
Comparison of Gait in Women with Degenerative Changes of the Hip Joint and Healthy Women Using the MoKA System—A Pilot Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Methods
2.3. Ethics Approval
2.4. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Katz, J.N.; Arant, K.R.; Loeser, R.F. Diagnosis and Treatment of Hip and Knee Osteoarthritis: A Review. JAMA 2021, 325, 568–578. [Google Scholar] [CrossRef] [PubMed]
- Loeser, R.F.; Goldring, S.R.; Scanzello, C.R.; Goldring, M.B. Osteoarthritis: A disease of the joint as an organ. Arthritis Rheum. 2012, 64, 697–707. [Google Scholar] [CrossRef] [PubMed]
- Kraus, V.B.; Blanco, F.J.; Englund, M.; Karsdal, M.A.; Lohmander, L.S. Call for standardized definitions of osteoarthritis and risk stratification for clinical trials and clinical use. Osteoarthr. Cartil. 2015, 23, 1233–1241. [Google Scholar] [CrossRef] [PubMed]
- Bombardier, C. L’impact de L’arthrite au Canada: Impact of Arthritis in Canada: Today and over the Next 30 Years; Alliance de L’arthrite du Canada: Toronto, ON, Canada, 2016. [Google Scholar]
- Jafarzadeh, S.R.; Felson, D.T. Updated Estimates Suggest a Much Higher Prevalence of Arthritis in United States Adults Than Previous Ones. Arthritis Rheumatol. 2018, 70, 185–192. [Google Scholar] [CrossRef]
- Collins, J.E.; Katz, J.N.; Dervan, E.E.; Losina, E. Trajectories and risk profiles of pain in persons with radiographic, symptomatic knee osteoarthritis: Data from the osteoarthritis initiative. Osteoarthr. Cartil. 2014, 22, 622–630. [Google Scholar] [CrossRef]
- Bastick, A.N.; Runhaar, J.; Belo, J.N.; Bierma-Zeinstra, S.M. Prognostic factors for progression of clinical osteoarthritis of the knee: A systematic review of observational studies. Arthritis Res. Ther. 2015, 17, 152. [Google Scholar] [CrossRef]
- Ataullah, A.H.M.; De Jesus, O. Gait Disturbances. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar] [PubMed]
- Pirker, W.; Katzenschlager, R. Gait disorders in adults and the elderly: A clinical guide. Wien. Klin. Wochenschr. 2017, 129, 81–95. [Google Scholar] [CrossRef]
- Beckwée, D.; Degelaen, M.; Eggermont, M.; Gonzalez-Rodriguez, M.; Lefeber, N.; Vaes, P.; Bautmans, I.; Swinnen, E. Validity and test-retest reliability of the Stride Analyzer in people with knee osteoarthritis. Gait Posture 2016, 49, 155–158. [Google Scholar] [CrossRef]
- Kobsar, D.; Masood, Z.; Khan, H.; Khalil, N.; Kiwan, M.Y.; Ridd, S.; Tobis, M. Wearable Inertial Sensors for Gait Analysis in Adults with Osteoarthritis-A Scoping Review. Sensors 2020, 20, 7143. [Google Scholar] [CrossRef]
- Simon, S.R. Quantification of human motion: Gait analysis-benefits and limitations to its application to clinical problems. J. Biomech. 2004, 37, 1869–1880. [Google Scholar] [CrossRef]
