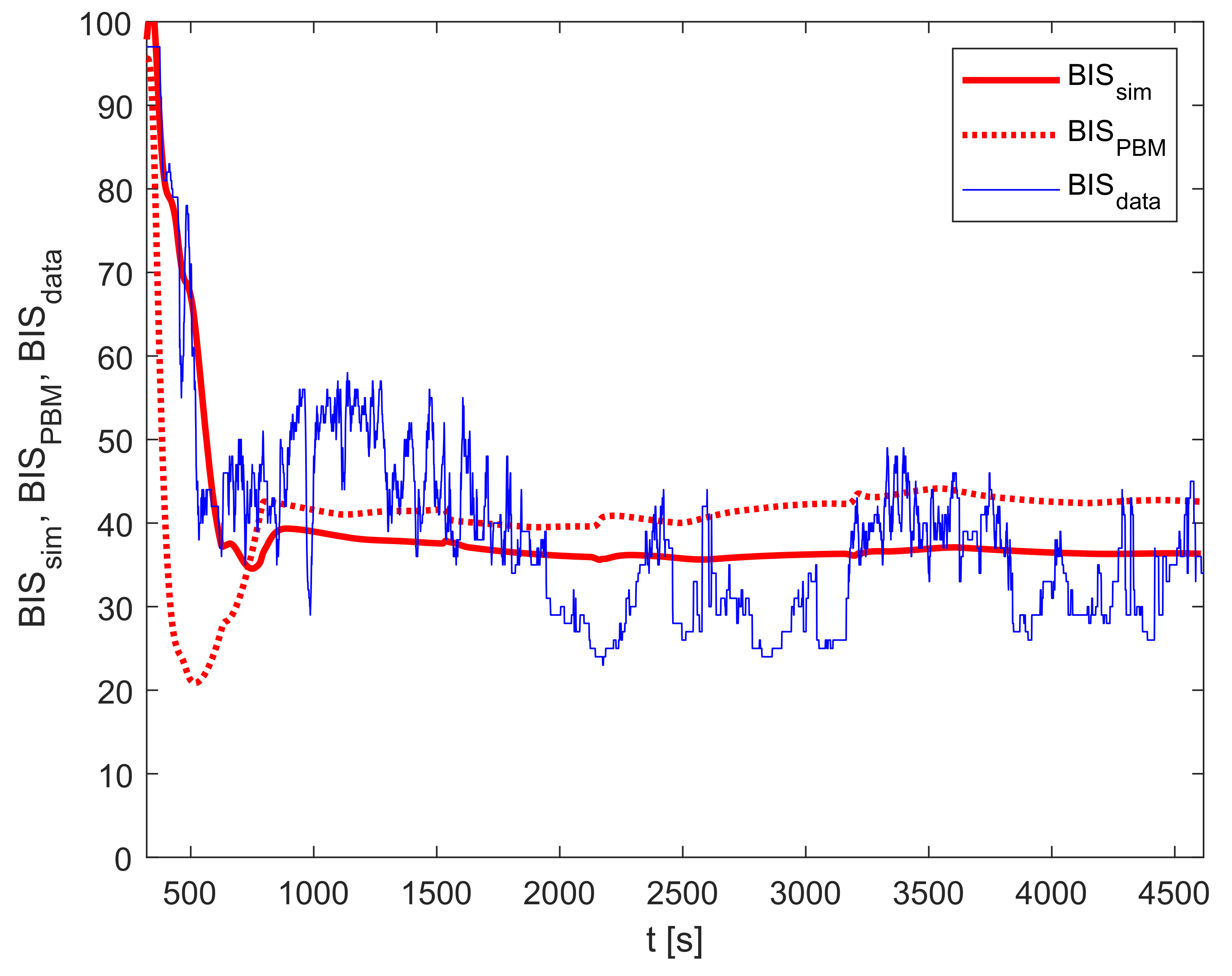
6.3. Model Validation
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Al-Rifai, Z.; Mulvey, D. Principles of total intravenous anaesthesia: Practical aspects of using total intravenous anaesthesia. BJA Educ. 2016, 16, 276–280. [Google Scholar] [CrossRef] [Green Version]
- Absalom, A.R.; Glen, J.B.; Zwart, G.J.; Schnider, T.W.; Struys, M.M. Target-Controlled Infusion: A Mature Technology. Anesth. Analg. 2016, 122, 70–78. [Google Scholar] [CrossRef]
- Wesselink, E.M.; Kappen, T.H.; Torn, H.M.; Slooter, A.J.; van Klei, W.A. Intraoperative hypotension and the risk of postoperative adverse outcomes: A systematic review. Br. J. Anaesth. 2018, 121, 706–721. [Google Scholar] [CrossRef] [Green Version]
- Tasbihgou, S.R.; Vogels, M.F.; Absalom, A.R. Accidental awareness during general anaesthesia–A narrative review. Anaesthesia 2018, 73, 112–122. [Google Scholar] [CrossRef]
- Potočnik, I.; Janković, V.N.; Štupnik, T.; Kremžar, B. Haemodynamic changes after induction of anaesthesia with sevoflurane vs. propofol. Signa Vitae 2011, 6, 52–57. [Google Scholar]
- Musizza, B.; Ribaric, S. Monitoring the Depth of Anaesthesia. Sensors 2010, 10, 10896–10935. [Google Scholar] [CrossRef]
- Hoymork, S.C.; Raeder, J.; Grimsmo, B.; Steen, P.A. Bispectral index, serum drug concentrations and emergence associated with individually adjusted target-controlled infusions of remifentanil and propofol for laparoscopic surgery. Br. J. Anaesth. 2003, 91, 773–780. [Google Scholar] [CrossRef] [Green Version]
- Sleigh, J.W. Depth of AnesthesiaPerhaps the Patient Isn’t a Submarine. Anesthesiology 2011, 115, 1149–1150. [Google Scholar] [CrossRef] [Green Version]
- Kataria, B.K.; Ved, S.A.; Nicodemus, H.F.; Hoy, G.R.; Lea, D.; Dubois, M.Y.; Mandema, J.W.; Shafer, S.L. The pharmacokinetics of propofol in children using three different data analysis approaches. Anesthesiology 1994, 80, 104–122. [Google Scholar] [CrossRef]
- Schüttler, J.; Ihmsen, H. Population pharmacokinetics of propofol: A multicenter study. Anesthesiology 2000, 92, 727–738. [Google Scholar] [CrossRef] [Green Version]
- Kenny, G.N.; White, M. Intravenous propofol anaesthesia using a computerised infusion system. Anaesthesia 1990, 46, 204–209. [Google Scholar] [CrossRef]
- Eleveld, D.J.; Colin, P.; Absalom, A.R.; Struys, M.M. Pharmacokinetic–pharmacodynamic model for propofol for broad application in anaesthesia and sedation. Br. J. Anaesth. 2018, 120, 942–959. [Google Scholar] [CrossRef]
- Neckebroek, M.; Ionescu, C.M.; van Amsterdam, K.; Smet, T.D.; Baets, P.D.; Decruyenaere, J.; Keyser, R.D.; Struys, M.M. A comparison of propofol-to-BIS post-operative intensive care sedation by means of target controlled infusion, Bayesian-based and predictive control methods: An observational, open-label pilot study. J. Clin. Monit. Comput. 2019, 33, 675–686. [Google Scholar] [CrossRef] [Green Version]
