
Kinetics in HBsAg after Stopping Entecavir or Tenofovir in Patients with Virological Relapse but Not Clinical Relapse

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Methods
2.3. Serological and Virological Testing
2.4. HBV Genotyping
2.5. Statistical Analysis
3. Results
3.1. Clinical Features of Patients with Sustained Virological Suppression and Patients with Virological Relapse but No Clinical Relapse
3.2. Clinical Features of Patients with and without Persistent Virological Suppression after Virological Relapse
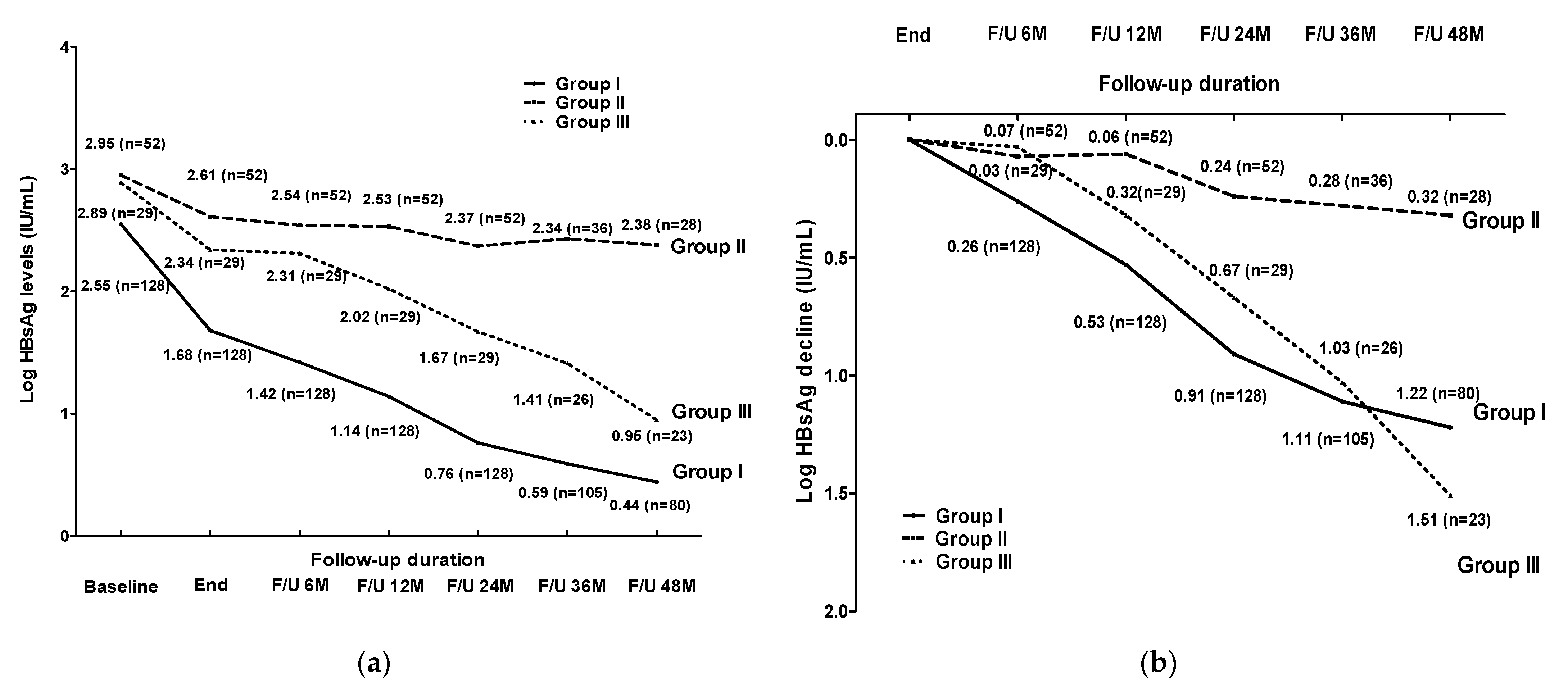
3.3. Comparison of HBsAg Changes between Groups I, II and III
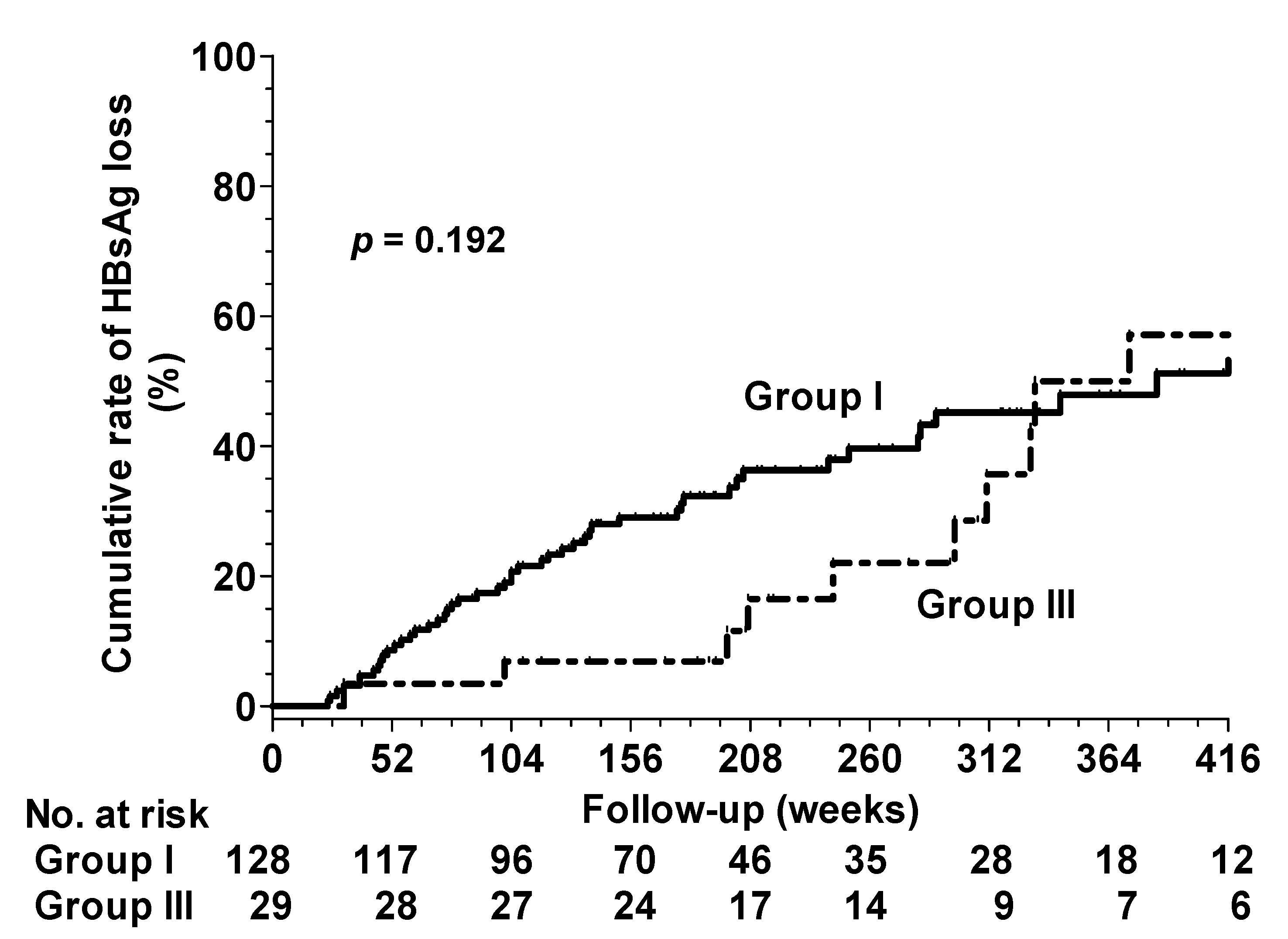
3.4. HBsAg Seroclearance in Groups I and III
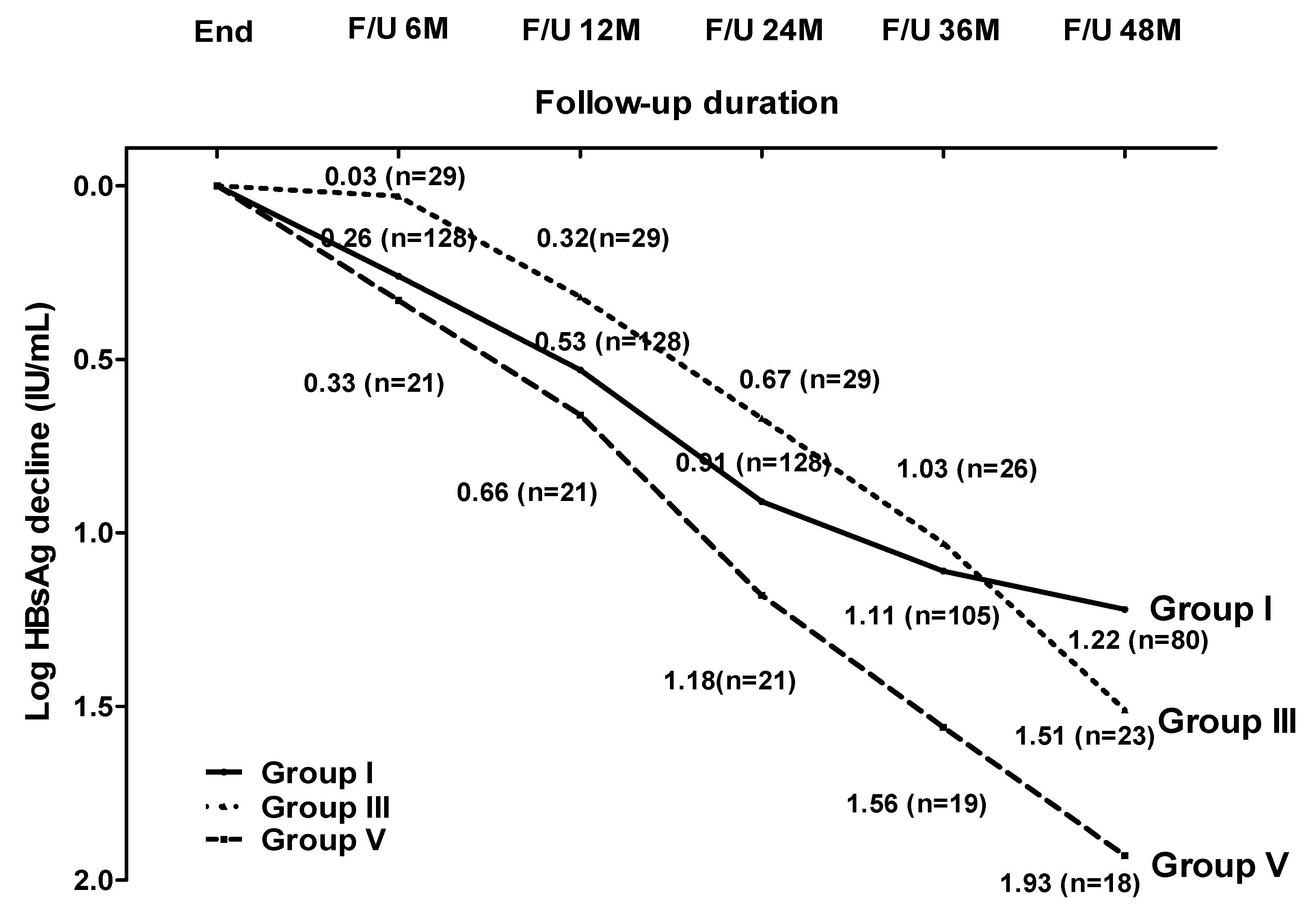
3.5. Clinical Features, HBsAg Decline and HBsAg Loss in Patients with ALT Flare without Retreatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lok, A.S.; McMahon, B.J.; Brown, R.S., Jr.; Wong, J.B.; Ahmed, A.T.; Farah, W.; Almasri, J.; Alahdab, F.; Benkhadra, K.; Mouchli, M.A.; et al. Antiviral therapy for chronic hepatitis B viral infection in adults: A systematic review and meta-analysis. Hepatology 2016, 63, 284–306. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Hu, T.H.; Hung, C.H.; Lu, S.N.; Wang, J.H.; Chang, M.H.; Changchien, C.S.; Lee, C.-M. A comparison of four-year entecavir efficacy in nucleos(t)ide analogue-naïve and -experienced adult Taiwanese chronic hepatitis B patients. Hepatol. Int. 2013, 7, 832–843. [Google Scholar] [CrossRef] [PubMed]
- Jeng, W.-J.; Sheen, I.-S.; Chen, Y.-C.; Hsu, C.-W.; Chien, R.-N.; Chu, C.-M.; Liaw, Y.-F. Off-therapy durability of response to entecavir therapy in hepatitis B e antigen-negative chronic hepatitis B patients. Hepatology 2013, 58, 1888–1896. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-H.; Lu, S.-N.; Hung, C.-H.; Wang, J.-H.; Hu, T.-H.; Changchien, C.-S.; Lee, C.-M. The role of hepatitis B surface antigen quantification in predicting HBsAg loss and HBV relapse after discontinuation of lamivudine treatment. J. Hepatol. 2014, 61, 515–522. [Google Scholar] [CrossRef]
- Chen, C.-H.; Hung, C.-H.; Hu, T.-H.; Wang, J.-H.; Lu, S.-N.; Su, P.-F.; Lee, C.-M. Association Between Level of Hepatitis B Surface Antigen and Relapse after Entecavir Therapy for Chronic Hepatitis B Virus Infection. Clin. Gastroenterol. Hepatol. 2015, 13, 1984–1992.e1. [Google Scholar] [CrossRef]