- Morris, J.R. Accelerometry--a technique for the measurement of human body movements. J. Biomech. 1973, 6, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Godfrey, A.; Conway, R.; Meagher, D.; OLaighin, G. Direct measurement of human movement by accelerometry. Med. Eng. Phys. 2008, 30, 1364–1386. [Google Scholar] [CrossRef] [PubMed]
- Mathie, M.J.; Coster, A.C.; Lovell, N.H.; Celler, B.G. Accelerometry: Providing an integrated, practical method for long-term, ambulatory monitoring of human movement. Physiol. Meas. 2004, 25, R1. [Google Scholar] [CrossRef] [PubMed]
- Karantonis, D.M.; Narayanan, M.R.; Mathie, M.; Lovell, N.H.; Celler, B.G. Implementation of a real-time human movement classifier using a triaxial accelerometer for ambulatory monitoring. IEEE Trans. Inf. Technol. Biomed. 2006, 10, 156–167. [Google Scholar] [CrossRef]
- Willemsen, A.T.; van Alsté, J.A.; Boom, H.B. Real-time gait assessment utilizing a new way of accelerometry. J. Biomech. 1990, 23, 859–863. [Google Scholar] [CrossRef]
- Willemsen, A.T.; Frigo, C.; Boom, H.B. Lower extremity angle measurement with accelerometers--error and sensitivity analysis. IEEE Trans. Biomed. Eng. 1991, 38, 1186–1193. [Google Scholar] [CrossRef]
- Shimada, Y.; Ando, S.; Matsunaga, T.; Misawa, A.; Aizawa, T.; Shirahata, T.; Itoi, E. Clinical application of acceleration sensor to detect the swing phase of stroke gait in functional electrical stimulation. Tohoku J. Exp. Med. 2005, 207, 197–202. [Google Scholar] [CrossRef]
- Pincivero, D.M.; Gandhi, V.; Timmons, M.K.; Coelho, A.J. Quadriceps femoris electromyogram during concentric, isometric and eccentric phases of fatiguing dynamic knee extensions. J. Biomech. 2006, 39, 246–254. [Google Scholar] [CrossRef]
- Schmitt, S.; Melnyk, M.; Alt, W.; Gollhofer, A. Novel approach for a precise determination of short-time intervals in ankle sprain experiments. J. Biomech. 2009, 42, 2823–2825. [Google Scholar] [CrossRef]
- Coley, B.; Najafi, B.; Paraschiv-Ionescu, A.; Aminian, K. Stair climbing detection during daily physical activity using a miniature gyroscope. Gait Posture 2005, 22, 287–294. [Google Scholar] [CrossRef]
- Lorussi, F.; Rocchia, W.; Scilingo, E.P.; Tognetti, A.; De Rossi, D. Wearable, redundant fabric-based sensor arrays for reconstruction of body segment posture. IEEE Sens. J. 2004, 4, 807–818. [Google Scholar] [CrossRef]
- Tao, W.; Liu, T.; Zheng, R.; Feng, H. Gait analysis using wearable sensors. Sensors 2012, 12, 2255–2283. [Google Scholar] [CrossRef] [PubMed]
