4.1. Participants, Study Design, and Ethics
The present study included healthy overweight or obese adults living in Bergen and the surrounding areas. Participants were recruited through advertising in the internal network at Haukeland University Hospital (Bergen, Norway) and posters (Bergen city centre and at Haukeland University Hospital). Recruitment took place in August and September 2013, and the study was conducted in September, October, and November 2013.
Eligibility criteria for participation in the study were age between 20 and 65 years, BMI >28 kg/m2, stable body weight with less than 5 kg fluctuation during the preceding 4 months, and fasting blood glucose <7.0 mmol/L. Exclusion criteria were known diseases or metabolic disturbances related to being overweight or obese, use of prescription medications that affect blood lipids or blood glucose concentrations, allergies towards fish or seafood, undertaking a weight loss diet, or tobacco use exceeding >15 cigarettes or snus/day. Pregnant or lactating women and candidates with a seafood consumption exceeding 200 g/week or taking dietary supplements including cod liver oil or other marine fatty acids were not included in the study.
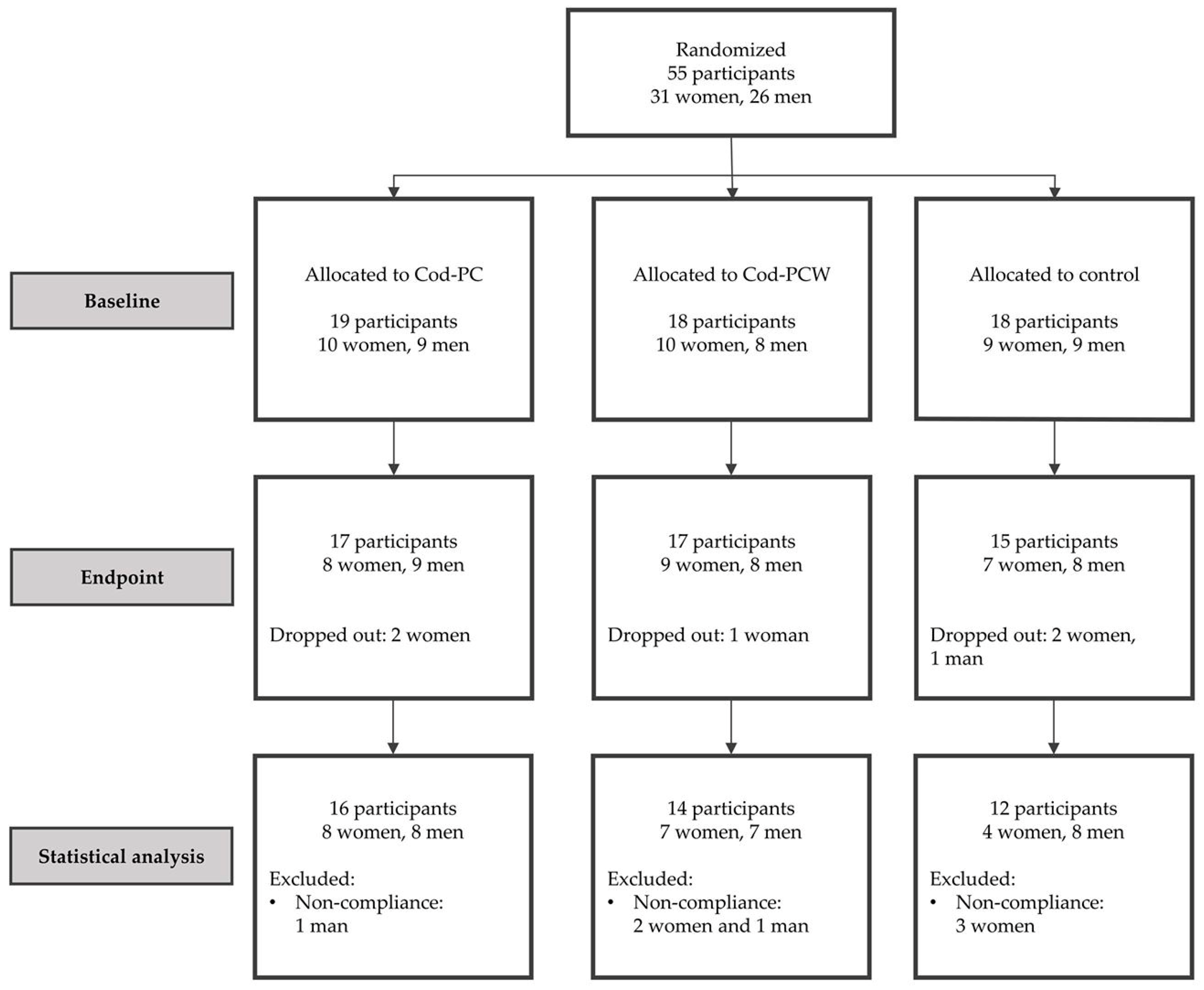
Fifty-five eligible volunteers were included in this randomized, parallel, double-blind intervention study conducted at the University of Bergen (Bergen, Norway). Participants were stratified according to gender, age, and BMI before randomization to one of the three experimental groups. The intervention tablets were coded (A, B, and C) by the manufacturer to ensure that all participants and personnel in the study were blinded. The study was conducted in accordance with the guidelines laid down by the Declaration of Helsinki and was approved by the Regional Ethics Committee of Western Norway (approval No.: 2011/572). All participants provided written informed consent before enrolment in the study. The study is registered at clinical trials.gov (NCT01894542).
