Abstract
Objective: CMV coinfection contributes to sustained immune activation in people with chronic HIV. In particular, asymptomatic CMV shedding in semen has been associated with increased local and systemic immune activation, even during suppressive antiretroviral therapy (ART). However, the effect of seminal CMV shedding in people with HIV in the earliest phase of HIV infection is not known. Methods: Using Luminex, we measured the concentration of 34 cytokines in the blood plasma of sixty-nine men who had sex with men with or without HIV and in subgroups of CMV shedders vs. non-shedders. Differences in blood plasma cytokines between groups were investigated using the multivariate supervised partial least squares discriminant analysis method. Results: Independently of CMV, we found that concentrations of IP-10, MIG, MCP-1, I-TAC 10, IL-16, and MIP-1β were modulated in the earliest phase of HIV infection compared with control individuals without HIV. In people with HIV, there was no difference in blood cytokines among CMV shedders vs. non-shedders. Conclusion: In early/acute HIV infection, asymptomatic CMV shedding in semen does not drive additional cytokine changes in blood. Early ART initiation should remain the priority, while the added benefit of CMV suppression during the various stages of HIV infection needs to be further investigated.
1. Introduction
Although antiretroviral therapy (ART) significantly improves the lifespan and general health of people with HIV (PWH), they remain at risk of developing non-AIDS comorbidities, such as end-stage organ disease and age-related diseases (reviewed in [1,2]). Increased morbidity and mortality in PWH are associated with inflammation and immune dysfunction, which persist even despite suppressive ART [3,4]. The reasons for persistent immune activation, a driving force of HIV disease, are likely multifactorial (reviewed in [5]). Besides low-level HIV replication, loss of regulatory cells, and gut damage resulting in bacterial and fungal translocation, CMV coinfection has been proposed as a key player in sustaining immune activation (reviewed in [6]).
CMV is a ubiquitous β-herpesvirus establishing lifelong infection through latency with periodic subclinical reactivation [7]. Although benign in heathy individuals, CMV exacerbates the development of HIV-triggered immunological abnormalities (reviewed in [5,8,9]) in PWH, amongst whom CMV prevalence is about 90% [10].
Despite ART, CMV seropositivity is associated with higher levels of differentiated CD4+ and CD8+ T-cells, leading to accelerated T-cell immunosenescence and ultimately immune exhaustion [11,12,13,14,15]. Strong associations have also been found between CMV IgG antibody levels and soluble markers of immune activation, such as C-reactive protein (CRP), sCD163 tumor necrosis factor–alpha, IL-6, and sCD14 [16,17,18,19,20,21].
PWH are more likely than the general population to have subclinical bursts of CMV replication at mucosal sites and in semen. CMV shedding in semen has been associated with increased local [22] and systemic [11,23,24] immune activation in people with chronic HIV and those suppressed on ART. However, the effect of asymptomatic CMV shedding in semen on immune activation in PWH in early/acute HIV infection has not been reported. If CMV replication were found to alter the cytokine network during early HIV infection, treatment of CMV in addition to ART could prevent subsequent immune disfunction, similar to valacyclovir for herpes simplex virus in chronic HIV [11]. Here, we investigated the effect of seminal CMV shedding (as a proxy of asymptomatic CMV replication) on systemic cytokine production in a cohort of PWH with early/acute infection.
Using the multivariate supervised partial least squares discriminant analysis (PLS-DA) statistical method, we found that early HIV infection is associated with cytokine changes in blood plasma, while the presence of CMV genital shedding is not associated with any systemic changes in cytokines.
2. Methods
2.1. Study Participants
Blood plasma samples from 69 individuals (48 PWH from the San Diego Primary Infection Cohort and 21 without HIV but with similar HIV risk factors from a control cohort) were analyzed for cytokine expression [22,25]. Blood plasma cytokines were analyzed for all 69 individuals. The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of the Human Research Protections Program at the University of California, San Diego (protocol code no.: 191088; approval date release: 8 June 2021). Informed consent was obtained from all subjects involved in the study.
Semen was collected as previously described [26]. Among PWH, 25 had genital CMV shedding and 22 did not. CMV shedding was available only for 47 out 48 PWH. CMV DNA was quantified in semen, following previously published methods [26]. Baseline count values were cell counts at study entry.
Since clinical CD4 and CD8 data were not available for people without HIV, CD4 and CD8 percentages were calculated from a flow cytometry panel on samples taken the same day as the samples analyzed in the cytokine assay.
2.2. Multiplex Bead Array Assay for Cytokine/Chemokine Quantification
- (i)
- The National Institutes of Health laboratory, part of the Microbicide Quality Assurance Program, performed Luminex measurements for 34 cytokines/chemokines involved in different immunological functions (Table S1) [27].
- (ii)
- Mediators of innate immunity, inflammation, and chemotaxis (Interleukin (IL)-1α, IL-1β, IL-6, IL-17, IL-18, IL-21, IL-22, IL-33, Cal, IL-8/CXCL8, MIG/CXCL9, IFN-inducible protein (IP)-10/CXCL10, I-TAC/CXCL11, TNF-α, monocyte chemotactic protein (MCP)-1/CCL2, macrophage inflammatory protein (MIP)-1α/CCL3, MIP-1β/CCL4, regulated on activation, normally T-cell expressed and secreted (RANTES/CCL5), Eotaxin/CCL11, MIP-3α/CCL20, and GRO-α/CXCL1.
- (iii)
- Mediators of hematopoiesis: macrophage colony-stimulating factor (M-CSF) and granulocyte macrophage colony-stimulating factor (GM-CSF)).
- (iv)
- Anti-inflammatory cytokines: IL-10, IL-13, and transforming growth factor (TGF)-β.
- (v)
- Mediators of lymphocytes activation, proliferation, and differentiation: IL-2, IL-4, IL-7, IL-12, IL-15, IL-16, CCL3, CCL4, CCL5, CCL20, and IFN-γ.
- (vi)
- Human CMV IL-10 homolog (cmvIl-10).
