
Dynamics of Viral Shedding and Symptoms in Patients with Asymptomatic or Mild COVID-19

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Symptom Score and Saliva Sample Collection
2.2. Laboratory Procedure
2.3. Statistical Analysis
3. Results
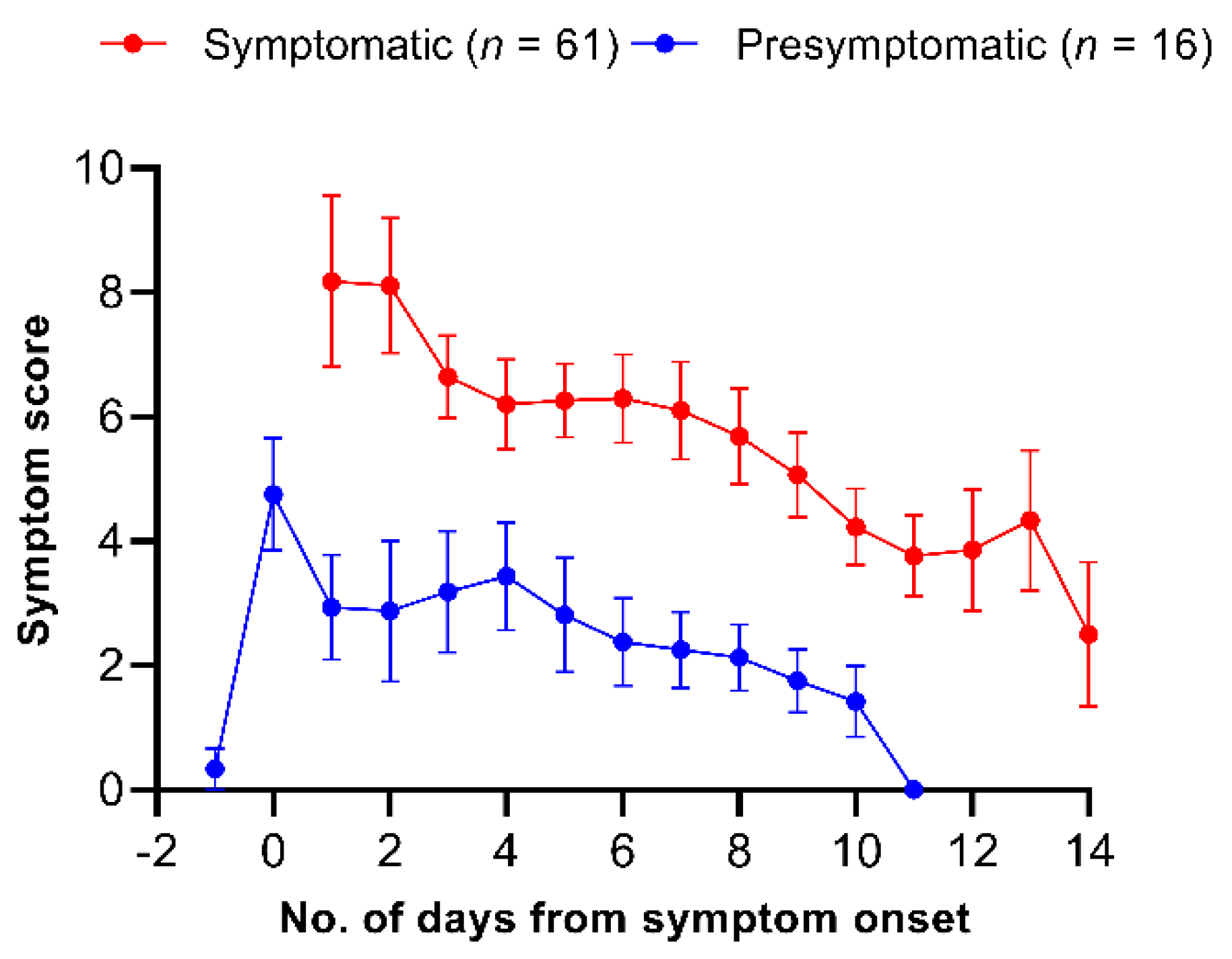
3.1. Dynamics of Symptoms in Patients with Mild COVID-19
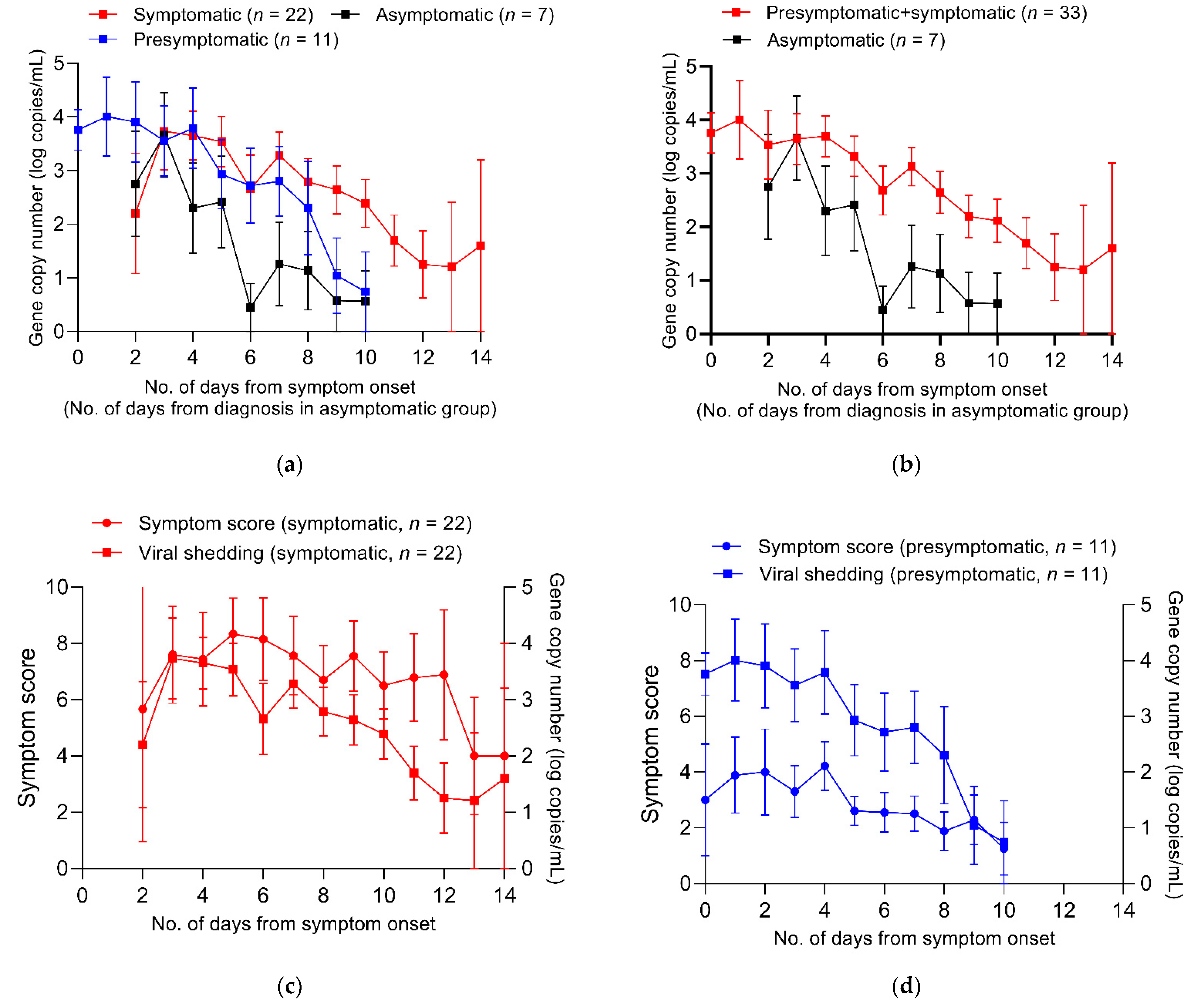
3.2. Viral Shedding Kinetics
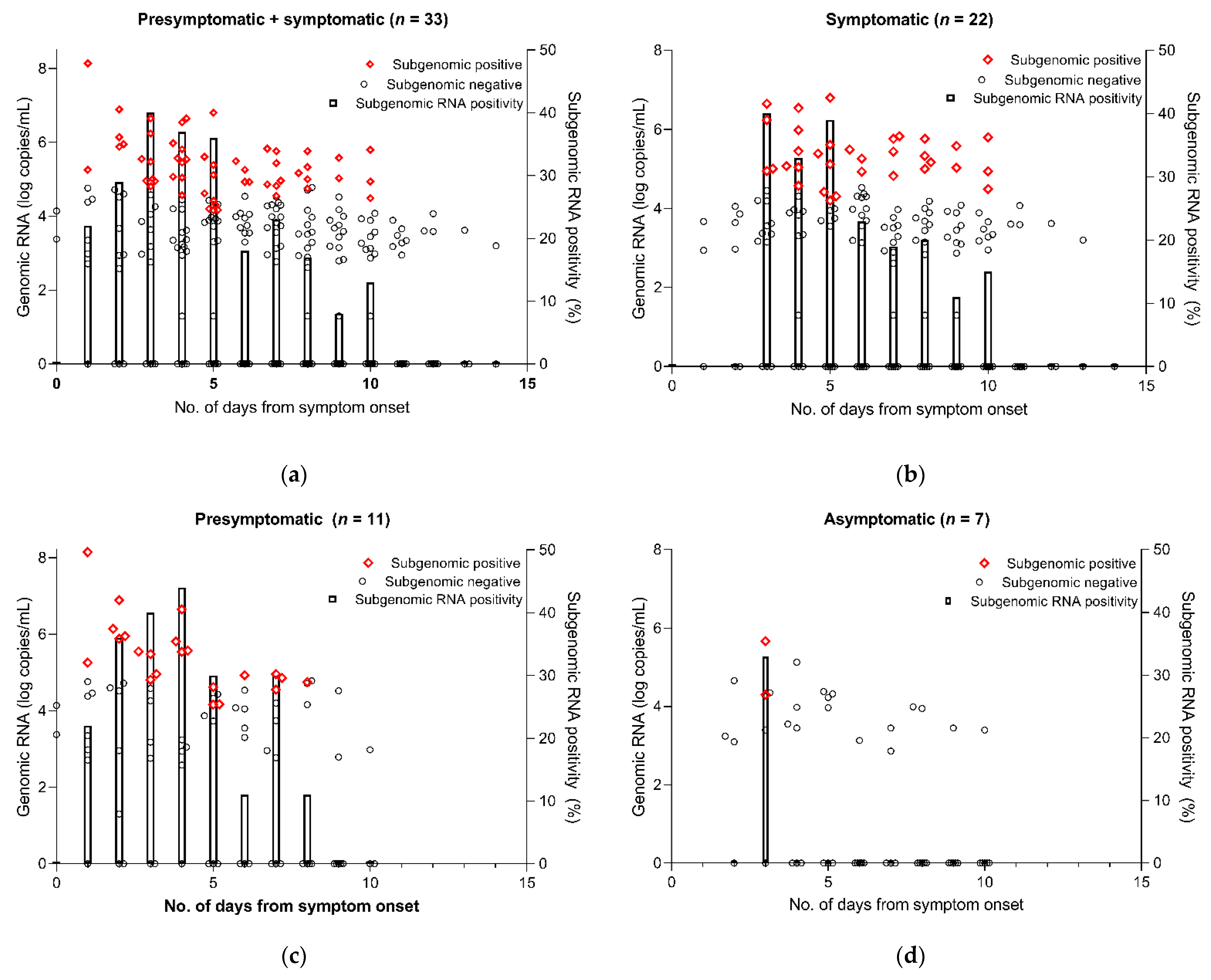
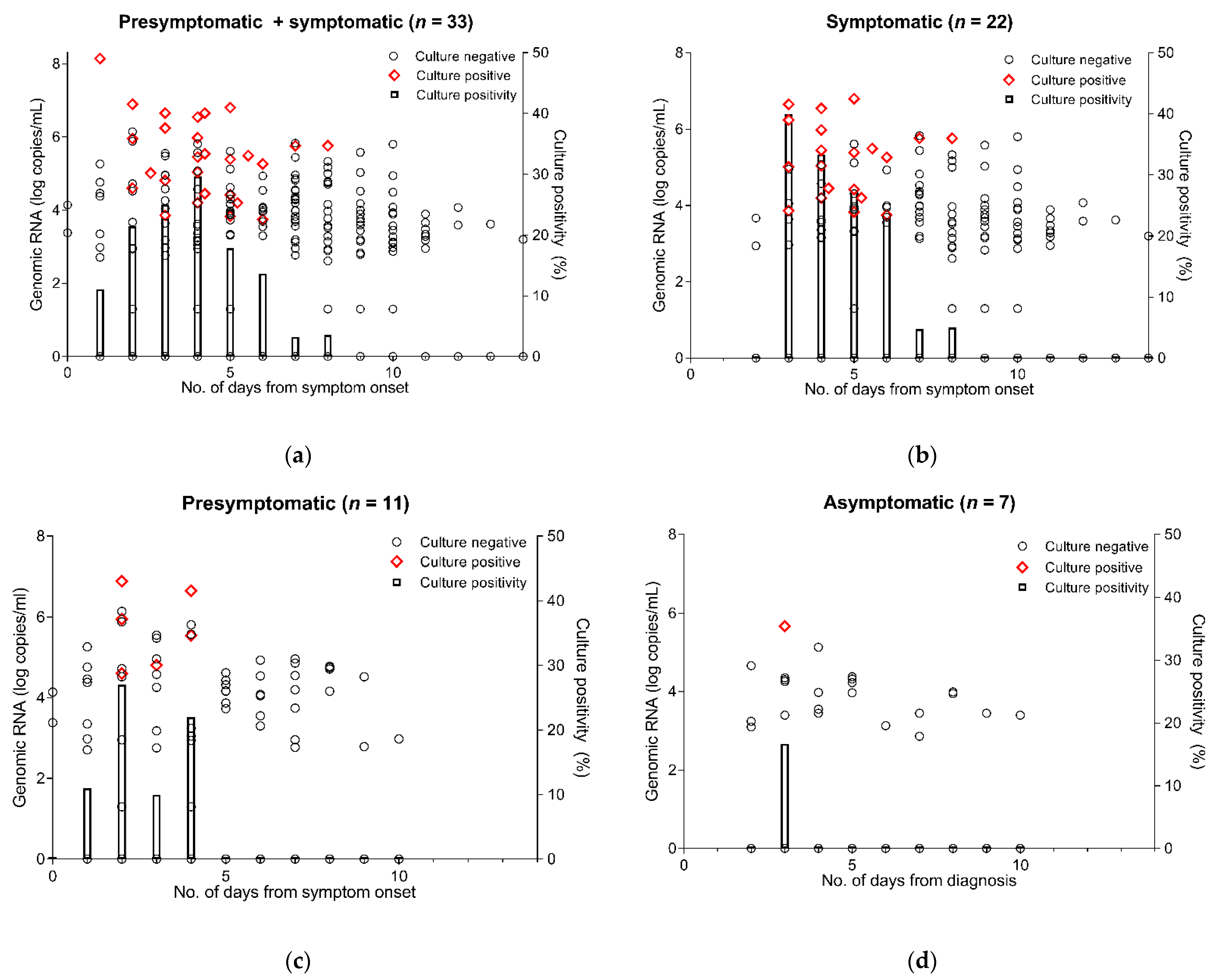
3.3. Subgenomic RNA Viral Shedding and Isolation of SARS-CoV-2 by Culture
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bae, S.; Lim, J.S.; Kim, J.Y.; Jung, J.; Kim, S.H. Transmission characteristics of SARS-CoV-2 that hinder effective control. Immune Netw. 2021, 21, e9. [Google Scholar] [CrossRef] [PubMed]
- Ra, S.; Lim, J.S.; Kim, G.; Kim, M.J.; Jung, J.; Kim, S.H. Upper respiratory viral load in asymptomatic individuals and mildly symptomatic patients with SARS-CoV-2 infection. Thorax 2021, 76, 61–63. [Google Scholar] [CrossRef] [PubMed]