4.2. Intervention and Protocol for Study Visits
Participants consumed 6 g of cod protein or control supplements daily for eight weeks (18 tablets per day). During the study period, participants were instructed to maintain their normal dietary habits and level of physical activity. Both intervention supplements contained fishmeal of residual material from Northeast Atlantic cod (Gadus morhua). Participants in the three intervention arms received either supplements containing protein from Cod-PC, supplements containing protein from Cod-PCW, or control supplements with no active ingredients (placebo).
Participants attended two study visits during the intervention period; one visit at baseline and one visit at endpoint, i.e., after eight weeks. Both study visits were conducted after an overnight fast (>10 h) which included no intake of food or drink except water and no use of tobacco or medications. Participants were advised to avoid intensive physical activity and alcohol intake during the 24 h preceding each study visit. Prior to the baseline visit, all participants received an e-mail with information about the study, the declaration of consent, and the forms to fill in their dietary records.
During the baseline visit, fasting blood glucose was measured using the Contour blood glucose meter (Bayer Consumer Care AG, Basel, Switzerland) to ensure that the participants’ fasting blood glucose was <7 mmol/L. Height was measured using a stadiometer (MZ10023-3, ADE GmbH & Co., Hamburg, Germany). Body composition was measured at the baseline and the endpoint visits using a bioelectrical impedance analyser (Tanita BC-418 Segmental Body Composition Analyzer, Arlington Heights, IL, USA) while participants were in a fasting state. Blood samples were collected at baseline and endpoint using an antecubital venous catheter. Fasting blood samples were drawn in the morning between 8:00 and 10:00 a.m., and postprandial samples were drawn after consuming a standardized breakfast meal. Blood samples were collected in Vacuette Z Serum Clot Activator Tubes (Greiner Bio-One, Frickenhausen, Germany) for isolation of serum and Vacuette K2EDTA (Greiner Bio-One GmbH, Germany) for isolation of plasma. GLP-1 was preserved in EDTA blood samples by immediately adding 10 μL dipeptidyl peptidase-IV Inhibitor (DRG Instruments GmbH, Marburg, Germany) per mL whole blood. Serum, plasma, and whole blood samples were stored at −80 °C until analysis.
The standardized breakfast meal consisted of two crisp breads (Wasa Frukost, Barilla AS, Stockholm, Sweden), 20 g margarine (Soft Flora, Mills DA, Oslo, Norway), 40 g cheese (Gräddost, Tine AS, Oslo, Norway), 4 crackers (Gjende original, Orkla Confectionery & Snacks, Solna, Sweden), and a drink containing 0.06 L fruit concentrate (Husholdningssaft, Rema 1000, Oslo, Norway) and 20 g glucose powder (Nutana, Mariager, Denmark) mixed with 0.25 L water. The total energy content of the standardized breakfast meal was 739 kcal and contained 13 g protein, 37 g fat, 87 g carbohydrate, and 3 g fibre. The participants were instructed to consume the breakfast meal within 10 min at the first visit and were encouraged to eat at similar pace during the second visit.
The subcutaneous adipose tissue biopsy was performed in the lower abdominal region of all participants, however, the quality of three samples (one from each group) was too poor for further analysis and the samples were discarded. The biopsy was initiated by applying an anaesthetic EMLA patch (Aspen Pharmacare, St Leonards NSW, Australia) on the biopsy area approximately 45 min before the biopsy, followed by a local anaesthetic injected in a fan shape (5 μL Lidokain 10 mg/mL FarmaPlus AS, Oslo, Norway). An incision (2–3 mm) was made using a scalpel, then a Hepafix syringe (Hepafix® from B.Braun, Melsungen AG, Melsungen, Germany) with a Sterican biopsy needle (B.Braun, Melsungen AG) was inserted and subcutaneous adipose tissue was extracted. The adipose tissue sample was immediately rinsed twice with sterile 0.9% NaCl (Ecoflac®, B.Braun, Melsungen AG) solution before it was transferred to liquid nitrogen. Biopsy samples were stored at −80 °C until analysis.
