
Development of Debiasing Technique for Lung Nodule Chest X-ray Datasets to Generalize Deep Learning Models
 ,
,  ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
1.1. Related Work
1.2. Importance to the Field
2. Materials and Methods
2.1. Datasets
2.2. Image Pre-Processing Operations
2.2.1. Histogram Equalization
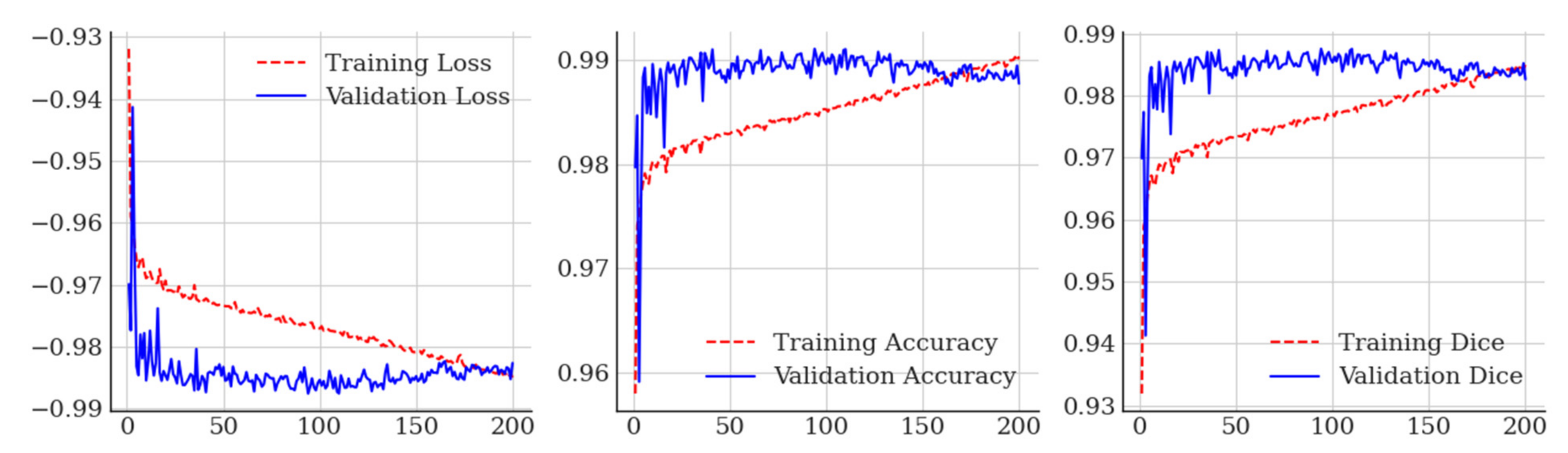