- Oran, D.P.; Topol, E.J. The proportion of SARS-CoV-2 infections that are asymptomatic. Ann. Intern. Med. 2021, 174, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Li, Y.Y.; Liu, M.J.; Fang, L.Q.; Dean, N.E.; Wong, G.W.; Yang, X.B.; Longini, I.; Halloran, M.E.; Wang, H.J.; et al. Household transmission of SARS-CoV-2 and risk factors for susceptibility and infectivity in Wuhan: A retrospective observational study. Lancet Infect. Dis. 2021, 21, 617–628. [Google Scholar] [CrossRef]
- Carrat, F.; Vergu, E.; Ferguson, N.M.; Lemaitre, M.; Cauchemez, S.; Leach, S.; Valleron, A.-J. Timelines of infection and disease in human influenza: A review of volunteer challenge studies. Am. J. Epidemiol. 2008, 167, 775–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bender, J.K.; Brandl, M.; Hohle, M.; Buchholz, U.; Zeitlmann, N. Analysis of asymptomatic and presymtomatic transmission in SARS-CoV-2 outbreak, Germany, 2020. Emerg. Infect. Dis. 2021, 27, 1159–1163. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.; Liu, F.; Chang, Z.; Lin, Y.; Ren, M.; Zheng, C.; Li, Y.; Peng, Z.; Qin, Y.; Yu, J.; et al. Assessing asymptomatic, pre-symptomatic and symptomatic transmission risk of SARS-CoV-2. Clin. Infect. Dis. 2021. