
Assessment of the Impact of Sensor-Based Ischemic Preconditioning with Different Cycling Periods on Upper Limb Strength in Bodybuilding Athletes

Abstract
:1. Introduction
2. Objective and Methods
2.1. Object
2.2. Methods
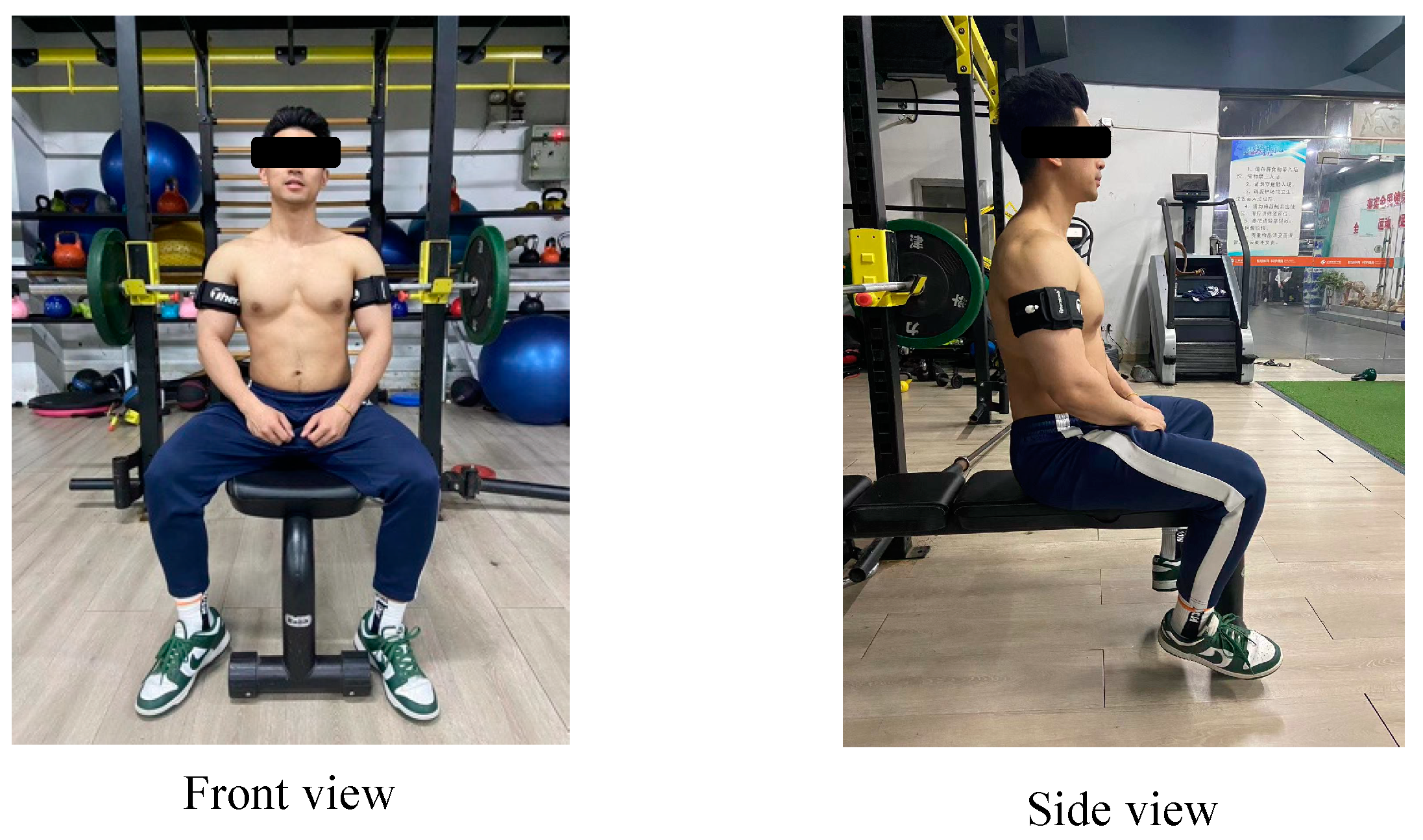
2.2.1. Experimental Design and Process
2.2.2. Main Test and Observation Indicators
2.3. Statistical Analysis
3. Results
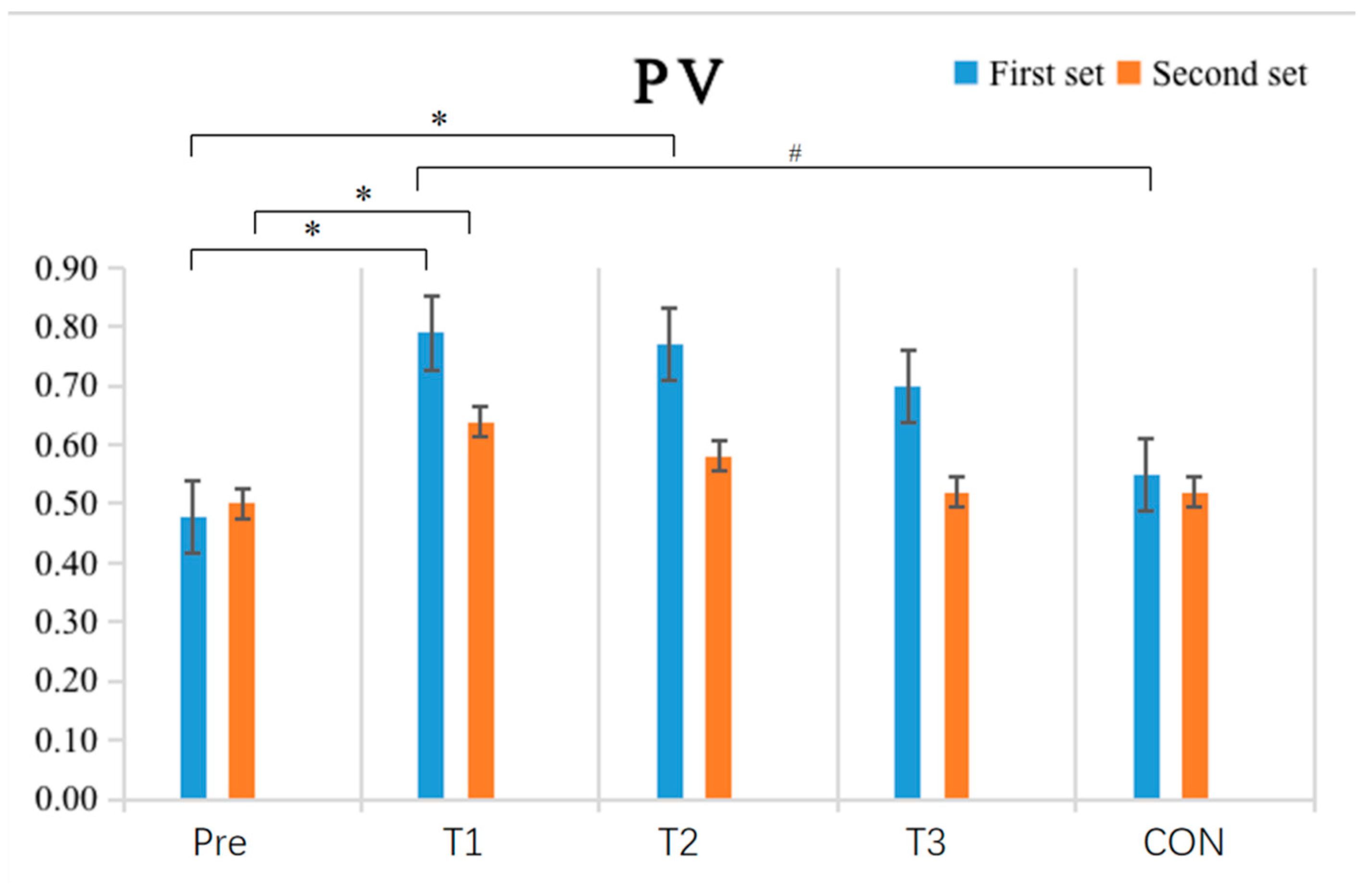
3.1. The Effect of IPC Intervention with Different Cycle Periods on Peak Velocity (PV)
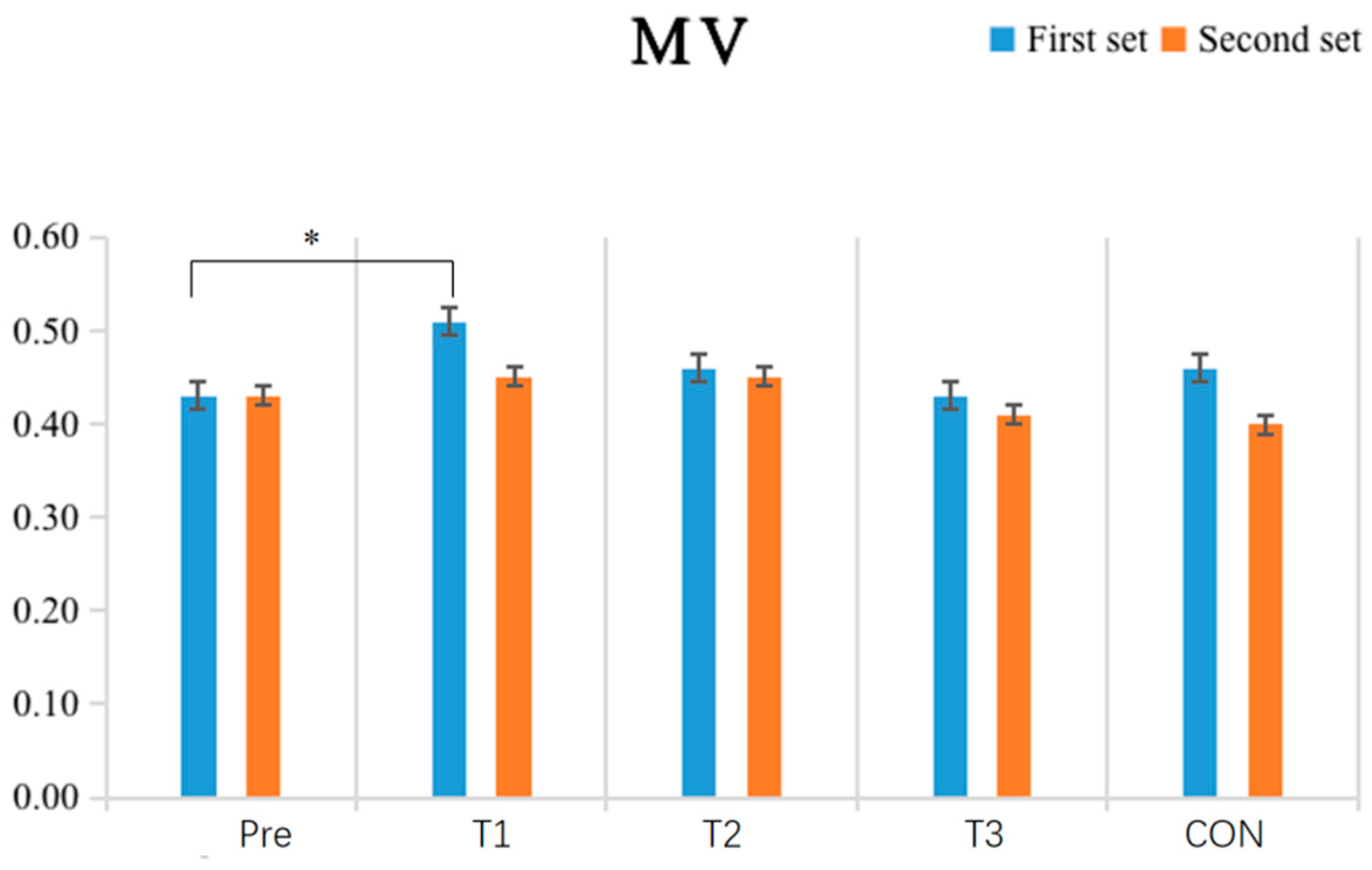
3.2. The Effect of IPC Intervention with Different Cycling Periods on Mean Velocity (MV)
3.3. The Impact of IPC Intervention with Different Cycling Periods on Peak Power (PP)
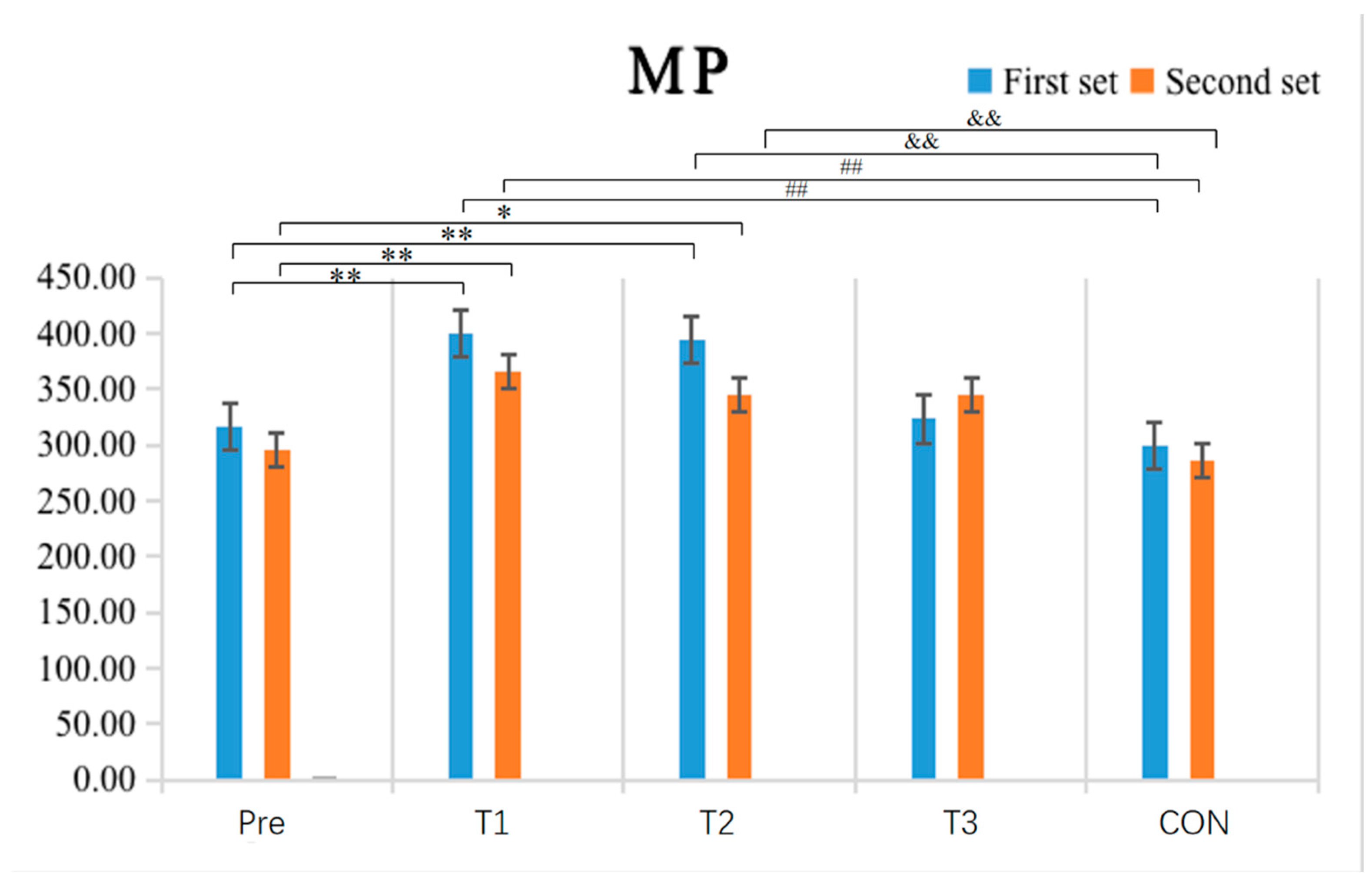
3.4. The Impact of IPC Intervention with Different Cycling Periods on Mean Power (MP)
3.5. The Impact of IPC Intervention with Different Cycling Periods on Time under Tension (TUT)
4. Discussion
4.1. The Impact of Single-Cycle IPC Intervention on Upper Limb Strength Performance
4.2. The Impact of Double-Cycle IPC Intervention on Upper Limb Strength Performance
4.3. The Impact of Triple-Cycle IPC Intervention on Upper Limb Strength Performance
4.4. Research Limitations
4.5. Originality and Contribution
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, Z.; Wu, Y. Ischemic preconditioning enhances athletic performance—Methods, applications, and mechanisms. Chin. J. Tissue Eng. Res. 2023, 27, 7. [Google Scholar]
