
MSK-TIM: A Telerobotic Ultrasound System for Assessing the Musculoskeletal System

 ,
,  , and
, and 
Abstract
1. Introduction
2. Methodology
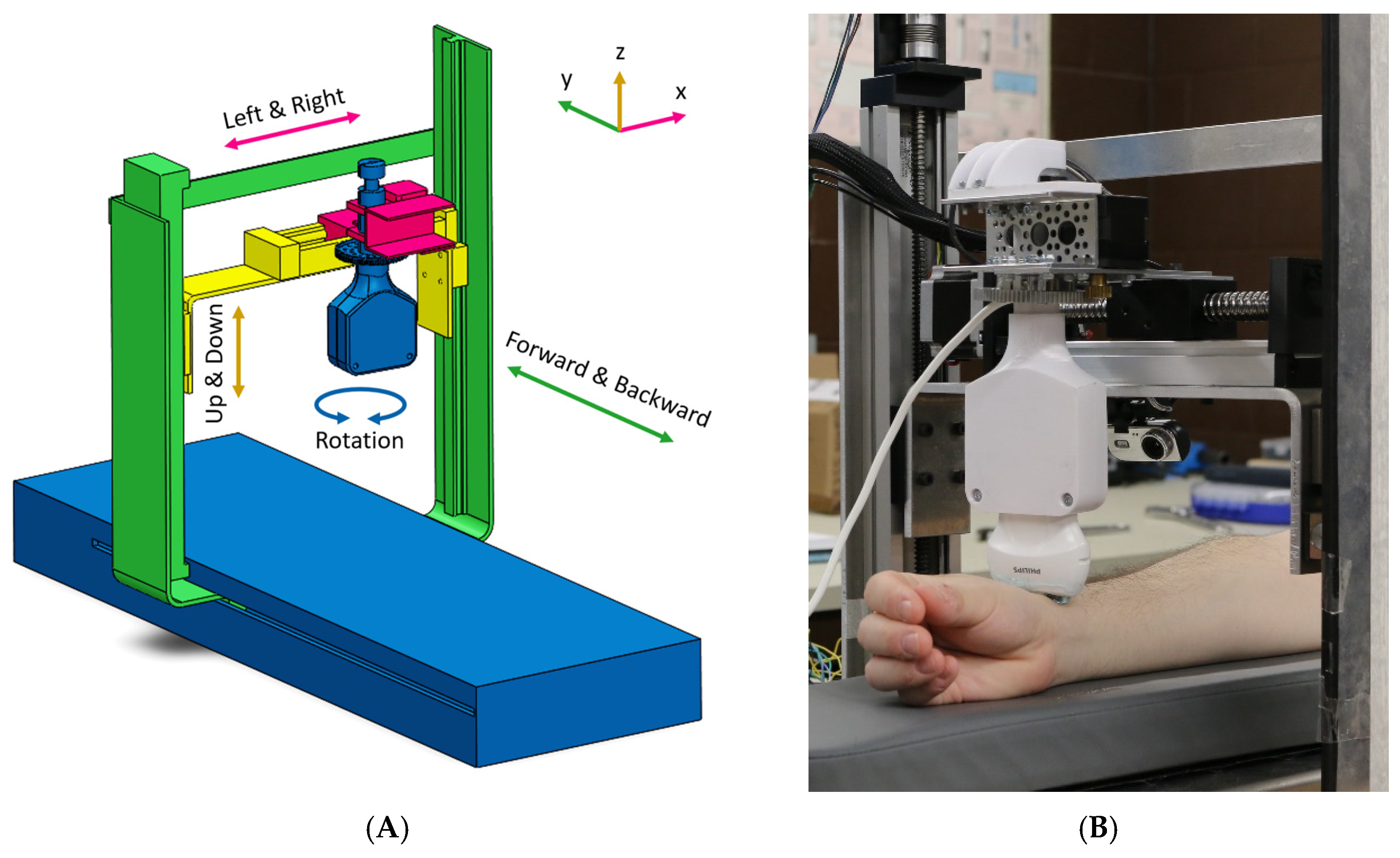
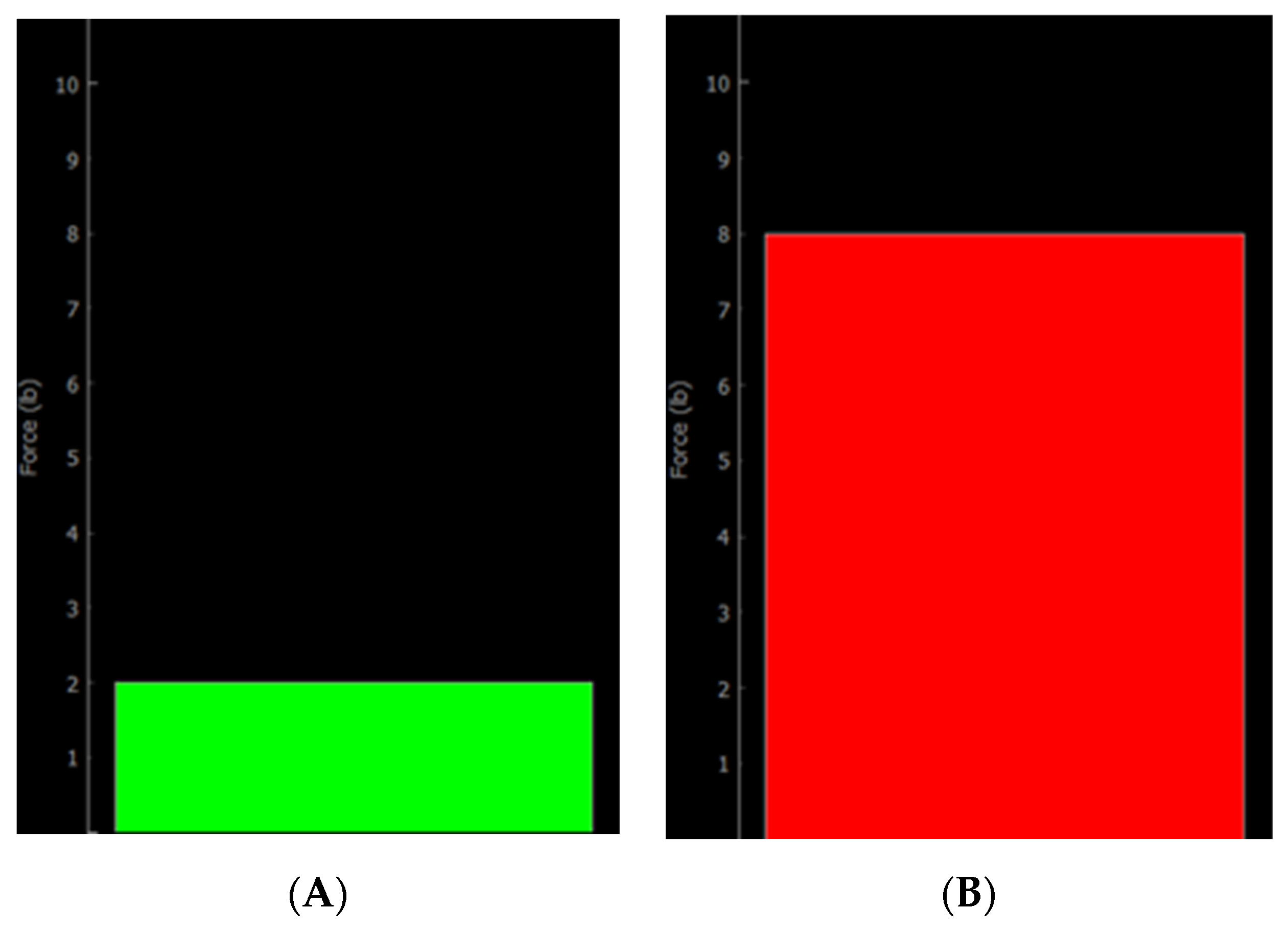
2.1. MSK-TIM System
2.2. Clinical Assessment
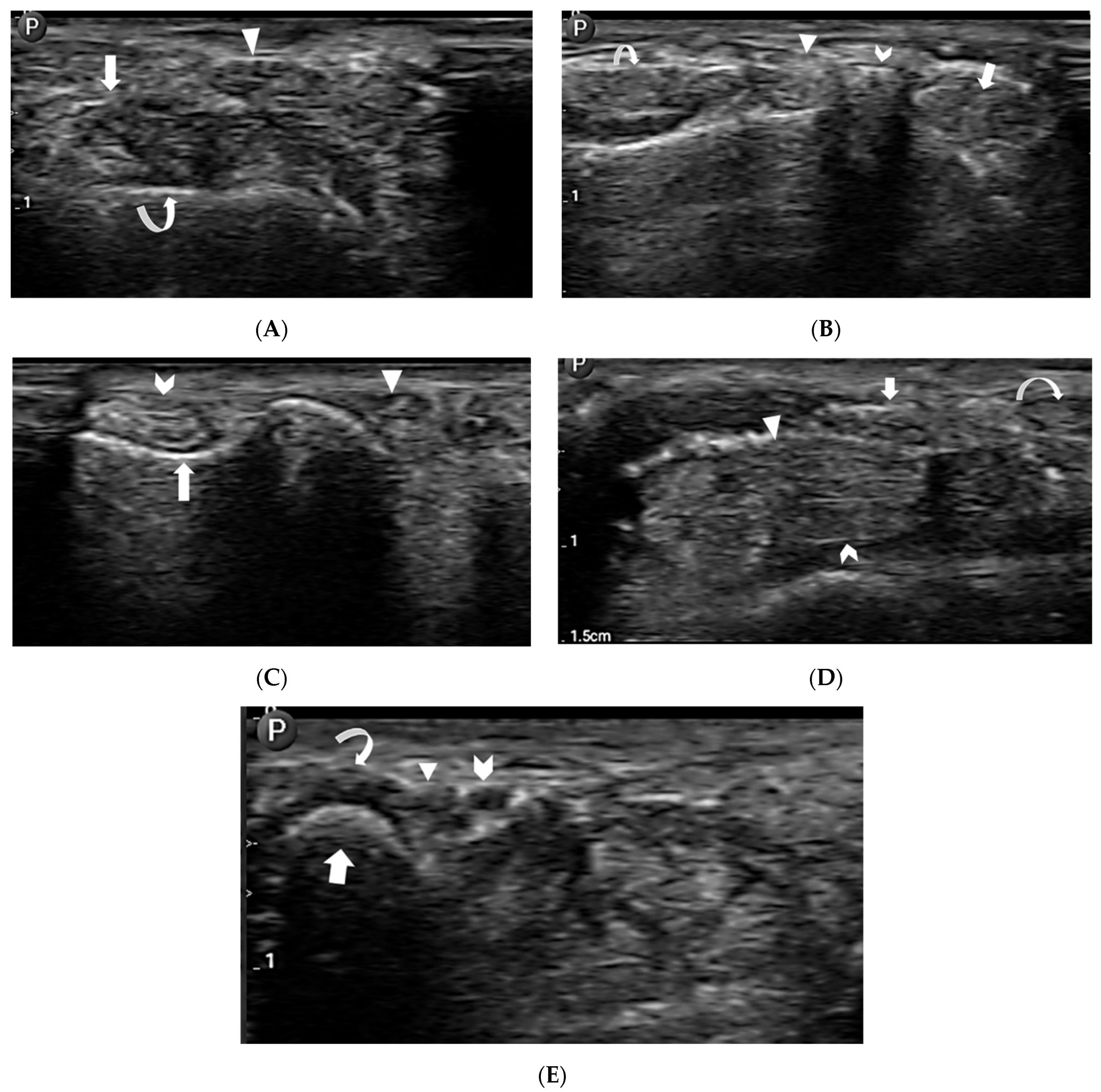
2.3. Anatomic Visualization
- Extensor tendon compartments:
- First extensor compartment—extensor pollicis brevis and abductor pollicis longus tendons (Figure 5A).
- Second extensor compartment—extensor carpi radialis longus and brevis tendons (Figure 5B).
- Third extensor compartment—extensor pollicis longus tendon (Figure 5A,B).
- Fourth extensor compartment—extensor digitorum longus tendons (Figure 5B).
- Fifth extensor compartment—extensor digiti minimi tendon (Figure 5C).
- Sixth extensor compartment—extensor carpi ulnaris tendon (Figure 5C).
- Flexor tendons:
- Median nerve (Figure 5D).