- Jeng, W.-J.; Chen, Y.-C.; Chien, R.-N.; Sheen, I.-S.; Liaw, Y.-F. Incidence and predictors of hepatitis B surface antigen seroclearance after cessation of nucleos(t)ide analogue therapy in hepatitis B e antigen-negative chronic hepatitis B. Hepatology 2018, 68, 425–434. [Google Scholar] [CrossRef]
- Chen, C.-H.; Hung, C.-H.; Wang, J.-H.; Lu, S.-N.; Lai, H.-C.; Hu, T.-H.; Lin, C.-H.; Peng, C.-Y. The Incidence of Hepatitis B Surface Antigen Loss Between Hepatitis B E Antigen-Negative Noncirrhotic Patients Who Discontinued or Continued Entecavir Therapy. J. Infect. Dis. 2019, 219, 1624–1633. [Google Scholar] [CrossRef]
- Hung, C.H.; Wang, J.H.; Lu, S.N.; Hu, T.H.; Lee, C.M.; Chen, C.H. Hepatitis B surface antigen loss and clinical outcomes between HBeAg-negative cirrhosis patients who discontinued or continued nucleoside analogue therapy. J. Viral Hepat. 2017, 24, 599–607. [Google Scholar] [CrossRef]
- Berg, T.; Simon, K.G.; Mauss, S.; Schott, E.; Heyne, R.; Klass, D.M.; Eisenbach, C.; Welzel, T.M.; Zachoval, R.; Felten, G.; et al. Long-term response after stopping tenofovir disoproxil fumarate in non-cirrhotic HBeAg-negative patients—FINITE study. J. Hepatol. 2017, 67, 918–924. [Google Scholar] [CrossRef]
- Chen, C.-H.; Hung, C.-H.; Wang, J.-H.; Lu, S.-N.; Hu, T.-H.; Lee, C.-M. Long-term incidence and predictors of hepatitis B surface antigen loss after discontinuing nucleoside analogues in noncirrhotic chronic hepatitis B patients. Clin. Microbiol. Infect. 2018, 24, 997–1003. [Google Scholar] [CrossRef] [Green Version]
- Liaw, Y.F.; Kao, J.H.; Piratvisuth, T.; Chan, H.L.; Chien, R.N.; Liu, C.J.; Gane, E.; Locarnini, S.; Lim, S.G.; Han, K.H.; et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: A 2012 update. Hepatol. Int. 2012, 6, 531–561. [Google Scholar] [CrossRef] [PubMed]
- Hung, C.-H.; Lu, S.-N.; Wang, J.-H.; Lee, C.-M.; Chen, T.-M.; Tung, H.-D.; Chen, C.-H.; Huang, W.-S.; Changchien, C.-S. Correlation between ultrasonographic and pathologic diagnoses of hepatitis B and C virus-related cirrhosis. J. Gastroenterol. 2003, 38, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Seto, W.-K.; Wong, D.K.-H.; Fung, J.; Huang, F.