Bead coupling was prepared according to the manufacturer’s recommendations. All standards and capture and detection antibodies were purchased from R&D (Minneapolis, MN, USA), except for IL-4 (Biolegend, San Diego, CA, USA), IL-12 (BD Biosciences, Franklin Lakes, NJ, USA), and IL-21 (Thermo Fisher, Waltham, MA, USA).
2.3. Statistical Analysis
Cytokines that were undetectable >70% of the time or more were excluded from the analysis. Undetectable cytokine values were replaced by the minimum of half the lower limit of detection. The limit of detection for each cytokine is provided in the Supplementary Materials. Log-transformed concentrations of cytokines were used for PLS-DA, as previously described [28]. PLS-DA models are particularly suitable when predictors (e.g., cytokines) have more variables than observations (here, HIV serostatus and CMV shedding status). PLS-DA allowed us to visualize the separation in the cytokine profiles between PWH and controls without HIV infection. In the subpopulation of PWH, PLS-DA allowed us to visualize the separation between individuals shedding CMV in their semen and those who did not. In addition, we fit a PLS-DA model, including all 3 groups (people without HIV, CMV shedders, and non-shedders among people with early/acute HIV infection).
The classification performance of the PLS-DA model was assessed with the perf function using 5-fold cross-validation repeated 100 times. From the performance results, a 2-component model was used for the PLS-DA model, as the performance and number of components necessary for the final model dropped off with 3 components or more. The difference in the PLS projections was measured using the E-statistic for a 2-sample difference in the multivariate normal distribution [29]. When PLS projections were different, the difference for each cytokine with variable importance in projection (VIP) >1 was further tested with the Wilcoxon signed-rank test. To correct for multiple comparisons, raw p-values were adjusted using the Benjamini–Hochberg procedure. Analyses were performed using R 4.1 (R core Team, Vienna, Austria) [30], the E-test was performed using the “energy” package [31], and the PLS-DA was performed using the “mixOmics” package [32].
In addition to the multivariate statistical analyses described above, cytokines were compared individually using a Wilcoxon rank-sum test to test for differences in median concentrations between groups analyzed by PLS-DA. In this confirmatory analysis, where each cytokine was analyzed individually, p-values, adjusted using the FDR method, were different to the adjusted p-values obtained in the PLS-DA method due to the larger number of comparisons.
3. Results
3.1. Participants, Samples, and Clinical Laboratory Findings
The cohort characteristics are summarized in Table 1. All 69 individuals included in this study were men originally enrolled in a cohort of individuals at high risk for HIV infection. Out of these 69 individuals, 21 remained seronegative and 48 seroconverted to HIV with a median estimated time of infection of about 12 weeks. There was no age difference between people with and without HIV, but there were significant differences in the mean values for CD4 and CD8 percentages. All PWH were men who had sex with men (MSM) off antiretroviral therapy. Among people without HIV, 81.0% were MSM and 28.6% received pre-exposure prophylaxis. PWH were mostly White (59.6%), Hispanic/Latino (21.3%), or Other/Multiracial (19.1%). No race or ethnicity data was available for people without HIV.

Table 1.
Demographic and clinical information: people with and without HIV.
Among PWH, 53.2% (n = 23) had detectable CMV in their semen, while 22 (46.8%) did not. The characteristics of people shedding CMV in semen or not are summarized in Table 2. Race, ethnicity, age, gender, CD4 T-cell counts, CD8 percentage at cytokine sample date, and HIV RNA levels were not statistically different between CMV shedders and non-shedders. CD4 percentage at cytokine sample date was significantly different between CMV shedders and non-shedders. The median CMV viral load among CMV shedders was 4.73 log10 copies/mL.
Table 2.
Demographic and clinical information: CMV shedders vs. non-shedders.
Thirty-four cytokines/chemokines (see Section 2) were measured in the blood of all 69 individuals. Differences in the concentrations of these markers were reported (i) for PWH in comparison to people living without HIV and (ii) for CMV shedders versus non-shedders among PWH.
3.2. Cytokine Profile in the Blood of People with Early/Acute HIV Is Different from That of Controls without HIV
We used the multivariate supervised PLS-DA statistical method to investigate the differences in blood cytokines between people with and without HIV. PLS-DA, which has demonstrated great success in modelling high-dimensional datasets to predict outcome, works by reducing the number of variables. In our study, the optimal model was obtained with two components or latent variables (LVs), with an error rate of 12% (Figure S1). As a result, our model suggests that blood cytokine values can predict early/acute HIV infection in PWH in comparison to people without HIV with 88% accuracy. Samples projected into the subspace spanned by the two LVs are shown as PLS projections (Figure 1A). LV1 explains 42% of variance in cytokines and 100% in HIV status; LV2 explains 28% of variance in cytokines and 69% in HIV status.
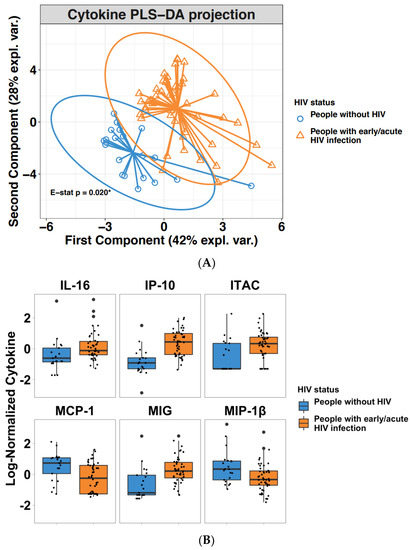
Figure 1.