- Ionescu, C.M.; Neckebroek, M.; Ghita, M.; Copot, D. An Open Source Patient Simulator for Design and Evaluation of Computer Based Multiple Drug Dosing Control for Anesthetic and Hemodynamic Variables. IEEE Access 2021. [Google Scholar] [CrossRef]
- Brogi, E.; Cyr, S.; Kazan, R.; Giunta, F.; Hemmerling, T.M. Clinical Performance and Safety of Closed-Loop Systems. Anesth. Analg. 2017, 124, 446–455. [Google Scholar] [CrossRef]
- Zaouter, C.; Joosten, A.; Rinehart, J.; Struys, M.M.; Hemmerling, T.M. Autonomous systems in anesthesia: Where do we stand in 2020? A narrative review. Anesth. Analg. 2020, 1120–1132. [Google Scholar] [CrossRef]
- Pasin, L.; Nardelli, P.; Pintaudi, M.; Greco, M.; Zambon, M.; Cabrini, L.; Zangrillo, A. Closed-loop delivery systems versus manually controlled administration of total IV Anesthesia: A meta-analysis of randomized clinical trials. Anesth. Analg. 2017, 124, 456–464. [Google Scholar] [CrossRef]
- Ghita, M.; Neckebroek, M.; Juchem, J.; Copot, D.; Muresan, C.I.; Ionescu, C.M. Bioimpedance Sensor and Methodology for Acute Pain Monitoring. Sensors 2020, 20, 6765. [Google Scholar] [CrossRef]
- Puri, G.D.; Kumar, B.; Aveek, J. Closed-loop anaesthesia delivery system (CLADS™) using bispectral index: A performance assessment study. Anaesth. Intensive Care 2007, 35, 357–362. [Google Scholar] [CrossRef] [Green Version]
- Liu, N.; Chazot, T.; Trillat, B.; Pirracchio, R.; Law-Koune, J.D.; Barvais, L.; Fischler, M. Feasibility of closed-loop titration of propofol guided by the Bispectral Index for general anaesthesia induction: A prospective randomized study. Eur. J. Anaesthesiol. 2006, 23, 465–469. [Google Scholar] [CrossRef]
- Marsh, B.; White, M.; Morton, N.; Kenny, G.N. Pharmacokinetic model driven infusion of propofol in children. Br. J. Anaesth. 1991, 67, 41–48. [Google Scholar] [CrossRef]
- Schnider, T.W.; Minto, C.F.; Gambus, P.L.; Andresen, C.; Goodale, D.B.; Shafer, S.L.; Youngs, E.J. The influence of method of administration and covariates on the pharmacokinetics of propofol in adult volunteers. Anesthesiology 1998, 88, 1170–1182. [Google Scholar] [CrossRef]
- Schnider, T.W.; Minto, C.F.; Shafer, S.L.; Gambus, P.L.; Andresen, C.; Goodale, D.B.; Youngs, E.J. The influence of age on propofol pharmacodynamics. Anesthesiology 1999, 90, 1502–1516. [Google Scholar] [CrossRef]
- Bauer, M.; Wilhelm, W.; Kraemer, T.; Kreuer, S.; Brandt, A.; Adams, H.A.; Hoff, G.; Larsen, R. Impact of bispectral index monitoring on stress response and propofol consumption in patients undergoing coronary artery bypass surgery. Anesthesiology 2004, 101, 1096–1104. [Google Scholar] [CrossRef] [Green Version]
