
A Sensor-Based Upper Limb Treatment in Hemiplegic Patients: Results from a Randomized Pilot Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Data Acquisition
- Fugl–Meyer Assessment Upper Extremity (FMA-UE) was used to measure sensorimotor function (score 0–126) [29]. The assessment tool includes subscales for motor function, sensory function, range of motion, and joint pain. Each item is evaluated on a 3-point ordinal scale ranging from 0 (not performed) to 2 (smooth and complete performance).
- -
- Motor function assessment evaluates reflex activity and range of motion in the shoulder, elbow, forearm, wrist, and hand. It involves testing flexion, extension, and rotation in specific positions. The subscale consists of 24 items, with a score range of 0 to 66.
- -
- Sensation. This has six items, and the score for this subscale ranges from 0 to 12.
- -
- Range of motion and joint pain. This has 12 items, which are scored for each range of motion and joint pain. The score for this subscale ranges from 0 to 48.
- -
- For the present study, we considered the range of joint pain (score 0–24) as a further indicator of feasibility in TG. A higher FMA-UE score indicates less upper limb impairment.
- The degree of independence and need for assistance in the basic activities of daily living (ADL) were measured using the Functional Independence Measure (FIM), which includes both motor and cognitive subscales. FIM is an 18-item ordinal scale with seven levels ranging from 1 (total dependence) to 7 (total independence), and the best score is 126. The FIM range in this study was from 18 to 126 [30].
- The global functional capacity was assessed with the Modified Barthel Index (BI) [31]. It scores from 0 to 100 (best score).
- Power Hand Grip (bilateral) was a measure of strength performed with a hydraulic dynamometer (Jamar Plus+, Performance Health, Chicago, USA) [32] and adjusted for patient body mass index.
- The Motor Evaluation Scale for Upper Extremity in Stroke (MESUPES) assesses the movements of the upper limb. It consists of two sections, one focusing on the arm and the other on the hand. In the arm section, participants are required to move the affected arm in different positions while supine and seated. The hand tasks evaluate the range of motion and hand orientation when manipulating small objects [33]. MESUPES scores range from 0 to 58, with a higher score indicating better performance.
- Arm disability was assessed with the Quick version of the Disabilities of the Arm, Shoulder, and Hand (Quick-DASH) questionnaire [34]. The Quick-DASH is an 11-item ordinal scale that rates items on a 5-level scale from 1 (no difficulty) to 5 (unable to do). It provides a summative score on a 100-point scale, with 100 indicating the most disability.
2.3. Rehabilitation Programme
Upper Limb Intervention
- For the wrist: radial and ulnar deviation movements, flexion and extension movements, and pronation and supination movements;
- For the hand: movement of opening and closing fingers;
- For the arm: up and down movements, left and right movements, and back and forth movements.
2.4. Measures
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bennett, D.A.; Krishnamurthi, R.V.; Barker-Collo, S.; Forouzanfar, M.H.; Naghavi, M.; Connor, M.; Lawes, C.M.; Moran, A.E.; Anderson, L.M.; Roth, G.A.; et al. The global burden of ischemic stroke: Findings of the GBD 2010 study. Glob. Heart 2014, 9, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Pollock, A.; Farmer, S.E.; Brady, M.C.; Langhorne, P.; Mead, G.E.; Mehrholz, J.; van Wijck, F. Interventions for improving upper limb function after stroke. Cochrane Database Syst. Rev. 2014, 2014, Cd010820. [Google Scholar] [CrossRef] [PubMed]