- Guyon’s canal contents:
- Bony anatomy:
3. Results
3.1. Anatomic Visualization
3.2. Radiologist’s Experience
3.3. Participants’ Experience
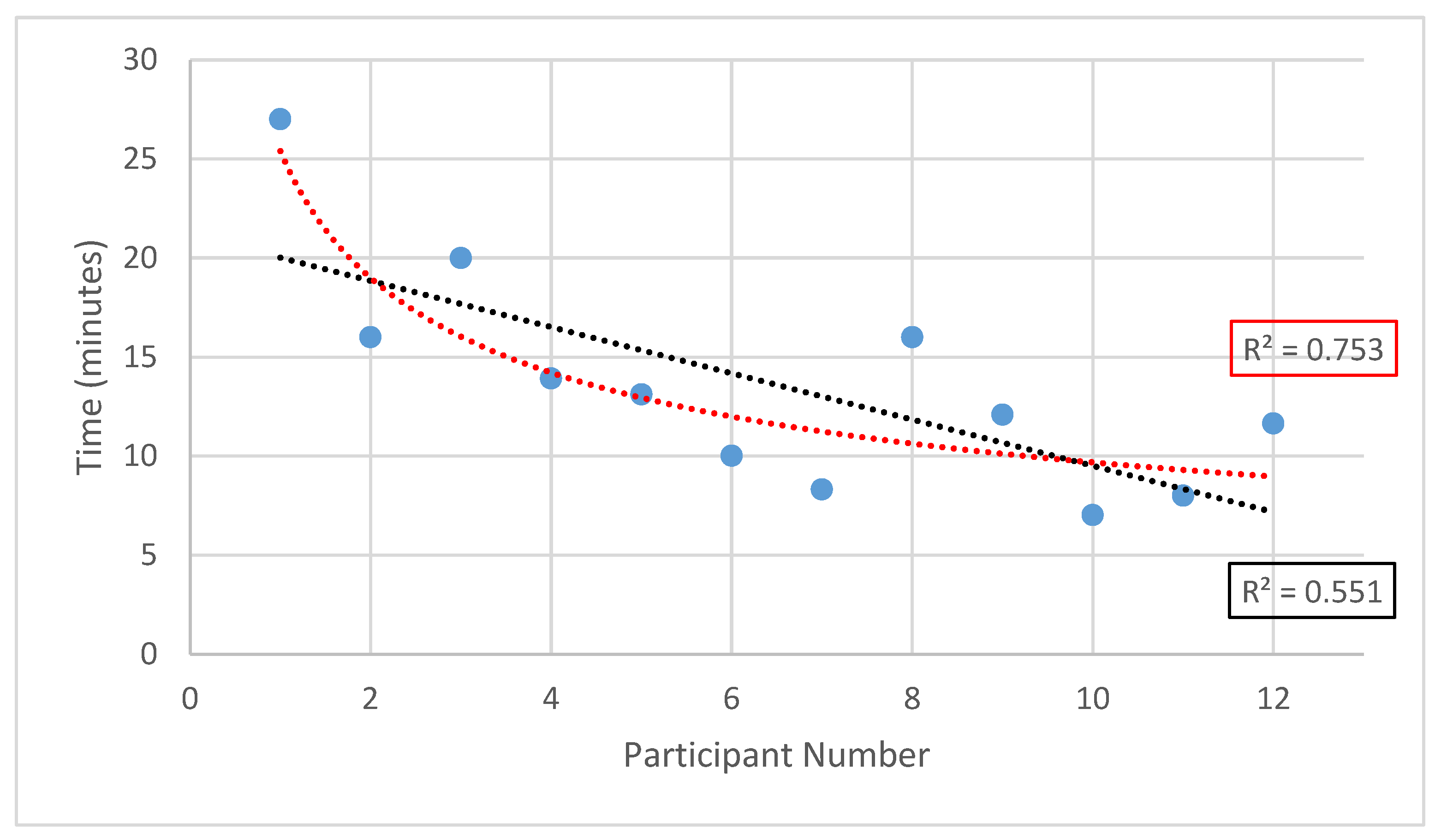
3.4. Delay and Time Measurement
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gyles, C. Robots in Medicine. Can. Vet. J. 2019, 60, 819–820. [Google Scholar]
- Gilbertson, M.W.; Anthony, B.W. An Ergonomic, Instrumented Ultrasound Probe for 6-Axis Force/Torque Measurement. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 140–143. [Google Scholar]
- Adams, S.J.; Penz, E.; Imeah, B.; Burbridge, B.; Obaid, H.; Babyn, P.; Mendez, I. Economic Evaluation of Telerobotic Ultra-sound Technology to Remotely Provide Ultrasound Services in Rural and Remote Communities. J. Ultrasound Med. 2022, 42, 109–123. [Google Scholar] [CrossRef]
- Obaid, M.; Zhang, Q.; Adams, S.J.; Fotouhi, R.; Obaid, H. Development and Assessment of a Telesonography System for Musculoskeletal Imaging. Eur. Radiol. Exp. 2021, 5, 29. [Google Scholar] [CrossRef]
- Rural Population (% of Total Population)|Data. Available online: https://data.worldbank.org/indicator/SP.RUR.TOTL.ZS (accessed on 24 January 2023).
