


Rildo: Real-World Multicenter Study on the Effectiveness and Safety of Single-Tablet Regimen of Dolutegravir plus Rilpivirine in Treatment-Experienced People Living with HIV
 , ,
, ,
Abstract
:1. Background
2. Patients and Methods
2.1. Study Design and Setting
2.2. Inclusion Criteria
2.3. Variables/Data Sources
2.4. Pharmacoeconomic Analysis
3. Results
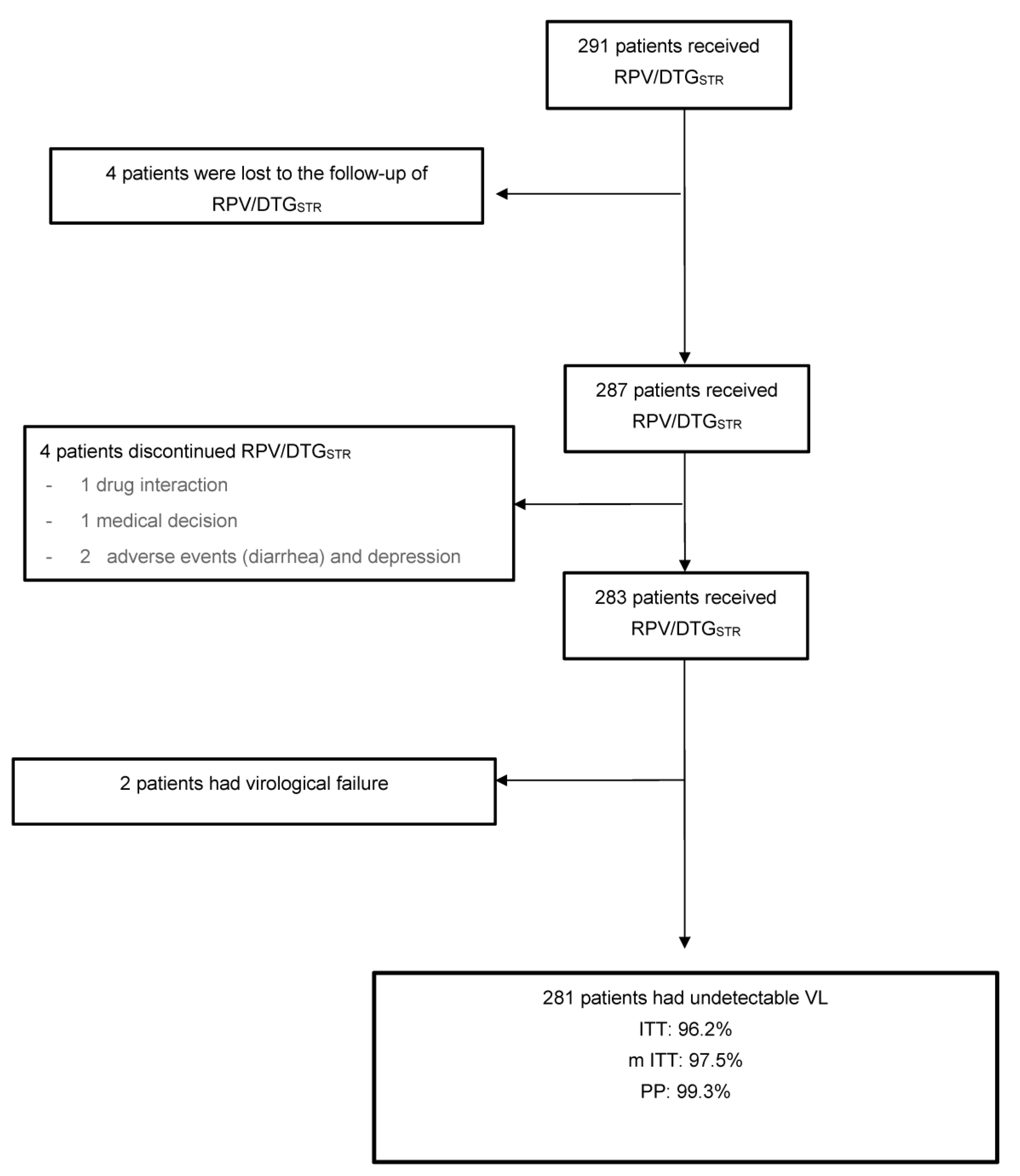
3.1. Study Population
3.2. DR Effectiveness and Safety
3.3. Analytical Parameters
3.4. Pharmacoeconomic Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Palella, F.J., Jr.; Delaney, K.M.; Moorman, A.C.; Loveless, M.O.; Fuhrer, J.; Satten, G.A.; Aschman, D.J.; Holmberg, S.D.; HIV Outpatient Study Investigators. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N. Engl. J. Med. 1998, 338, 853–860. [Google Scholar] [CrossRef]
- European AIDS Clinical Society GUIDELINES Version 10.1 October 2020. Available online: https://www.eacsociety.org/guidelines/guidelines-archive/ (accessed on 17 September 2022).