- Johnson, W.; Onuma, O.; Owolabi, M.; Sachdev, S. Stroke: A global response is needed. Bull. World Health Organ. 2016, 94, 634–634a. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.W.; Ma, S.R.; Choi, J.B. The Effect of Kinesio Taping Combined with Virtual-Reality-Based Upper Extremity Training on Upper Extremity Function and Self-Esteem in Stroke Patients. Healthcare 2023, 11, 1813. [Google Scholar] [CrossRef] [PubMed]
- Etoom, M.; Hawamdeh, M.; Hawamdeh, Z.; Alwardat, M.; Giordani, L.; Bacciu, S.; Scarpini, C.; Foti, C. Constraint-induced movement therapy as a rehabilitation intervention for upper extremity in stroke patients: Systematic review and meta-analysis. Int. J. Rehabil. Res. 2016, 39, 197–210. [Google Scholar] [CrossRef] [PubMed]
- Maulden, S.A.; Gassaway, J.; Horn, S.D.; Smout, R.J.; DeJong, G. Timing of initiation of rehabilitation after stroke. Arch. Phys. Med. Rehabil. 2005, 86, S34–S40. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Cohen, L.G.; Hallett, M. Nervous system reorganization following injury. Neuroscience 2002, 111, 761–773. [Google Scholar] [CrossRef]
- Teasell, R.W.; Murie Fernandez, M.; McIntyre, A.; Mehta, S. Rethinking the continuum of stroke rehabilitation. Arch. Phys. Med. Rehabil. 2014, 95, 595–596. [Google Scholar] [CrossRef] [PubMed]
- Stinear, C.M.; Lang, C.E.; Zeiler, S.; Byblow, W.D. Advances and challenges in stroke rehabilitation. Lancet Neurol. 2020, 19, 348–360. [Google Scholar] [CrossRef]
- Oujamaa, L.; Relave, I.; Froger, J.; Mottet, D.; Pelissier, J.Y. Rehabilitation of arm function after stroke. Literature review. Ann. Phys. Rehabil. Med. 2009, 52, 269–293. [Google Scholar] [CrossRef]
- French, B.; Thomas, L.H.; Coupe, J.; McMahon, N.E.; Connell, L.; Harrison, J.; Sutton, C.J.; Tishkovskaya, S.; Watkins, C.L. Repetitive task training for improving functional ability after stroke. Cochrane Database Syst. Rev. 2016, 11, Cd006073. [Google Scholar] [CrossRef]
- Hayward, K.S.; Brauer, S.G. Dose of arm activity training during acute and subacute rehabilitation post stroke: A systematic review of the literature. Clin. Rehabil. 2015, 29, 1234–1243. [Google Scholar] [CrossRef] [PubMed]
- Moulaei, K.; Bahaadinbeigy, K.; Haghdoostd, A.A.; Nezhad, M.S.; Sheikhtaheri, A. Overview of the role of robots in upper limb disabilities rehabilitation: A scoping review. Arch. Public Health 2023, 81, 84. [Google Scholar] [CrossRef] [PubMed]
- Langhorne, P.; Bernhardt, J.; Kwakkel, G. Stroke rehabilitation. Lancet 2011, 377, 1693–1702. [Google Scholar] [CrossRef]
- Kwakkel, G.; Kollen, B.J.; van der Grond, J.; Prevo, A.J. Probability of regaining dexterity in the flaccid upper limb: Impact of severity of paresis and time since onset in acute stroke. Stroke 2003, 34, 2181–2186. [Google Scholar] [CrossRef]
- Maciejasz, P.; Eschweiler, J.; Gerlach-Hahn, K.; Jansen-Troy, A.; Leonhardt, S. A survey on robotic devices for upper limb rehabilitation. J. Neuroeng. Rehabil. 2014, 11, 3. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, M.; Palazzolo, J.J.; Krol, J.; Krebs, H.I.; Hogan, N.; Volpe, B.T. Robot-aided sensorimotor arm training improves outcome in patients with chronic stroke. Neurology 2003, 61, 1604–1607. [Google Scholar] [CrossRef]
- Lo, A.C.; Guarino, P.D.; Richards, L.G.; Haselkorn, J.K.; Wittenberg, G.F.; Federman, D.G.; Ringer, R.J.; Wagner, T.H.; Krebs, H.I.; Volpe, B.T.; et al. Robot-assisted therapy for long-term upper-limb impairment after stroke. N. Engl. J. Med. 2010, 362, 1772–1783. [Google Scholar] [CrossRef]
- Vanoglio, F.; Bernocchi, P.; Mulè, C.; Garofali, F.; Mora, C.; Taveggia, G.; Scalvini, S.; Luisa, A. Feasibility and efficacy of a robotic device for hand rehabilitation in hemiplegic stroke patients: A randomized pilot controlled study. Clin. Rehabil. 2017, 31, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Hesse, S.; Schimdt, H.; Werner, C.; Bardeleben, A. Upper and lower extremity robotics devices for rehabilitation and for studying motor control. Curr. Opin. Neurol. 2003, 16, 705–710. [Google Scholar] [CrossRef]