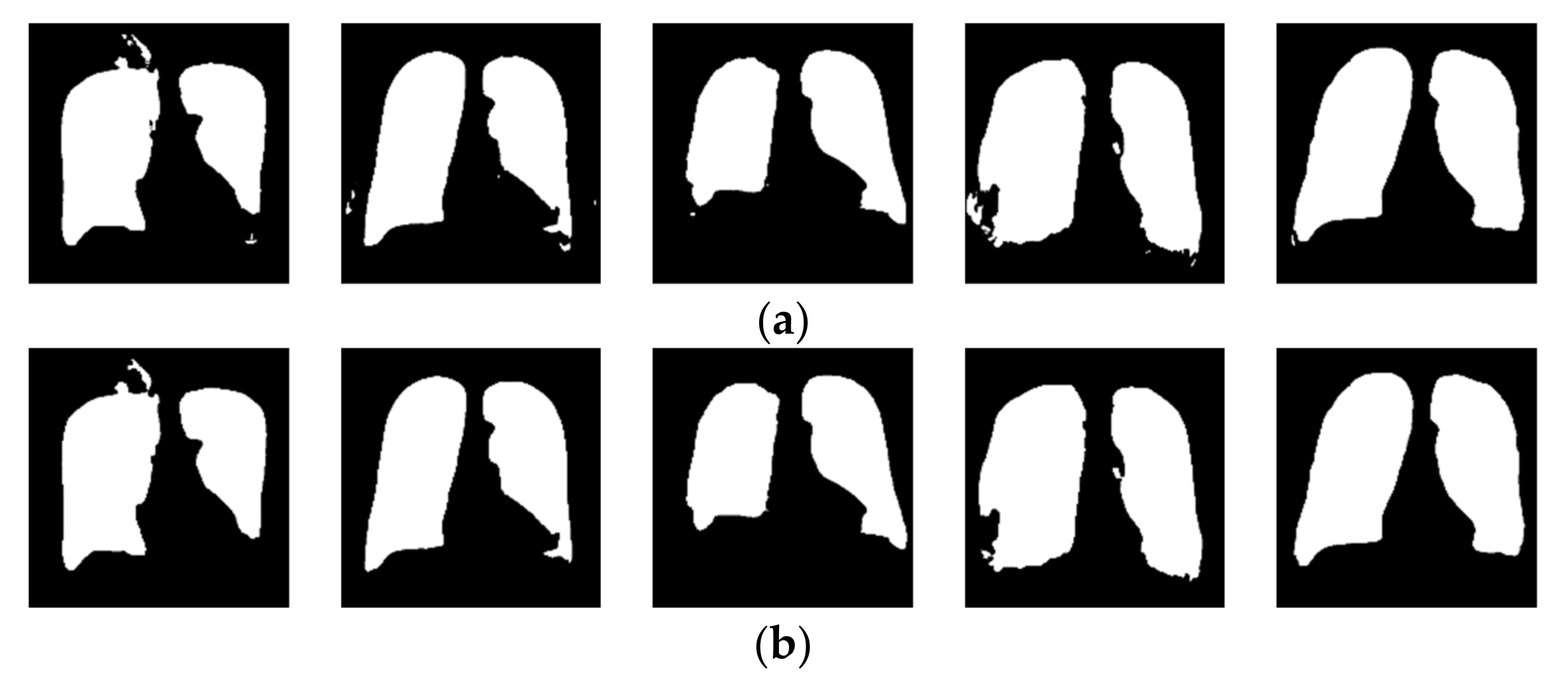
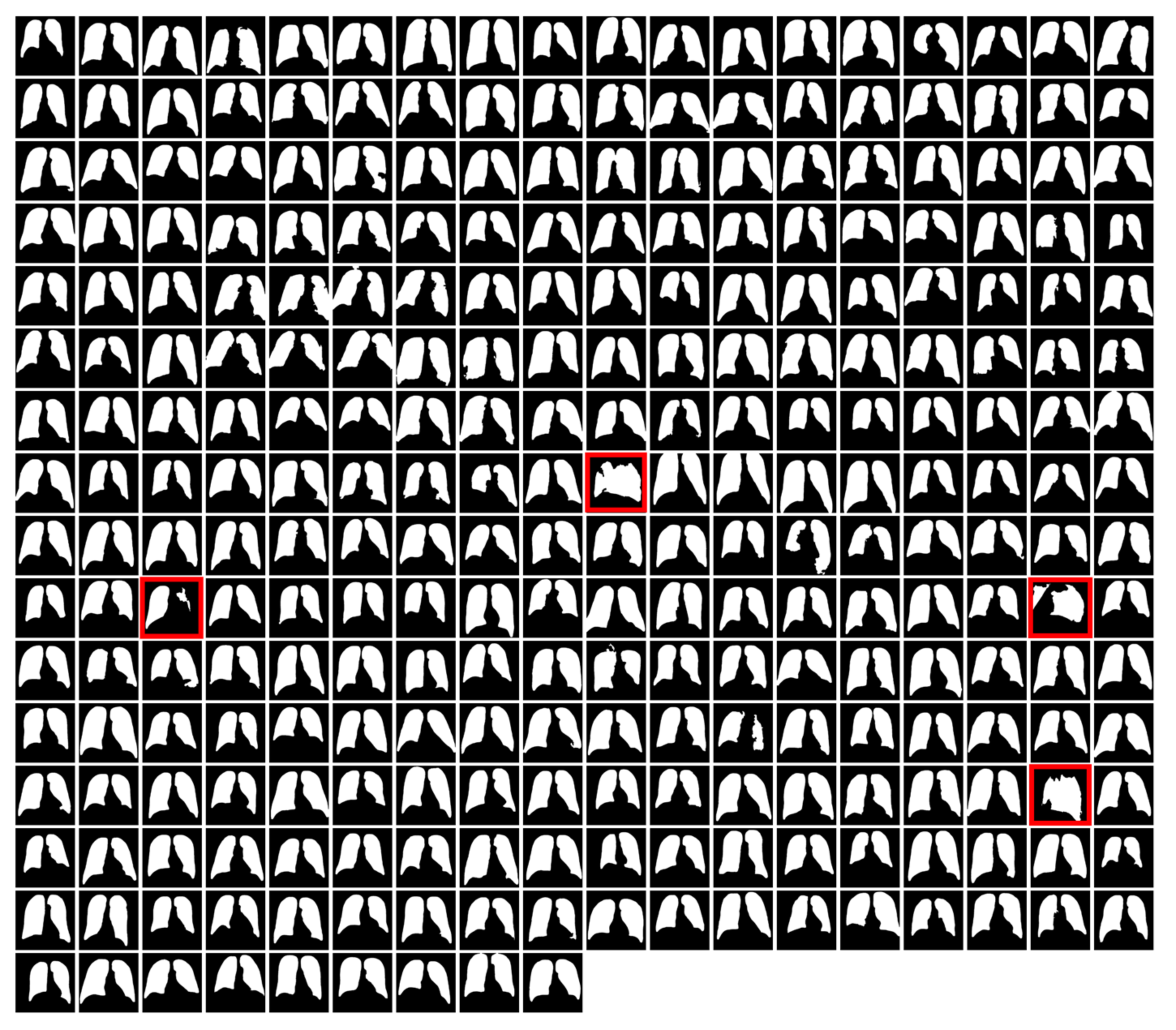
2.2.2. Lung Field Segmentation
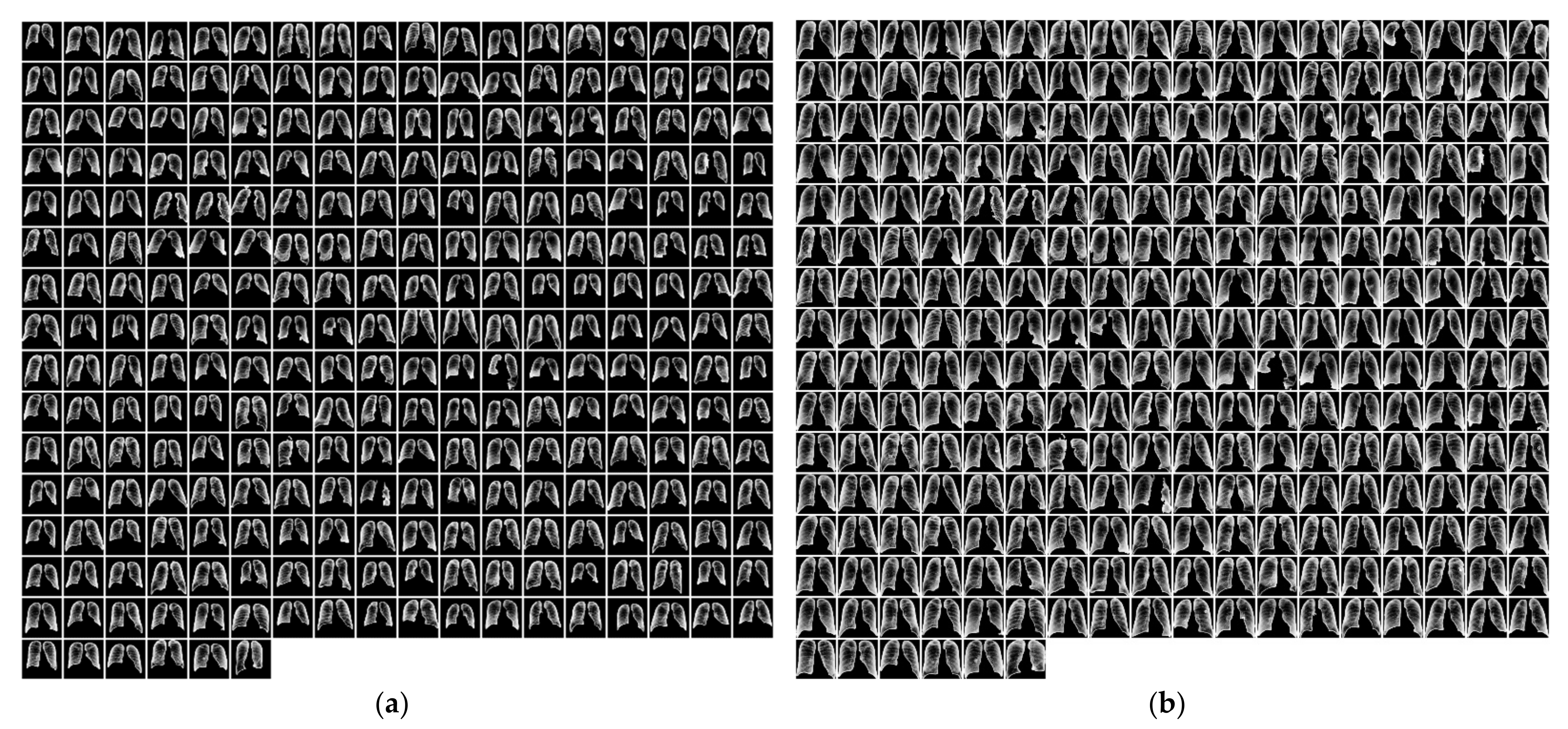
2.2.3. Segmented Lung Field Cropping
2.2.4. Rib and Bone Suppression
2.3. Deep Learning Model
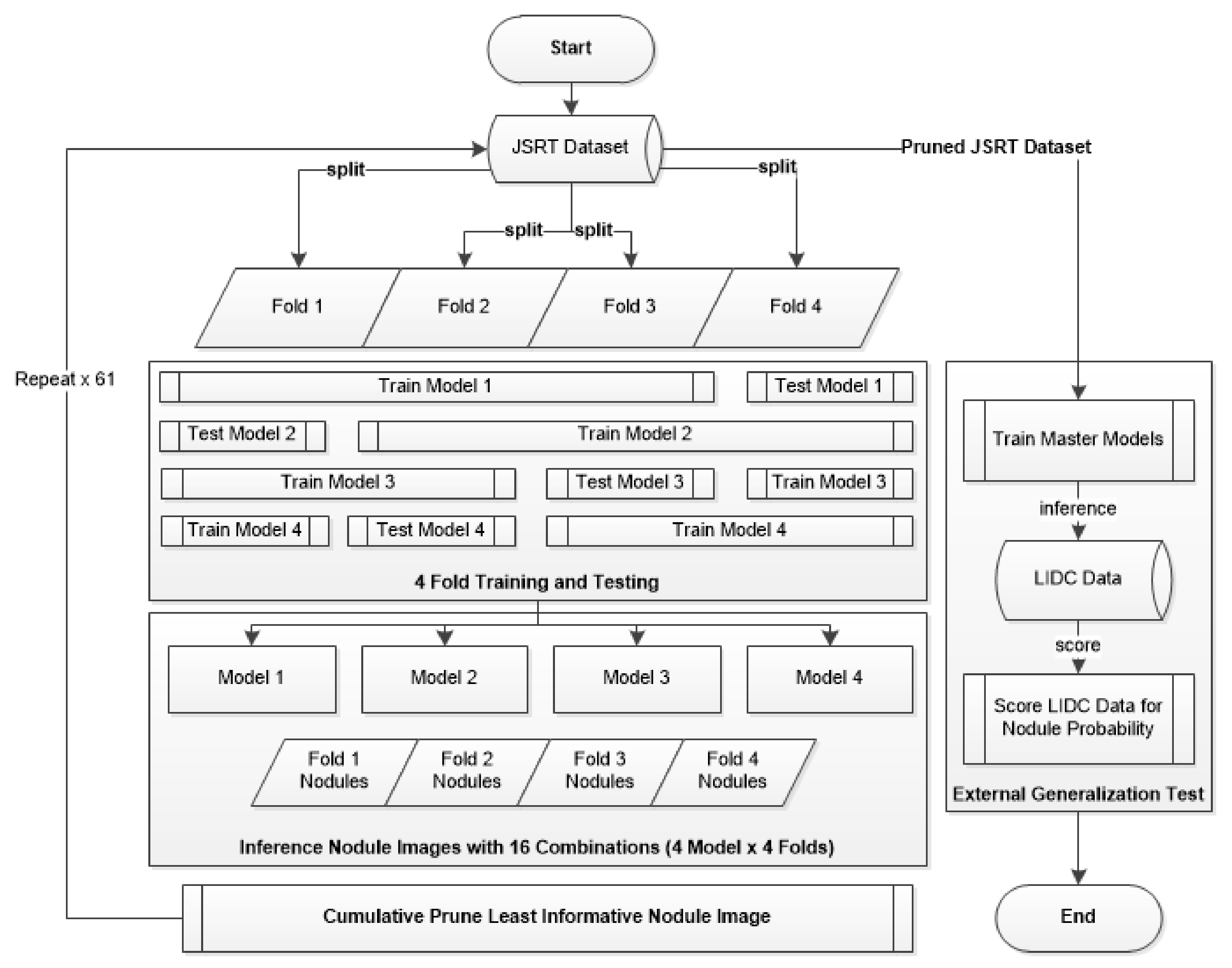
2.4. Evolutionary Pruning Algorithm
2.5. Experiment Setup and Ablation Studies
3. Results
