
A Contemporary Systematic Review on Repartition of HPV-Positivity in Oropharyngeal Cancer Worldwide

 , ,
, , 
Abstract
:1. Introduction
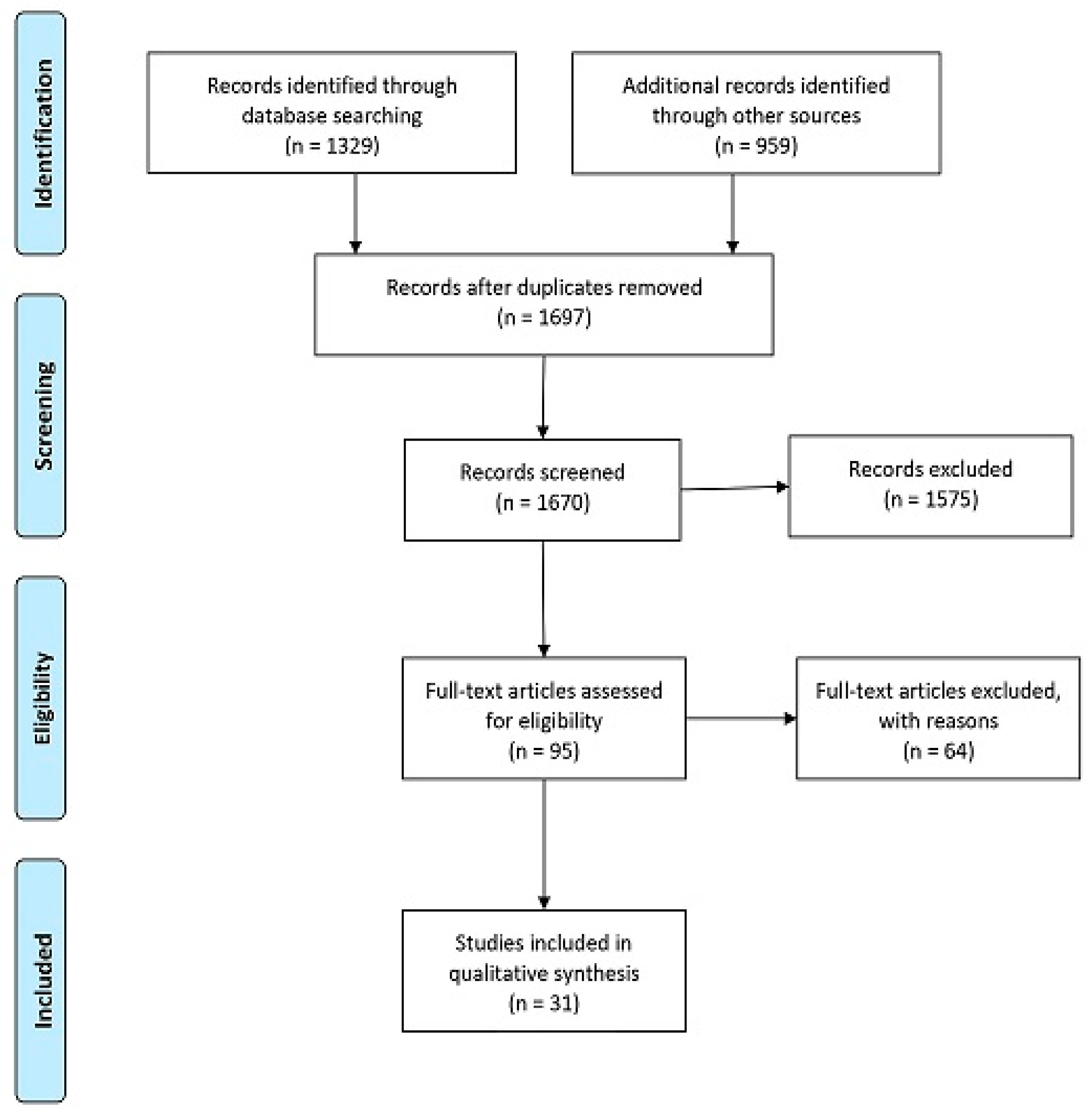
2. Materials and Methods
2.1. Search Strategy and Data Extraction
- HPV or human papillomavirus or human papilloma virus
- Oropharyn_ cancer or oropharyn_ neoplasm or oropharyn_ carcinoma or oropharyn_ malignancy or oropharyn_ tumor or oropharyn_ tumour
- Incidence or frequency or prevalence
2.2. Data Analysis
3. Results
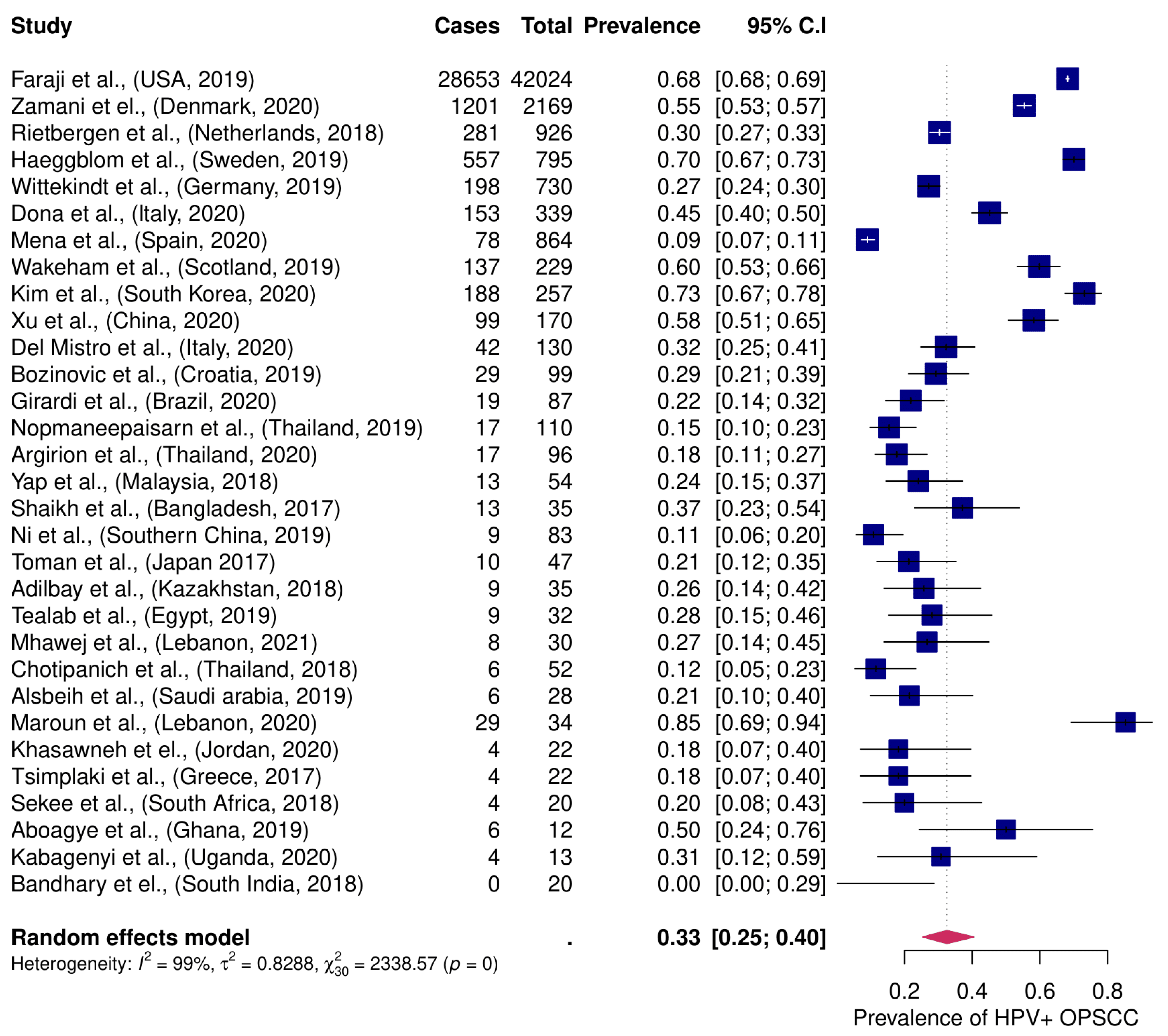
3.1. Global Burden of HPV+ OPSCC
3.2. HPV Detection Methods and Definition
3.3. HPV Genotypes
3.4. Clinical Characteristics of HPV+ OPSCC
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [Green Version]
- Chaturvedi, A.K.; Anderson, W.F.; Lortet-Tieulent, J.; Curado, M.P.; Ferlay, J.; Franceschi, S.; Rosenberg, P.S.; Bray, F.; Gillison, M.L. Worldwide Trends in Incidence Rates for Oral Cavity and Oropharyngeal Cancers. J. Clin. Oncol. 2013, 31, 4550–4559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalianis, T. Human papillomavirus and oropharyngeal cancer, the epidemics, and significance of additional clinical biomarkers for prediction of response to therapy (review). Int. J. Oncol. 2014, 45, 1799–1805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamani, M.; Grønhøj, C.; Jensen, D.H.; Carlander, A.F.; Agander, T.; Kiss, K.; Olsen, C.; Baandrup, L.; Nielsen, F.C.; Andersen, E.; et al. The current epidemic of HPV-associated oropharyngeal cancer: An 18-year Danish population-based study with 2,169 patients. Eur. J. Cancer 2020, 134, 52–59. [Google Scholar] [CrossRef]
- Bouvard, V.; Baan, R.; Straif, K.; Grosse, Y.; Secretan, B.; El Ghissassi, F.; Benbrahim-Tallaa, L.; Guha, N.; Freeman, C.; Galichet, L.; et al. A review of human carcinogens--Part B: Biological agents. Lancet Oncol. 2009, 10, 321–322. [Google Scholar] [CrossRef]
- Hayes, D.N.; Van Waes, C.; Seiwert, T.Y. Genetic Landscape of Human Papillomavirus-Associated Head and Neck Cancer and Comparison to Tobacco-Related Tumors. J. Clin. Oncol. 2015, 33, 3227–3234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, J.S.; Khan, R.A.; Masand, R.P.; Chernock, R.D.; Zhang, Q.; Al-Naief, N.S.; Muller, S.; McHugh, J.B.; Prasad, M.L.; Brandwein-Gensler, M.; et al. Recognition of nonkeratinizing morphology in oropharyngeal squamous cell carcinoma—A prospective cohort and interobserver variability study. Histopathology 2012, 60, 427–436. [Google Scholar] [CrossRef] [Green Version]
- Grønhøj, C.; Jensen, D.H.; Dehlendorff, C.; Marklund, L.; Wagner, S.; Mehanna, H.; Munck-Wikland, E.; Ramqvist, T.; Näsman, A.; Wittekindt, C.; et al. Development and external validation of nomograms in oropharyngeal cancer patients with known HPV-DNA status: A European Multicentre Study (OroGrams). Br. J. Cancer 2018. [Google Scholar] [CrossRef]