- Kurita, T.; Morita, K.; Kazama, T.; Sato, S. Influence of cardiac output on plasma propofol concentrations during constant infusion in swine. Anesthesiology 2002, 96, 1498–1503. [Google Scholar] [CrossRef]
- Kurita, T.; Uraoka, M.; Jiang, Q.; Suzuki, M.; Morishima, Y.; Morita, K.; Sato, S. Influence of cardiac output on the pseudo-steady state remifentanil and propofol concentrations in swine. Acta Anaesthesiol. Scand. 2013, 57, 754–760. [Google Scholar] [CrossRef]
- Blažič, A.; Škrjanc, I.; Logar, V. Soft sensor of bath temperature in an electric arc furnace based on a data-driven Takagi–Sugeno fuzzy model. Appl. Soft Comput. 2021, 113, 107949. [Google Scholar] [CrossRef]
- Nogueira, F.N.; Mendonça, T.; Rocha, P. Positive state observer for the automatic control of the depth of anesthesia—Clinical results. Comput. Methods Programs Biomed. 2019, 171, 99–108. [Google Scholar] [CrossRef] [Green Version]
- Schiavo, M.; Padula, F.; Latronico, N.; Paltenghi, M.; Visioli, A. A modified PID-based control scheme for depth-of-hypnosis control: Design and experimental results. Comput. Methods Programs Biomed. 2022, 219, 106763. [Google Scholar] [CrossRef]
- Padula, F.; Ionescu, C.; Latronico, N.; Paltenghi, M.; Visioli, A.; Vivacqua, G. Optimized PID control of depth of hypnosis in anesthesia. Comput. Methods Programs Biomed. 2017, 144, 21–35. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Cava, J.M.; Carlson, F.B.; Troeng, O.; Cervin, A.; van Heusden, K.; Dumont, G.A.; Soltesz, K. Robust PID control of propofol anaesthesia: Uncertainty limits performance, not PID structure. Comput. Methods Programs Biomed. 2021, 198, 105783. [Google Scholar] [CrossRef]
- Hosseinzadeh, M. Robust control applications in biomedical engineering: Control of depth of hypnosis. Control. Appl. Biomed. Eng. Syst. 2020, 89–125. [Google Scholar] [CrossRef]
- Dumont, G.A.; Martinez, A.; Ansermino, J.M. Robust control of depth of anesthesia. Int. J. Adapt. Control. Signal Process. 2009, 23, 435–454. [Google Scholar] [CrossRef]
- Heusden, K.V.; Dumont, G.A.; Soltesz, K.; Petersen, C.L.; Umedaly, A.; West, N.; Ansermino, J.M. Design and clinical evaluation of robust PID control of propofol anesthesia in children. IEEE Trans. Control. Syst. Technol. 2014, 22, 491–501. [Google Scholar] [CrossRef] [Green Version]
- Sawaguchi, Y.; Furutani, E.; Shirakami, G.; Araki, M.; Fukuda, K. A model-predictive hypnosis control system under total intravenous anesthesia. IEEE Trans. Biomed. Eng. 2008, 55, 874–887. [Google Scholar] [CrossRef] [Green Version]
- Pawłowski, A.; Schiavo, M.; Latronico, N.; Paltenghi, M.; Visioli, A. Model predictive control using MISO approach for drug co-administration in anesthesia. J. Process. Control 2022, 117, 98–111. [Google Scholar] [CrossRef]
- Mendez, J.A.; Leon, A.; Marrero, A.; Gonzalez-Cava, J.M.; Reboso, J.A.; Estevez, J.I.; Gomez-Gonzalez, J.F. Improving the anesthetic process by a fuzzy rule based medical decision system. Artif. Intell. Med. 2018, 84, 159–170. [Google Scholar] [CrossRef]