(A) Two-dimensional PLS projections of blood cytokines in people with and without HIV. Shown are PLS-DA projections in two LVs with ellipses representing Hotelling’s 2-samples T2 with 95% confidence intervals in blood plasma for people with early/acute HIV (orange triangles) or without HIV (blue circles). The E-statistic was used to test the statistical differences in the separation between the cytokine profiles of the two groups. The multivariate distance between people with and without HIV was significant (p = 0.02). (B) Effect of early/acute HIV infection on chemokines/cytokines in blood. The statistical significance of 12 cytokines with VIP > 1 identified in the PLS-DA model were tested by Wilcoxon Rank Sum test. Six out of 12 remained significant. Shown is the difference of the log10-transformed concentrations of the 6 chemokine/cytokines in people with or without HIV and plotted as boxplots. For each cytokine and each boxplot, each point represents a participant’s cytokine concentration, the box represents the interquartile range (IQR), the middle line represents the median, while the points beyond the whiskers are outliers.
PLS projections showed distinct separation between the cytokine profiles in people with HIV versus people without HIV. Confidence ellipses for each class were plotted to highlight the strength of the discrimination (confidence level set to 95%). The separation between the two groups, measured as the energy (E) statistic, was statistically different (E-statistic p = 0.02) (Figure 1A).
In our PLS-DA model, each cytokine was assigned a weight or loading for both LV1 and LV2. These loadings were used to define a VIP score, which reflects the importance of a given cytokine. Cytokines with VIP > 1, which were deemed important to predict acute HIV infection, were IP-10, MCP-1, MIP-1β GM-CSF, MIG, IL-18, I-TAC, IL-17, RANTES, IL-16, eotaxin, and TNFα (in descending order) (Table 3 and Table S2). When subjected to Wilcoxon rank-sum testing, only 6 cytokines remained significant (Table 4). These cytokines were IP-10, MIG, MCP-1, I-TAC 10, IL-16, and MIP-1β (from most to least significant). IP-10, MIG, I-TAC, and IL-16 were upregulated 2.7, 1.34, 1.17, and 1.23 times, respectively, while MCP-1 and MIP-1β were downregulated 2.35 and 1.49 times (Figure 1B). The same cytokines were found to be statistically significant between people with early/acute HIV and people without HIV in an independent individual cytokine analysis (Table S3).
Table 3.
VIP scores for each cytokine: people with and without HIV.
Table 4.
Results from Wilcoxon rank-sum test: people with and without HIV.
3.3. Seminal CMV Shedding Does Not Impact Blood Plasma Cytokines of People Living with HIV during Early Infection
Among PWH, 25 individuals shed seminal CMV, while 22 did not. We next investigated whether blood cytokines were influenced by seminal CMV shedding. Among all documented parameters, only CMV shedding was different (see Table 2). Similar to what was done for the previous analysis in predicting early/acute HIV-infection, the PLS-DA model used here was initially fitted with ten components to evaluate the performance and the number of components necessary for the optimal model. The best model was also obtained with two components or variables, although it was very poor. The error rate using two components was 45%, which is only slightly better than guessing at random (Figure S2). Samples projected into the subspace spanned by the two components are presented in Figure 2. PLS projections showed a large overlap between the cytokine profiles of CMV shedders versus non-shedders. The separation between the two groups was not statistically different (E-statistic p = 0.748) (Figure 2). Furthermore, none of the cytokines with the highest VIP (Table 5 and Table S4) was statistically different between CMV shedders and non-shedders according to Wilcoxon rank-sum testing (Table 6). Similar results were found in an independent individual cytokine analysis (Table S5).
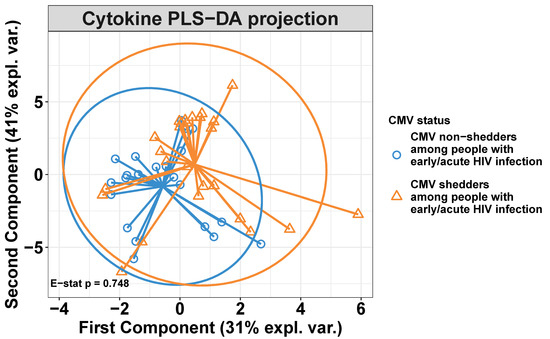
Figure 2.
Two-dimensional PLS projections of blood cytokines in CMV shedders versus non-shedders. Shown are the PLS-DA projections in two LVs with ellipses representing Hotelling’s two-sample T2 with 95% confidence intervals in the blood plasma of people with early/acute HIV who shed CMV (orange triangles) and people who did not shed CMV (blue circles). PLS projections showed a large overlap between the cytokine profiles of CMV shedders versus non-shedders. The separation between the two groups, measured as the energy (E) statistic, was not statistically different (E-statistic p = 0.748).
Table 5.
VIP scores for each cytokine: CMV shedders versus non-shedders.
Table 6.
Results from Wilcoxon rank-sum test: CMV shedders versus non-shedders.
In an attempt to compare each of the two PWH groups separately with the control group of people without HIV, we performed a new PLS-DA analysis based on a three-group model (people without HIV and CMV shedders or non-shedders among PWH). PLS projections showed distinct separation between the cytokine profiles of people without HIV and people with early/acute HIV whether they shed CMV or not. Moreover, there was no separation between CMV shedders and non-shedders in PWH (Figures S3 and S4). Furthermore, cytokines with VIP > 1 in the three-group analysis were similar to the ones obtained in the PLS-DA analysis of people with and without HIV (Table S6).
4. Discussion
CMV, a common β-herpesvirus, is one of the largest and most immunogenic viruses that infects humans. Despite its inflammatory potential, it rarely causes inflammatory conditions in immunocompetent individuals. In PWH however, CMV coinfection has been linked to non-AIDS comorbidities, such as cardiovascular disease, neurocognitive complications, cancer, fragility, and immunological aging (reviewed in [5,33,34]). The reason behind these adverse health outcomes is partly due to chronic activation as a result of CMV infection itself and the magnitude of the host’s immune response against CMV. Indeed, in PWH, CMV becomes the target of a large proportion of circulating T-cells, which skews the immune system toward a CMV-specific response, thus maintaining systemic immune activation/inflammation [35,36]. In PWH, despite suppressive ART, CMV has been associated with T-cell immunosenescence and immune exhaustion [11,18,23,24,37,38,39,40], slower decay of HIV DNA [41], and lower overall survival [20,42]. Furthermore, in PWH on ART, higher anti-CMV IgG antibody levels are associated with higher plasma levels of markers of gut damage translocation [40], and proinflammatory cytokines [16,17,18,19,20,21], including sCD14, a marker of monocyte activation. Although the associations between CMV replication and systemic inflammation in PWH during suppressive ART have been well documented, it not clear whether CMV replication is associated with systemic immune activation during the earliest phase of untreated HIV infection and therefore a potential target for early CMV intervention. Here, we investigated whether genital CMV shedding contributed to systemic immune activation, as evaluated by the concentration of 34 blood cytokines in PWH in the early/acute phase of HIV infection. We used PLS-DA, a supervised principal component-type analysis that is well adapted to datasets comprising a large number of variables (cytokines) [28,43].