- Iandolo, R.; Marini, F.; Semprini, M.; Laffranchi, M.; Mugnosso, M.; Cherif, A.; De Michieli, L.; Chiappalone, M.; Zenzeri, J. Perspectives and challenges in robotic neurorehabilitation. Appl. Sci. 2019, 9, 3183. [Google Scholar] [CrossRef]
- Qassim, H.M.; Wan Hasan, W.Z. A Review on Upper Limb Rehabilitation Robots. Appl. Sci. 2020, 10, 6976. [Google Scholar] [CrossRef]
- Amorim, P.; Serra, H.; Sousa, B.S.; Dias, P.; Castelo-Branco, M.; Martins, H. Chronic stroke survivors’ perspective on the use of serious games to motivate upper limb rehabilitation—A qualitative study. Health Informat. J. 2023, 29, 14604582231171932. [Google Scholar] [CrossRef]
- Vinolo, G.M.J.; Gonzalez-Medina, G.; Lucena-Anton, D.; Perez-Cabezas, V.; Ruiz-Molinero, M.D.C.; Martín-Valero, R. Augmented Reality in Physical Therapy: Systematic Review and Meta-analysis. JMIR Serious Games 2021, 9, e30985. [Google Scholar] [CrossRef]
- Khokale, R.S.; Mathew, G.; Ahmed, S.; Maheen, S.; Fawad, M.; Bandaru, P.; Zerin, A.; Nazir, Z.; Khawaja, I.; Sharif, I.; et al. Virtual and Augmented Reality in Post-stroke Rehabilitation: A Narrative Review. Cureus 2023, 15, e37559. [Google Scholar] [CrossRef]
- Leong, S.C.; Tang, Y.M.; Toh, F.M.; Fong, K.N.K. Examining the effectiveness of virtual, augmented, and mixed reality (VAMR) therapy for upper limb recovery and activities of daily living in stroke patients: A systematic review and meta-analysis. J. Neuroeng. Rehabil. 2022, 19, 93. [Google Scholar] [CrossRef]
- Sheean, G.; McGuire, J.R. Spastic Hypertonia and Movement Disorders: Pathophysiology, Clinical Presentation, and Quantification. PMR 2009, 1, 827–833. [Google Scholar] [CrossRef]
- Bamford, J.; Sandercock, P.; Dennis, M.; Burn, J.; Warlow, C. Classification and natural history of clinically identifiable subtypes of cerebral infarction. Lancet 1991, 337, 1521–1526. [Google Scholar] [CrossRef]
- Fugl-Meyer, A.R.; Jaasko, L.; Leyman, I.; Olsson, S.; Steglind, S. The post-stroke hemiplegic patient. A method for evaluation physical performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar] [CrossRef]
- Granger, C.V.; Cotter, A.C.; Hamilton, B.B.; Fiedler, R.C. Functional assessment: A study of persons after stroke. Arch. Phys. Med. Rehabil. 1993, 74, 133–138. [Google Scholar]
- Shah, S.; Vanclay, F.; Cooper, B. Improving the sensitivity of the Barthel Index for stroke rehabilitation. J. Clin. Epidemiol. 1989, 42, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Mathiowetz, V.; Kashman, N.; Volland, G.; Weber, K.; Dowe, M.; Rogers, S. Grip and pinch strengh: Normative data for adults. Arch. Phys. Med. Rehabil. 1985, 66, 69–74. [Google Scholar] [PubMed]
- Johansson, G.M.; Häger, C.K. Measurement properties of the Motor Evaluation Scale for Upper Extremity in Stroke patients (MESUPES). Disabil. Rehabil. 2012, 34, 288–294. [Google Scholar] [CrossRef]
- Beaton, D.E.; Wright, J.G.; Katz, J.N. Upper Extremity Collaborative Group. Development of the Quick DASH: Comparison of three item-reduction approaches. J. Bone Jt. Surg. Am. 2005, 87, 1038–1046. [Google Scholar]
- Bhambhani, Y.N.; Clarkson, H.M.; Gomes, P.S. Axillary crutch walking: Effects of three training programs. Arch. Phys. Med. Rehabil. 1990, 71, 484–489. [Google Scholar] [PubMed]
- National Institute for Health and Care Excellence. Stroke Rehabilitation: Long-Term Rehabilitation after Stroke; CG162; NICE: London, UK, 2013. [Google Scholar]
- Gloreha.com. Available online: https://www.gloreha.com/gloreha-aria/ (accessed on 12 February 2024).