-Y.; Liu, K.S.-H.; Lai, C.-L.; Yuen, M.-F. Linearized hepatitis B surface antigen and hepatitis B core-related antigen in the natural history of chronic hepatitis B. Clin. Microbiol. Infect. 2014, 20, 1173–1180. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.-M.; Chen, C.-H.; Lu, S.-N.; Tung, H.-D.; Chou, W.-J.; Wang, J.-H.; Chen, T.-M.; Hung, C.-H.; Huang, C.-C.; Chen, W.-J. Prevalence and Clinical Implications of Hepatitis B Virus Genotypes in Southern Taiwan. Scand. J. Gastroenterol. 2003, 38, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Boni, C.; Laccabue, D.; Lampertico, P.; Giuberti, T.; Viganò, M.; Schivazappa, S.; Alfieri, A.; Pesci, M.; Gaeta, G.B.; Brancaccio, G.; et al. Restored Function of HBV-Specific T Cells after Long-term Effective Therapy With Nucleos(t)ide Analogues. Gastroenterology 2012, 143, 963–973.e9. [Google Scholar] [CrossRef] [PubMed]
- Höner Zu Siederdissen, C.; Rinker, F.; Maasoumy, B.; Wiegand, S.B.; Filmann, N.; Falk, C.S.; Deterding, K.; Port, K.; Mix, C.; Manns, M.P.; et al. Viral and Host Responses after Stopping Long-term Nucleos(t)ide Analogue Therapy in HBeAg-Negative Chronic Hepatitis B. J. Infect. Dis. 2016, 214, 1492–1497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papatheodoridis, G.V.; Rigopoulou, E.I.; Papatheodoridi, M.; Zachou, K.; Xourafas, V.; Gatselis, N.; Hadziyannis, E.; Vlachogiannakos, J.; Manolakopoulos, S.; Dalekos, G.N. DARING-B: Discontinuation of effective entecavir or tenofovir disoproxil fumarate long-term therapy before HBsAg loss in non-cirrhotic HBeAg-negative chronic hepatitis B. Antivir. Ther. 2018, 23, 677–685. [Google Scholar] [CrossRef]
- Hadziyannis, S.J.; Sevastianos, V.; Rapti, I.; Vassilopoulos, D.; Hadziyannis, E. Sustained responses and loss of HBsAg in HBeAg-negative patients with chronic hepatitis B who stop long-term treatment with adefovir. Gastroenterology 2012, 143, 629–636. [Google Scholar] [CrossRef]
- Guidotti, L.G.; Ando, K.; Hobbs, M.V.; Ishikawa, T.; Runkel, L.; Schreiber, R.D.; Chisari, F.V. Cytotoxic T lymphocytes inhibit hepatitis B virus gene expression by a noncytolytic mechanism in transgenic mice. Proc. Natl. Acad. Sci. USA 1994, 91, 3764–3768. [Google Scholar] [CrossRef] [Green Version]