- Perez-Molina, J.A.; Rubio, R.; Rivero, A.; Pasquau, J.; Suárez-Lozano, I.; Riera, M.; Estébanez, M.; Santos, J.; Sanz-Moreno, J.; Troya, J.; et al. Dual treatment with atazanavir-ritonavir plus lamivudine versus triple treatment with atazanavir-ritonavir plus two nucleos(t)ides in virologically stable patients with HIV-1 (SALT): 48week results from a randomised, open-label, non-inferiority trial. Lancet Infect. Dis. 2015, 15, 775–784. [Google Scholar] [CrossRef] [PubMed]
- Cahn, P.; Madero, J.S.; Arribas, J.R.; Antinori, A.; Ortiz, R.; Clarke, A.E.; Hung, C.-C.; Rockstroh, J.K.; Girard, P.-M.; Sievers, J.; et al. Dolutegravir plus lamivudine versus dolutegravir plus tenofovir disoproxil fumarate and emtricitabine in antiretroviral-naive adults with HIV-1 infection (GEMINI-1 and GEMINI-2): Week 48 results from two multicentre, double-blind, randomised, non-inferiority, phase 3 trials. Lancet 2019, 393, 143–155. [Google Scholar] [PubMed]
- Rolle, C.P.; Berhe, M.; Singh, T.; Ortiz, R.; Wurapa, A.; Ramgopal, M.; Leone, P.A.; Matthews, J.E.; Dalessandro, M.; Underwood, M.R.; et al. Dolutegravir/lamivudine as a first-line regimen in a test-and-treat setting for newly diagnosed people living with HIV. AIDS 2021, 35, 1957–1965. [Google Scholar] [CrossRef]
- Hidalgo-Tenorio, C.; Pasquau, J.; Vinuesa, D.; Ferra, S.; Terrón, A.; SanJoaquín, I.; Payeras, A.; Martínez, O.J.; López-Ruz, M.Á.; Omar, M.; et al. DOLAVI Real-Life Study of Dolutegravir Plus Lamivudine in Naive HIV-1 Patients (48 Weeks). Viruses 2022, 14, 524. [Google Scholar] [CrossRef] [PubMed]
- van Wyk, J.; Ajana, F.; Bisshop, F.; De Wit, S.; Osiyemi, O.; Portilla Sogorb, J.; Routy, J.-P.; Wyen, C.; Ait-Khaled, M.; Nascimento, M.C.; et al. Efficacy and Safety of Switching to Dolutegravir/Lamivudine Fixed-Dose 2-Drug Regimen vs Continuing a Tenofovir Alafenamide-Based 3- or 4-Drug Regimen for Maintenance of Virologic Suppression in Adults Living With Human Immunodeficiency Virus Type 1: Phase 3, Randomized, Noninferiority TANGO Study. Clin. Infect. Dis. 2020, 71, 1920–1929. [Google Scholar]
- Llibre, J.M.; Brites, C.; Cheng, C.Y.; Osiyemi, O.; Galera, C.; Hocqueloux, L.; Maggiolo, F.; Degen, O.; Taylor, S.; Blair, E.; et al. Efficacy and Safety of Switching to the 2-Drug Regimen Dolutegravir/Lamivudine Versus Continuing a 3- or 4-Drug Regimen for Maintaining Virologic Suppression in Adults Living With HIV-1: Week 48 Results From the Phase 3, Non-inferiority SALSA Randomized Trial. Clin. Infect. Dis. 2022, ciac130. [Google Scholar]
- Hidalgo-Tenorio, C.; Cortés, L.L.; Gutiérrez, A.; Santos, J.; Omar, M.; Gálvez, C.; Sequera, S.; De Jesús, S.E.; Téllez, F.; Fernández, E.; et al. DOLAMA study: Effectiveness, safety and pharmacoeconomic analysis of dual therapy with dolutegravir and lamivudine in virologically suppressed HIV-1 patients. Medicine 2019, 98, e16813. [Google Scholar] [CrossRef]