- Arya, K.N.; Verma, R.; Garg, R.K. Estimating the minimal clinically important difference of an upper extremity recovery measure in subacute stroke patients. Top. Stroke Rehabil. 2011, 18 (Suppl. S1), 599–610. [Google Scholar] [CrossRef] [PubMed]
- Huynh, B.P.; DiCarlo, J.A.; Vora, I.; Ranford, J.; Gochyyev, P.; Lin, D.J.; Kimberley, T.J. Sensitivity to Change and Responsiveness of the Upper Extremity Fugl-Meyer Assessment in Individuals with Moderate to Severe Acute Stroke. Neurorehabilit. Neural Repair 2023, 37, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Bertani, R.; Melegari, C.; De Cola, M.C.; Bramanti, A.; Bramanti, P.; Calabrò, R.S. Effects of robot-assisted upper limb rehabilitation in stroke patients: A systematic review with meta-analysis. Neurol. Sci. 2017, 38, 1561–1569. [Google Scholar] [CrossRef] [PubMed]
- Takebayashi, T.; Takahashi, K.; Amano, S.; Gosho, M.; Sakai, M.; Hashimoto, K.; Hachisuka, K.; Uchiyama, Y.; Domen, K. Robot-Assisted Training as Self-Training for Upper-Limb Hemiplegia in Chronic Stroke: A Randomized Controlled Trial. Stroke 2022, 53, 2182–2191. [Google Scholar] [CrossRef]
- Clark, W.E.; Sivan, M.; O’Connor, R.J. Evaluating the use of robotic and virtual reality rehabilitation technologies to improve function in stroke survivors: A narrative review. J. Rehabil. Assist. Technol. Eng. 2019, 6, 2055668319863557. [Google Scholar] [CrossRef]
- Yates, M.; Kelemen, A.; Sik Lanyi, C. Virtual reality gaming in the rehabilitation of the upper extremities post-stroke. Brain Inj. 2016, 30, 855–863. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.H.; Ryu, H.; Jang, S.H. A task-specific interactive game-based virtual reality rehabilitation system for patients with stroke: A usability test and two clinical experiments. J. Neuroeng. Rehabil. 2014, 11, 32. [Google Scholar] [CrossRef] [PubMed]