- McClary, H.; Koch, R.; Chisari, F.V.; Guidotti, L.G. Relative Sensitivity of Hepatitis B Virus and Other Hepatotropic Viruses to the Antiviral Effects of Cytokines. J. Virol. 2000, 74, 2255–2264. [Google Scholar] [CrossRef] [Green Version]
- Phillips, S.; Chokshi, S.; Riva, A.; Evans, A.; Williams, R.; Naoumov, N.V. CD8+T Cell Control of Hepatitis B Virus Replication: Direct Comparison between Cytolytic and Noncytolytic Functions. J. Immunol. 2010, 184, 287–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, Y.; Stadler, D.; Lucifora, J.; Reisinger, F.; Webb, D.; Hösel, M.; Michler, T.; Wisskirchen, K.; Cheng, X.; Zhang, K.; et al. Interferon-γ and Tumor Necrosis Factor-α Produced by T Cells Reduce the HBV Persistence Form, cccDNA, without Cytolysis. Gastroenterology 2016, 150, 194–205. [Google Scholar] [CrossRef] [PubMed]
- García-López, M.; Lens, S.; Pallett, L.J.; Testoni, B.; Rodríguez-Tajes, S.; Mariño, Z.; Bartres, C.; García-Pras, E.; Leonel, T.; Perpiñán, E.; et al. Viral and immune factors associated with successful treatment withdrawal in HBeAg-negative chronic hepatitis B patients. J. Hepatol. 2021, 74, 1064–1074. [Google Scholar] [CrossRef] [PubMed]
- Rivino, L.; Le Bert, N.; Gill, U.S.; Kunasegaran, K.; Cheng, Y.; Tan, D.Z.; Becht, E.; Hansi, N.K.; Foster, G.R.; Su, T.-H.; et al. Hepatitis B virus–specific T cells associate with viral control upon nucleos(t)ide-analogue therapy discontinuation. J. Clin. Investig. 2018, 128, 668–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tout, I.; Loureiro, D.; Mansouri, A.; Soumelis, V.; Boyer, N.; Asselah, T. Hepatitis B surface antigen seroclearance: Immune mechanisms, clinical impact, importance for drug development. J. Hepatol. 2020, 73, 409–422. [Google Scholar] [CrossRef]
- Rinker, F.; Zimmer, C.L.; Höner Zu Siederdissen, C.; Manns, M.P.; Kraft, A.R.M.; Wedemeyer, H.; Björkström, N.K.; Cornberg, M. Hepatitis B virus-specific T cell responses after stopping nucleos(t)ide analogue therapy in HBeAg-negative chronic hepatitis B. J. Hepatol. 2018, 69, 584–593. [Google Scholar] [CrossRef]
- Zimmer, C.L.; Rinker, F.; Höner Zu Siederdissen, C.; Manns, M.P.; Wedemeyer, H.; Cornberg, M.; Björkström, N.K. Increased NK Cell Function after Cessation of Long-Term Nucleos(t)ide Analogue Treatment in Chronic Hepatitis B Is Associated with Liver Damage and HBsAg Loss. J. Infect. Dis. 2018, 217, 1656–1666. [Google Scholar] [CrossRef]