- Shull, P.B.; Jirattigalachote, W.; Hunt, M.A.; Cutkosky, M.R.; Delp, S.L. Quantified self and human movement: A review on the clinical impact of wearable sensing and feedback for gait analysis and intervention. Gait Posture 2014, 40, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Apollo Guidance and Navigation Considerations of Apollo IMU Gimbal Lock MIT Instrumentation Laboratory Document E-1344; David Hoag; April 1963. Available online: https://www.nasa.gov/history/alsj/e-1344.htm (accessed on 20 August 2024).
- Zhou, L.; Tunca, C.; Fischer, E.; Brahms, C.M.; Ersoy, C.; Granacher, U.; Arnrich, B. Validation of an IMU Gait Analysis Algorithm for Gait Monitoring in Daily Life Situations. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2020, 2020, 4229–4232. [Google Scholar] [CrossRef]
- Nierwińska, K.; Myśliwiec, A.; Konarska-Rawluk, A.; Lipowicz, A.; Małecki, A.; Knapik, A. SMART System in the Assessment of Exercise Tolerance in Adults. Sensors 2023, 23, 9624. [Google Scholar] [CrossRef]
- Agarwala, P.; Salzman, S.H. Six-Minute Walk Test: Clinical Role, Technique, Coding, and Reimbursement. Chest 2020, 157, 603–611. [Google Scholar] [CrossRef]
- Kobsar, D.; Charlton, J.M.; Tse, C.T.F.; Esculier, J.F.; Graffos, A.; Krowchuk, N.M.; Thatche, D.; Hunt, M.A. Validity and reliability of wearable inertial sensors in healthy adult walking: A systematic review and meta-analysis. J. Neuroeng. Rehabil. 2020, 17, 62. [Google Scholar] [CrossRef]
- Kushwaha, N.S.; Kumar, A.; Shukla, R.; Kumar, D.; Yadav, G.; Sharma, V.; Abbas, M.Z.; Parihar, K. Functional Outcomes and Gait Analysis of Total Hip Arthroplasty Through Lateral Hardinge Approach and Gluteus Medius-Sparing Approach: A Prospective Study. Cureus 2024, 16, e54323. [Google Scholar] [CrossRef]
- Kim, B.I.; Wixted, C.M.; Wu, C.J.; Hinton, Z.W.; Jiranek, W.A. Inertial Sensor Gait Analysis of Trendelenburg Gait in Patients Who Have Hip Osteoarthritis. J. Arthroplast. 2024, 39, 1741–1746. [Google Scholar] [CrossRef]
- Sato, H.; Kijima, H.; Iwami, T.; Tsukamoto, H.; Saito, H.; Kudo, D.; Kimura, R.; Kasukawa, Y.; Miyakoshi, N. Unicompartmental Knee Arthroplasty for Osteoarthritis Eliminates Lateral Thrust: Associations between Lateral Thrust Detected by Inertial Measurement Units and Clinical Outcomes. Sensors 2024, 24, 2019. [Google Scholar] [CrossRef]
- Kuś, M.; Myśliwiec, A.; Knapik, A. Gait analysis after hip arthroplasty using the moka system—Case study. In Rehabilitation and Physioterapy after COVID-19; Beno, P., Knapik, A., Rottermund, J., Sramka, M., Eds.; Medical University of Silesia: Katowice, Poland, 2023; pp. 87–96. [Google Scholar]
- Millor, N.; Lecumberri, P.; Gómez, M.; Martínez-Ramírez, A.; Izquierdo, M. An evaluation of the 30-s chair stand test in older adults: Frailty detection based on kinematic parameters from a single inertial unit. J. Neuroeng. Rehabil. 2013, 10, 86. [Google Scholar] [CrossRef] [PubMed]