- Gao, X.; Wang, A.; Fan, J.; Zhang, T.; Li, C.; Yue, T.; Hurr, C. The effect of ischemic preconditioning on repeated sprint cycling performance: A randomized crossover study. J. Sports Med. Phys. Fit. 2024; ahead of print. [Google Scholar]
- Macdougall, K.B.; Mcclean, Z.J.; Macintosh, B.R.; Fletcher, J.R.; Aboodarda, S.J. Ischemic Preconditioning, but not Priming Exercise, Improves Exercise Performance in Trained Rock Climbers. J. Strength Cond. Res. 2023, 37, 2149–2157. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Yang, H.; Chen, F.; Li, B.; Meng, X. RNA sequencing reveals the potential mechanism of exercise preconditioning for cerebral ischemia reperfusion injury in rats. Brain Behav. 2024, 14, e3608. [Google Scholar] [CrossRef]
- Fan, Z.; Shi, L.; Wu, Y. The application effect and mechanism of remote ischemic preconditioning in enhancing sports performance. China Sport Sci. Technol. 2023, 59, 13. [Google Scholar]
- Dao, A.T.; Zagaar, M.A.; Levine, A.T.; Alkadhi, K.A. Comparison of the Effect of Exercise on Late-Phase LTP of the Dentate Gyrus and CA1 of Alzheimer’s Disease Model. Mol. Neurobiol. 2016, 53, 6859–6868. [Google Scholar] [CrossRef]
- De Oliveira, G.T.; Souza HL, R.; Prazeres, E.O.; Bernardes, B.P.; Patterson, S.D.; Arriel, R.A.; Camilo, G.B.; Hohl, R.; Meireles, A.; Marocolo, M. A Practical Approach for Ischemic Preconditioning Intervention in Sports: A Pilot Study for Cuff Thigh Occlusion Pressure Estimation Based on Systolic Blood Pressure. J. Hum. Kinet. 2024, 91, 157–164. [Google Scholar] [CrossRef] [PubMed]
- French, C.; Robbins, D.; Gernigon, M.; Gordon, D. The effects of lower limb ischaemic preconditioning: A systematic review. Front. Physiol. 2023, 14, 1323310. [Google Scholar] [CrossRef]