- Marsh-Feiley, G.; Eadie, L.; Wilson, P. Telesonography in Emergency Medicine: A Systematic Review. PLoS ONE 2018, 13, e0194840. [Google Scholar] [CrossRef]
- Adams, S.; Burbridge, B.; Obaid, H.; Stoneham, G.; Babyn, P.; Mendez, I. Telerobotic Sonography for Remote Diagnostic Imaging: Narrative Review of Current Developments and Clinical Applications. J. Ultrasound Med. 2021, 40, 1287–1306. [Google Scholar] [CrossRef]
- Wang, S.; Housden, J.; Noh, Y.; Singh, D.; Singh, A.; Skelton, E.; Matthew, J.; Tan, C.; Back, J.; Lindenroth, L.; et al. Robotic-Assisted Ultrasound for Fetal Imaging: Evolution from Single-Arm to Dual-Arm System. In Proceedings of the Annual Conference Towards Autonomous Robotic Systems, London, UK, 17 July 2019; Springer: Cham, Switzerland, 2019; pp. 27–38. [Google Scholar]
- Giuliani, M.; Szczęśniak-Stańczyk, D.; Mirnig, N.; Stollnberger, G.; Szyszko, M.; Stańczyk, B.; Tscheligi, M. User-Centred Design and Evaluation of a Tele-Operated Echocardiography Robot. Health Technol. 2020, 10, 649–665. [Google Scholar] [CrossRef]
- Nouaille, L.; Vieyres, P.; Poisson, G. Process of Optimisation for a 4 DOF Tele-Echography Robot. Robotica 2012, 30, 1131–1145. [Google Scholar] [CrossRef]
- Swerdlow, D.; Cleary, K.; Wilson, E.; Azizi-Koutenaei, B.; Monfaredi, R. Robotic Arm–Assisted Sonography: Review of Technical Developments and Potential Clinical Applications. Am. J. Roentgenol. 2017, 208, 733–738. [Google Scholar] [CrossRef]
- Dhyani, M.; Roll, S.C.; Gilbertson, M.W.; Orlowski, M.; Anvari, A.; Li, Q.; Anthony, B.; Samir, A.E. A Pilot Study to Precisely Quantify Forces Applied by Sonographers While Scanning: A Step toward Reducing Ergonomic Injury. Work Read. Mass 2017, 58, 241–247. [Google Scholar] [CrossRef]
- Raina, D.; Singh, H.; Saha, S.K.; Arora, C.; Agarwal, A.; SH, C.; Rangarajan, K.; Nandi, S. Comprehensive Telerobotic Ultrasound System for Abdominal Imaging: Development and in-Vivo Feasibility Study. In Proceedings of the 2021 International Symposium on Medical Robotics (ISMR), Atlanta, GA, USA, 17–19 November 2021; pp. 1–7. [Google Scholar]
- Santos, L.; Cortesão, R.; Quintas, J. Twin Kinematics Approach for Robotic-Assisted Tele-Echography. In Proceedings of the 2019 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), Macau, China, 3–8 November 2019; pp. 1339–1346. [Google Scholar]