- Baker, R.; Esquenazi, A.; Benedetti, M.G.; Desloovere, K. Gait analysis: Clinical facts. Eur. J. Phys. Rehabil. Med. 2016, 52, 560–574. [Google Scholar] [PubMed]
- Demir, Y.P.; Yildirim, S.A. Different walk aids on gait parameters and kinematic analysis of the pelvis in patients with Adult Neuromuscular Disease. Neurosciences 2019, 24, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Aanestad, M.; Grisot, M.; Hanseth, O.; Vassilakopoulou, P. Information Infrastructures for eHealth. In Information Infrastructures within European Health Care: Working with the Installed Base [Internet]; Aanestad, M., Grisot, M., Hanseth, O., Vassilakopoulou, P., Eds.; Springer: Cham, Switzerland, 2017. [Google Scholar] [PubMed]
- Klöpfer-Krämer, I.; Brand, A.; Wackerle, H.; Müßig, J.; Kröger, I.; Augat, P. Gait analysis—Available platforms for outcome assessment. Injury 2020, 51 (Suppl. S2), 90–96. [Google Scholar] [CrossRef]
- Chang, W.Y.; Choi, S.; Yoo, S.J.; Lee, J.; Lim, C. Factors Associated with Osteoarthritis and Their Influence on Health-Related Quality of Life in Older Adults with Osteoarthritis: A Study Based on the 2020 Korea National Health and Nutrition Examination Survey. Int. J. Environ. Res. Public Health 2023, 20, 6073. [Google Scholar] [CrossRef]
- Eaton, C.B. Obesity as a risk factor for osteoarthritis: Mechanical versus metabolic. Rhode Isl. Med. J. 2004, 87, 201. [Google Scholar]
- Felson, D.T. Obesity and vocational and avocational overload of the joint as risk factors for osteoarthritis. J. Rheumatol. Suppl. 2004, 70, 2–5. [Google Scholar]
- Alberti, K.G.M.M.; Zimmet, P.Z. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet. Med. 1998, 15, 539–553. [Google Scholar] [CrossRef]
- Jin, X.; Beguerie, J.R.; Zhang, W.; Blizzard, L.; Otahal, P.; Jones, G.; Ding, C. Circulating C reactive protein in osteoarthritis: A systematic review and meta-analysis. Ann. Rheum. Dis. 2015, 74, 703–710. [Google Scholar] [CrossRef]
- Stannus, O.P.; Jones, G.; Blizzard, L.; Cicuttini, F.M.; Ding, C. Associations between serum levels of inflammatory markers and change in knee pain over 5 years in older adults: A prospective cohort study. Ann. Rheum. Dis. 2013, 72, 535–540. [Google Scholar] [CrossRef]
- Kluzek, S.; Newton, J.; Arden, N. Is osteoarthritis a metabolic disorder? Br. Med. Bull. 2015, 115, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Xie, D.-X.; Wei, J.; Zeng, C.; Yang, T.; Li, H.; Wang, Y.-L.; Long, H.-Z.; Wu, Z.-Y.; Qian, Y.-X.; Li, K.-H. Association between metabolic syndrome and knee osteoarthritis: A cross-sectional study. BMC Musculoskelet. Disord. 2017, 18, 533. [Google Scholar] [CrossRef] [PubMed]