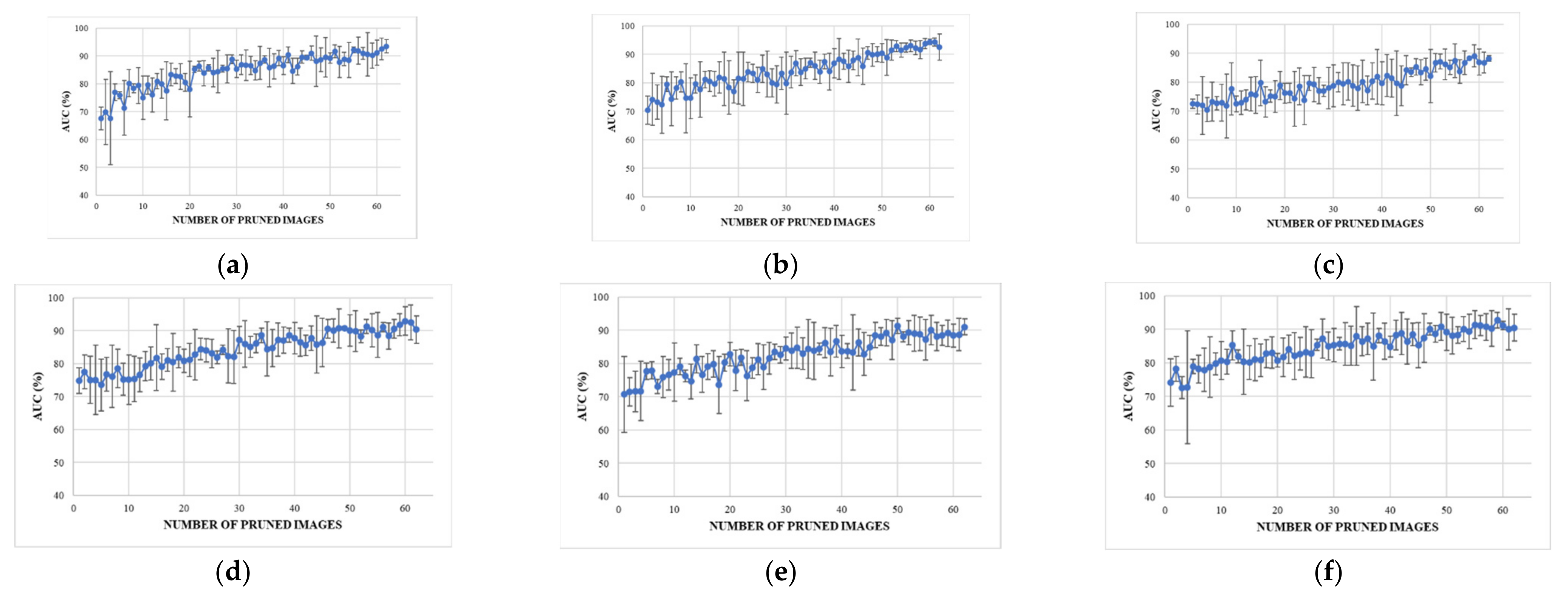
3.1. Internal Four-Fold Training and Testing
3.1.1. Internal Testing Result in A (No Debiasing Operations)
3.1.2. Internal Testing Result B (Rib Suppression Operator)
3.1.3. Internal Testing Result C (Segmentation Operator)
3.1.4. Internal Testing Result D (Segmentation + Rib Suppression Operators)
3.1.5. Internal Testing Result E (Segmentation + Cropping Operators)