- Mirghani, H.; Casiraghi, O.; Guerlain, J.; Amen, F.; He, M.X.; Ma, X.J.; Luo, Y.; Mourareau, C.; Drusch, F.; Lakdhar, A.B.; et al. Diagnosis of HPV driven oropharyngeal cancers: Comparing p16 based algorithms with the RNAscope HPV-test. Oral. Oncol. 2016, 62, 101–108. [Google Scholar] [CrossRef]
- Mariz, B.A.L.A.; Kowalski, L.P.; William, W.N.; de Castro, G.; Chaves, A.L.F.; Santos, M.; de Oliveira, T.B.; Araújo, A.L.D.; Normando, A.G.C.; Ribeiro, A.C.P.; et al. Global prevalence of human papillomavirus-driven oropharyngeal squamous cell carcinoma following the ASCO guidelines: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2020, 156. [Google Scholar] [CrossRef]
- Stjernstrøm, K.D.; Jensen, J.S.; Jakobsen, K.K.; Grønhøj, C.; von Buchwald, C. Current status of human papillomavirus positivity in oropharyngeal squamous cell carcinoma in Europe: A systematic review. Acta Otolaryngol. 2019, 139, 1112–1116. [Google Scholar] [CrossRef]
- Aboagye, E.; Agyemang-Yeboah, F.; Duduyemi, B.M.; Obirikorang, C. Human papillomavirus detection in head and neck squamous cell carcinomas at a tertiary hospital in Sub-Saharan Africa. Sci. World J. 2019, 2019. [Google Scholar] [CrossRef] [Green Version]
- Faraji, F.; Rettig, E.M.; Tsai, H.L.; El Asmar, M.; Fung, N.; Eisele, D.W.; Fakhry, C. The prevalence of human papillomavirus in oropharyngeal cancer is increasing regardless of sex or race, and the influence of sex and race on survival is modified by human papillomavirus tumor status. Cancer 2019, 125, 761–769. [Google Scholar] [CrossRef] [PubMed]
- Bandhary, S.K.; Shetty, V.; Saldanha, M.; Gatti, P.; Devegowda, D.; Pushkal, S.R.; Shetty, A.K. Detection of human papilloma virus and risk factors among patients with head and neck squamous cell carcinoma attending a tertiary referral centre in South India. Asian Pacific J. Cancer Prev. 2018, 19, 1325–1330. [Google Scholar] [CrossRef]
- Maroun, C.A.; Al Feghali, K.; Traboulsi, H.; Dabbous, H.; Abbas, F.; Dunya, G.; Ziade, G.; Mahfouz, R.; Youssef, B.; Tamim, H.; et al. HPV-related oropharyngeal cancer prevalence in a middle eastern population using E6/E7 PCR. Infect. Agent. Cancer 2020, 15, 1–7. [Google Scholar] [CrossRef]
- Tealab, S.H.; Sedhom, N.F.H.; Hassouna, A.; Gouda, I.; Ismail, H. Prevalence of human papilloma virus in oropharyngeal, tongue and lip squamous cell carcinoma: An experience from the Egyptian National Cancer Institute. J. Investig. Med. 2019, 67, 1061–1066. [Google Scholar] [CrossRef] [PubMed]