- Hocine, N.; Gouaïch, A.; Cerri, S.A.; Mottet, D.; Froger, J.; Laffont, I. Adaptation in serious games for upper-limb rehabilitation: An approach to improve training outcomes. User Model. User-Adapt. Interact. 2015, 25, 65–98. [Google Scholar] [CrossRef]
- Tahir, A.; Bai, S.; Shen, M. A Wearable Multi-Modal Digital Upper Limb Assessment System for Automatic Musculoskeletal Risk Evaluation. Sensors 2023, 23, 4863. [Google Scholar] [CrossRef] [PubMed]
- Aprile, I.; Guardati, G.; Cipollini, V.; Papadopoulou, D.; Monteleone, S.; Redolfi, A.; Garattini, R.; Sacella, G.; Noro, F.; Galeri, S.; et al. Influence of Cognitive Impairment on the Recovery of Subjects with Subacute Stroke Undergoing Upper Limb Robotic Rehabilitation. Brain Sci. 2021, 11, 587. [Google Scholar] [CrossRef]
- Kim, G.J.; Parnandi, A.; Eva, S.; Schambra, H. The use of wearable sensors to assess and treat the upper extremity after stroke: A scoping review. Disabil. Rehabil. 2022, 44, 6119–6138. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Control Group (n = 11) | Treatment Group (n = 10) | p-Value | |
|---|---|---|---|
| Males, n (%) | 9 (82%) | 8 (80%) | |
| Age, years | 71 ± 13 | 68 ± 15 | 0.8639 |
| BMI, kg/m2 | 24.2 ± 3.9 | 26.8 ± 3.1 | 0.1464 |
| Time from acute event to inclusion, days | 12.7 ± 4.9 | 16.6 ± 5.9 | 0.0611 |
| Ischemic stroke, n (%) | 8 (73%) | 5 (50%) | 0.5344 |
| Haemorrhagic stroke, n (%) | 3 (27%) | 5 (50%) | |
| Paretic side: | |||
| 6 (54%) | 5 (50%) | 0.8188 |
| 5 (46%) | 5 (50%) | |
| Ashworth spasticity index of the following: | |||
| 0.47 ± 0.55 | 0.54 ± 0.74 | 0.8578 |
| 0.47 ± 0.71 | 0.44 ± 0.57 | 0.9713 |
| FIM, score | 66.9 ± 10.2 | 65.7 ± 24.5 | 0.8053 |
| Barthel Index, score | 31.1 ± 12.7 | 32.5 ± 21.1 | 0.6723 |
| Motor Skill FMA-UE, score | 30.7 ± 18.3 | 31.0 ± 13.4 | 0.8602 |