- Agarwal, K.; Lok, J.; Carey, I.; Shivkar, Y.; Biermer, M.; Berg, T.; Lonjon-Domanec, I. A case of HBV-induced liver failure in the REEF-2 Phase 2 trial: Implications for finite treatment strategies in HBV ‘cure’. J. Hepatol. 2022, in press. [Google Scholar] [CrossRef]
- Tanaka, E.; Matsumoto, A. Guidelines for avoiding risks resulting from discontinuation of nucleoside/nucleotide analogs in patients with chronic hepatitis B. Hepatol. Res. 2014, 44, 1–8. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable Mean ± SD or N (%) | Patients with Sustained Virological Suppression (n = 128) | Patients with Virological Relapse but No Clinical Relapse (n = 81) | p Value |
|---|---|---|---|
| Age (years) | 50.7 ± 10.7 | 51.0 ± 11.1 | 0.834 |
| Sex (male vs. female) | 104:24 | 62:19 | 0.412 |
| Entecavir:TDF | 76:52 | 61:20 | 0.018 |
| ALT (U/L) | 305.8 ± 422.3 | 257.9 ± 264.8 | 0.361 |
| Total bilirubin (mg/dL) | 2.45 ± 4.46 | 1.58 ± 1.71 | 0.081 |
| NA-naive | 89 (69.5%) | 56 (69.1%) | 0.952 |
| HBV DNA (log IU/mL) | 4.97 ± 1.80 | 5.73 ± 1.31 | 0.001 |
| HBV genotype | - | - | 0.094 |
| B | 84 (65.6%) | 62 (76.5%) | - |
| C | 44 (34.4%) | 19 (23.5%) | - |
| FIB-4 index | 3.35 ± 3.57 | 2.61 ± 2.22 | 0.098 |
| HBsAg at baseline (log10 IU/mL) | 2.54 ± 1.03 | 2.93 ± 0.70 | 0.004 |
| HBsAg at EOT (log10 IU/mL) | 1.67 ± 1.05 | 2.51 ± 0.71 | <0.001 |
| HBcrAg at baseline (log10 IU/mL) | 4.57 ± 1.60 | 4.89 ± 1.60 | 0.175 |
| HBcrAg < 3 at baseline (log10 IU/mL) | 38 (29.6%) | 16 (19.7%) | 0.121 |
| HBcrAg at EOT (log10 U/mL) | 3.30 ± 0.59 | 3.32 ± 0.71 | 0.845 |
| HBcrAg < 3 at EOT (log10 U/mL) | 75 (58.6%) | 45 (55.5%) | 0.739 |
| Treatment duration (weeks) | 169.8 ± 52.6 | 167.3 ± 44.4 | 0.725 |
| Consolidation duration (weeks) | 141.9 ± 55.0 | 137.8 ± 46.0 | 0.581 |
| Variable Mean ± SD or N (%) | Group II (n = 52) | Group III (n = 29) | p Value |
|---|---|---|---|
| Age (years) | 51.6 ± 10.9 | 50.0 ± 11.5 | 0.530 |
| Sex (male vs. female) | 40:12 | 22:7 | 0.914 |
| Entecavir:TDF | 38:14 | 23:6 | 0.533 |
| ALT (U/L) | 240.0 ± 205.3 | 290.0 ± 349.1 | 0.419 |
| Total bilirubin (mg/dL) | 1.79 ± 1.99 | 1.21 ± 0.95 | 0.143 |
| NA-naïve status | 39 (75%) | 17 (58.6%) | 0.126 |