First, we looked at the modulations of blood plasma cytokines associated with early/acute HIV infection independent of CMV. Our findings that plasma concentrations of IP-10, MIG, MCP-1, I-TAC, IL-16, and MIP-1β were modulated in early/acute HIV infection compared with people living without HIV are in agreement with previous reports [25,44,45]. Interestingly, IP-10, MIG, and I-TAC, which were upregulated here in early/acute phase, were the cytokines that were most downregulated in a study on the effect of early ART in PWH [43]. This particular finding for IP-10, MIG, and I-TAC was not surprising, as these three cytokines are all involved in Th1 trafficking in response to HIV infection via their receptor CXCR3.
In our cohort of people with early/acute HIV-infection, 53% of individuals shed CMV in semen, while 47% did not. Seminal CMV shedding is associated with higher seminal HIV levels in semen [26,46,47,48,49,50], contributing to higher risk of transmission [51,52]. However, little is known about the role of genital CMV shedding on systemic immune activation in PWH in early/acute phase. In particular, the effect of frequent asymptomatic CMV episodic bursts in semen on blood cytokines has not been addressed. Using PLS-DA, we found that PLS projections of blood cytokines in CMV shedders versus non-shedders strongly overlapped, suggesting that CMV replication in semen does not alter blood cytokines during early/acute HIV infection.
Although PLS-DA is considered particularly suitable for datasets with a large number of variables, such as cytokines, as used in our study, as an additional confirmatory analysis we compared all cytokines individually using a Wilcoxon rank-sum test in (i) people with early/acute HIV compared to people without HIV and (ii) in CMV shedders versus non-shedders among PWH. We found that the cytokines statistically different in the individual cytokine analysis were similar to the ones reported to be statistically different in our combined analysis of people with early/acute HIV compared to people without HIV (Table S5). Similarly, both PLS-DA and individual cytokine analysis showed that no cytokines were statically different between CMV shedders and non-shedders among PWH (Table S6). Altogether, these data validated our approach and our choice to apply PLS-DA to our dataset.
Positive correlations between the presence of CMV and soluble markers of inflammation and immune activation in blood have been previously reported in six studies [16,17,18,19,20,21]. However, all the studies correlated the markers of inflammation with CMV IgG antibody levels. Our study focused on CMV shedding and not IgG levels, as caution has been urged when considering CMV IgG antibodies as surrogate markers of active CMV replication [23,53]. For example, CMV replicates intermittently and may not have been “captured” in cross-sectional studies using CMV IgG. In fact, one of the studies reported on the association between CMV IgG and concentrations of sCD14 in blood although replicating CMV was not found [17]. CMV IgG levels or actual CMV replication aside, the differences in results between the six previous studies and our study may simply be related to the stage of HIV disease. While we investigated the effect of CMV shedding on systemic cytokines in early/acute HIV, all the other studies were performed in virologically suppressed or ART long-term PWH.
Our results suggest that CMV shedding in the male genital tract is not the main driver of systemic immune activation in the early phase of HIV infection. This contrasts with the later phase of HIV infection, in which CMV contributes to immune activation even when HIV replication is controlled on ART. Indeed, we and others have shown that asymptomatic shedding of CMV in the male genital tract is associated with increased systemic T-cell immune activation and proliferation and with higher levels of HIV DNA in peripheral CD4 T-cells [22,23,24].
We acknowledge certain limitations to our study. First, this is a cross-sectional study involving a single time point, which may not be fully reflective of CMV DNA and cytokine changes over time. Second, we did not have information on seminal cytokines and possible correlations with seminal shedding. Third, our study cohort was entirely composed of men. Our findings may not be relevant to women in whom frequent bursts of asymptomatic CMV reactivation have also been documented [54,55,56,57]. We acknowledge the evidence that the immune response to CMV may differ by sex [34]. For example, unlike what has been previously described for men, the presence of CMV DNA was not associated with increased HIV DNA in women [58]. Fourth, due to the limited sample size, the comparison between CMV shedders and non-shedders could be underpowered, thus limiting the statistical significance of the results. Finally, since absolute CD4 and CD8 T-cell counts were only available for PWH but not for controls, we provided CD4 and CD8 as percentages of total lymphocytes for all individuals for comparison.
Despite these limitations, to our knowledge, this is the first study on the effect of active CMV replication in semen on systemic cytokines in early/acute HIV infection. Our study may be one piece in the puzzle aiming at deciphering the exact role of CMV in contributing to persistent immune activation in PWH. Our results suggest that HIV rather than CMV replication in the male genital tract drives immune activation in the early phase of HIV infection. Thus, starting ART in early/acute HIV infection remains a priority to limit immune activation [59,60].