- Aboud, M.; Orkin, C.; Podzamczer, D.; Bogner, J.R.; Baker, D.; Khuong-Josses, M.A.; Parks, D.; Angelis, K.; Kahl, L.P.; Blair, E.A.; et al. Efficacy and safety of dolutegravir-rilpivirine for maintenance of virological suppression in adults with HIV-1: 100-week data from the randomised, open-label, phase 3 SWORD-1 and SWORD-2 studies. Lancet HIV 2019, 6, e576–e587. [Google Scholar] [CrossRef]
- Maissenhaelter, B.E.; Woolmore, A.L.; Schlag, P.M. Real-world evidence research based on big data: Motivation-challenges-success factors. Onkologe 2018, 24, 91–98. [Google Scholar] [CrossRef] [Green Version]
- Wertz, R.T. Intention to treat: Once randomized, always analyzed. Clin. Aphasiol. 1995, 23, 57–64. [Google Scholar]
- Abraha, I.; Montedori, A. Modified inten- tion to treat reporting in randomised controlled trials: Systematic review. BMJ 2010, 340, c2697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Day, S. Analysis Issues, ITT, Post-Hoc, and Subgroups. Johns Hopkins University. 2008. Available online: http://ocw.jhsph.edu/courses/Biostat-MedicalProductRegulation/biomed_lec7_day.pdf (accessed on 17 September 2022).
- Imaz, A.; Garcia, F.; di Yacovo, S.; Llibre, J.M. Perfil de resistencias a rilpivirina. Enferm. Infecc. Y Microbiol. Clín. 2013, 31, 36–43. [Google Scholar] [CrossRef]
- Mazzitelli, M.; Trunfio, M.; Putaggio, C.; Sasset, L.; Leoni, D.; Lo Menzo, S.; Mengato, D.; Cattelan, A.M. Viro-Immunological, Clinical Outcomes and Costs of Switching to BIC/TAF/FTC in a Cohort of People Living with HIV: A 48-Week Prospective Analysis. Biomedicines 2022, 10, 1823. [Google Scholar] [CrossRef]
- Eron, J.J.; Orkin, C.; Cunningham, D.; Pulido, F.; Post, F.A.; De Wit, S.; Lathouwers, E.; Hufkens, V.; Jezorwski, J.; Petrovic, R.; et al. Week 96 efficacy and safety results of the phase 3, randomized EMERALD trial to evaluate switching from boosted-protease inhibitors plus emtricitabine/tenofovir disoproxil fumarate regimens to the once daily, single- tablet regimen of darunavir/cobicistat/emtricitabine/tenofovir alafenamide (D/C/F/TAF) in treatment-experienced, virologically-suppressed adults living with HIV-1. Antivir. Res. 2019, 170, 104543. [Google Scholar]
- Punekar, Y.S.; Parks, D.; Joshi, M.; Kaur, S.; Evitt, L.; Chounta, V.; Radford, M.; Jha, D.; Ferrante, S.; Sharma, S.; et al. Effectiveness and safety of dolutegravir two-drug regimens in virologically suppressed people living with HIV: A systematic literature review and meta-analysis of real-world evidence. HIV Med. 2021, 22, 423–433. [Google Scholar] [CrossRef]
- Llibre, J.M.; Hung, C.C.; Brinson, C.; Castelli, F.; Girard, P.M.; Kahl, L.P.; Blair, E.A.; Angelis, K.; Wynne, B.; Vandermeulen, K.; et al. Efficacy, safety, and tolerability of dolutegravir-rilpivirine for the maintenance of virological suppression in adults with HIV-1: Phase 3, randomised, non-inferiority SWORD-1 and SWORD-2 studies. Lancet 2018, 391, 839–849. [Google Scholar] [CrossRef]