| HBV DNA (log IU/mL) | 5.79 ± 1.24 | 5.61 ± 1.43 | 0.538 |
| HBV genotype | - | - | 0.512 |
| B | 41 (78.8%) | 21 (72.4%) | - |
| C | 11 (21.2%) | 8 (17.6%) | - |
| FIB-4 | 2.62 ± 2.32 | 2.61 ± 2.07 | 0.98 |
| HBsAg at initial treatment (log10 IU/mL) | 2.95 ± 0.64 | 2.89 ± 0.82 | 0.695 |
| HBsAg at EOT (log10 IU/mL) | 2.61 ± 0.64 | 2.34 ± 0.80 | 0.091 |
| HBcrAg at initial treatment (log10 U/mL) | 4.91 ± 1.52 | 4.83 ± 1.75 | 0.833 |
| HBcrAg at EOT (log10 U/mL) | 3.23 ± 0.46 | 3.50 ± 1.01 | 0.125 |
| Treatment duration (weeks) | 162.3 ± 23.2 | 176.3 ± 67.2 | 0.173 |
| Consolidation duration (weeks) | 129.6 ± 27.3 | 142.5 ± 65.8 | 0.061 |
| Time to first VR from EOT (weeks) | 50.2 ± 54.9 | 71.4 ± 82.5 | 0.169 |
| HBV DNA at the first VR (log10 IU/mL) | 4.17 ± 0.59 | 4.13 ± 0.51 | 0.761 |
| HBsAg at the first VR (log10 IU/mL) | 2.52 ± 0.73 | 2.14 ± 0.80 | 0.035 |
| HBsAg decline from EOT to the first VR | 0.10 ± 0.23 | 0.20 ± 0.29 | 0.096 |
| Post-Treatment HBsAg Kinetics | ||||
|---|---|---|---|---|
| HBsAg Kinetics | Beta | Standard Error | 95% CI | p Value |
| Groups | ||||
| I | Ref | |||
| II | 0.336 | 0.084 | 0.171–0.501 | <0.001 |
| III | −0.014 | 0.142 | −0.293–0.264 | 0.92 |
| Time (per month) | −0.023 | 0.002 | −0.026–0.019 | <0.001 |
| Age (per year) | 0.007 | 0.005 | −0.002–0.016 | 0.132 |
| Sex (male vs. female) | 0.006 | 0.099 | −0.188–0.2 | 0.954 |
| TDF vs. entecavir | −0.031 | 0.097 | −0.222–0.159 | 0.746 |
| HBV genotype (C vs. B) | −0.146 | 0.101 | −0.344–0.051 | 0.146 |
| NA-naïve (yes vs. no) | 0.189 | 0.098 | −0.004–0.382 | 0.055 |
| GPT (per U/L) | −0.00018 | 0.00011 | −0.0004–0.00003 | 0.096 |
| HBV DNA (per log IU/mL) | −0.017 | 0.037 | −0.089–0.054 | 0.639 |
| Treatment duration (per week) | −0.004 | 0.003 | −0.009–0.002 | 0.233 |
| Consolidation duration (per week) | 0.001 | 0.003 | −0.004–0.007 | 0.603 |
| HBsAg at initial treatment (per log IU/mL) | −0.076 | 0.058 | −0.189–0.037 | 0.189 |
| HBcrAg at initial treatment (per log U/L) | 0.089 | 0.032 | 0.027–0.151 | 0.005 |
| HBsAg at EOT (per log IU/mL) | 1.15 | 0.054 | 1.045–1.256 | <0.001 |
| HBcrAg at EOT (per log U/L) | 0.084 | 0.051 | −0.016–0.184 | 0.1 |
| Post-Treatment HBsAg Decline | ||||
|---|---|---|---|---|
| HBsAg Decline | Beta | Standard Error | 95% CI | p Value |