| Quick-DASH, score | 46.1 ± 25.7 | 55.9 ± 16.5 | 0.5727 |
| MESUPES, score | 22.4 ± 13.0 | 18.4 ± 12.9 | 0.6219 |
| Grip injured hand, score | 10.0 ± 8.3 | 8.6 ± 4.0 | 0.8603 |
| Grip healthy hand, score | 24.9 ± 11.0 | 30.2 ± 11.6 | 0.2599 |
| FMA Single Items | Control Group (Mean ± SD) | Treatment Group (Mean ± SD) | Changes between Post- and Pre-Intervention [Mean ± SD (95% CI)] | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | p Value | Pre | Post | p Value | ΔCG | ΔTG | p Value | |
| A. Upper Extremity | 17.6 ± 9.5 | 23.4 ± 10.1 | 0.0018 | 19.1 ± 6.4 | 25.1 ± 5.5 | 0.0007 | 5.8 ± 4.6 (2.7~8.9) | 6.0 ± 3.7 (3.3~8.7) | 0.9644 |
| B. Wrist | 3.5 ± 3.9 | 5.5 ± 2.8 | 0.0645 | 3.9 ± 3.01 | 5.9 ± 2.8 | 0.0059 | 1.9 ± 3.1 (−0.1~3.9) | 2.0 ± 1.8 (0.7~3.3) | 0.8602 |
| C. Hand | 6.6 ± 5.4 | 9.7 ± 4.8 | 0.0045 | 5.9 ± 4.7 | 10.1 ± 3.5 | 0.0089 | 3.1 ± 2.8 (1.2~4.9) | 4.2 ± 4.0 (1.3~7.1) | 0.4724 |
| D. Coordination /Speed | 2.9 ± 2.2 | 3.9 ± 1.9 | 0.0127 | 2.1 ± 1.7 | 2.6 ± 2.2 | 0.3221 | 1 ± 1.1 (0.3~1.7) | 0.5 ± 1.5 (−0.6~1.6) | 0.4790 |
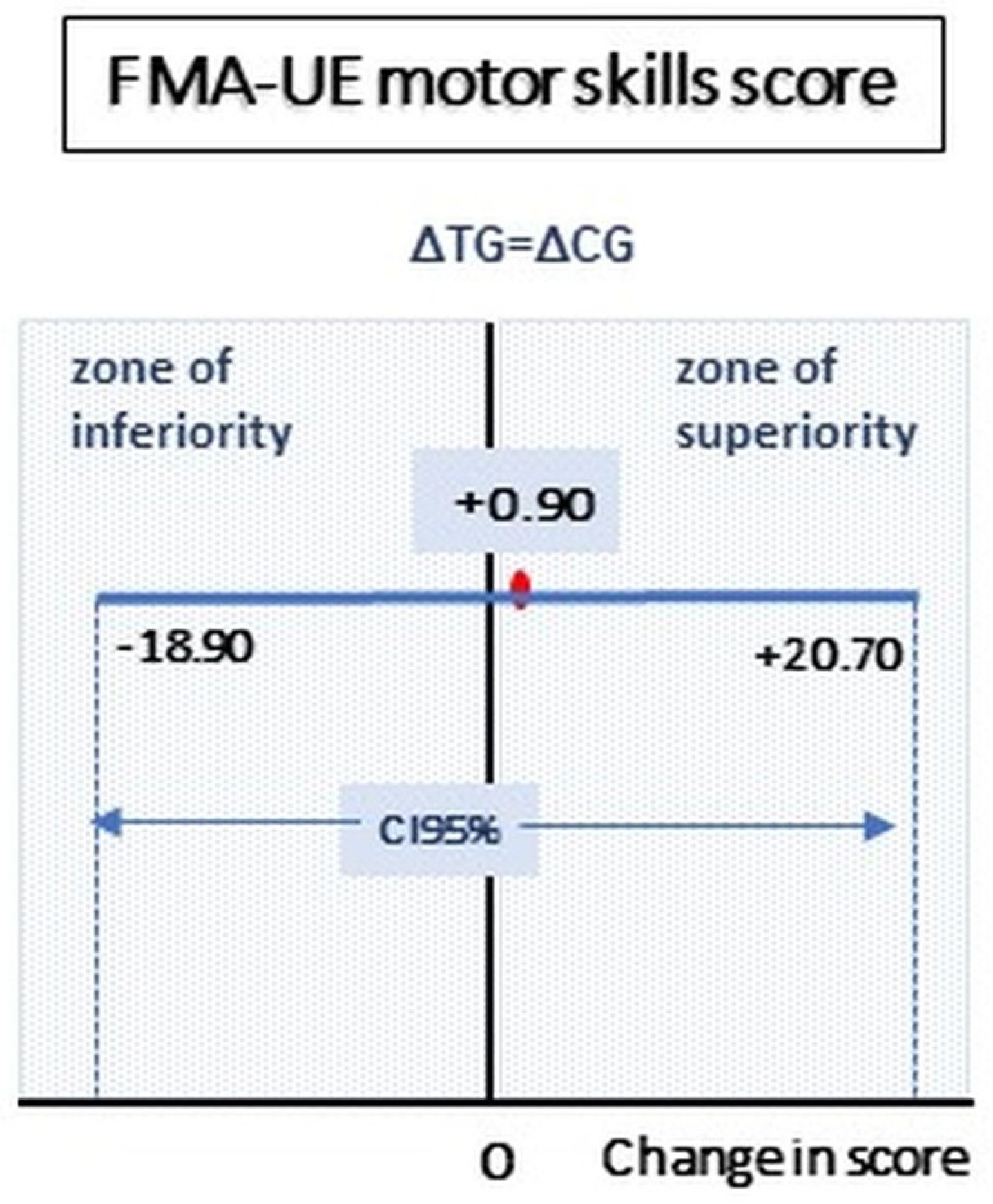
| (A–D) FMA motor skills, Figure 2 | 30.7 ± 18.3 | 42.5 ± 18.4 | 0.0017 | 31.0 ± 13.4 | 43.7 ± 11.4 | 0.0011 | 11.8 ± 9.2 (5.6~18.0) | 12.7 ± 8.6 (6.6~18.8) | 0.8664 |
| H. Sensation | 10.6 ±2.4 | 11.6 ± 0.9 | 0.1688 | 8.2 ± 4.5 | 10 ± 2.5 | 0.1309 | 1 ± 2.2 (−0.5~2.5) | 1.8 ± 3.4 (−0.7~4.3) | 0.6745 |
| J. Passive Joint motion | 16.2 ± 6.6 | 18.8 ± 6.8 | 0.0193 | 20.2 ± 3.7 | 21.3 ± 2.9 | 0.0399 | 2.6 ± 3.1 (0.5~4.7) | 1.1 ± 1.5 (0.1~2.1) | 0.1114 |
| J. Joint Pain | 23.4 ± 1.8 | 23.2 ± 2.7 | 0.8639 | 20.1 ± 3.8 | 21.8 ± 2.9 | 0.0220 | −0.2 ± 3.4 (−2.5~2.1) | 1.7 ± 2.0 (0.3~3.1) | 0.1551 |
| Barthel Index | FIM | ||
|---|---|---|---|
| Control Group | Pre | 31.1 ± 12.7 | 66.9 ± 10.2 |
| Post | 71.8 ± 20.1 | 103.5 ± 15.6 | |
| Within group p value | 0.0002 | <0.0001 | |