- Kabagenyi, F.; Otiti, J.; Namwagala, J.; Kamulegeya, A.; Kalungi, S. A descriptive study of human papilloma virus in upper aero-digestive squamous cell carcinoma at Uganda cancer institute assessed by P16 immunohistochemistry. Cancers Head Neck 2020, 5. [Google Scholar] [CrossRef] [PubMed]
- Sekee, T.R.; Burt, F.J.; Goedhals, D.; Goedhals, J.; Munsamy, Y.; Seedat, R.Y. Human papillomavirus in head and neck squamous cell carcinomas in a South African cohort. Papillomavirus Res. 2018, 6, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Argirion, I.; Zarins, K.R.; McHugh, J.; Cantley, R.L.; Teeramatwanich, W.; Laohasiriwong, S.; Kasemsiri, P.; Naruikon, J.; Srimanta, P.; Chinn, S.B.; et al. Increasing prevalence of HPV in oropharyngeal carcinoma suggests adaptation of p16 screening in Southeast Asia. J. Clin. Virol. 2020, 132, 104637. [Google Scholar] [CrossRef]
- Kim, Y.; Joo, Y.H.; Kim, M.S.; Lee, Y.S. Prevalence of high-risk human papillomavirus and its genotype distribution in head and neck squamous cell carcinomas. J. Pathol. Transl. Med. 2020, 54, 411–418. [Google Scholar] [CrossRef]
- Xu, T.; Shen, C.; Wei, Y.; Hu, C.; Wang, Y.; Xiang, J.; Sun, G.H.; Su, F.; Wang, Q.; Lu, X. Human papillomavirus (HPV) in Chinese oropharyngeal squamous cell carcinoma (OPSCC): A strong predilection for the tonsil. Cancer Med. 2020, 9, 6556–6564. [Google Scholar] [CrossRef]
- Ni, G.; Huang, K.; Luan, Y.; Cao, Z.; Chen, S.; Ma, B.; Yuan, J.; Wu, X.; Chen, G.; Wang, T.; et al. Human papillomavirus infection among head and neck squamous cell carcinomas in southern China. PLoS ONE 2019, 14, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Nopmaneepaisarn, T.; Tangjaturonrasme, N.; Rawangban, W.; Vinayanuwattikun, C.; Keelawat, S.; Bychkov, A. Low prevalence of p16-positive HPV-related head-neck cancers in Thailand: Tertiary referral center experience. BMC Cancer 2019, 19, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Chotipanich, A.; Siriarechakul, S.; Mungkung, O. Role of high-risk human papillomavirus in the etiology of oral and oropharyngeal cancers in Thailand: A case–control study. SAGE Open Med. 2018, 6, 205031211876560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaikh, M.H.; Khan, A.I.; Sadat, A.; Chowdhury, A.H.; Jinnah, S.A.; Gopalan, V.; Lam, A.K.; Clarke, D.T.W.; McMillan, N.A.J.; Johnson, N.W. Prevalence and types of high-risk human papillomaviruses in head and neck cancers from Bangladesh. BMC Cancer 2017, 17, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toman, J.; Von Larson, S.; Umeno, H.; Kurita, T.; Furusaka, T.; Hasegawa, H.; Prasad, M.L.; Sasaki, C.T. HPV-Positive Oropharyngeal Cancer Via p16 Immunohistochemistry in Japan. Ann. Otol. Rhinol. Laryngol. 2017, 126, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Yap, L.F.; Lai, S.L.; Rhodes, A.; Sathasivam, H.P.; Abdullah, M.A.; Pua, K.C.; Rajadurai, P.; Cheah, P.L.; Thavaraj, S.; Robinson, M.; et al. Clinico-pathological features of oropharyngeal squamous cell carcinomas in Malaysia with reference to HPV infection. Infect. Agent. Cancer 2018, 13, 1–6. [Google Scholar] [CrossRef]