- Farnaghi, S.; Crawford, R.; Xiao, Y.; Prasadam, I. Cholesterol metabolism in pathogenesis of osteoarthritis disease. Int. J. Rheum. Dis. 2017, 20, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Ibara, T.; Anan, M.; Karashima, R.; Hada, K.; Shinkoda, K.; Kawashima, M.; Takahashi, M. Coordination Pattern of the Thigh, Pelvic, and Lumbar Movements during the Gait of Patients with Hip Osteoarthritis. J. Healthc. Eng. 2020, 2020, 9545825. [Google Scholar] [CrossRef]
- Boekesteijn, R.J.; Smolders, J.M.H.; Busch, V.J.J.F.; Geurts, A.C.H.; Smulders, K. Independent and sensitive gait parameters for objective evaluation in knee and hip osteoarthritis using wearable sensors. BMC Musculoskelet. Disord. 2021, 22, 242. [Google Scholar] [CrossRef]
- Wada, O.; Tateuchi, H.; Ichihashi, N. The correlation between movement of the center of mass and the kinematics of the spine, pelvis, and hip joints during body rotation. Gait Posture 2014, 39, 60–64. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Parameter | Group | Mean | Min–Max | p | R-Distance |
|---|---|---|---|---|---|
| Age [years] | SGL | 71.33 | 69–73 | −0.35 | |
| SGR | 65.83 | 60–78 | −0.30 | ||
| CG | 67.60 | 60–79 | −0.35 | ||
| Height [cm] | SGL | 71.33 | 164–166 | ||
| SGR | 163 | 152–174 | |||
| CG | 160 | 148–177 | |||
| Weight [kg] | SGL | 86 | 84.0–88.0 | ||
| SGR | 81.50 | 67.0–96.0 | |||
| CG | 69.26 | 57.4–88.9 | |||
| BMI | SGL | 31.98 | 30.2–32.2 | −0.31 | |
| SGR | 30.79 | 24.6–36.8 | |||
| CG | 27.46 | 22.1–35.6 | −0.39 | ||
| 6MWT distance [m] | SGL | 284.50 | 227–374 | SGR-CG: <0.05 SGL-CG: <0.01 | |
| SGR | 269.10 | 210–367 | |||
| CG | 469.50 | 400–576 |
| Group | Time | Pelvis | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Sagittal Plane | Frontal Plane | Transverse Plane | ||||||||
| Min–Max | Change: Max–Min | Min–Max | Change: Max–Min | Min–Max | Change: Max–Min | |||||
| ° | % | ° | % | ° | % | |||||
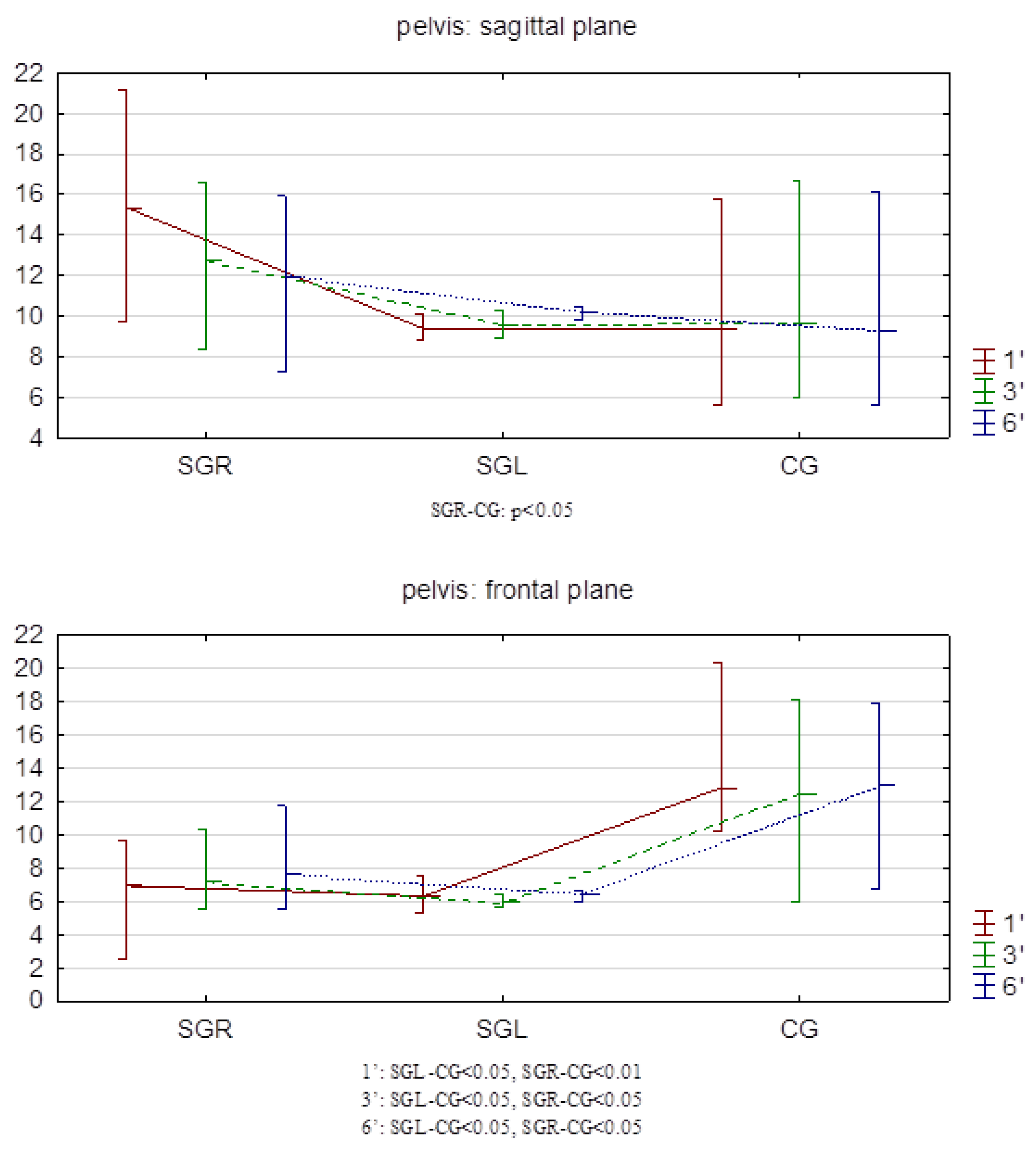
| I. SGR | 1′ | 20.1–29.5 | 9.4 | −3.8–2.6 | 6.3 | −11.0–10.0 | 21.0 | |||
| 3′ | 20.0–29.6 | 9.6 | 2.1 | −3.7–2.3 | 6.0 | 4.7 | −12.9–11.1 | 24.0 | 1.5 | |
| 6′ | 19.9–30.1 | 10.2 | 8.5 | −4.1–2.4 | 6.4 | 1.6 | −13.0–13.1 | 26.1 | 2.5 | |
| average | 9.7 | 5.5 | 6.2 | 3.2 | 23.7 | 2.0 | ||||
| II. SGL | 1′ | 22.5–37.9 | 15.4 | −3.9–3.0 | 6.9 | −11.5–11.9 | 23.4 | |||
| 3′ | 21.5–34.3 | 12.8 | 1.7 | −3.9–3.3 | 7.2 | 4.3 | −14.6–14.1 | 28.7 | 22.6 | |
| 6′ | 21.8–33.8 | 12.0 | 2.2 | −4.6–3.0 | 7.6 | 10.1 | −9.9–12.7 | 22.6 | 3.4 | |
| average | 13.4 | 2.0 | 7.2 | 7.2 | 24.9 | 9.6 | ||||