4.3. Production, Analyses, and Contents of Intervention Tablets
Cod residual material from cod fillet production was processed on-board the fishing vessel Granit (Halstensen Granit AS, Bekkjarvik, Norway). The fish residuals were grinded and heat treated in a continuous cooker before mechanical pressing to separate most of the aqueous fraction (stickwater) containing water-soluble protein from the solid phase (presscake). The solid phase was dried onboard the fishing vessel to produce a presscake meal, while the stickwater was frozen and transported to land where it was thawed and concentrated before mixed with the presscake meal and dried at Nofima (Bergen, Norway). Two fishmeals were produced for inclusion in the supplements. The Cod-PC tablets contained a meal based on cod presscake as the sole source of protein, containing only remnants of water-soluble protein corresponding to 15.5% of crude protein, and the Cod-PCW tablets contained a meal based on presscake with the addition of water-soluble protein in the form of stickwater, corresponding to 35.4% of crude protein.
All intervention tablets contained similar amounts of sorbitol, tricalcium phosphate, and magnesium stearate. The cod protein supplements contained fishmeal from cod residual material (
Table 5). Microcrystalline cellulose was used as a filler and replaced fishmeal in the control supplements. Tablets were produced by Faun Pharma AS (Vestby, Norway). All analyses of the intervention tablets were conducted by Nofima BioLab (Bergen, Norway). Ten tablets from each supplement were crushed and mixed, and two samples from each supplement were taken for each analysis. The presented results are the means of two measurements. The microorganism Salmonella was analysed using PCR combined with NMKL method 71 [
27] and aerobe microorganisms were analysed with Petrifilm™ Aerobic Count Plate (ISO 4833-1). Enterobacteriaceae were analysed using the colony count technique (ISO 21528-2), Coliform bacteria and Escherichia coli were analysed using Petrifilm™ Coliform/Escherichia coli Count Plate (NordVal 014), and Presumptive Bacillus cereus was analysed using the colony count technique (ISO 7932). Mould and yeast were analysed with Petrifilm™ Mold and Yeast Count plate (NordVal 016). The crude protein content (N × 6.25) of the supplements was determined by the Dumas method (AOAC 990.03). Water-soluble protein content was determined based on the Kjeldahl method (ISO 5983-2). Total amino acid composition was measured by HPLC according to the method of Cohen and Michaud [
28]. Tryptophan was determined by the method of Miller [
29]. Taurine was measured in the water-soluble protein by HPLC using the Waters Pico-Tag method [
30]. Fat content and fatty acid composition was prepared according to the AOCS method Ce 1b-89 and measured as previously described by Oterhals and Nygård [
31].
The daily intake of the amino acids arginine, histidine, isoleucine, lysine, methionine, phenylalanine, threonine, tryptophan and valine from intervention tablets were comparable in the Cod-PC and Cod-PCW tablets (i.e., less than 40 mg/day difference), whereas the intake of leucine was higher from the Cod-PC tablets compared with the Cod-PCW tablets, and glycine and taurine from the Cod-PCW tablets were higher than from the Cod-PC tablets (
Table 6). The essential fatty acids 18:2n-6 and 18:3n-3 and the long-chain n-3 PUFAs were found in slightly higher amounts in the Cod-PC tablets compared to the Cod-PCW tablets, whereas the amounts of these fatty acids were below detection levels in the control tablets (
Table 6).
4.6. Analyses of mRNA Expression in Subcutaneous Adipose Tissue
Total RNA was purified from subcutaneous white adipose tissue using the RNeasy Mini Kit (Qiagen, Hilden, Germany) according to the manufacturer’s protocol. RNA concentration and quality were measured using QIAxpert (Qiagen, Hilden, Germany). High Capacity cDNA Reverse Transcription Kit (Applied Biosystems, CA, USA) was used to synthesize cDNA from 150 ng total RNA per sample. cDNA was diluted 1:5 with PCR-grade water before qPCR was performed (in triplicate) using the LightCycler480 rapid thermal cycler system (Roche Diagnostics GmbH, Basel, Switzerland) with the LightCycler 480 SYBR Green I Master (Roche, Basel, Switzerland). The following primers were used: DGAT1; forward primer 3′actaccgtggcatcctgaac’5 and reverse primer 3′ataaccgggcattgctca’5, DGAT2; forward primer 3′actaccgtggcatcctgaac’5 and reverse primer 3′ataaccgggcattgctca’5, LPL; forward primer 3′caggcctttgagatttctctgt’5 and reverse primer 3′gaaggagtaggtcttatttgtggaa’5, CD36; forward primer 3′tggaacagaggctgacaactt’5 and reverse primer 3′ttgattttgatagatatgggatgc’5. As reference genes, 3 primer pairs were tested: Hypoxanthine phosphoribosyltransferase 1 (HPRT1); forward primer 3′tgaccttgatttattttgcatacc’5 and reverse primer 3′cgagcaagacgttcagtcct’5, importin 8 (IPO8); forward primer 3′acagcactgcaggaggtgta’5 and reverse primer 3′gcctccctgttgttcaatct’5, TATA-box binding protein (TBP) forward primer 3′tgaatcttggttgtaaacttgacc’5 and reverse primer 3′ctcatgattaccgcagcaaa’5. Of these reference genes, IPO8 had least variation in readings of samples in triplets, therefore results are presented relative to IPO8.





{kind=link}
{kind=link}