- Kataoka, R.; Song, J.S.; Yamada, Y.; Hammert, W.B.; Seffrin, A.; Spitz, R.W.; Wong, V.; Kang, A.; Loenneke, J.P. The Impact of Different Ischemic Preconditioning Pressures on Pain Sensitivity and Resistance Exercise Performance. J. Strength Cond. Res. 2024, 38, 864–872. [Google Scholar] [CrossRef]
- Montoye, A.H.K.; Neph, S.E.; Plouffe, A.A.; Vondrasek, J.D.; Nordbeck, J.T.; Cox, B.A.; Vranish, J.R. Understanding lower limb blood flow occlusion parameters for use in field-based settings. J. Sports Sci. 2023, 41, 850–858. [Google Scholar] [CrossRef]
- Mohammadkhani, R.; Ranjbar, K.; Salehi, I.; Komaki, A.; Zarrinkalam, E.; Amiri, P. Comparison of the preconditioning effect of different exercise training modalities on myocardial ischemia-reperfusion injury. PLoS ONE 2023, 18, e0295169. [Google Scholar] [CrossRef]
- Barbosa, T.C.; Machado, A.C.; Braz, I.D.; Fernandes, I.A.; Vianna, L.C.; Nobrega, A.C.L.; Silva, B.M. Remote ischemic preconditioning delays fatigue development during handgrip exercise. Scand. J. Med. Sci. Sports 2015, 25, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Patterson, S.D.; Bezodis, N.E.; Glaister, M.; Pattison, J.R. The Effect of Ischemic Preconditioning on Repeated Sprint Cycling Performance. Med. Sci. Sports Exerc. 2015, 47, 1652–1658. [Google Scholar] [CrossRef] [PubMed]
- Kraus, A.S.; Pasha, E.P.; Machin, D.R.; Alkatan, M.; Kloner, R.A.; Tanaka, H. Bilateral Upper Limb Remote Ischemic Preconditioning Improves Anaerobic Power. Open Sports Med. J. 2015, 9, 889. [Google Scholar] [CrossRef]