- Wagner, C.R.; Stylopoulos, N.; Jackson, P.G.; Howe, R.D. The Benefit of Force Feedback in Surgery: Examination of Blunt Dissection. Presence Teleoperators Virtual Environ. 2007, 16, 252–262. [Google Scholar] [CrossRef]
- Li, M.; Luo, S.; Nanayakkara, T.; Seneviratne, L.D.; Dasgupta, P.; Althoefer, K. Multi-Fingered Haptic Palpation Using Pneumatic Feedback Actuators. Sens. Actuators Phys. 2014, 218, 132–141. [Google Scholar] [CrossRef]
- AbbasiMoshaii, A.; Najafi, F. Design, Evaluation and Prototyping of a New Robotic Mechanism for Ultrasound Imaging. J. Comput. Appl. Mech. 2019, 50, 108–117. [Google Scholar] [CrossRef]
- Gilbertson, M.; Anthony, B. Force and Position Control System for Freehand Ultrasound. IEEE Trans. Robot. 2015, 31, 835–849. [Google Scholar] [CrossRef]
- Mathiassen, K.; Fjellin, J.E.; Glette, K.; Hol, P.K.; Elle, O.J. An Ultrasound Robotic System Using the Commercial Robot UR5. Front. Robot. AI 2016, 3, 1. [Google Scholar] [CrossRef]
- Huang, Q.; Lan, J. Remote Control of a Robotic Prosthesis Arm with Six-Degree-of-Freedom for Ultrasonic Scanning and Three-Dimensional Imaging. Biomed. Signal Process. Control 2019, 54, 101606. [Google Scholar] [CrossRef]
- Duan, B.; Xiong, L.; Guan, X.; Fu, Y.; Zhang, Y. Tele-Operated Robotic Ultrasound System for Medical Diagnosis. Biomed. Signal Process. Control 2021, 70, 102900. [Google Scholar] [CrossRef]
- Adambounou, K.; Adjenou, V.; Salam, A.P.; Farin, F.; N’Dakena, K.G.; Gbeassor, M.; Arbeille, P. A Low-Cost Tele-Imaging Platform for Developing Countries. Front. Public Health 2014, 2, 1. [Google Scholar] [CrossRef]
- Ito, K.; Sugano, S.; Takeuchi, R.; Nakamura, K.; Iwata, H. Usability and Performance of a Wearable Tele-Echography Robot for Focused Assessment of Trauma Using Sonography. Med. Eng. Phys. 2013, 35, 165–171. [Google Scholar] [CrossRef]
- Batty, T.; Ehrampoosh, A.; Shirinzadeh, B.; Zhong, Y.; Smith, J. A Transparent Teleoperated Robotic Surgical System with Predictive Haptic Feedback and Force Modelling. Sensors 2022, 22, 9770. [Google Scholar] [CrossRef]
- Slama, T.; Trevisani, A.; Aubry, D.; Oboe, R.; Kratz, F. Experimental Analysis of an Internet-Based Bilateral Teleoperation System with Motion and Force Scaling Using a Model Predictive Controller. IEEE Trans. Ind. Electron. 2008, 55, 3290–3299. [Google Scholar] [CrossRef]