- Nakagawa, F.; Lodwick, R.K.; Smith, C.J.; Smith, R.; Cambiano, V.; Lundgren, J.D.; Valerie, D.; Phillips, A.N. Projected life expectancy of people with HIV according to timing of diagnosis. AIDS 2012, 26, 335–343. [Google Scholar] [CrossRef] [Green Version]
- Back, D. 2-Drug regimens in HIV treatment: Pharmacological considerations. GERMS 2017, 7, 113–114. [Google Scholar] [CrossRef] [Green Version]
- van Wyk, J.; Orkin, C.; Rubio, R.; Bogner, J.; Baker, D.; Khuong-Josses, M.A. Brief Report: Durable Suppression and Low Rate of Virologic Failure 3 Years After Switch to Dolutegravir + Rilpivirine 2-Drug Regimen: 148-Week Results From the SWORD-1 and SWORD-2 Randomized Clinical Trials. J. Acquir. Immune Defic. Syndr. 2020, 85, 325–330. [Google Scholar] [CrossRef]
- Palacios, R.; Mayorga, M.; González-Domenech, C.M.; Hidalgo-Tenorio, C.; Gálvez, C.; Muñoz-Medina, L.; de la Torre, J.; Lozano, A.; Castaño, M.; Omar, M.; et al. Safety and Efficacy of Dolutegravir plus Rilpivirine in Treatment-Experienced HIV-Infected Patients: The DORIVIR Study. J. Int. Assoc. Provid. AIDS Care 2018, 17, 2325958218760847. [Google Scholar] [CrossRef] [PubMed]
- Capetti, A.F.; Cossu, M.V.; Sterrantino, G.; Barbarini, G.; Di Giambenedetto, S.; De Socio, G.V.; Orofino, G.; Di Biagio, A.; Celesia, B.M.; Rusconi, S.; et al. Dolutegravir Plus Rilpivirine as a Switch Option in cART-Experienced Patients: 96-Week Data. Ann. Pharmacother. 2018, 52, 740–746. [Google Scholar] [CrossRef]
- Troya, J.; Dueñas, C.; Irazola, I.; de Los Santos, I.; de la Fuente, S.; Gil, D.; Hernández, C.; Galindo, M.J.; Gómez, J.; Delgado, E.; et al. Dolutegravir plus rilpivirine: Benefits beyond viral suppression: DORIPEX retrospective study. Medicine 2022, 101, e29252. [Google Scholar] [CrossRef] [PubMed]
- McComsey, G.A.; Lupo, S.; Parks, D.; Poggio, M.C.; De Wet, J.; Kahl, L.P.; Angelis, K.; Wynne, B.; Vandermeulen, K.; Gartland, M.; et al. Switch from tenofovir disoproxil fumarate combination to dolutegravir with rilpivirine improves parameters of bone health. AIDS 2018, 32, 477–485. [Google Scholar] [CrossRef]
- Llibre, J.M.; Cortés LF, L.; Aylott, A.; Wynne, B.; Matthews, J.; Van Solingen-Ristea, R.; Vandermeulen, K.; van Wyk, J.; Kahl, L.P. Brief Report: Evaluation of Inflammation and Atherogenesis Biomarkers Through 148 Weeks Postswitch to Dolutegravir and Rilpivirine in SWORD-1/SWORD-2. J. Acquir. Immune Defic. Syndr. 2022, 91, 73–78. [Google Scholar] [CrossRef]
- Anderson, S.J.; Hsu, C.Y.; Ou, H.T.; Ko, N.Y.; Yang, C.T.; Lopes, S. Cost-Effectiveness of Juluca for Human Immunodeficiency Virus Infection Treatment in Virologically Suppressed Adults in Taiwan. Value Health Reg. Issues 2021, 24, 216–223. [Google Scholar] [CrossRef]


{kind=link}
| Variable | N = 291 |
|---|---|
| Age (years), mean (± SD) | 51.3 (±11.4) |
| Male, n (%) | 226 (77.7) |
| Time from HIV diagnosis (year), median (IQR) | 19.7 (10.6–27) |
| CD4 nadir, mean (± SD) | 283.5 ± 204.6 |
| Baseline VL < 50 copies/mL, n (%), 95% CI | 287 (98.6) (97.1–99.9) |