- Salagas, A.; Tsoukos, A.; Terzis, G.; Paschalis, V.; Katsikas, C.; Krzysztofik, M.; Wilk, M.; Zajac, A.; Bogdanis, G.C. Effectiveness of either short-duration ischemic pre-conditioning, single-set high-resistance exercise, or their combination in potentiating bench press exercise performance. Front. Physiol. 2022, 13, 1083299. [Google Scholar] [CrossRef]
- Beaven, C.M.; Cook, C.J.; Kilduff, L.; Drawer, S.; Gill, N. Intermittent lower-limb occlusion enhances recovery after strenuous exercise. Appl. Physiol. Nutr. Metab. 2012, 37, 1132–1139. [Google Scholar] [CrossRef]
- Rodrigues, A.L.; Ide, B.N.; Sasaki, J.E.; De Oliveira, D.C.X.; Assumpção, C.D.O.; Marocolo, M.; Mota, G.R. Ischemic Preconditioning Improves the Bench-Press Maximal Strength in Resistance-Trained Men. Int. J. Exerc. Sci. 2023, 16, 217–229. [Google Scholar]
- Wilk, M.; Krzysztofik, M.; Filip, A.; Lockie, R.G.; Zajac, A. The Acute Effects of External Compression With Blood Flow Restriction on Maximal Strength and Strength-Endurance Performance of the Upper Limbs. Front. Physiol. 2020, 11, 567. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela, P.L.; Martín-Candilejo, R.; Sánchez-Martínez, G.; Marins, J.C.B.; de la Villa, P.; Sillero-Quintana, M. Ischemic Preconditioning and Muscle Force Capabilities. J. Strength Cond. Res. 2021, 35, 2187–2192. [Google Scholar] [CrossRef]
- Wilk, M.; Golas, A.; Zmijewski, P.; Krzysztofik, M.; Filip, A.; Del Coso, J.; Tufano, J.J. The Effects of the Movement Tempo on the One-Repetition Maximum Bench Press Results. J. Hum. Kinet. 2020, 72, 151–159. [Google Scholar] [CrossRef]