- Alsbeih, G.; Al-Harbi, N.; Bin Judia, S.; Al-Qahtani, W.; Khoja, H.; El-Sebaie, M.; Tulbah, A. Prevalence of human papillomavirus (HPV) infection and the association with survival in saudi patients with head and neck squamous cell carcinoma. Cancers 2019, 11, 820. [Google Scholar] [CrossRef] [Green Version]
- Khasawneh, A.I.; Himsawi, N.; Abu-Raideh, J.; Salameh, M.; Abdullah, N.; Khasawneh, R.; Saleh, T. Prevalence of Human Papillomavirus Associated with Head and Neck Squamous Cell Carcinoma in Jordanian Patients. Open Microbiol. J. 2020, 14, 57–64. [Google Scholar] [CrossRef]
- Mhawej, R.; Ghorra, C.; Naderi, S.; Khoueir, N.; Abou Hamad, W.; Melkane, A.E. Human papillomavirus prevalence and clinicopathological associations in oropharyngeal squamous cell carcinoma in the Lebanese population. J. Laryngol. Otol. 2018, 132, 636–641. [Google Scholar] [CrossRef]
- Girardi, F.M.; Wagner, V.P.; Martins, M.D.; Abentroth, A.L.; Hauth, L.A. Prevalence of p16 expression in oropharyngeal squamous cell carcinoma in southern Brazil. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 130, 681–691. [Google Scholar] [CrossRef]
- Donà, M.G.; Rollo, F.; Pichi, B.; Spriano, G.; Moretto, S.; Covello, R.; Pellini, R.; Benevolo, M. Evolving profile of hpv-driven oropharyngeal squamous cell carcinoma in a national cancer institute in italy: A 10-year retrospective study. Microorganisms 2020, 8, 1498. [Google Scholar] [CrossRef]
- Haeggblom, L.; Attoff, T.; Jingru, Y.; Holzhauser, S.; Vlastos, A.; Mirzae, L.; Ährlund-Richter, A.; Munck-wikland, E.; Marklund, L.; Lalle, H.-N.; et al. Changes in incidence and prevalence of human papillomavirus in tonsillar and base of tongue cancer during 2000-2016 in the Stockholm region and Sweden. Head Neck 2018, 1–8. [Google Scholar] [CrossRef]
- Mena, M.; Frias-Gomez, J.; Taberna, M.; Quirós, B.; Marquez, S.; Clavero, O.; Baena, A.; Lloveras, B.; Alejo, M.; León, X.; et al. Epidemiology of human papillomavirus-related oropharyngeal cancer in a classically low-burden region of southern Europe. Sci. Rep. 2020, 10, 1–11. [Google Scholar] [CrossRef]
- Rietbergen, M.M.; van Bokhoven, A.A.J.D.; Lissenberg-Witte, B.I.; Heideman, D.A.M.; Leemans, C.R.; Brakenhoff, R.H.; Bloemena, E. Epidemiologic associations of HPV-positive oropharyngeal cancer and (pre)cancerous cervical lesions. Int. J. Cancer 2018, 143, 283–288. [Google Scholar] [CrossRef]
