1. Introduction
Nucleos(t)ide analogues (NAs) have been used for patients with chronic hepatitis B (CHB). NAs can suppress hepatitis B virus (HBV) replication and reduce hepatic inflammation. However, hepatitis B surface antigen (HBsAg) loss rarely occurs during long-term NA treatment [
1,
2], and the frequency of HBV relapse is high after the discontinuation of NA therapy [
3,
4,
5].
Despite HBV relapse being a frequent occurrence after NA therapy withdrawal, previous researchers have demonstrated that the rate of HBsAg loss significantly increases after the discontinuation of NA therapy [
6,
7,
8,
9]. Recent studies have demonstrated that the rate of HBsAg seroclearance was the highest in sustained responders after NA therapy cessation [
6,
10]. Moreover, patients who did not require retreatment after clinical relapse had a higher rate of HBsAg loss than those who required retreatment [
6,
10]. Our previous study demonstrated that, at 5 years after NA cessation, the cumulative probability of HBsAg seroclearance was 12.8% among 37 patients who experienced virological relapse, but not clinical relapse, following the withdrawal of entecavir treatment [
10]. Therefore, some patients in this group could achieve persistent virological suppression, a subsequent decline in HBsAg levels, or even HBsAg loss after virological relapse, although ALT flares did not occur in these patients. Thus, the investigation of the incidence and predictors of persistent virological suppression in patients with virological relapse but not clinical relapse is merited. Furthermore, it remains unclear whether the decline in the HBsAg levels and HBsAg loss rate for patients with virological relapse but not clinical relapse is similar to that of sustained responders. The aims were to study the incidence and predictors of persistent virological suppression after virological relapse without clinical relapse and compare the change in HBsAg and the HBsAg loss rate between HBeAg-negative patients with persistent virological relapse after virological relapse and patients with a sustained response after the withdrawal of entecavir or tenofovir disoproxil fumarate (TDF) therapy.
4. Discussion
In this study, 128 (25.4%) of the 504 patients achieved persistent virological suppression and 81 (16.1%) experienced virological relapse but not clinical relapse. Our previous study demonstrated that, out of 250 patients who discontinued entecavir, 71 (28.4%) had persistent virological suppression and 35 (15%) developed virological relapse but did not develop clinical relapse or require retreatment [
7]. Another study of 691 patients who discontinued NA therapy showed that 144 (20.8%) did not have virological relapse and 128 (18.5%) had virological relapse but not clinical relapse [
6]. The relapse rates of the two groups in this study are consistent with those of previous studies [
6,
7]. However, the rate of persistent virological suppression after virological relapse in the patients with virological relapse but not clinical relapse has rarely been reported. In this study, 29 (35.8%) of 81 patients achieved persistent virological suppression after virological relapse. These results raise two important points. Firstly, around 35% of patients could achieve persistent virological suppression after HBV flare but not ALT flare. Secondly, how can beneficial virological relapse be differentiated from a detrimental relapse?