- Dragutinovic, B.; Jacobs, M.W.; Feuerbacher, J.F.; Goldmann, J.P.; Cheng, S.; Schumann, M. Evaluation of the Vmaxpro sensor for assessing movement velocity and load-velocity variables: Accuracy and implications for practical use. Biol Sport 2024, 41, 41–51. [Google Scholar] [CrossRef]
- Cruz, R.S.; De Aguiar, R.A.; Turnes, T.; Salvador, A.F.; Caputo, F. Effects of ischemic preconditioning on short-duration cycling performance. Appl. Physiol. Nutr. Metab. 2016, 41, 825–831. [Google Scholar] [CrossRef] [PubMed]
- Cruz RS, O.; Pereira, K.L.; De Aguiar, R.A.; Turnes, T.; Denadai, B.S.; Caputo, F. Effects of ischemic conditioning on maximal voluntary plantar flexion contractions. J. Electromyogr. Kinesiol. 2019, 48, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Marocolo, M.; Hohl, R.; Arriel, R.A.; Mota, G.R. Ischemic preconditioning and exercise performance: Are the psychophysiological responses underestimated? Eur. J. Appl. Physiol. 2023, 123, 683–693. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, D.; Suga, T.; Kido, K.; Honjo, T.; Hamaoka, T.; Isaka, T. Acute remote ischemic preconditioning has no effect on quadriceps muscle endurance. Transl. Sports Med. 2020, 3, 314–320. [Google Scholar] [CrossRef]
- Slysz, J.T.; Petrick, H.L.; Marrow, J.P.; Burr, J. An examination of individual responses to ischemic preconditioning and the effect of repeated ischemic preconditioning on cycling performance. Eur. J. Sport Sci. 2020, 20, 633–640. [Google Scholar] [CrossRef]