| Groups | ||||
| I | Ref | |||
| II | −0.335 | 0.083 | −0.499–0.172 | <0.001 |
| III | 0.021 | 0.143 | −0.259–0.301 | 0.886 |
| Time (per month) | 0.022 | 0.002 | 0.019–0.026 | <0.001 |
| Age (per year) | −0.007 | 0.005 | −0.016–0.002 | 0.138 |
| Sex (male vs. female) | −0.013 | 0.099 | −0.206–0.181 | 0.897 |
| TDF vs. entecavir | 0.028 | 0.097 | −0.162–0.217 | 0.775 |
| HBV genotype (C vs. B) | 0.138 | 0.101 | −0.059–0.336 | 0.17 |
| NA-naïve (yes vs. no) | −0.186 | 0.098 | −0.379–0.007 | 0.058 |
| GPT (per U/L) | 0.00019 | 0.00011 | −0.00003–0.00041 | 0.091 |
| HBV DNA (per log IU/mL) | 0.019 | 0.036 | −0.052–0.091 | 0.597 |
| Treatment duration (per week) | 0.003 | 0.003 | −0.003–0.009 | 0.277 |
| Consolidation duration (per week) | −0.001 | 0.003 | −0.006–0.004 | 0.667 |
| HBsAg at initial treatment (per log IU/mL) | 0.092 | 0.06 | −0.026–0.209 | 0.127 |
| HBcrAg at initial treatment (per log U/L) | −0.093 | 0.032 | −0.156–0.03 | 0.004 |
| HBsAg at EOT (per log IU/mL) | −0.162 | 0.056 | −0.271−0.053 | 0.004 |
| HBcrAg at EOT (per log U/L) | −0.082 | 0.051 | −0.183–0.018 | 0.107 |
| Variable | Comparison | Univariate Analysis HR (95% CI) p Value | Multivariate Analysis HR (95% CI) p Value | ||
|---|---|---|---|---|---|
| Age (years) | Increase per year | 1.015 (0.991–1.039) | 0.217 | - | - |
| Sex | Male vs. female | 1.181 (0.641–2.177) | 0.594 | - | - |
| ALT (U/L) | Increase per U/L | 1.000 (1.000–1.001) | 0.553 | - | - |
| Total bilirubin | Increase per mg/dL | 1.004 (0.938–1.076) | 0.900 | - | - |
| HBV DNA | Increase per log IU/mL | 0.867 (0.754–0.997) | 0.045 | - | - |
| HBV genotype | C vs. B | 0.946 (0.562–1.591) | 0.833 | - | - |
| HBsAg at initial treatment | Increase per log IU/mL | 0.630 (0.488–0813) | <0.001 | - | - |
| HBsAg at EOT | Increase per log IU/mL | 0.393 (0.305–0.506) | <0.001 | 0.390 (0.300–0.508) | <0.001 |
| HBcrAg at initial treatment | Increase per log U/mL | 0.828 (0.724–0.946) | 0.005 | - | - |
| HBcrAg at EOT | Increase per log U/mL | 0.766 (0.589–0.995) | 0.046 | - | - |
| Treatment duration | Increase per week | 1.006 (1.002–1.009) | 0.002 | 1005 (1.001–1.008) | 0.005 |
| Consolidation duration | Increase per week | 1.006 (1.003–1.010) | <0.001 | - | - |
| Subgroups | III vs. I | 0.805 (0.581–1.117) | 0.195 | - | - |