3.1.6. Internal Testing Result F (Segmentation + Cropping + Suppression Operators)
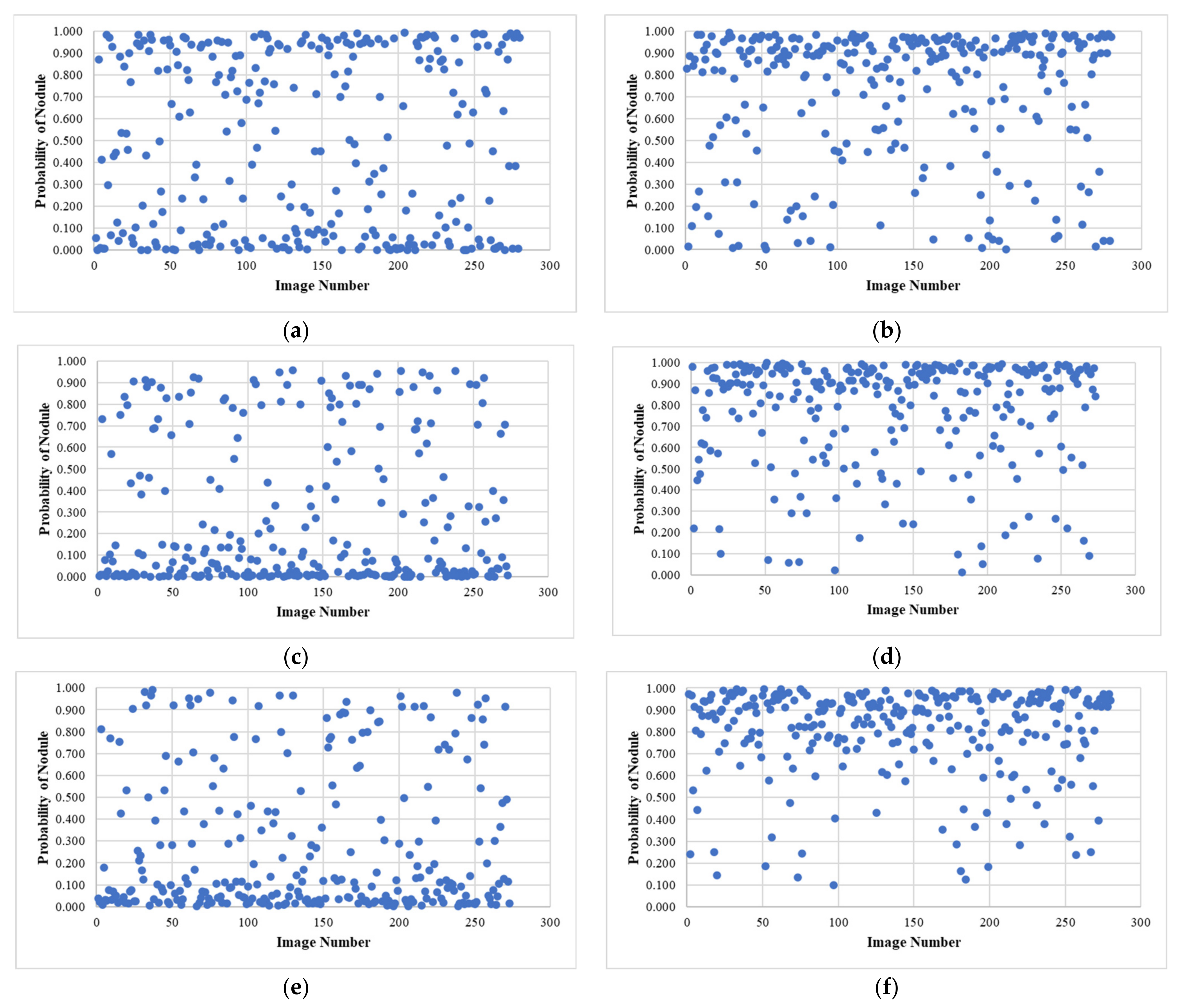
3.2. Pruned Records Analysis (from Experiment F)
3.3. External Testing Evaluation Using Pruned Models
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Fact Sheet—Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 2 November 2021).