- Tsimplaki, E.; Argyri, E.; Sakellaridis, A.; Kyrodimos, E.; Xesfyngi, D.; Panotopoulou, E. Oropharyngeal and laryngeal but not oral cancers are strongly associated with high-risk human papillomavirus in 172 Greek patients. J. Med. Virol. 2017, 89, 170–176. [Google Scholar] [CrossRef]
- Božinović, K.; Sabol, I.; Rakušić, Z.; Jakovčević, A.; Šekerija, M.; Lukinović, J.; Prgomet, D.; Grce, M. HPV-driven oropharyngeal squamous cell cancer in Croatia—Demography and survival. PLoS ONE 2019, 14, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Mistro, A.; Frayle, H.; Menegaldo, A.; Favaretto, N.; Gori, S.; Nicolai, P.; Spinato, G.; Romeo, S.; Tirelli, G.; da Mosto, M.C.; et al. Age-independent increasing prevalence of Human Papillomavirus-driven oropharyngeal carcinomas in North-East Italy. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wittekindt, C.; Wagner, S.; Bushnak, A.; Prigge, E.S.; Von Knebel Doeberitz, M.; Wurdemann, N.; Bernhardt, K.; Pons-Kuhnemann, J.; Maulbecker-Armstrong, C.; Klussmann, J.P. Increasing incidence rates of oropharyngeal squamous cell carcinoma in Germany and significance of disease burden attributed to human papillomavirus. Cancer Prev. Res. 2019, 12, 375–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adilbay, D.; Adilbayev, G.; Kidirbayeva, G.; Shipilova, V.; Sadyk, Z.; Koyanbekova, G.; Sokolenko, E.; Klozar, J. HPV infection and P16 expression in oral and oropharyngeal cancer in Kazakhstan. Infect. Agent. Cancer 2018, 13, 2–5. [Google Scholar] [CrossRef] [PubMed]
- Wakeham, K.; Pan, J.; Pollock, K.G.; Millan, D.; Bell, S.; McLellan, D.; McPhaden, A.; Conway, D.I.; Graham, S.V.; Kavanagh, K.; et al. A Prospective Cohort Study of Human Papillomavirus-Driven Oropharyngeal Cancers: Implications for Prognosis and Immunisation. Clin. Oncol. 2019, 31, e132–e142. [Google Scholar] [CrossRef]
- Lewis, J.S.; Beadle, B.; Bishop, J.A.; Chernock, R.D.; Colasacco, C.; Lacchetti, C.; Moncur, J.T.; Rocco, J.W.; Schwartz, M.R.; Seethala, R.R.; et al. Human papillomavirus testing in head and neck carcinomas guideline from the college of American pathologists. Arch. Pathol. Lab. Med. 2018, 142, 559–597. [Google Scholar] [CrossRef] [Green Version]
- Castellsagué, X.; Alemany, L.; Quer, M.; Halec, G.; Quirós, B.; Tous, S.; Clavero, O.; Alòs, L.; Biegner, T.; Szafarowski, T.; et al. HPV Involvement in Head and Neck Cancers: Comprehensive Assessment of Biomarkers in 3680 Patients. J. Natl. Cancer Inst. 2016, 108, 1–12. [Google Scholar] [CrossRef]