| Viral load of HIV, log10, median (IQR) | 0 (0–0) |
| Baseline CD4, (cell/uL), mean (± SD) | 785.4 (±355.7) |
| Baseline CD4/CD8 ratio, mean (± SD) | 0.99 (±0.58) |
| History of AIDS (A3, B3, C), n (%), 95% CI | 12 5(42.9) (37.9–49.7) |
| HBs antigen positive, n (%) HB core antibody positive, n (%), 95% CI IgG HCV-positive (cured), n (%), 95% CI History of infectious transmission diseases, n (%) Smoking, n (%), CI 95% | 1 (0.3) 8 (2.7) (1.2–5.4) 67 (23) (18.8–29) 35 (12) 155 (53.3) (44.8–56.7) |
Risk factor for HIV infection, n (%)
| 54 (18.6) 184 (63.2) 48 (16.5) 2 (2.2) |
| Previous ART lines, median (IQR) | 5 (3–7) |
| Time on ART (years), median (IQR) | 15.3 (7.5–22.1) |
| Previous ART regimen, n (%) 3DR INSTI NNRTI PI 2DR INSTI + NNRTI Lamivudine + PI PI + NNRTI 1DR DRV/r or cob LOP/r | 100 (34.4) 53 (53) 20 (20) 27 (27) 91 (31.3) 40 (43.9) 26 (28.6) 25(27.4) 100 (34.4) 98 (98) 2 (2) |
| History of ARV with INSTI, n (%) History of ARV with NNRTI, n (%) | 87 (29.9) 111 (38.1) |
| Time (years) since genotype resistance test, median (IQR) | 13.5 (8.3–17.3) |
| Resistances to a NNRTI by patient | Resistance to RPV Y 181C, V179I Y181C, G190A, M184V M 184v, Y181C, V179I K103N, Y181C, V 106M K103N, V108I, M184I Decreased susceptibility to RPV K103N, G190A, M184V (2 patients) M184V, V106A, V 179D (2 patients) K103N, V108I, Y181C K101/E, G190A Sensible to RPV K103N, E138A K103N, M184V, P225HG106A, M184V |
| Median time (months) of RPV/DTGSTR administration (IQR) | 14 (9.5–21) |
| Reason for change to RPV/DTGSTR, n (%) | |
| Simplification/optimization Avoiding long-term drug toxicity Virological failure due to poor adherence to MTR | 203 (69.8) 78 (26.8) 10 (3.4) |
| Effectiveness | N = 291 |
|---|---|
| Intention-to-treat (ITT) analysis, (%) n/N * Modified ITT (mITT) analysis, (%) n/N ** Per-protocol (PP) analysis, (%) n/N *** | 96.2 (280/291) 97.5 (280/287) 99.3 (281/283) |
| n = 287 | |
| Blips, n (%) | 10 (3.5) |
| Virological failure, n (%) | 2 (0.69) |
| Adverse effects, n (%) | 2 (0.69) |
| PLHIV | Age Years | S | Years Since HIV Diagnosis Stage | ART (Total Time, Previous ART and Time) Previous Lines | Baseline VL | VL in VF | ** RS | Month VF | Observations |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 59 | M | 28.7 and B3 | 27 years in ART DRV/cob (49 months) 8 lines | <50 cop/mL | 173,000 cop/mL | Not available | 3 months | Abandoned ART and follow-up |
| 2 | 57 | F | 33.3 and B2 | 26 years in ART EVG/c/TAF/FTC (27 months) 14 lines | 25,700 cop/mL | 122,200 cop/mL | Not available | 19 months | Null adherence |
| Baseline | Last Visit | p Value | |
|---|---|---|---|
| CD4 (cells/uL), mean ± SD | 785.4 ± 355.7 | 772.7 ± 342.3 | 0.43 |
| CD4/CD8 ratio, mean ± SD | 0.99 ± 0.58 | 1.01 ± 0.54 | 0.013 |
| Creatinine clearance mL/h, mean ± SD | 117.5 ± 458.3 | 122.8 ± 592.3 | 0.001 |
| Total cholesterol (mg/dL), mean ± SD | 190.6 ± 39.4 | 176.8 ± 35.5 | 0.0001 |