| Treatment Group | Pre | 32.5 ± 21.1 | 65.7 ± 24.5 |
| Post | 67.4 ± 21.1 | 98.0 ± 23.6 | |
| Within group p-value | 0.0005 | <0.0001 | |
| Changes between groups | ΔCG (T1 − T0) | 40.7 ± 24.0 (24.6~56.8) | 36.6 ± 15.4 (26.3~47.0) |
| ΔTG (T1 − T0) | 34.9 ± 21.1 (19.8~50.0) | 32.3 ± 12.0 (23.8~40.8) | |
| Between groups p-value | 0.5073 | 0.0907 |
| Quick-DASH | MESUPES | Power Hand Grip | ||
|---|---|---|---|---|
| Control Group | Pre | 46.1 ± 25.7 | 22.4 ± 13.0 | 10.0 ± 8.3 |
| Post | 43.2 ± 28.9 | 31.7 ± 10.6 | 15.8 ± 10.5 | |
| Within group p value | 0.7919 | 0.010 | 0.010 | |
| Treatment Group | Pre | 55.9 ± 16.5 | 18.4 ± 12.9 | 8.6 ± 4.0 |
| Post | 45.2 ± 18.2 | 27.5 ± 13.9 | 17.2 ± 8.6 | |
| Within group p-value | 0.1377 | 0.010 | 0.0201 | |
| Changes between groups | ΔCG (T1-T0) | −2.9 ± 35.7 (−26.9~21.1) | 9.4 ± 8.7 (3.5~15.2) | 5.7 ± 5.3 (2.1~9.3) |
| ΔTG (T1-T0) | −10.7 ± 20.7 (−25.5~4.1) | 9.1 ± 8.8 (2.8~15.4) | 8.7 ± 9.7 (1.7~15.6) | |
| Between groups p-value | 0.6504 | 0.8603 | 0.5068 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vanoglio, F.; Comini, L.; Gaiani, M.; Bonometti, G.P.; Luisa, A.; Bernocchi, P. A Sensor-Based Upper Limb Treatment in Hemiplegic Patients: Results from a Randomized Pilot Study. Sensors 2024, 24, 2574. https://doi.org/10.3390/s24082574
Vanoglio F, Comini L, Gaiani M, Bonometti GP, Luisa A, Bernocchi P. A Sensor-Based Upper Limb Treatment in Hemiplegic Patients: Results from a Randomized Pilot Study. Sensors. 2024; 24(8):2574. https://doi.org/10.3390/s24082574
Chicago/Turabian StyleVanoglio, Fabio, Laura Comini, Marta Gaiani, Gian Pietro Bonometti, Alberto Luisa, and Palmira Bernocchi. 2024. "A Sensor-Based Upper Limb Treatment in Hemiplegic Patients: Results from a Randomized Pilot Study" Sensors 24, no. 8: 2574. https://doi.org/10.3390/s24082574