- Näsman, A.; Du, J.; Dalianis, T. A global epidemic increase of an HPV-induced tonsil and tongue base cancer—potential benefit from a pan-gender use of HPV vaccine. J. Intern. Med. 2020, 287, 134–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lehtinen, M.; Luostarinen, T.; Vänskä, S.; Söderlund-Strand, A.; Eriksson, T.; Natunen, K.; Apter, D.; Baussano, I.; Harjula, K.; Hokkanen, M.; et al. Gender-neutral vaccination provides improved control of human papillomavirus types 18/31/33/35 through herd immunity: Results of a community randomized trial (III). Int. J. Cancer 2018, 143, 2299–2310. [Google Scholar] [CrossRef] [PubMed]
- Mehanna, H.; Bryant, T.S.; Babrah, J.; Louie, K.; Bryant, J.L.; Spruce, R.J.; Batis, N.; Olaleye, O.; Jones, J.; Struijk, L.; et al. Human Papillomavirus (HPV) Vaccine Effectiveness and Potential Herd Immunity for Reducing Oncogenic Oropharyngeal HPV-16 Prevalence in the United Kingdom: A Cross-sectional Study. Clin. Infect. Dis. 2019, 69, 1296–1302. [Google Scholar] [CrossRef] [Green Version]
- Wolff, E.; Elfström, K.M.; Haugen Cange, H.; Larsson, S.; Englund, H.; Sparén, P.; Roth, A. Cost-effectiveness of sex-neutral HPV-vaccination in Sweden, accounting for herd-immunity and sexual behaviour. Vaccine 2018, 36, 5160–5165. [Google Scholar] [CrossRef] [PubMed]
- Schache, A.G.; Liloglou, T.; Risk, J.M.; Filia, A.; Jones, T.M.; Sheard, J.; Woolgar, J.A.; Helliwell, T.R.; Triantafyllou, A.; Robinson, M.; et al. Evaluation of human papilloma virus diagnostic testing in oropharyngeal squamous cell carcinoma: Sensitivity, specificity, and prognostic discrimination. Clin. Cancer Res. 2011, 17, 6262–6271. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Authors (Area, Publication Year) | Centre/Data Source | Study Period | Cases | Age Median | F:M Ratio in Total | Share of HPV+ Patients in % | OPSCC Sublocations (Share of HPV+ Patients in %) | Definition of HPV Positivity Based on | ||
|---|---|---|---|---|---|---|---|---|---|---|
| HPV+ | HPV- | Overall | ||||||||
| Africa | ||||||||||
| Ghana, 2019 [12] | Tertiary Hospital, Kusami | 2007–2016 | 12 | - | - | - | - | 50 | - | HPV DNA |
| Egypt, 2019 [16] | National Cancer institute | 2008–2015 | 32 | - | - | - | 1:1 | 28 | - | HPV DNA and p16 (>70%) |
| Uganda, 2020 [17] | Uganda Cancer Institute | 2018–2019 | 13 | - | - | - | - | 31 | - | p16 (>70%) |
| South Africa, 2018 [18] | Universitas Academic Hospital | 2014–2017 | 20 | - | - | - | - | 20 | - | p16 (>70%) |
| Asian-Pacific | ||||||||||
| South India, 2018 [14] | K.S.Hegde Medical Academy | 2014–2016 | 20 | - | - | - | - | 0 | - | HPV DNA |
| Thailand, 2020 [19] | Srinagarind Hospital | 2012–2017 | 96 | 55 * | 57 * | - | 1:4.6 | 18 | TSCC (41%), BTSCC (7%) soft palate, other (4%) | HPV DNA and p16 (>70%) |