- Merigo, L.; Beschi, M.; Padula, F.; Latronico, N.; Paltenghi, M.; Visioli, A. Event-Based control of depth of hypnosis in anesthesia. Comput. Methods Programs Biomed. 2017, 147, 63–83. [Google Scholar] [CrossRef] [Green Version]
- Neckebroek, M.; Ghita, M.; Ghita, M.; Copot, D.; Ionescu, C.M. Pain Detection with Bioimpedance Methodology from 3-Dimensional Exploration of Nociception in a Postoperative Observational Trial. J. Clin. Med. 2020, 9, 684. [Google Scholar] [CrossRef] [Green Version]
- Janda, M.; Schubert, A.; Bajorat, J.; Hofmockel, R.; Nöldge-Schomburg, G.F.; Lampe, B.P.; Simanski, O. Design and implementation of a control system reflecting the level of analgesia during general anesthesia. Biomed. Tech. 2013, 58, 1–11. [Google Scholar] [CrossRef]
- Hemmerling, T.M.; Arbeid, E.; Wehbe, M.; Cyr, S.; Taddei, R.; Zaouter, C.; Reilly, C.S. Evaluation of a novel closed-loop total intravenous anaesthesia drug delivery system: A randomized controlled trial. Br. J. Anaesth. 2013, 110, 1031–1039. [Google Scholar] [CrossRef] [PubMed]
- Peñaranda, C.C.; Arroyave, F.D.C.; Gómez, F.J.; Corredor, P.A.P.; Fernández, J.M.; Botero, M.V.; Bedoya, J.D.B.; Toro, C.M. Technical and clinical evaluation of a closed loop TIVA system with SEDLineTM spectral density monitoring: Multicentric prospective cohort study. Perioper. Med. 2020, 9, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Karer, G. Modelling of Target-Controlled Infusion of Propofol for Depth-of-Anaesthesia Simulation in Matlab-Simulink. In Proceedings of The 9th EUROSIM Congress on Modelling and Simulation, EUROSIM 2016, The 57th SIMS Conference on Simulation and Modelling SIMS 2016; Linköping University Electronic Press: Linköping, Sweden, 2018; Volume 142, pp. 49–54. [Google Scholar] [CrossRef]
- Karer, G.; Novak-Jankovič, V.; Stecher, A.; Potočnik, I. Modelling of BIS-Index Dynamics for Total Intravenous Anesthesia Simulation in Matlab-Simulink. IFAC PapersOnLine 2018, 51, 355–360. [Google Scholar] [CrossRef]
- Ni, K.; Cooter, M.; Gupta, D.K.; Thomas, J.; Hopkins, T.J.; Miller, T.E.; James, M.L.; Kertai, M.D.; Berger, M. Paradox of age: Older patients receive higher age-adjusted minimum alveolar concentration fractions of volatile anaesthetics yet display higher bispectral index values. Br. J. Anaesth. 2019, 123, 288–297. [Google Scholar] [CrossRef]
- Kreuzer, M.; Stern, M.A.; Hight, D.; Berger, S.; Schneider, G.; Sleigh, J.W.; Garciá, P.S. Spectral and Entropic Features Are Altered by Age in the Electroencephalogram in Patients under Sevoflurane Anesthesia. Anesthesiology 2020, 132, 1003–1016. [Google Scholar] [CrossRef]