- De Groot, P.C.; Thijssen, D.H.; Sanchez, M.; Ellenkamp, R.; Hopman, M.T.E. Ischemic preconditioning improves maximal performance in humans. Eur. J. Appl. Physiol. 2010, 108, 141–146. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year (Age) | Height (cm) | Weight (kg) | Training Years | Bench Press 1RM (kg) |
|---|---|---|---|---|
| 20.34 ± 1.70 | 176.30 ± 6.17 | 80.15 ± 7.71 | 4.34 ± 2.11 | 124 ± 18.97 |
| Bench Press Test | Group | Pre-Test (m/s) | Post-Test (m/s) | t-Value | p-Value | Time Effect | Group × Time Interaction | Effect Size (η2) |
|---|---|---|---|---|---|---|---|---|
| First | T1 | 0.476 ± 0.088 | 0.821 ± 0.27 * | −3.708 | p = 0.02 | p < 0.001 | p = 1.667 | 0.442 |
| T2 | 0.772 ± 0.252 * | −3.506 | p = 0.035 | |||||
| T3 | 0.696 ± 0.291 | −2.599 | p = 0.186 | |||||
| CON | 0.51 ± 0.061 # | −0.876 | p = 0.986 | |||||
| Second | T1 | 0.501 ± 0.118 | 0.639 ± 0.186 * | −2.59 | p = 0.024 | p = 0.007 | p = 0.447 | 0.183 |
| T2 | 0.571 ± 0.038 | −1.554 | p = 0.773 | |||||
| T3 | 0.518 ± 0.103 | −1.250 | p = 0.911 | |||||
| CON | 0.509 ± 0.104 | −0.278 | p = 0.994 |
| Bench Press Test | Group | Pre-Test (m/s) | Post-Test (m/s) | t-Value | p-Value | Time Effect | Group × Time Interaction | Effect Size (η2) |
|---|---|---|---|---|---|---|---|---|
| First | T1 | 0.44 ± 0.053 | 0.509 ± 0.018 * | −2.935 | p = 0.045 | p = 0.017 | p = 0.249 | 0.148 |
| T2 | 0.456 ± 0.021 | −0.948 | p = 0.979 | |||||
| T3 | 0.421 ± 0.083 | −0.102 | p = 0.983 | |||||
| CON | 0.458 ± 0.042 | −1.02 | p = 0.968 | |||||
| Second | T1 | 0.42 ± 0.071 | 0.451 ± 0.05 | −0.973 | p = 0.773 | p = 0.723 | p = 0.199 | 0.004 |
| T2 | 0.466 ± 0.71 | 1.61 | p = 0.741 | |||||