- Noguera Cundar, A. Evaluation of Delay for a Musculoskeletal (MSK) Robotic System for Teleultrasound Tasks. Master’s Thesis, University of Saskatchewan, Saskatoon, SK, Canada, 2021. [Google Scholar]
- Legeza, P.; Britz, G.W.; Shah, A.; Sconzert, K.; Sungur, J.-M.; Chinnadurai, P.; Sinha, K.; Lumsden, A.B. Impact of Network Performance on Remote Robotic-Assisted Endovascular Interventions in Porcine Model. J. Robot. Surg. 2022, 16, 29–35. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Radiologist’s Assessment | |||||
| 1 | 2 | 3 | 4 | 5 | |
| Communication | 0 (0) | 0 (0) | 0 (0) | 4 (33) | 8 (67) |
| Image quality | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 12 (100) |
| Ergonomics | 0 (0) | 0 (0) | 0 (0) | 6 (50) | 6 (50) |
| Convenience | 0 (0) | 0 (0) | 0 (0) | 4 (33) | 8 (67) |
| Participants’ Assessment | |||||
| 1 | 2 | 3 | 4 | 5 | |
| Comfort | 0 (0) | 0 (0) | 3 (25) | 5 (42) | 4 (33) |
| Communication | 0 (0) | 1 (8) | 0 (0) | 3 (25) | 8 (67) |
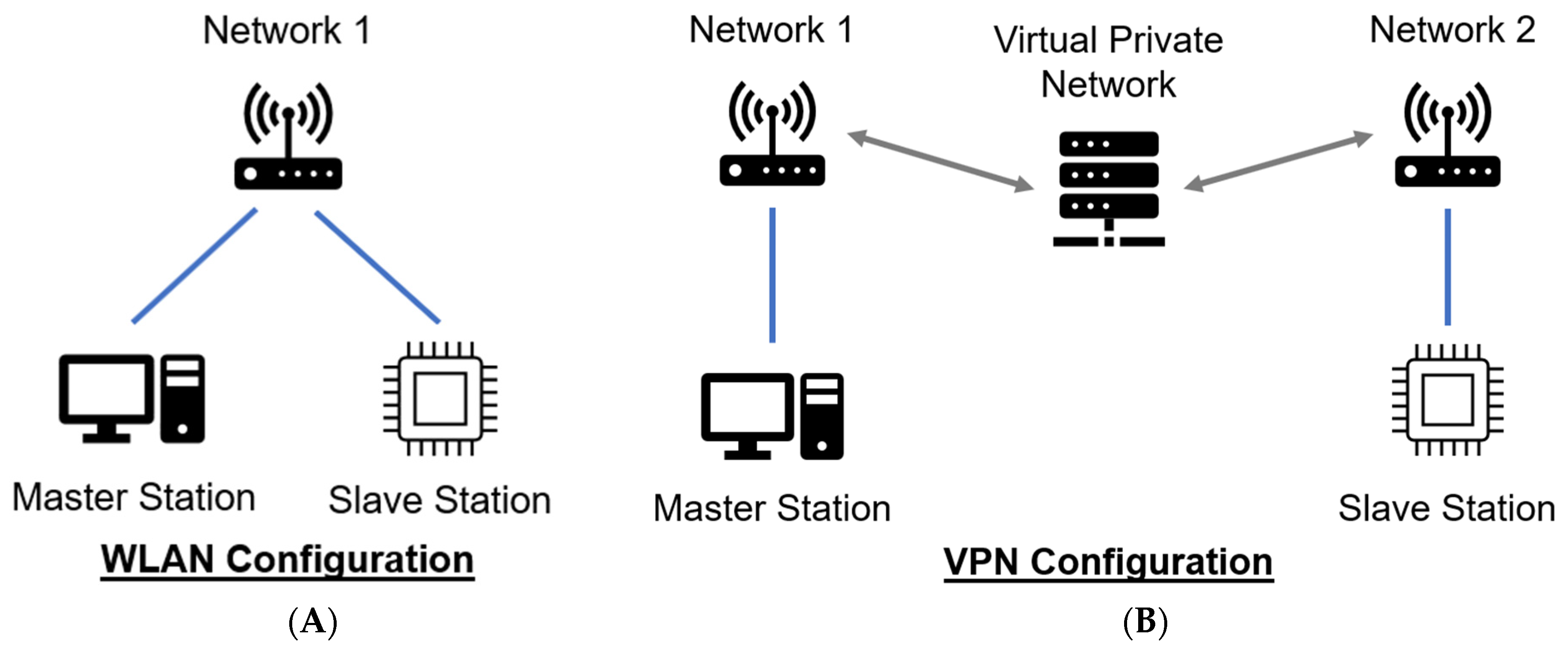
| Network Configuration | ||
|---|---|---|
| WLAN | VPN | |
| 5th Percentile (ms) | 8 | 10 |
| Median (ms) | 11 | 13 |
| Mean (ms) | 28 | 26 |
| 95th Percentile (ms) | 235 | 195 |
| Maximum (ms) | 285 | 3613 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ochitwa, Z.; Fotouhi, R.; Adams, S.J.; Noguera Cundar, A.P.; Obaid, H. MSK-TIM: A Telerobotic Ultrasound System for Assessing the Musculoskeletal System. Sensors 2024, 24, 2368. https://doi.org/10.3390/s24072368
Ochitwa Z, Fotouhi R, Adams SJ, Noguera Cundar AP, Obaid H. MSK-TIM: A Telerobotic Ultrasound System for Assessing the Musculoskeletal System. Sensors. 2024; 24(7):2368. https://doi.org/10.3390/s24072368
Chicago/Turabian StyleOchitwa, Zachary, Reza Fotouhi, Scott J. Adams, Adriana Paola Noguera Cundar, and Haron Obaid. 2024. "MSK-TIM: A Telerobotic Ultrasound System for Assessing the Musculoskeletal System" Sensors 24, no. 7: 2368. https://doi.org/10.3390/s24072368
APA StyleOchitwa, Z., Fotouhi, R., Adams, S. J., Noguera Cundar, A. P., & Obaid, H. (2024). MSK-TIM: A Telerobotic Ultrasound System for Assessing the Musculoskeletal System. Sensors, 24(7), 2368. https://doi.org/10.3390/s24072368