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Perera, R.A.; Tso, E.; Tsang, O.T.; Tsang, D.N.; Fung, K.; Leung, Y.W.; Chin, A.W.; Chu, D.K.; Cheng, S.M.; Poon, L.L.; et al. SARS-CoV-2 Virus Culture and Subgenomic RNA for Respiratory Specimens from Patients with Mild Coronavirus Disease. Emerg. Infect. Dis. 2020, 26, 2701–2704. [Google Scholar] [CrossRef] [PubMed]
- Wölfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Müller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ford, L.; Lee, C.; Pray, I.W.; Cole, D.; Bigouette, J.P.; Abedi, G.R.; Bushman, D.; Delahoy, M.J.; Currie, D.W.; Cherney, B.; et al. Epidemiologic characteristics associated with SARS-CoV-2 antigen-based test results, rRT-PCR cycle threshold values, subgenomic RNA, and viral culture results from university testing. Clin. Infect. Dis. 2021, 73, e1348–e1355. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Bae, J.Y.; Bae, S.; Cha, H.H.; Kwon, J.S.; Suh, M.H.; Lee, H.J.; Jung, J.; Kim, M.J.; Cui, C.; et al. Diagnostic usefulness of subgenomic RNA detection of viable SARS-CoV-2 in patients with COVID-19. Clin. Microbiol. Infect. 2021, S1198-743X(21)00466-3, Online ahead of print. [Google Scholar] [CrossRef]