- Blandin Knight, S.; Crosbie, P.A.; Balata, H.; Chudziak, J.; Hussell, T.; Dive, C. Progress and prospects of early detection in lung cancer. Open Biol. 2017, 7, 170070. [Google Scholar] [CrossRef]
- Sadate, A.; Occean, B.V.; Beregi, J.-P.; Hamard, A.; Addala, T.; de Forges, H.; Fabbro-Peray, P.; Frandon, J. Systematic review and meta-analysis on the impact of lung cancer screening by low-dose computed tomography. Eur. J. Cancer 2020, 134, 107–114. [Google Scholar] [CrossRef]
- Henschke, C.I.; McCauley, D.I.; Yankelevitz, D.F.; Naidich, D.P.; McGuinness, G.; Miettinen, O.S.; Libby, D.M.; Pasmantier, M.W.; Koizumi, J.; Altorki, N.K.; et al. Early Lung Cancer Action Project: Overall design and findings from baseline screening. Lancet 1999, 354, 99–105. [Google Scholar] [CrossRef]
- Edelman Saul, E.; Guerra, R.B.; Edelman Saul, M.; Lopes da Silva, L.; Aleixo, G.F.P.; Matuda, R.M.K.; Lopes, G. The challenges of implementing low-dose computed tomography for lung cancer screening in low- and middle-income countries. Nat. Cancer 2020, 1, 1140–1152. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Dajac, J.; Kamdar, J.; Moats, A.; Nguyen, B. To Screen or not to Screen: Low Dose Computed Tomography in Comparison to Chest Radiography or Usual Care in Reducing Morbidity and Mortality from Lung Cancer. Cureus 2016, 8, e589. [Google Scholar] [CrossRef]
- Pinsky, P.F. Lung cancer screening with low-dose CT: A world-wide view. Transl. Lung Cancer Res. 2018, 7, 234–242. [Google Scholar] [CrossRef]
- Shankar, A.; Saini, D.; Dubey, A.; Roy, S.; Bharati, S.J.; Singh, N.; Khanna, M.; Prasad, C.P.; Singh, M.; Kumar, S.; et al. Feasibility of lung cancer screening in developing countries: Challenges, opportunities and way forward. Transl. Lung Cancer Res. 2019, 8, S106–S121. [Google Scholar] [PubMed]
- WHO Portable Digital Radiography System: Technical Specifications. Available online: https://www.who.int/publications/i/item/9789240033818 (accessed on 15 November 2021).
- Cavoukian, A. Privacy by Design; Information and Privacy Commissioner of Ontario: Toronto, ON, Canada, 2012; pp. 170–208. [Google Scholar]
- Wahlstrom, K.; Ul-Haq, A.; Burmeister, O. Privacy by design. Australas. J. Inf. Syst. 2020, 24. [Google Scholar] [CrossRef]
- Blanco-Justicia, A.; Domingo-Ferrer, J.; Martínez, S.; Sánchez, D.; Flanagan, A.; Tan, K.E. Achieving security and privacy in federated learning systems: Survey, research challenges and future directions. Eng. Appl. Artif. Intell. 2021, 106, 104468. [Google Scholar] [CrossRef]
- Allaouzi, I.; Ben Ahmed, M. A Novel Approach for Multi-Label Chest X-Ray Classification of Common Thorax Diseases. IEEE Access 2019, 7, 64279–64288. [Google Scholar] [CrossRef]
- Bharati, S.; Podder, P.; Mondal, M.R.H. Hybrid deep learning for detecting lung diseases from X-ray images. Inform. Med. Unlocked 2020, 20, 100391. [Google Scholar] [CrossRef] [PubMed]
- Irvin, J.; Rajpurkar, P.; Ko, M.; Yu, Y.; Ciurea-Ilcus, S.; Chute, C.; Marklund, H.; Haghgoo, B.; Ball, R.; Shpanskaya, K.; et al. CheXpert: A Large Chest Radiograph Dataset with Uncertainty Labels and Expert Comparison. Proc. AAAI Conf. Artif. Intell. 2019, 33, 590–597. [Google Scholar] [CrossRef]
- Pham, H.; Le, T.; Ngo, D.; Tran, D.; Nguyen, H. Interpreting chest X-rays via CNNs that exploit hierarchical disease dependencies and uncertainty labels. Neurocomputing 2021, 437, 186–194. [Google Scholar] [CrossRef]
- Chen, B.; Li, J.; Guo, X.; Lu, G. DualCheXNet: Dual asymmetric feature learning for thoracic disease classification in chest X-rays. Biomed. Signal Process. Control 2019, 53, 101554. [Google Scholar] [CrossRef]
- Dsouza, A.M.; Abidin, A.Z.; Wismüller, A. Automated Identification of Thoracic Pathology from Chest Radiographs with Enhanced Training Pipeline; Mori, K., Hahn, H.K., Eds.; Medical Imaging 2019: Computer-Aided Diagnosis; SPIE: Bellingham, WA, USA, 2019. [Google Scholar]
- Ho, T.; Gwak, J. Multiple Feature Integration for Classification of Thoracic Disease in Chest Radiography. Appl. Sci. 2019, 9, 4130. [Google Scholar] [CrossRef]
- Ivo, M.B.; Hannes, N.; Michael, G.; Tobias, K.; Axel, S. Comparison of Deep Learning Approaches for Multi-Label Chest X-Ray Classification. Sci. Rep. 2019, 9, 6381. [Google Scholar]
- Wang, H.; Wang, S.; Qin, Z.; Zhang, Y.; Li, R.; Xia, Y. Triple attention learning for classification of 14 thoracic diseases using chest radiography. Med. Image Anal. 2021, 67, 101846. [Google Scholar] [CrossRef]
- Wang, X.; Peng, Y.; Lu, L.; Lu, Z.; Bagheri, M.; Summers, R.M. ChestX-Ray8: Hospital-Scale Chest X-Ray Database and Benchmarks on Weakly-Supervised Classification and Localization of Common Thorax Diseases. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 3462–3471. [Google Scholar]
- Liu, H.; Wang, L.; Nan, Y.; Jin, F.; Wang, Q.; Pu, J. SDFN: Segmentation-based deep fusion network for thoracic disease classification in chest X-ray images. Comput. Med. Imaging Graph. 2019, 75, 66–73. [Google Scholar] [CrossRef]
- Mendoza, J.; Pedrini, H. Detection and classification of lung nodules in chest X-ray images using deep convolutional neural networks. Comput. Intell. 2020, 36, 370–401. [Google Scholar] [CrossRef]
- Simkó, G.; Orbán, G.; Máday, P.; Horváth, G. Elimination of clavicle shadows to help automatic lung nodule detection on chest radiographs. In Proceedings of the 4th European Conference of the International Federation for Medical and Biological Engineering, ECIFMBE 2008, Antwerp, Belgium, 23–27 November 2008; pp. 488–491. [Google Scholar]