| South Korea, 2020 [20] | Catholic Medical Center hospitals, Seoul St. Mary’s Hospital, Bucheon St. Mary’s Hospital | 2011–2019 | 257 | - | - | - | - | 73 | TSCC (78%), BTSCC (61%), soft palate, uvula, other (38%) | HPV DNA and p16 (>70%) |
| China, 2020 [21] | Fudan University Shanghai Cancer Center | 2007–2019 | 170 | 56 | 59 | - | 1:6 | 58 | TSCC (69%), BTSCC (42%), soft palate, pharyngeal wall (27%) | p16 (>70%) |
| Southern China, 2019 [22] | Foshan First People’s Hospital, First Affiliated Hospital of Guangdong Pharmaceutical University, Second Affiliated Hospital of Wenzhou Medical University | 2009–2017 | 83 | - | - | - | 1:4 | 11 | TSCC (48%), BTSCC (19%), palate (50%) | HPV DNA and p16 (>75%) |
| Thailand, 2019 [23] | King Chulalongkorn Memorial Hospital | 2010–2016 | 110 | 59 * | 59 * | 59 * | 1:6 | 15 | TSCC (35%) | HPV DNA and p16 (>70%) |
| Thailand, 2018 [24] | Chonburi and Lopburi cancer hospitals | 2016 | 52 | - | - | 60.4 | 1:12 | 12 | TSCC (9%), BTSCC (1%), other (16%) | HPV DNA (only 16/18) |
| Bangladesh, 2017 [25] | Dhaka Medical College Hospital | 2014–2016 | 35 | - | - | - | - | 36 | - | HPV DNA |
| Japan, 2017 [26] | Nihon University, Kurume University | 2010–2015 | 47 | 57 * | 64 * | - | 1:8 | 22 | - | p16 (>70%) |
| Malaysia, 2018 [27] | - | 2004–2015 | 54 | 62 * | 67 * | 65 * | 1:2 | 24 | - | p16 (>70%) |
| Middle East | ||||||||||
| Lebanon, 2020 [15] | American university og Beirut Medical Center | 1972–2017 | 34 | 59 * | 58 * | 59 * | 1:3 | 85 | TSCC (86%), BTSCC (82%), soft palate (100%) | HPV DNA |
| Saudi Arabia, 2019 [28] | KFSHRC Hospital | 2002–2016 | 28 | - | - | - | 1:1.8 | 21 | TSCC (25%, BTSCC (21%), soft palate (1%) | HPV DNA and p16 (>70%) |
| Jordan, 2020 [29] | King Hussein Cancer and Medical Centers | 2013–2018 | 22 | - | - | - | - | 18 | TSCC (33%), BTSCC (50%), soft palate (33%) | HPV DNA |
| Lebanon, 2021 [30] | Hotel Dieu de France Hospital | 2010–2016 | 30 | 60 * | 64 * | 58 * | 1:2 | 27 | lymfoid areas (77%), non-lymfoid areas (23%) | HPV DNA and p16 (>10%) |
| North America | ||||||||||
| USA, 2019 [13] | United States National Cancer Database | 2010–2015 | 42.024 | 59 * | 62 * | 60 * | 1:4.8 | 68 | TSCC(72%), BTSCC (67%), other (50%) | - |
| South America | ||||||||||
| Brazil, 2020 [31] | Ana Nery Hospital | 2017–2019 | 87 | 61 * | 62 * | 61 * | 1:6 | 21 | - | p16 (>75%) |
| Europe | ||||||||||
| Denmark, 2020 [4] | Rigshospitalet, University of Copenhagen | 2000–2017 | 2169 | 61 ** | 65 ** | 62 ** | 1:2.6 | 55 | TSCC (71%), BTSCC (58%), other (17%) | HPV DNA and p16 (>75%) |
| ltaly, 2020 [32] | Italian Cancer Institute | 2010–2019 | 339 | - | - | 61 | 1:3.5 | 48 | TSCC (58%), BTSCC (49%), other (20%) | HPV DNA and p16 (>75%) |
| Sweden, 2019 [33] | Stockholm | 2000–2016 | 795 | - | - | - | 1:3 | 70 | TSCC (74%), BTSCC (63%) | HPV DNA and p16 (>70%) |