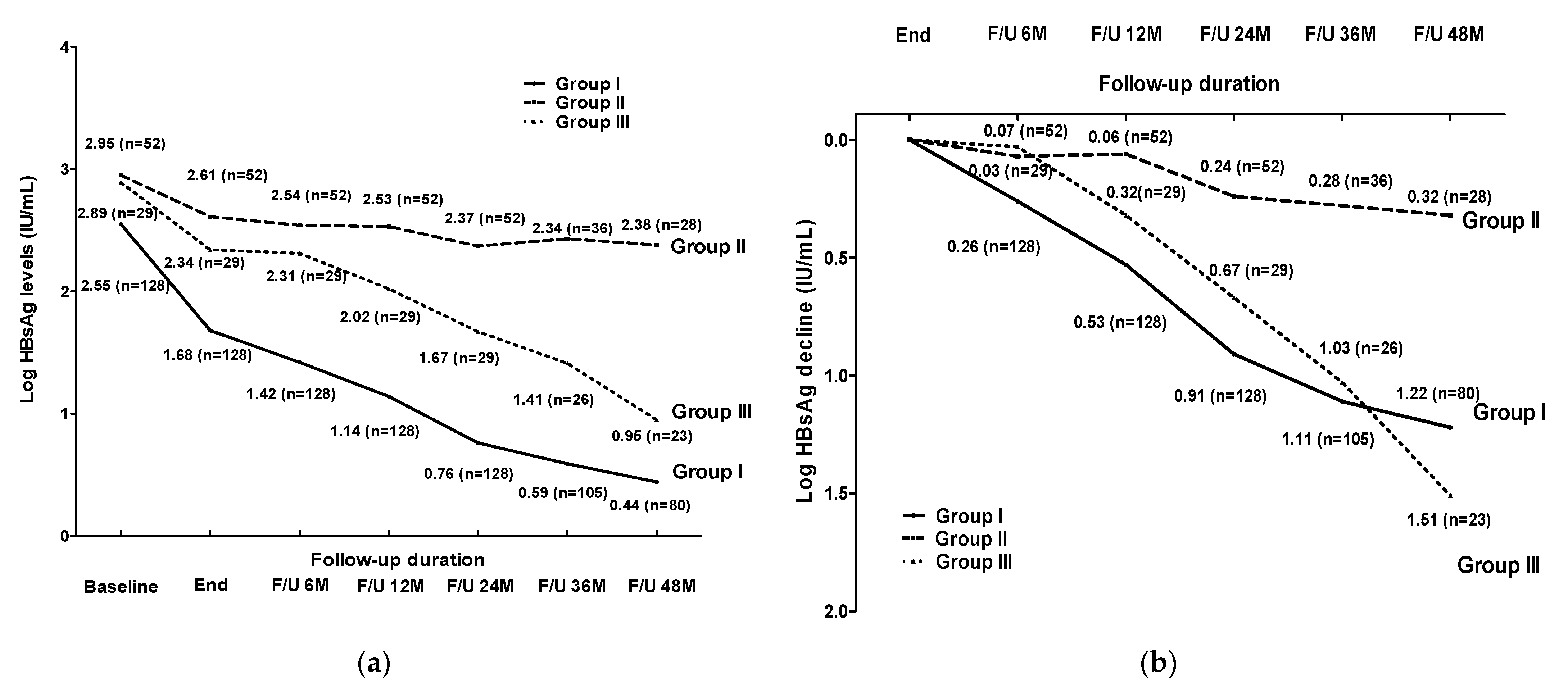
Unfortunately, no factor at the baseline or EOT of entecavir or TDF therapy could significantly predict persistent virological suppression after virological relapse in these patients. During the off-therapy follow-up, the patients who achieved virological suppression (Group III) had lower HBsAg levels at the time of virological relapse than the patients without virological suppression (Group II). However, no optimal HBsAg level at the time of virological relapse would predict persistent virological suppression. Thus, only HBV DNA and HBsAg levels, monitored after virological relapse (without clinical relapse), could distinguish the two groups.
Previous studies showed that the rate of HBsAg seroclearance was the highest in patients with sustained virological suppression after stopping NA therapy [
6,
10]. Previous studies also found that patients who do not require retreatment after clinical relapse develop higher HBsAg loss rates than patients who received retreatment [
6,
10]. However, post-treatment HBsAg changes or declines have rarely been reported in patients who achieve viral suppression after virological relapse without clinical relapse. In this study, patients with persistent viral suppression after virological relapse had similar HBsAg changes and declines compared to those with sustained virological suppression after stopping NA therapy. One previous study demonstrated that the HBV-specific T-cell response in the host may be a recovery after the long-term suppression of HBV by NA therapy [
15]. However, the efficient immune response must be triggered by the re-exposure to the antigens of HBV [
16]. Virological relapse occurs frequently after stopping NA therapy and may induce an immune response against HBV. Thus, patients with an “effective immune response” still exhibit a subsequent decrease in HBsAg levels after an HBV flare without an ALT flare [
17,
18]. HBV clearance by the immune system required cytotoxic CD4+ and CD8+ T lymphocytes to kill infected cells by the virus. Cytotoxic T cells could inhibit HBV by killing infected cells but could also suppress the virus by secreting cytokines, such as IFN-γ and TNF-α, that inhibit HBV replication via a non-cytolytic mechanism [
19,
20,
21,
22]. In this study, among the patients who developed persistent virological suppression after virological relapse without clinical relapse, HBV may be suppressed through noncytolytic immune mechanisms. On the contrary, the HBsAg levels at EOT in Group I were lower than those in Group III. The reduction in the HBsAg levels potentially restored anti-HBV immune responses. Previous studies showed that increased frequencies of functional HBV-specific CD8+ T cells at EOT correlate with sustained viral control off-treatment, with the absence of HBV reactivation [
23,
24]. This means that the host immunity had been modulated during the long period of NA treatment and become more effective to suppress HBV replication in Group I [
18,
25]. This was reasonable to explain why no significant difference was presented in the post-treatment HBsAg changes and declines between Groups I, III and V. The patients who had viremia and ALT levels < 2× ULN represent a “grey zone” for antiviral treatment. We suggest that, instead of immediate retreatment, the ALT, HBV DNA and HBsAg levels should be carefully monitored in patients who experience virological relapse but not clinical relapse after discontinuing NA therapy.