- Orbán, G.; Horváth, Á.; Horváth, G. Lung nodule detection on Rib eliminated radiographs. In Proceedings of the 12th Mediterranean Conference on Medical and Biological Engineering and Computing, MEDICON 2010, Chalkidiki, Greece, 27–30 May 2010; pp. 363–366. [Google Scholar]
- Horváth, Á.; Orbán, G.; Horváth, G. An X-ray CAD system with ribcage suppression for improved detection of lung lesions. Period. Polytech. Electr. Eng. 2013, 57, 19–33. [Google Scholar] [CrossRef]
- Gang, P.; Zhen, W.; Zeng, W.; Gordienko, Y.; Kochura, Y.; Alienin, O.; Rokovyi, O.; Stirenko, S. Dimensionality reduction in deep learning for chest X-ray analysis of lung cancer. In Proceedings of the 2018 tenth international conference on advanced computational intelligence (ICACI), Xiamen, China, 29–31 March 2018; pp. 878–883. [Google Scholar]
- Robinson, C.; Trivedi, A.; Blazes, M.; Ortiz, A.; Desbiens, J.; Gupta, S.; Dodhia, R.; Bhatraju, P.K.; Liles, W.C.; Lee, A.; et al. Deep learning models for COVID-19 chest X-ray classification: Preventing shortcut learning using feature disentanglement. medRxiv 2021. Preprint. [Google Scholar]
- Zhao, Q.; Adeli, E.; Pohl, K.M. Training confounder-free deep learning models for medical applications. Nat. Commun. 2020, 11, 6010. [Google Scholar] [CrossRef] [PubMed]
- Creager, E.; Madras, D.; Jacobsen, J.-H.; Weis, M.; Swersky, K.; Pitassi, T.; Zemel, R. Flexibly fair representation learning by disentanglement. In Proceedings of the International Conference on Machine Learning, Long Beach, CA, USA, 9–15 June 2019; pp. 1436–1445. [Google Scholar]
- Roy, P.C.; Boddeti, V.N. Mitigating information leakage in image representations: A maximum entropy approach. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Long Beach, CA, USA, 16–20 June 2019; pp. 2586–2594. [Google Scholar]
- Xie, Q.; Dai, Z.; Du, Y.; Hovy, E.; Neubig, G. Controllable Invariance through Adversarial Feature Learning. Adv. Neural Inf. Process. Syst. 2017, 30, 585–596. [Google Scholar]
- DeGrave, A.J.; Janizek, J.D.; Lee, S.-I. AI for radiographic COVID-19 detection selects shortcuts over signal. Nat. Mach. Intell. 2021, 3, 610–619. [Google Scholar] [CrossRef]
- Seyyed-Kalantari, L.; Liu, G.; McDermott, M.; Chen, I.Y.; Ghassemi, M. CheXclusion: Fairness gaps in deep chest X-ray classifiers. Pac. Symp. Biocomput. 2021, 26, 232–243. [Google Scholar]
- Roberts, M.; Driggs, D.; Thorpe, M.; Gilbey, J.; Yeung, M.; Ursprung, S.; Aviles-Rivero, A.I.; Etmann, C.; McCague, C.; Beer, L.; et al. Common pitfalls and recommendations for using machine learning to detect and prognosticate for COVID-19 using chest radiographs and CT scans. Nat. Mach. Intell. 2021, 3, 199–217. [Google Scholar] [CrossRef]
- Abadi, M.; Barham, P.; Chen, J.; Chen, Z.; Davis, A.; Dean, J.; Devin, M.; Ghemawat, S.; Irving, G.; Isard, M.; et al. TensorFlow: A system for large-scale machine learning. In Proceedings of the 12th USENIX Symposium on Operating Systems Design and Implementation, Savannah, GA, USA, 2–4 November 2016; pp. 265–283. [Google Scholar]
- Van Eck, N.J.; Waltman, L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics 2010, 84, 523–538. [Google Scholar] [CrossRef]
- Shiraishi, J.; Katsuragawa, S.; Ikezoe, J.; Matsumoto, T.; Kobayashi, T.; Komatsu, K.-I.; Matsui, M.; Fujita, H.; Kodera, Y.; Doi, K. Development of a Digital Image Database for Chest Radiographs with and without a Lung Nodule. Am. J. Roentgenol. 2000, 174, 71–74. [Google Scholar] [CrossRef]
- Gohagan, J.K.; Prorok, P.C.; Hayes, R.B.; Kramer, B.S. The Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Trial of the National Cancer Institute: History, organization, and status. Control. Clin. Trials 2000, 21, 251S–272S. [Google Scholar] [CrossRef]
- Murphy, K.; van Ginneken, B.; Schilham, A.M.R.; de Hoop, B.J.; Gietema, H.A.; Prokop, M. A large-scale evaluation of automatic pulmonary nodule detection in chest CT using local image features and k-nearest-neighbour classification. Med. Image Anal. 2009, 13, 757–770. [Google Scholar] [CrossRef] [PubMed]
- Van Ginneken, B.; Katsuragawa, S.; Ter Haar Romeny, B.M.; Doi, K.; Viergever, M.A. Automatic detection of abnormalities in chest radiographs using local texture analysis. IEEE Trans. Med. Imaging 2002, 21, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Hardie, R.C.; Rogers, S.K.; Wilson, T.; Rogers, A. Performance analysis of a new computer aided detection system for identifying lung nodules on chest radiographs. Med. Image Anal. 2008, 12, 240–258. [Google Scholar] [CrossRef]
- Suzuki, K.; Abe, H.; MacMahon, H.; Doi, K. Image-processing technique for suppressing ribs in chest radiographs by means of massive training artificial neural network (MTANN). IEEE Trans. Med. Imaging 2006, 25, 406–416. [Google Scholar] [CrossRef]
- Ardila, D.; Kiraly, A.P.; Bharadwaj, S.; Choi, B.; Reicher, J.J.; Peng, L.; Tse, D.; Etemadi, M.; Ye, W.; Corrado, G.; et al. End-to-end lung cancer screening with three-dimensional deep learning on low-dose chest computed tomography. Nat. Med. 2019, 25, 954–961. [Google Scholar] [CrossRef] [PubMed]
- Setio, A.A.A.; Traverso, A.; de Bel, T.; Berens, M.S.N.; Bogaard, C.V.D.; Cerello, P.; Chen, H.; Dou, Q.; Fantacci, M.E.; Geurts, B.; et al. Validation, comparison, and combination of algorithms for automatic detection of pulmonary nodules in computed tomography images: The LUNA16 challenge. Med. Image Anal. 2017, 42, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Schilham, A.M.R.; van Ginneken, B.; Loog, M. A computer-aided diagnosis system for detection of lung nodules in chest radiographs with an evaluation on a public database. Med. Image Anal. 2006, 10, 247–258. [Google Scholar] [CrossRef]