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/v14081833/s1, Figure S1: Classification error for people with early/acute HIV or people without HIV in PLSDA model estimated using k-fold CV; Figure S2: Classification error for CMV shedders versus CMV non-shedders in PLSDA model estimated using k-fold CV; Figure S3: Two-dimensional PLS projections of blood cytokines in people without HIV and in CMV shedders versus non-shedders among people with early/acute HIV; Figure S4: The statistical significance of 12 cytokines with VIP > 1 identified in the PLS-DA model (comparing people with early/acute HIV versus people without HIV) were tested by Wilcoxon Rank Sum test. Table S1: Lower limits of detection for each Cytokine included in the assay and percentage of participants with undetectable values for each cytokine split the respective analysis; Table S2: Median (range) of log-transformed and normalized concentrations of cytokine with VIP > 1 in people with early HIV infection and people without HIV; Table S3: Median (range) for each log-normalized cytokine in people with early/acute HIV and people without HIV. Cytokines were individually tested using Wilcoxon rank-sum test to compare groups; Table S4: Median (range) of log-transformed and normalized concentrations of cytokine with VIP > 1 in CMV shedders versus non-shedders; Table S5: Median (range) for each log-normalized cytokine in CMV shedders vs non-shedders among people with early/acute HIV. Cytokines were individually tested using Wilcoxon rank-sum test to compare groups; Table S6: VIP scores for each cytokine in a PLS-DA 3-group model: people without HIV and CMV shedders versus non shedders among people with early/acute HIV.
Author Contributions
Conceptualization: C.V., A.W., J.M.D., L.M. and S.G.; data curation, A.W., S.A.R. and S.L.; formal analysis: C.V., A.W., J.M.D., W.F. and S.G.; funding acquisition: L.M. and S.G.; methodology: C.V., A.W., S.A.R., S.L., L.M. and S.G.; supervision: L.M. and S.G.; validation: W.F.; writing—original draft preparation, C.V.; writing—review and editing, C.V., A.W., J.M.D., S.A.R., S.L., W.F., L.M. and S.G. All authors have read and agreed to the published version of the manuscript.
Funding
This publication was supported by grants AI147821, AI106039, DA051915, AI158293, AI106039, and MH100974, as well as the James B. Pendleton Charitable Trust and the San Diego Center for AIDS Research (SD CFAR P30 AI036214).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of the Human Research Protections Program at the University of California, San Diego (protocol code no.: 191088; approval date release: 08/06/2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data available upon request.
Acknowledgments
We are grateful to all the study participants and all the nurses at all the enrollment sites.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| HIV | Human Immunodeficiency Virus |
| CMV | Cytomegalovirus |
| PLS-DA | Partial least squares-discriminant analysis |
| MSM | Men who have sex with men |
References
- Deeks, S.G.; Phillips, A.N. HIV infection, antiretroviral treatment, ageing, and non-AIDS related morbidity. BMJ 2009, 338, a3172. [Google Scholar] [CrossRef] [PubMed]
- Hunt, P.W. HIV and inflammation: Mechanisms and consequences. Curr. HIV/AIDS Rep. 2012, 9, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Deeks, S.G.; Verdin, E.; McCune, J.M. Immunosenescence and HIV. Curr. Opin. Immunol. 2012, 24, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Lederman, M.M.; Funderburg, N.T.; Sekaly, R.P.; Klatt, N.R.; Hunt, P.W. Residual immune dysregulation syndrome in treated HIV infection. Adv. Immunol. 2013, 119, 51–83. [Google Scholar]
- Freeman, M.L.; Lederman, M.M.; Gianella, S. Partners in Crime: The Role of CMV in Immune Dysregulation and Clinical Outcome During HIV Infection. Curr. HIV/AIDS Rep. 2016, 13, 10–19. [Google Scholar] [CrossRef]
- Deeks, S.G.; Lewin, S.R.; Havlir, D.V. The end of AIDS: HIV infection as a chronic disease. Lancet 2013, 382, 1525–1533. [Google Scholar] [CrossRef]
- Britt, W. Manifestations of human cytomegalovirus infection: Proposed mechanisms of acute and chronic disease. Curr. Top. Microbiol. Immunol. 2008, 325, 417–470. [Google Scholar]
- Gianella, S.; Massanella, M.; Wertheim, J.O.; Smith, D.M. The Sordid Affair Between Human Herpesvirus and HIV. J. Infect. Dis. 2015, 212, 845–852. [Google Scholar] [CrossRef]
- Christensen-Quick, A.; Vanpouille, C.; Lisco, A.; Gianella, S. Cytomegalovirus and HIV Persistence: Pouring Gas on the Fire. AIDS Res. Hum. Retrovir. 2017, 33, S23–S30. [Google Scholar] [CrossRef]
- Robain, M.; Carre, N.; Dussaix, E.; Salmon-Ceron, D.; Meyer, L.; SEROCO Study Group. Incidence and sexual risk factors of cytomegalovirus seroconversion in HIV-infected subjects. Sex. Transm. Dis. 1998, 25, 476–480. [Google Scholar] [CrossRef]
- Hunt, P.W.; Martin, J.N.; Sinclair, E.; Epling, L.; Teague, J.; Jacobson, M.A.; Tracy, R.P.; Corey, L.; Deeks, S.G. Valganciclovir reduces T cell activation in HIV-infected individuals with incomplete CD4+ T cell recovery on antiretroviral therapy. J. Infect. Dis. 2011, 203, 1474–1483. [Google Scholar] [CrossRef] [PubMed]
- Wittkop, L.; Bitard, J.; Lazaro, E.; Neau, D.; Bonnet, F.; Mercie, P.; Dupon, M.; Hessamfar, M.; Ventura, M.; Malvy, D.; et al. Effect of cytomegalovirus-induced immune response, self antigen-induced immune response, and microbial translocation on chronic immune activation in successfully treated HIV type 1-infected patients: The ANRS CO3 Aquitaine Cohort. J. Infect. Dis. 2013, 207, 622–627. [Google Scholar] [CrossRef] [PubMed]