| T3 | 0.432 ± 0.23 | 0.901 | p = 0.984 | |||||
| CON | 0.399 ± 0.09 | −0.823 | p = 0.991 |
| Bench Press Test | Group | Pre-Test (m/s) | Post-Test (m/s) | t-Value | p-Value | Time Effect | Group × Time Interaction | Effect Size (η2) |
|---|---|---|---|---|---|---|---|---|
| First | T1 | 401.7 ± 58.91 | 552.71 ± 78.4 ** | −4.584 | p = 0.001 | p = 0.003 | p = 0.011 | 0.22 |
| T2 | 421.3 ± 66.41 | −1.295 | p = 0.895 | |||||
| T3 | 415.67 ± 91.23 | −0.419 | p = 0.973 | |||||
| CON | 403.93 ± 60.71 # | −0.067 | p = 0.981 | |||||
| Second | T1 | 361.3 ± 88.2 | 429.16 ± 183.1 | −1.764 | p = 0.647 | p = 0.133 | p = 0.706 | 0.062 |
| T2 | 391.59 ± 45.8 | −0.652 | p = 0.998 | |||||
| T3 | 354.13 ± 84.8 | −0.24 | p = 0.991 | |||||
| CON | 383.1 ± 99.2 | −0.419 | p = 0.983 |
| Bench Press Test | Group | Pre-Test (m/s) | Post-Test (m/s) | t-Value | p-Value | Time Effect | Group × Time Interaction | Effect Size (η2) |
|---|---|---|---|---|---|---|---|---|
| First | T1 | 309.21 ± 54.39 | 391.61 ± 33.19 ** | −4.271 | p = 0.004 | p = 0.001 | p < 0.001 | 0.409 |
| T2 | 394.92 ± 58.45 ** | −4.025 | p = 0.004 | |||||
| T3 | 307.11 ± 93.21 | −0.382 | p = 0.873 | |||||
| CON | 299.68 ± 66.39 #& | 1.646 | p = 0.683 | |||||
| Second | T1 | 296.01 ± 30.12 | 359.2 ± 39.41 ** | −4.39 | p = 0.003 | p < 0.001 | p = 0.003 | 0.311 |
| T2 | 345.02 ± 61.83 * | −3.279 | p = 0.039 | |||||
| T3 | 309.4 ± 39.16 | −3.511 | p = 0.074 | |||||
| CON | 286.33 ± 42.62 #& | 0.833 | p = 0.991 |
| Bench Press Test | Group | Pre-Test (m/s) | Post-Test (m/s) | t-Value | p-Value | Time Effect | Group × Time Interaction | Effect Size (η2) |