| Antiviral agents | TDF vs. entecavir | 1.448 (0.840–2.496) | 0.183 | - | - |
| Variable Mean ± SD or N (%) | Patients with Sustained Virological Suppression (n = 128) | Patients with Clinical Relapse (n = 60) | p Value |
|---|---|---|---|
| Age (years) | 50.7 ± 10.7 | 49.7 ± 10.1 | 0.564 |
| Sex (male vs. female) | 104:24 | 46:14 | 0.466 |
| Entecavir:TDF | 76:52 | 41:19 | 0.238 |
| ALT (U/L) | 305.8 ± 422.3 | 251.1 ± 365.3 | 0.563 |
| Total bilirubin (mg/dL) | 2.45 ± 4.46 | 2.19 ± 4.47 | 0.673 |
| NA-naive | 89 (69.5%) | 41 (68.3%) | 0.868 |
| HBV DNA (log IU/mL) | 4.97 ± 1.80 | 5.51 ± 1.39 | 0.039 |
| HBV genotype | - | - | 0.003 |
| B | 84 (65.6%) | 52 (86.7%) | - |
| C | 44 (34.4%) | 8 (23.3%) | - |
| HBsAg at baseline (log10 IU/mL) | 2.54 ± 1.03 | 2.83 ± 0.72 | 0.054 |
| HBsAg at EOT (log10 IU/mL) | 1.67 ± 1.05 | 2.58 ± 0.49 | <0.001 |
| HBcrAg at baseline (log10 IU/mL) | 4.57 ± 1.60 | 4.91 ± 1.58 | 0.185 |
| HBcrAg at EOT (log10 U/mL) | 3.30 ± 0.59 | 3.39 ± 0.58 | 0.351 |
| Treatment duration (weeks) | 169.8 ± 52.6 | 165.7 ± 49.0 | 0.613 |
| Consolidation duration (weeks) | 141.9 ± 55.0 | 137.1 ± 47.6 | 0.564 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tseng, T.-N.; Kuo, Y.-H.; Hu, T.-H.; Hung, C.-H.; Wang, J.-H.; Lu, S.-N.; Chen, C.-H. Kinetics in HBsAg after Stopping Entecavir or Tenofovir in Patients with Virological Relapse but Not Clinical Relapse. Viruses 2022, 14, 1189. https://doi.org/10.3390/v14061189
Tseng T-N, Kuo Y-H, Hu T-H, Hung C-H, Wang J-H, Lu S-N, Chen C-H. Kinetics in HBsAg after Stopping Entecavir or Tenofovir in Patients with Virological Relapse but Not Clinical Relapse. Viruses. 2022; 14(6):1189. https://doi.org/10.3390/v14061189
Chicago/Turabian StyleTseng, Tzu-Ning, Yuan-Hung Kuo, Tsung-Hui Hu, Chao-Hung Hung, Jing-Houng Wang, Sheng-Nan Lu, and Chien-Hung Chen. 2022. "Kinetics in HBsAg after Stopping Entecavir or Tenofovir in Patients with Virological Relapse but Not Clinical Relapse" Viruses 14, no. 6: 1189. https://doi.org/10.3390/v14061189
APA StyleTseng, T.-N., Kuo, Y.-H., Hu, T.-H., Hung, C.-H., Wang, J.-H., Lu, S.-N., & Chen, C.-H. (2022). Kinetics in HBsAg after Stopping Entecavir or Tenofovir in Patients with Virological Relapse but Not Clinical Relapse. Viruses, 14(6), 1189. https://doi.org/10.3390/v14061189