- Caby, F.; Guihot, A.; Lambert-Niclot, S.; Guiguet, M.; Boutolleau, D.; Agher, R.; Valantin, M.A.; Tubiana, R.; Calvez, V.; Marcelin, A.G.; et al. Determinants of a Low CD4/CD8 Ratio in HIV-1-Infected Individuals Despite Long-term Viral Suppression. Clin. Infect. Dis. 2016, 62, 1297–1303. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.M.; Nakazawa, M.; Freeman, M.L.; Anderson, C.M.; Oliveira, M.F.; Little, S.J.; Gianella, S. Asymptomatic CMV Replication During Early Human Immunodeficiency Virus (HIV) Infection Is Associated With Lower CD4/CD8 Ratio During HIV Treatment. Clin. Infect. Dis. 2016, 63, 1517–1524. [Google Scholar] [CrossRef] [PubMed]
- Picat, M.Q.; Pellegrin, I.; Bitard, J.; Wittkop, L.; Proust-Lima, C.; Liquet, B.; Moreau, J.F.; Bonnet, F.; Blanco, P.; Thiébaut, R.; et al. Integrative Analysis of Immunological Data to Explore Chronic Immune T-Cell Activation in Successfully Treated HIV Patients. PLoS ONE 2017, 12, e0169164. [Google Scholar] [CrossRef]
- Burdo, T.H.; Lo, J.; Abbara, S.; Wei, J.; DeLelys, M.E.; Preffer, F.; Rosenberg, E.S.; Williams, K.C.; Grinspoon, S. Soluble CD163, a novel marker of activated macrophages, is elevated and associated with noncalcified coronary plaque in HIV-infected patients. J. Infect. Dis. 2011, 204, 1227–1236. [Google Scholar] [CrossRef]
- Hodowanec, A.; Williams, B.; Hanson, B.; Livak, B.; Keating, S.; Lurain, N.; Adeyemi, O.M. Soluble CD163 But Not Soluble CD14 Is Associated With Cytomegalovirus Immunoglobulin G Antibody Levels in Virologically Suppressed HIV+ Individuals. J. Acquir. Immune. Defic. Syndr. 2015, 70, e171–e174. [Google Scholar] [CrossRef]
- Freeman, M.L.; Mudd, J.C.; Shive, C.L.; Younes, S.A.; Panigrahi, S.; Sieg, S.F.; Lee, S.A.; Hunt, P.W.; Calabrese, L.H.; Gianella, S.; et al. CD8 T-Cell Expansion and Inflammation Linked to CMV Coinfection in ART-treated HIV Infection. Clin. Infect. Dis. 2016, 62, 392–396. [Google Scholar] [CrossRef]
- Lurain, N.S.; Hanson, B.A.; Hotton, A.L.; Weber, K.M.; Cohen, M.H.; Landay, A.L. The Association of Human Cytomegalovirus with Biomarkers of Inflammation and Immune Activation in HIV-1-Infected Women. AIDS Res. Hum. Retrovir. 2016, 32, 134–143. [Google Scholar] [CrossRef]
- Patel, E.U.; Gianella, S.; Newell, K.; Tobian, A.A.; Kirkpatrick, A.R.; Nalugoda, F.; Grabowski, M.K.; Gray, R.H.; Serwadda, D.; Quinn, T.C.; et al. Elevated cytomegalovirus IgG antibody levels are associated with HIV-1 disease progression and immune activation. AIDS 2017, 31, 807–813. [Google Scholar] [CrossRef]
- Vita, S.; Lichtner, M.; Marchetti, G.; Mascia, C.; Merlini, E.; Cicconi, P.; Vullo, V.; Viale, P.; Costantini, A.; Monforte, A.D.; et al. Brief Report: Soluble CD163 in CMV-Infected and CMV-Uninfected Subjects on Virologically Suppressive Antiretroviral Therapy in the ICONA Cohort. JAIDS J. Acquir. Immune Defic. Syndr. 2017, 74, 347–352. [Google Scholar] [CrossRef]
- Gianella, S.; Strain, M.C.; Rought, S.E.; Vargas, M.V.; Little, S.J.; Richman, D.D.; Spina, C.A.; Smith, D.M. Associations between Virologic and Immunologic Dynamics in Blood and in the Male Genital Tract. J. Virol. 2012, 86, 1307–1315. [Google Scholar] [CrossRef] [PubMed]
- Gianella, S.; Massanella, M.; Richman, D.D.; Little, S.J.; Spina, C.A.; Vargas, M.V.; Lada, S.M.; Daar, E.S.; Dube, M.P.; Haubrich, R.H.; et al. Cytomegalovirus Replication in Semen Is Associated with Higher Levels of Proviral HIV DNA and CD4 + T Cell Activation during Antiretroviral Treatment. J. Virol. 2014, 88, 7818–7827. [Google Scholar] [CrossRef] [PubMed]
- Dan, J.M.; Massanella, M.; Smith, D.M.; Spina, C.A.; Schrier, R.; Daar, E.S.; Dube, M.P.; Morris, S.R.; Gianella, S. Brief Report: Effect of CMV and HIV Transcription on CD57 and PD-1 T-Cell Expression During Suppressive ART. J. Acquir. Immune. Defic. Syndr. 2016, 72, 133–137. [Google Scholar] [CrossRef]
- Vanpouille, C.; Introini, A.; Morris, S.R.; Margolis, L.; Daar, E.S.; Dube, M.P.; Little, S.J.; Smith, D.; Lisco, A.; Gianella, S. Distinct cytokine/chemokine network in semen and blood characterize different stages of HIV infection. AIDS 2016, 30, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Gianella, S.; Mehta, S.R.; Strain, M.C.; Young, J.A.; Vargas, M.V.; Little, S.J.; Richman, D.D.; Pond, S.L.K.; Smith, D.M. Impact of seminal cytomegalovirus replication on HIV-1 dynamics between blood and semen. J. Med. Virol. 2012, 84, 1703–1709. [Google Scholar] [CrossRef]
- Fichorova, R.N.; Richardson-Harman, N.; Alfano, M.; Belec, L.; Carbonneil, C.; Chen, S.; Cosentino, L.; Curtis, K.; Dezzutti, C.S.; Donoval, B.; et al. Biological and Technical Variables Affecting Immunoassay Recovery of Cytokines from Human Serum and Simulated Vaginal Fluid: A Multicenter Study. Anal. Chem. 2008, 80, 4741–4751. [Google Scholar] [CrossRef]
- Vanpouille, C.; Frick, A.; Rawlings, S.; Hoenigl, M.; Lisco, A.; Margolis, L.; Gianella, S. Cytokine Network and Sexual Human Immunodeficiency Virus Transmission in Men Who Have Sex With Men. Clin. Infect. Dis. 2019, 71, 2655–2662. [Google Scholar] [CrossRef]
- Székely, G.J.; Rizzo, M.L. Energy statistics: A class of statistics based on distances. J. Stat. Plan. Inference 2013, 143, 1249–1272. [Google Scholar] [CrossRef]
- Mair, P.; Hofmann, E.; Gruber, K.; Hatzinger, R.; Zeileis, A.; Hornik, K. Motivation, values, and work design as drivers of participation in the R open source project for statistical computing. Proc. Natl. Acad. Sci. USA 2015, 112, 14788–14792. [Google Scholar] [CrossRef]
- Rizzo, M.L.; Székely, G.J. E-Statistics: Multivariate Inference via the Energy of Data. 2021. Available online: https://github.com/mariarizzo/energy (accessed on 25 May 2022).