| HDL cholesterol (mg/dL), mean ± SD | 52.1 ± 15.4 | 54.2 ± 15.1 | 0.482 |
| LDL cholesterol (mg/dL), mean ± SD | 118.9 ± 32.2 | 106.2 ± 29.8 | 0.0001 |
| TC/HDL ratio, mean ± SD | 3.9 ± 0.9 | 3.6 ± 0.9 | 0.0001 |
| Triglycerides (mg/dL), mean ± SD | 130.9 ± 73.9 | 115.3 ± 68.5 | 0.0001 |
| Bilirubin (mg/dL), mean ± SD | 0.7 ± 0.4 | 0.7 ± 0.3 | |
| GPT (UI/dL), mean ± SD | 26.8 ± 21.9 | 29.5 ± 25.1 | 0.0001 |
| GGT (UI/dL), mean ± SD | 38.9 ± 63.8 | 34.9 ± 56.2 | 0.794 |
| FA (UI/dL), mean ± SD | 77.8 ± 39.6 | 73.4 ± 32.5 | 0.0001 |
| Interleukin-6 (pg/mL), mean ± SD | 3.9 ± 5.8 | 4.1 ± 0.6 | 0.851 |
| D-dimer (UEF/mL), mean ± SD | 0.4 ± 0.4 | 0.4 ± 0.6 | 0.251 |
| Fibrinogen, mg/dL, mean ± SD | 283.9 ± 92.3 | 273.5 ± 116.8 | 0.054 |
| PCR, mg/dL | 3.3 ± 4.2 | 3.1 ± 4.5 | 0.093 |
| (a) Cost Minimization among the Different ARTs | ||||
| ARTs Compared | Differential Cost Per Year | |||
| RPV/DTGSTR vs. BIC/TAF/FTC | EUR −473.40 | |||
| RPV/DTGSTR vs. DRV/c/TAF/FTC | EUR −555.60 | |||
| RPV/DTGSTR vs. DTG/3TC | EUR 687.72 | |||
| (b) Cost-Effectiveness Table | ||||
| ART | Effectiveness | Cost (€/Year) | CER | ICER |
| DTG/3TC | 87.9% | EUR 4851 | 55 | 87 |
| BIC/FTC/TAF | 94.8.0% | EUR 6012 | 63 | −175 |
| DRV/c/FTC/TAF | 90.7% | EUR 6095 | 67 | −82 |
| RPV/DTGSTR | 97.5% | EUR 5539 | 57 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hidalgo-Tenorio, C.; Vinuesa, D.; García-Vallecillos, C.; Muñoz-Medina, L.; Sequera, S.; Javier, R.; López-Ruz, M.Á.; Sadyrbaeva-Dolgova, S.; Pasquau, J. Rildo: Real-World Multicenter Study on the Effectiveness and Safety of Single-Tablet Regimen of Dolutegravir plus Rilpivirine in Treatment-Experienced People Living with HIV. Viruses 2022, 14, 2626. https://doi.org/10.3390/v14122626
Hidalgo-Tenorio C, Vinuesa D, García-Vallecillos C, Muñoz-Medina L, Sequera S, Javier R, López-Ruz MÁ, Sadyrbaeva-Dolgova S, Pasquau J. Rildo: Real-World Multicenter Study on the Effectiveness and Safety of Single-Tablet Regimen of Dolutegravir plus Rilpivirine in Treatment-Experienced People Living with HIV. Viruses. 2022; 14(12):2626. https://doi.org/10.3390/v14122626
Chicago/Turabian StyleHidalgo-Tenorio, Carmen, David Vinuesa, Coral García-Vallecillos, Leopoldo Muñoz-Medina, Sergio Sequera, Rosario Javier, Miguel Ángel López-Ruz, Svetlana Sadyrbaeva-Dolgova, and Juan Pasquau. 2022. "Rildo: Real-World Multicenter Study on the Effectiveness and Safety of Single-Tablet Regimen of Dolutegravir plus Rilpivirine in Treatment-Experienced People Living with HIV" Viruses 14, no. 12: 2626. https://doi.org/10.3390/v14122626
APA StyleHidalgo-Tenorio, C., Vinuesa, D., García-Vallecillos, C., Muñoz-Medina, L., Sequera, S., Javier, R., López-Ruz, M. Á., Sadyrbaeva-Dolgova, S., & Pasquau, J. (2022). Rildo: Real-World Multicenter Study on the Effectiveness and Safety of Single-Tablet Regimen of Dolutegravir plus Rilpivirine in Treatment-Experienced People Living with HIV. Viruses, 14(12), 2626. https://doi.org/10.3390/v14122626