Another important issue is whether the HBsAg loss rate in patients who achieve persistent viral suppression after virological relapse is similar to that of patients who have a sustained virological suppression. Previous studies showed that the T cells are less exhausted and display a higher proliferative capacity after discontinuing NA therapy in patients that subsequently achieve HBsAg loss [
24,
26]. In addition, the augmentation of the natural cytotoxic responses of the NK cells was associated with HBsAg seroclearance after discontinuing NA treatment [
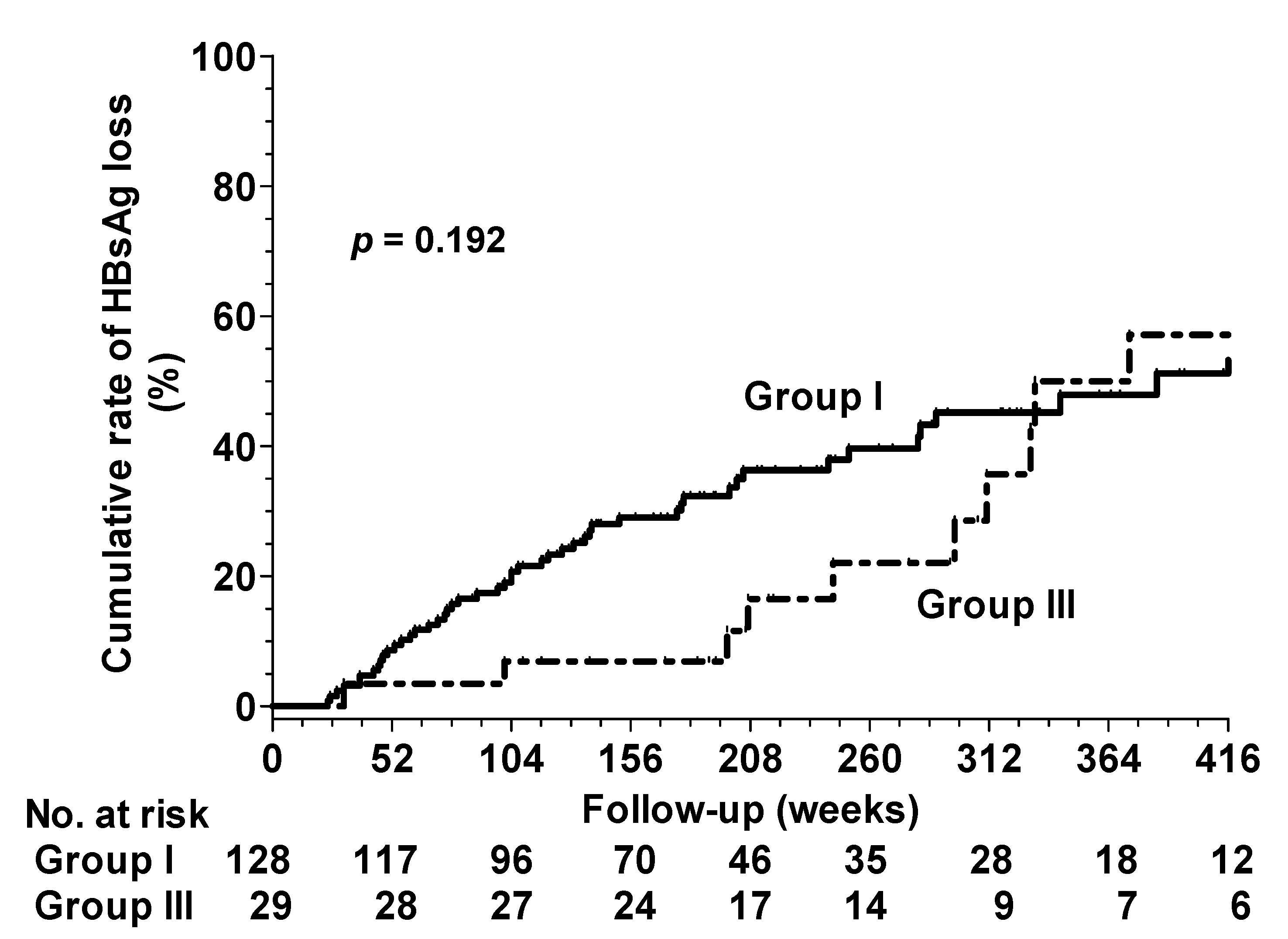
27]. We found no significant differences in the HBsAg loss rates at 8 years between the patients in Groups I and III. The patients in Group III may exhibit a similar T cell immune response to those in Group I after triggering active HBV replication, which accelerates HBsAg decline and loss. However, the duration of HBsAg loss was longer in Group III than in Group I (mean duration: 272.8 ± 135.2 versus 197.7 ± 123.6 weeks,
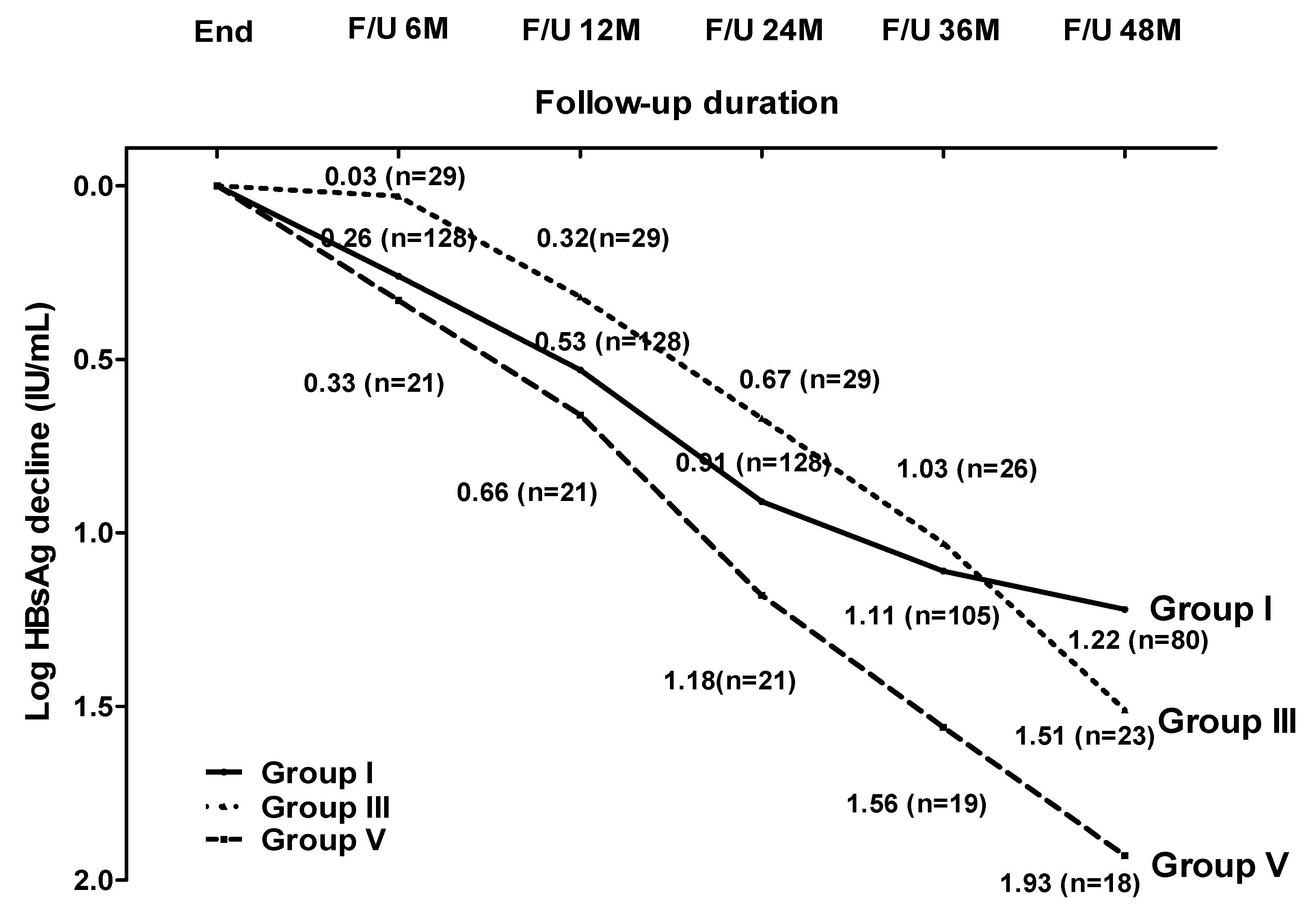
p = 0.004). This may be explained by the higher HBsAg level at EOT in Group III and by the fact that most patients experienced virological relapse within the first 4 years (28/29) after the cessation of entecavir or TDF. After triggering an effective immune response by the HBV flare, the patients in Group III achieved larger HBsAg declines after virological relapse, followed by HBsAg loss. A similar phenomenon was also observed in