- Le Cao, K.A.; Costello, M.E.; Lakis, V.A.; Bartolo, F.; Chua, X.Y.; Brazeilles, R.; Rondeau, P. MixMC: A Multivariate Statistical Framework to Gain Insight into Microbial Communities. PLoS ONE 2016, 11, e0160169. [Google Scholar] [CrossRef] [PubMed]
- Gianella, S.; Letendre, S. Cytomegalovirus and HIV: A Dangerous Pas de Deux. J. Infect. Dis. 2016, 214, S67–S74. [Google Scholar] [CrossRef] [PubMed]
- Leng, S.X.; Margolick, J.B. Aging, sex, inflammation, frailty, and CMV and HIV infections. Cell. Immunol. 2019, 348, 104024. [Google Scholar] [CrossRef]
- Ouyang, Q.; Wagner, W.M.; Zheng, W.; Wikby, A.; Remarque, E.J.; Pawelec, G. Dysfunctional CMV-specific CD8+ T cells accumulate in the elderly. Exp. Gerontol. 2004, 39, 607–613. [Google Scholar] [CrossRef]
- Sylwester, A.W.; Mitchell, B.L.; Edgar, J.B.; Taormina, C.; Pelte, C.; Ruchti, F.; Sleath, P.R.; Grabstein, K.H.; Hosken, N.A.; Kern, F.; et al. Broadly targeted human cytomegalovirus-specific CD4+ and CD8+ T cells dominate the memory compartments of exposed subjects. J. Exp. Med. 2005, 202, 673–685. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Villar, S.; Sainz, T.; Lee, S.A.; Hunt, P.W.; Sinclair, E.; Shacklett, B.L.; Ferre, A.L.; Hayes, T.L.; Somsouk, M.; Hsue, P.Y.; et al. HIV-infected individuals with low CD4/CD8 ratio despite effective antiretroviral therapy exhibit altered T cell subsets, heightened CD8+ T cell activation, and increased risk of non-AIDS morbidity and mortality. PLoS Pathog. 2014, 10, e1004078. [Google Scholar] [CrossRef]
- Cao, W.; Mehraj, V.; E Kaufmann, D.; Li, T.; Routy, J.-P. Elevation and persistence of CD8 T-cells in HIV infection: The Achilles heel in the ART era. J. Int. AIDS Soc. 2016, 19, 20697. [Google Scholar] [CrossRef]
- Christensen-Quick, A.; Massanella, M.; Frick, A.; Rawlings, S.; Spina, C.; Vargas-Meneses, M.; Schrier, R.; Nakazawa, M.; Anderson, C.; Gianella, S. Subclinical Cytomegalovirus DNA Is Associated with CD4 T Cell Activation and Impaired CD8 T Cell CD107a Expression in People Living with HIV despite Early Antiretroviral Therapy. J. Virol. 2019, 93, e00179-19. [Google Scholar] [CrossRef]
- Ramendra, R.; Isnard, S.; Lin, J.; Fombuena, B.; Ouyang, J.; Mehraj, V.; Zhang, Y.; Finkelman, M.; Costiniuk, C.; Lebouché, B.; et al. Cytomegalovirus Seropositivity Is Associated With Increased Microbial Translocation in People Living With Human Immunodeficiency Virus and Uninfected Controls. Clin. Infect. Dis. 2019, 71, 1438–1446. [Google Scholar] [CrossRef]
- Gianella, S.; Anderson, C.M.; Var, S.R.; de Oliveira, M.F.; Lada, S.M.; Vargas, M.V.; Massanella, M.; Little, S.J.; Richman, D.D.; Strain, M.C.; et al. Replication of Human Herpesviruses Is Associated with Higher HIV DNA Levels during Antiretroviral Therapy Started at Early Phases of HIV Infection. J. Virol. 2016, 90, 3944–3952. [Google Scholar] [CrossRef]
- Spector, S.A.; Hsia, K.; Crager, M.; Pilcher, M.; Cabral, S.; Stempien, M.J. Cytomegalovirus (CMV) DNA Load Is an Independent Predictor of CMV Disease and Survival in Advanced AIDS. J. Virol. 1999, 73, 7027–7030. [Google Scholar] [CrossRef]
- Rawlings, S.A.; Torres, F.; Wells, A.; Lisco, A.; Fitzgerald, W.; Margolis, L.; Gianella, S.; Vanpouille, C. Effect of HIV suppression on the cytokine network in blood and seminal plasma: A longitudinal study. AIDS 2021, 36, 621–630. [Google Scholar] [CrossRef] [PubMed]
- Katsikis, P.D.; Mueller, Y.M.; Villinger, F. The cytokine network of acute HIV infection: A promising target for vaccines and therapy to reduce viral set-point? PLoS Pathog. 2011, 7, e1002055. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Liu, X.; Meyers, K.; Liu, L.; Su, B.; Wang, P.; Li, Z.; Li, L.; Zhang, T.; Li, N.; et al. Cytokine cascade and networks among MSM HIV seroconverters: Implications for early immunotherapy. Sci. Rep. 2016, 6, 36234. [Google Scholar] [CrossRef] [PubMed]
- Speck, C.E.; Coombs, R.W.; Koutsky, L.A.; Zeh, J.; Ross, S.O.; Hooton, T.M.; Collier, A.C.; Corey, L.; Cent, A.; Dragavon, J.; et al. Risk factors for HIV-1 shedding in semen. Am. J. Epidemiol. 1999, 150, 622–631. [Google Scholar] [CrossRef] [PubMed]