- Barrett, B.; Brown, R.; Mundt, M.; Safdar, N.; Dye, L.; Maberry, R.; Alt, J. The Wisconsin Upper Respiratory Symptom Survey is responsive, reliable, and valid. J. Clin. Epidemiol. 2005, 58, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Barrett, B.; Brown, R.; Voland, R.; Maberry, R.; Turner, R. Relations among questionnaire and laboratory measures of rhinovirus infection. Eur. Respir. J. 2006, 28, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.A.; Weber, W.J.; Martin, E.T.; Mccarty, R.L.; Englund, J.A. Development of a symptom score for clinical studies to identify children with a documented viral upper respiratory tract infection. Pediatr. Res. 2010, 68, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.H.; Park, A.K.; Kim, J.M.; Kim, H.M.; Lee, N.-J.; Woo, S.H.; Lee, C.Y.; Lee, J.; Rhee, J.E.; Kim, E.-J. COVID-19 variant surveillance in the Republic of Korea. Public Health Wkly. Rep. 2021, 14, 922–929. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 89) | Asymptomatic (n = 12) | Presymptomatic (n = 16) | Symptomatic (n = 61) | p Value |
|---|---|---|---|---|---|
| Sex | 0.35 | ||||
| Female | 51 (57.3) | 6 (50.0) | 7 (43.8) | 38 (62.3) | |
| Male | 38 (42.7) | 6 (50.0) | 9 (56.2) | 23 (37.7) | |
| Age, median years (IQR) | 49 (34–60) | 61 (51–62.5) | 58 (42–62) | 44 (33–55) | 0.001 |
| Underlying condition | |||||
| Hypertension | 20 (22.5) | 3 (25.0) | 6 (37.5) | 11 (18.0) | 0.25 |
| Diabetes | 8 (9.0) | 1 (8.3) | 2 (12.5) | 5 (8.2) | 0.86 |
| Asthma | 2 (2.2) | 0 (0) | 0 (0) | 2 (3.3) | 0.63 |
| Pregnancy | 1 (1.1) | 0 (0) | 0 (0) | 1 (1.6) | 0.79 |
| Smoking | 12 (13.5) | 2 (16.7) | 2 (12.5) | 8 (13.1) | 0.92 |
| Days from diagnosis to admission | 0.83 | ||||
| 0 | 77 (86.5) | 11 (91.7) | 14 (87.5) | 52 (85.2) | |
| 1 | 12 (13.5) | 1 (8.3) | 2 (12.5) | 9 (14.8) | |
| Days from symptom onset to admission, median (IQR) | 2 (1–3) | NA | 0 (0–0) | 2 (1–3) | <0.001 |
| Length of stay, median days (IQR) | 11 (11–11) | 11 (11–11) | 11 (11–11) | 11 (11–11) | 0.37 |
| Clinical course | 0.18 | ||||
| Discharge per protocol | 82 (92.1) | 12 (100) | 16 (100) | 54 (88.5) | |