the patients with persistent virological suppression after clinical relapse (Group V). T-cell activation could benefit in HBsAg decline or loss. However, severe hepatitis due to HBV reactivation—and even hepatic decompensation or mortality—following NA withdrawal has been reported [
8,
28]. Thus, close monitoring after NA withdrawal for timely retreatment is needed to reduce the risks of hepatic decompensation and mortality induced by severe hepatitis.
Comparisons of post-treatment HBsAg kinetics and declines after entecavir or TDF withdrawal have been rarely reported. In our study, there was no significant difference in the post-treatment HBsAg change and decline between the patients who discontinued entecavir and TDF therapy among all subgroup patients.
Tanaka E et al. used HBsAg and HBcrAg levels at EOT to stratify CHB patients into three groups (low-risk, medium-risk and high-risk) in order to predict sustained virological response after the discontinuation of NA [
29]. The rates of sustained virological response at 2 years were 80–90%, 50% and 10–20% in the low-, medium- and high-risk groups, respectively. Therefore, the discontinuation NA can be considered in the low-risk group, and continuous NA treatment is recommended in the high-risk group. In our study, the rates of sustained virological response at 2 years were 80%, 64.8% and 63.5% in the low-, medium- and high-risk groups, respectively, for all 209 patients (Groups I + II + III). In our study, only patients with sustained virological suppression and patients with virological relapse without clinical relapse were included. Thus, the sustained virological response rates were high in the medium- and high-risk groups. Our study found that the sustained virological response rate at 2 years was 80% in the low-risk group, which was consistent with this previous study [
29]. Therefore, further studies are needed to validate the practicality of this risk stratification after NA withdrawal.
There are some limitations. Firstly, this was a retrospective and one-single-center study. Further, multi-center and prospective studies are needed to confirm our findings. Secondly, the number of patients with virological relapse with or without clinical relapse was limited. Thirdly, the population of this study only consisted of Asians, and the HBV genotypes B or C were predominant. It remains unclear whether the same HBsAg decline or HBsAg loss rate would be observed between Groups I, III and V for different ethnicities and HBV genotypes. Fourthly, the follow-up schedule of the serum HBV DNA varied from 1–3 months within the first 12 months following the discontinuation of NA therapy and every 3–6 months thereafter. The patients would have been followed for different visit times, and perhaps the appearance of the virological relapse was transient. This may have led to missed events of HBV relapse and misclassification, particularly in the group without virological relapse.


 ,
, 




{kind=link}
{kind=link}
{kind=link}