| Spain, 2020 [34] | Catalan Institute of Oncology-Bellvitge, Hospital, Hospital del Mar, Hospital Parc Taulí and Hospital de la Santa Creu i Sant Pau | 1991–2016 | 864 | 59 * | - | 60 * | 1:8 | 10 | TSCC (15%), BTSCC (8%), others (3%) | HPV DNA and p16 (>70%) |
| Netherlands, 2018 [35] | VU University Medical Center | 2000–2015 | 926 | 59 | 61 | - | 1:2 | 30 | TSCC (39%), BTSCC (38%), soft palate, uvula, other (8%) | HPV DNA and p16 (staining not specified) |
| Greece, 2017 [36] | St. Svvas Regionl Anticancer Oncology University of Athens | 2013–2015 | 22 | - | - | 59 | 1:2 | 18 | TSCC (27%), BTSCC (14%), soft palate (0%) | HPV DNA |
| Croatia, 2019 [37] | University hospital Center Zagreb | 2002–2015 | 99 | 60 | 60 | 60 | 1:4 | 29 | TSCC(43%), BTSCC (45%) soft palatae, other (17%) | HPV DNA and HPV RNA |
| Italy, 2020 [38] | Treviso Regional Hospital, Hospital of Mirano, and Trieste Cattinara Hospital | 2000–2018 | 130 | - | - | 65 | 1:3 | 32 | TSCC (26%), BTSCC (28%), other (5%) | HPV DNA and p16 (>70%) |
| Germany, 2019 [39] | ENT-Giessen | 2000–2017 | 730 | - | - | - | - | 27 | - | HPV DNA and p16 (>70%) |
| Kazakhstan, 2018 [40] | Kazakh Institute of Oncology and Radiology | 2015–2017 | 35 | - | - | - | 1:2.5 | 26 | - | HPV DNA and p16 (>70%) |
| Scotland, 2019 [41] | West of Scotland Cancer Network | 2013–2015 | 229 | - | - | 60 | 1:3 | 60 | - | HPV DNA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carlander, A.F.; Jakobsen, K.K.; Bendtsen, S.K.; Garset-Zamani, M.; Lynggaard, C.D.; Jensen, J.S.; Grønhøj, C.; Buchwald, C.v. A Contemporary Systematic Review on Repartition of HPV-Positivity in Oropharyngeal Cancer Worldwide. Viruses 2021, 13, 1326. https://doi.org/10.3390/v13071326
Carlander AF, Jakobsen KK, Bendtsen SK, Garset-Zamani M, Lynggaard CD, Jensen JS, Grønhøj C, Buchwald Cv. A Contemporary Systematic Review on Repartition of HPV-Positivity in Oropharyngeal Cancer Worldwide. Viruses. 2021; 13(7):1326. https://doi.org/10.3390/v13071326
Chicago/Turabian StyleCarlander, Amanda F., Kathrine K. Jakobsen, Simone K. Bendtsen, Martin Garset-Zamani, Charlotte D. Lynggaard, Jakob Schmidt Jensen, Christian Grønhøj, and Christian von Buchwald. 2021. "A Contemporary Systematic Review on Repartition of HPV-Positivity in Oropharyngeal Cancer Worldwide" Viruses 13, no. 7: 1326. https://doi.org/10.3390/v13071326
APA StyleCarlander, A. F., Jakobsen, K. K., Bendtsen, S. K., Garset-Zamani, M., Lynggaard, C. D., Jensen, J. S., Grønhøj, C., & Buchwald, C. v. (2021). A Contemporary Systematic Review on Repartition of HPV-Positivity in Oropharyngeal Cancer Worldwide. Viruses, 13(7), 1326. https://doi.org/10.3390/v13071326