|---|---|---|---|---|---|---|---|---|
| First | T1 | 22.1 ± 4.9 | 32.9 ± 6.51 ** | −4.767 | p < 0.001 | p < 0.001 | p = 0.035 | 0.461 |
| T2 | 29.5 ± 5.93 | −3.105 | p = 0.103 | |||||
| T3 | 28.8 ± 5.59 | −2.799 | p = 0.229 | |||||
| CON | 24.1 ± 7.01 # | −0.437 | p = 0.993 | |||||
| Second | T1 | 17.31 ± 3.88 | 26.4 ± 3.91 ** | −4.482 | p = 0.002 | p = 0.007 | p = 0.447 | 0.424 |
| T2 | 23.1 ± 4.3 | −3.004 | p = 0.135 | |||||
| T3 | 20.8 ± 5.16 | −1.871 | p = 0.966 | |||||
| CON | 18.9 ± 5.17 # | −0.936 | p = 0.972 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niu, X.; Xia, Q.; Xu, J.; Tang, L. Assessment of the Impact of Sensor-Based Ischemic Preconditioning with Different Cycling Periods on Upper Limb Strength in Bodybuilding Athletes. Sensors 2024, 24, 5943. https://doi.org/10.3390/s24185943
Niu X, Xia Q, Xu J, Tang L. Assessment of the Impact of Sensor-Based Ischemic Preconditioning with Different Cycling Periods on Upper Limb Strength in Bodybuilding Athletes. Sensors. 2024; 24(18):5943. https://doi.org/10.3390/s24185943
Chicago/Turabian StyleNiu, Xuehan, Qifei Xia, Jie Xu, and Li Tang. 2024. "Assessment of the Impact of Sensor-Based Ischemic Preconditioning with Different Cycling Periods on Upper Limb Strength in Bodybuilding Athletes" Sensors 24, no. 18: 5943. https://doi.org/10.3390/s24185943
APA StyleNiu, X., Xia, Q., Xu, J., & Tang, L. (2024). Assessment of the Impact of Sensor-Based Ischemic Preconditioning with Different Cycling Periods on Upper Limb Strength in Bodybuilding Athletes. Sensors, 24(18), 5943. https://doi.org/10.3390/s24185943