| Transfer to hospital | 7 (7.9) | 0 (0) | 0 (0) | 7 (11.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bae, S.; Kim, J.Y.; Lim, S.Y.; Park, H.; Cha, H.H.; Kwon, J.-S.; Suh, M.H.; Lee, H.J.; Lim, J.S.; Jung, J.; et al. Dynamics of Viral Shedding and Symptoms in Patients with Asymptomatic or Mild COVID-19. Viruses 2021, 13, 2133. https://doi.org/10.3390/v13112133
Bae S, Kim JY, Lim SY, Park H, Cha HH, Kwon J-S, Suh MH, Lee HJ, Lim JS, Jung J, et al. Dynamics of Viral Shedding and Symptoms in Patients with Asymptomatic or Mild COVID-19. Viruses. 2021; 13(11):2133. https://doi.org/10.3390/v13112133
Chicago/Turabian StyleBae, Seongman, Ji Yeun Kim, So Yun Lim, Heedo Park, Hye Hee Cha, Ji-Soo Kwon, Mi Hyun Suh, Hyun Jung Lee, Joon Seo Lim, Jiwon Jung, and et al. 2021. "Dynamics of Viral Shedding and Symptoms in Patients with Asymptomatic or Mild COVID-19" Viruses 13, no. 11: 2133. https://doi.org/10.3390/v13112133
APA StyleBae, S., Kim, J. Y., Lim, S. Y., Park, H., Cha, H. H., Kwon, J.-S., Suh, M. H., Lee, H. J., Lim, J. S., Jung, J., Kim, M. J., Chong, Y. P., Lee, S.-O., Choi, S.-H., Kim, Y. S., Lee, H. Y., Lee, S., Park, M.-S., & Kim, S.-H. (2021). Dynamics of Viral Shedding and Symptoms in Patients with Asymptomatic or Mild COVID-19. Viruses, 13(11), 2133. https://doi.org/10.3390/v13112133