- Goutelle, S.; Maurin, M.; Rougier, F.; Barbaut, X.; Bourguignon, L.; Ducher, M.; Maire, P. The Hill equation: A review of its capabilities in pharmacological modelling. Fundam. Clin. Pharmacol. 2008, 22, 633–648. [Google Scholar] [CrossRef]
- Operator’s Guide: Infusion Workstation: Orchestra Base Primea. Available online: https://www.google.com.hk/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwiUuIrb1Jb8AhWmr1YBHV7oAjAQFnoECAkQAQ&url=http%3A%2F%2Fwww.frankshospitalworkshop.com%2Fequipment%2Fdocuments%2Finfusion_pumps%2Fuser_manuals%2FFresenius%2520Orchestra%2520Base%2520Unit%2520-%2520User%2520manual.pdf&usg=AOvVaw0-StEgOXitUKevQvWEwzsx (accessed on 26 October 2022).
- Martín-Mateos, I.; Méndez, J.A.; Reboso, J.A.; Leõn, A. Modelling propofol pharmacodynamics using BIS-guided anaesthesia. Anaesthesia 2013, 68, 1132–1140. [Google Scholar] [CrossRef]
- Andonovski, G.; Lughofer, E.; Skrjanc, I. Evolving Fuzzy Model Identification of Nonlinear Wiener-Hammerstein Processes. IEEE Access 2021, 9, 158470–158480. [Google Scholar] [CrossRef]
- Škrjanc, I.; Andonovski, G.; Iglesias, J.A.; Sesmero, M.P.; Sanchis, A. Evolving Gaussian on-line clustering in social network analysis. Expert Syst. Appl. 2022, 207, 117881. [Google Scholar] [CrossRef]
- Ožbot, M.; Lughofer, E.; Škrjanc, I. Evolving Neuro-Fuzzy Systems based Design of Experiments in Process Identification. IEEE J. Mag.|IEEE Xplore 2022. [Google Scholar] [CrossRef]
- Åström, K.J.; Wittenmark, B. Adaptive Control, 2nd ed.; Addison-Wesley Publishing Company: Boston, MA, USA, 1995. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| 4.27l | |
| 0.443 + 0.0107·(/kg − 77) − − 0.0159·(/kg − 59) + + 0.0062·(/cm − 177)/min | |
| 0.302 − 0.0056·(/years − 53)/min | |
| 0.196/min | |
| [1.29 − 0.024·(/years − 53)] · ·[18.9 − 0.391·( − 53)]/min | |
| 0.0035/min | |
| 0.456/min |
| Parameter | Value |
|---|---|
| 95.6 | |
| 8.9 | |
| 2.23 | |
| 1.58 |
| Without residual model | N/A | N/A | |
| With residual model | |||
| Improvement | N/A | N/A |
| Without residual model | |||
| With residual model | |||
| Improvement |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karer, G.; Škrjanc, I. Improved Individualized Patient-Oriented Depth-of-Hypnosis Measurement Based on Bispectral Index. Sensors 2023, 23, 293. https://doi.org/10.3390/s23010293
Karer G, Škrjanc I. Improved Individualized Patient-Oriented Depth-of-Hypnosis Measurement Based on Bispectral Index. Sensors. 2023; 23(1):293. https://doi.org/10.3390/s23010293
Chicago/Turabian StyleKarer, Gorazd, and Igor Škrjanc. 2023. "Improved Individualized Patient-Oriented Depth-of-Hypnosis Measurement Based on Bispectral Index" Sensors 23, no. 1: 293. https://doi.org/10.3390/s23010293
APA StyleKarer, G., & Škrjanc, I. (2023). Improved Individualized Patient-Oriented Depth-of-Hypnosis Measurement Based on Bispectral Index. Sensors, 23(1), 293. https://doi.org/10.3390/s23010293