- Sheth, P.M.; Danesh, A.; Sheung, A.; Rebbapragada, A.; Shahabi, K.; Kovacs, C.; Halpenny, R.; Tilley, D.; Mazzulli, T.; Macdonald, K.; et al. Disproportionately High Semen Shedding of HIV Is Associated with Compartmentalized Cytomegalovirus Reactivation. J. Infect. Dis. 2006, 193, 45–48. [Google Scholar] [CrossRef]
- Lisco, A.; Munawwar, A.; Introini, A.; Vanpouille, C.; Saba, E.; Feng, X.; Grivel, J.-C.; Singh, S.; Margolis, L. Semen of HIV-1–Infected Individuals: Local Shedding of Herpesviruses and Reprogrammed Cytokine Network. J. Infect. Dis. 2011, 205, 97–105. [Google Scholar] [CrossRef]
- Gianella, S.; Morris, S.R.; Anderson, C.; Spina, C.A.; Vargas, M.V.; Young, J.A.; Richman, D.D.; Little, S.J.; Smith, D. Herpes viruses and HIV-1 drug resistance mutations influence the virologic and immunologic milieu of the male genital tract. AIDS 2013, 27, 39–47. [Google Scholar] [CrossRef]
- Gianella, S.; Smith, D.; Vargas, M.V.; Little, S.J.; Richman, D.D.; Daar, E.S.; Dube, M.P.; Zhang, F.; Ginocchio, C.C.; Haubrich, R.H.; et al. Shedding of HIV and Human Herpesviruses in the Semen of Effectively Treated HIV-1–Infected Men Who Have Sex With Men. Clin. Infect. Dis. 2013, 57, 441–447. [Google Scholar] [CrossRef]
- Gianella, S.; Morris, S.R.; Vargas, M.V.; Young, J.A.; Callahan, B.; Richman, U.D.; Little, S.J.; Smith, D.M. Role of Seminal Shedding of Herpesviruses in HIV Type 1 Transmission. J. Infect. Dis. 2012, 207, 257–261. [Google Scholar] [CrossRef]
- Gianella, S.; Scheffler, K.; Mehta, S.R.; Little, S.J.; Freitas, L.; Morris, S.R.; Smith, D.M. Seminal Shedding of CMV and HIV Transmission among Men Who Have Sex with Men. Int. J. Environ. Res. Public Health 2015, 12, 7585–7592. [Google Scholar] [CrossRef] [PubMed]
- Lupton, J.; Vernamonti, J.; McCabe, C.; Noble, J.; Yin, H.Z.; Eyre, R.C.; Kiessling, A.A. Cytomegalovirus and human immunodeficiency virus in semen of homosexual men. Fertil. Steril. 2014, 101, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Mostad, S.B.; Kreiss, J.K.; Ryncarz, A.J.; Overbaugh, J.; Mandaliya, K.; Chohan, B.; Ndinya-Achola, J.; Bwayo, J.J.; Corey, L. Cervical shedding of cytomegalovirus in human immunodeficiency virus type 1-infected women. J. Med. Virol. 1999, 59, 469–473. [Google Scholar] [CrossRef]
- Mitchell, C.; Hitti, J.; Paul, K.; Agnew, K.; Cohn, S.E.; Luque, A.E.; Coombs, R. Cervicovaginal Shedding of HIV Type 1 Is Related to Genital Tract Inflammation Independent of Changes in Vaginal Microbiota. AIDS Res. Hum. Retrovir. 2011, 27, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Schoenfisch, A.L.; Dollard, S.C.; Amin, M.; Gardner, L.I.; Klein, R.S.; Mayer, K.; Rompalo, A.; Sobel, J.D.; Cannon, M.J. Cytomegalovirus (CMV) shedding is highly correlated with markers of immunosuppression in CMV-seropositive women. J. Med. Microbiol. 2011, 60, 768–774. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Gianella, S.; Redd, A.D.; Grabowski, M.K.; Tobian, A.A.R.; Serwadda, D.; Newell, K.; Patel, E.U.; Kalibbala, S.; Ssebbowa, P.; Gray, R.H.; et al. Vaginal Cytomegalovirus Shedding Before and After Initiation of Antiretroviral Therapy in Rakai, Uganda. J. Infect. Dis. 2015, 212, 899–903. [Google Scholar] [CrossRef] [PubMed]
- Gianella, S.; Tran, S.M.; Morris, S.; Vargas, M.; Porrachia, M.; Oliveira, M.F.; Lada, S.; Zhao, M.; Ellsworth, G.B.; Mathad, J.S.; et al. Sex Differences in CMV Replication and HIV Persistence During Suppressive ART. Open Forum Infect. Dis. 2020, 7, ofaa289. [Google Scholar] [CrossRef]
- Cao, W.; Mehraj, V.; Trottier, B.; Baril, J.-G.; Leblanc, R.; Lebouche, B.; Cox, J.; Tremblay, C.; Lu, W.; Singer, J.; et al. Early Initiation Rather Than Prolonged Duration of Antiretroviral Therapy in HIV Infection Contributes to the Normalization of CD8 T-Cell Counts. Clin. Infect. Dis. 2015, 62, 250–257. [Google Scholar] [CrossRef]
- Routy, J.-P.; Mehraj, V. Very early antiretroviral therapy permits CD8 T cells to keep HIV reservoirs at bay. Ann. Transl. Med. 2017, 5, 434. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).