- Suzuki, K.; Shiraishi, J.; Abe, H.; MacMahon, H.; Doi, K. False-positive reduction in computer-aided diagnostic scheme for detecting nodules in chest radiographs by means of massive training artificial neural network. Acad. Radiol. 2005, 12, 191–201. [Google Scholar] [CrossRef]
- Xu, X.W.; Doi, K.; Kobayashi, T.; MacMahon, H.; Giger, M.L. Development of an improved CAD scheme for automated detection of lung nodules in digital chest images. Med. Phys. 1997, 24, 1395–1403. [Google Scholar] [CrossRef]
- Armato, S.G.; McLennan, G.; Bidaut, L.; McNitt-Gray, M.F.; Meyer, C.R.; Reeves, A.P.; Zhao, B.; Aberle, D.R.; Henschke, C.I.; Hoffman, E.A.; et al. The Lung Image Database Consortium (LIDC) and Image Database Resource Initiative (IDRI): A Completed Reference Database of Lung Nodules on CT Scans. Med. Phys. 2011, 38, 915–931. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Munich, Germany, 5–9 October 2015; pp. 234–241. [Google Scholar]
- Mason, D. SU-E-T-33: Pydicom: An open source DICOM library. Med. Phys. 2011, 38, 3493. [Google Scholar] [CrossRef]
- Murphy, A.; Jones, J. Radiographic Contrast. 2018. Available online: https://radiopaedia.org/articles/58718 (accessed on 16 July 2023).
- Shuyue, C.; Honghua, H.; Yanjun, Z.; Xiaomin, X. Study of automatic enhancement for chest radiograph. J. Digit. Imaging 2006, 19, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Zech, J.R.; Badgeley, M.A.; Liu, M.; Costa, A.B.; Titano, J.J.; Oermann, E.K. Variable generalization performance of a deep learning model to detect pneumonia in chest radiographs: A cross-sectional study. PLoS Med. 2018, 15, e1002683. [Google Scholar] [CrossRef] [PubMed]
- Badgeley, M.A.; Zech, J.R.; Oakden-Rayner, L.; Glicksberg, B.S.; Liu, M.; Gale, W.; McConnell, M.V.; Percha, B.; Snyder, T.M.; Dudley, J.T. Deep learning predicts hip fracture using confounding patient and healthcare variables. NPJ Digit. Med. 2019, 2, 31. [Google Scholar] [CrossRef]
- Rabinovich, A.; Vedaldi, A.; Belongie, S. Does Image Segmentation Improve Object Categorization? Cornell University: Ithaca, NY, USA, 2020. [Google Scholar]
- Teixeira, L.O.; Pereira, R.M.; Bertolini, D.; Oliveira, L.S.; Nanni, L.; Cavalcanti, G.D.C.; Costa, Y.M.G. Impact of Lung Segmentation on the Diagnosis and Explanation of COVID-19 in Chest X-ray Images. Sensors 2021, 21, 7116. [Google Scholar] [CrossRef]
- Candemir, S.; Antani, S. A review on lung boundary detection in chest X-rays. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 563–576. [Google Scholar] [CrossRef]
- Hwang, S.; Park, S. Accurate lung segmentation via network-wise training of convolutional networks. In Deep Learning in Medical Image Analysis and Multimodal Learning for Clinical Decision Support; Springer: Berlin/Heidelberg, Germany, 2017; pp. 92–99. [Google Scholar]
- Novikov, A.A.; Lenis, D.; Major, D.; Hladůvka, J.; Wimmer, M.; Bühler, K. Fully Convolutional Architectures for Multi-Class Segmentation in Chest Radiographs. IEEE Trans. Med. Imaging 2017, 37, 1865–1876. [Google Scholar] [CrossRef]
- Jaeger, S.; Candemir, S.; Antani, S.; Wáng, Y.-X.J.; Lu, P.-X.; Thoma, G. Two public chest X-ray datasets for computer-aided screening of pulmonary diseases. Quant. Imaging Med. Surg. 2014, 4, 475–477. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very Deep Convolutional Networks for Large-Scale Image Recognition. arXiv 2015, arXiv:1409.1556. [Google Scholar]
- Huang, G.; Liu, Z.; Maaten, L.V.D.; Weinberger, K.Q. Densely Connected Convolutional Networks. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 2261–2269. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 26 June–1 July 2016; pp. 770–778. [Google Scholar]
- Zhang, Z.; Liu, Q.; Wang, Y. Road Extraction by Deep Residual U-Net. IEEE Geosci. Remote Sens. Lett. 2018, 15, 749–753. [Google Scholar] [CrossRef]
- Alom, M.Z.; Yakopcic, C.; Hasan, M.; Taha, T.; Asari, V. Recurrent residual U-Net for medical image segmentation. J. Med. Imaging 2019, 6, 014006. [Google Scholar] [CrossRef] [PubMed]
- Zuo, Q.; Chen, S.; Wang, Z. R2AU-Net: Attention Recurrent Residual Convolutional Neural Network for Multimodal Medical Image Segmentation. Secur. Commun. Netw. 2021, 2021, 6625688. [Google Scholar] [CrossRef]
- Munawar, F.; Azmat, S.; Iqbal, T.; Grönlund, C.; Ali, H. Segmentation of Lungs in Chest X-Ray Image Using Generative Adversarial Networks. IEEE Access 2020, 8, 153535–153545. [Google Scholar] [CrossRef]
- Souza, J.C.; Bandeira Diniz, J.O.; Ferreira, J.L.; França Da Silva, G.L.; Corrêa Silva, A.; de Paiva, A.C. An automatic method for lung segmentation and reconstruction in chest X-ray using deep neural networks. Comput. Methods Programs Biomed. 2019, 177, 285–296. [Google Scholar] [CrossRef]
- Horváth, Á. Bone Shadow Eliminated Images of the JSRT Database; Budapest University of Technology and Economics (BME): Budapest, Hungary, 2021. [Google Scholar]
- Gusarev, M.; Kuleev, R.; Khan, A.; Rivera, A.R.; Khattak, A.M. Deep learning models for bone suppression in chest radiographs. In Proceedings of the 2017 IEEE Conference on Computational Intelligence in Bioinformatics and Computational Biology (CIBCB), Manchester, UK, 23–25 August 2017; pp. 1–7. [Google Scholar]
- Flam, D. Deep Learning Models for Bone Suppression in Chest Radiographs. Available online: https://github.com/danielnflam/Deep-Learning-Models-for-bone-suppression-in-chest-radiographs (accessed on 16 July 2023).