| III. CG | 1′ | 19.1–28.5 | 9.3 | −6.4–6.5 | 12.8 | −11.3–11.4 | 22.7 | |||
| 3′ | 19.2–28.8 | 9.6 | 3.2 | −3.3–9.1 | 12.5 | 2.3 | −10.8–12.5 | 23.3 | 2.6 | |
| 6′ | 19.2–28.5 | 9.3 | 0 | −3.7–9.3 | 13.0 | 1.6 | −12.5–11.5 | 24.0 | 5.7 | |
| average | 9.4 | 1.6 | 12.8 | 2.0 | 23.3 | 4.2 | ||||
| Group | Time | Left Lower Limb | |||||
|---|---|---|---|---|---|---|---|
| Frontal Plane | Transverse Plane | ||||||
| Min–Max | Change: Max–Min | Min–Max | Change: Max–Min | ||||
| o | % | o | % | ||||
| I. SGR | 1′ | −6.9–8.3 | 15.2 | −35.4–12.2 | 47.6 | ||
| 3′ | −6.0–8.6 | 15.6 | 2.3 | −19.9–25.8 | 45.7 | 3.9 | |
| 6′ | −6.1–9.2 | 15.3 | 0.7 | −6.3–8.8 | 15.1 | 68.2 | |
| average | 15.4 | 1.5 | 36.1 | 36.1 | |||
| II. SGL | 1′ | −12.4–9.6 | 22.0 | −14.4–13.4 | 27.8 | ||
| 3′ | −13.3–10.1 | 23.4 | 6.4 | −12.2–22.0 | 34.2 | 23.0 | |
| 6′ | −13.8–10.4 | 24.4 | 10.9 | −22.6–5.7 | 28.3 | 1.8 | |
| average | 23.3 | 8.7 | 30.1 | 12.4 | |||
| III. CG | 1′ | −8.4–10.3 | 18.7 | −15.9–16.3 | 32.2 | ||
| 3′ | −8.5–12.0 | 20.5 | 9.6 | −22.6–11.6 | 34.2 | 6.2 | |
| 6′ | −9.0–12.0 | 21.0 | 12.3 | −30.9–5.8 | 36.7 | 14.0 | |
| average | 20.1 | 11.0 | 34.4 | 10.1 | |||
| Right lower limb | |||||||
| I. SGR | 1′ | −8.8–7.2 | 16.0 | −13.7–16.8 | 30.5 | ||
| 3′ | −10.9–6.3 | 17.2 | 7.5 | −23.4–8.8 | 32.2 | 5.6 | |
| 6′ | −10.5–6.2 | 16.7 | 4.4 | −45.1–−12.0 | 33.1 | 8.5 | |
| average | 16.6 | 6.0 | 31.9 | 7.1 | |||
| II. SGL | 1′ | −7.4–7.2 | 14.6 | −12.5–17.9 | 30.4 | ||
| 3′ | −7.1–7.3 | 14.4 | 1.4 | −11.4–24.2 | 35.6 | 17.1 | |
| 6′ | −6.9–6.5 | 13.4 | 8.2 | −0.4–30.7 | 31.1 | 2.3 | |
| average | 14.1 | 4.8 | 32.4 | 9.7 | |||
| III. CG | 1′ | −9.5–11.0 | 20.5 | −12.8–18.5 | 31.3 | ||
| 3′ | −9.1–11.2 | 20.4 | 0.5 | −15.1–21.7 | 36.8 | 17.6 | |
| 6′ | −8.9–12.7 | 21.6 | 5.4 | −12.8–25.1 | 37.9 | 21.1 | |
| average | 20.8 | 3.0 | 35.3 | 19.4 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuś, M.; Wasiuk-Zowada, D.; Henke, M.; Szefler-Derela, J.; Knapik, A. Comparison of Gait in Women with Degenerative Changes of the Hip Joint and Healthy Women Using the MoKA System—A Pilot Study. Sensors 2024, 24, 6417. https://doi.org/10.3390/s24196417
Kuś M, Wasiuk-Zowada D, Henke M, Szefler-Derela J, Knapik A. Comparison of Gait in Women with Degenerative Changes of the Hip Joint and Healthy Women Using the MoKA System—A Pilot Study. Sensors. 2024; 24(19):6417. https://doi.org/10.3390/s24196417
Chicago/Turabian StyleKuś, Maciej, Dagmara Wasiuk-Zowada, Magdalena Henke, Justyna Szefler-Derela, and Andrzej Knapik. 2024. "Comparison of Gait in Women with Degenerative Changes of the Hip Joint and Healthy Women Using the MoKA System—A Pilot Study" Sensors 24, no. 19: 6417. https://doi.org/10.3390/s24196417