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Deng, J.; Dong, W.; Socher, R.; Li, L.; Kai, L.; Li, F.-F. ImageNet: A large-scale hierarchical image database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; pp. 248–255. [Google Scholar]
- Horry, M.; Chakraborty, S.; Paul, M.; Ulhaq, A.; Pradhan, B.; Saha, M.; Shukla, N. COVID-19 Detection through Transfer Learning using Multimodal Imaging Data. IEEE Access 2020, 8, 149808–149824. [Google Scholar] [CrossRef]
- Ausawalaithong, W.; Thirach, A.; Marukatat, S.; Wilaiprasitporn, T. Automatic Lung Cancer Prediction from Chest X-ray Images Using the Deep Learning Approach. In Proceedings of the 11th Biomedical Engineering International Conference (BMEiCON), Chiang Mai, Thailand, 21–24 November 2018. [Google Scholar]
- Von Berg, J.; Young, S.; Carolus, H.; Wolz, R.; Saalbach, A.; Hidalgo, A.; Giménez, A.; Franquet, T. A novel bone suppression method that improves lung nodule detection. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 641–655. [Google Scholar] [CrossRef]
- Franchi, P.; Contegiacomo, A.; Cicchetti, G.; Bonomo, L.; Larici, A. Missed lung cancer: When, where, and why? Diagn. Interv. Radiol. 2017, 23, 118–126. [Google Scholar]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cluster | Number of Papers | Central Paper/s | Imaging Mode | Connecting Theme | Data Source |
|---|---|---|---|---|---|
| 1 | 36 | [40,41] | CXR | Connected by the use of JSRT [40] and PLCO [41] datasets as a lung nodule dataset, along with a deep learning approach for image analysis and nodule classification. | JSRT PLCO |
| 2 | 29 | [42,43] | CT/CXR | Connected using local feature analysis, linear filtering, clustering techniques, and other non-deep learning techniques. | LIDC |
| 3 | 24 | [44] | CXR | Artificial intelligence and machine learning methods, including ANN, SVM, and KNN. Typically used the JSRT database. | JSRT |
| 4 | 23 | [45] | CXR | Rib/bone suppression and image enhancement techniques, including wavelet transform methods. | JSRT |
| 5 | 17 | [46,47] | CT | Use of deep learning and shape analysis to diagnose lung cancer from chest CT images. | Luna16 |
| 6 | 12 | [48,49] | CXR | KNN classification of nodules as blobs. Used stratification of JSRT to train/calibrate schemes to reduce false positive detection by algorithms. | JSRT |
| 7 | 12 | [50] | CXR | A set of older papers using various techniques to detect nodules and reduce false-positive detections | Private Data JSRT |
| Dataset | Nodule Image Count | Non-Nodule Image Count | Image Size/Format | Label Accuracy AUC-ROC |
|---|---|---|---|---|
| JSRT | 154 images from 154 patients | 93 images from 93 patients | Universal Image Format 2048 × 2048 12-bit grayscale | 20 radiologists from 4 institutions. 0.833 ± 0.045 |
| LIDC | 280 images from 157 patients | 0 | DICOM Extracted and compressed to 512 × 512 PNG using Pydicom [53] | Not provided |
| Experiment | Segmentation | Cropping | Rib Suppression | Sample Image |
|---|---|---|---|---|
| A | False | False | False |  |
| B | False | False | True |  |
| C | True | False | False |  |
| D | True | False | True |  |
| E | True | True | False |  |
| F | True | True | True |  |
| Filename | Image | JSRT Metadata Notes | Radiologist Observations |
|---|---|---|---|
| JPCLN151.png |  | Extremely subtle 14 mm |
Extremely subtle Behind cardiac silhouette Overlaps vascular marking |
| JPCLN003.png |  | Obvious 30 mm |
Obvious Overlaps vascular markings |
| JPCLN130.png |  | Extremely subtle 30 mm |
Extremely subtle Behind cardiac silhouette |
| JPCLN141.png |  | Extremely subtle 10 mm |
Extremely subtle Behind rib/clavicle |
| JPCLN142.png |  | Extremely subtle 10 mm | Not visible. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Horry, M.J.; Chakraborty, S.; Pradhan, B.; Paul, M.; Zhu, J.; Loh, H.W.; Barua, P.D.; Acharya, U.R. Development of Debiasing Technique for Lung Nodule Chest X-ray Datasets to Generalize Deep Learning Models. Sensors 2023, 23, 6585. https://doi.org/10.3390/s23146585
Horry MJ, Chakraborty S, Pradhan B, Paul M, Zhu J, Loh HW, Barua PD, Acharya UR. Development of Debiasing Technique for Lung Nodule Chest X-ray Datasets to Generalize Deep Learning Models. Sensors. 2023; 23(14):6585. https://doi.org/10.3390/s23146585
Chicago/Turabian StyleHorry, Michael J., Subrata Chakraborty, Biswajeet Pradhan, Manoranjan Paul, Jing Zhu, Hui Wen Loh, Prabal Datta Barua, and U. Rajendra Acharya. 2023. "Development of Debiasing Technique for Lung Nodule Chest X-ray Datasets to Generalize Deep Learning Models" Sensors 23, no. 14: 6585. https://doi.org/10.3390/s23146585
APA StyleHorry, M. J., Chakraborty, S., Pradhan, B., Paul, M., Zhu, J., Loh, H. W., Barua, P. D., & Acharya, U. R. (2023). Development of Debiasing Technique for Lung Nodule Chest X-ray Datasets to Generalize Deep Learning Models. Sensors, 23(14), 6585. https://doi.org/10.3390/s23146585