
Gen Z and HIV—Strategies for Optimizing the Care of the Next Generation of Adolescents Living with HIV
Abstract
:1. Introduction
2. Heterogeneity of Adolescents Living with HIV
3. Preferred Antiretrovirals for Adolescents Living with HIV
4. Medication Side Effects
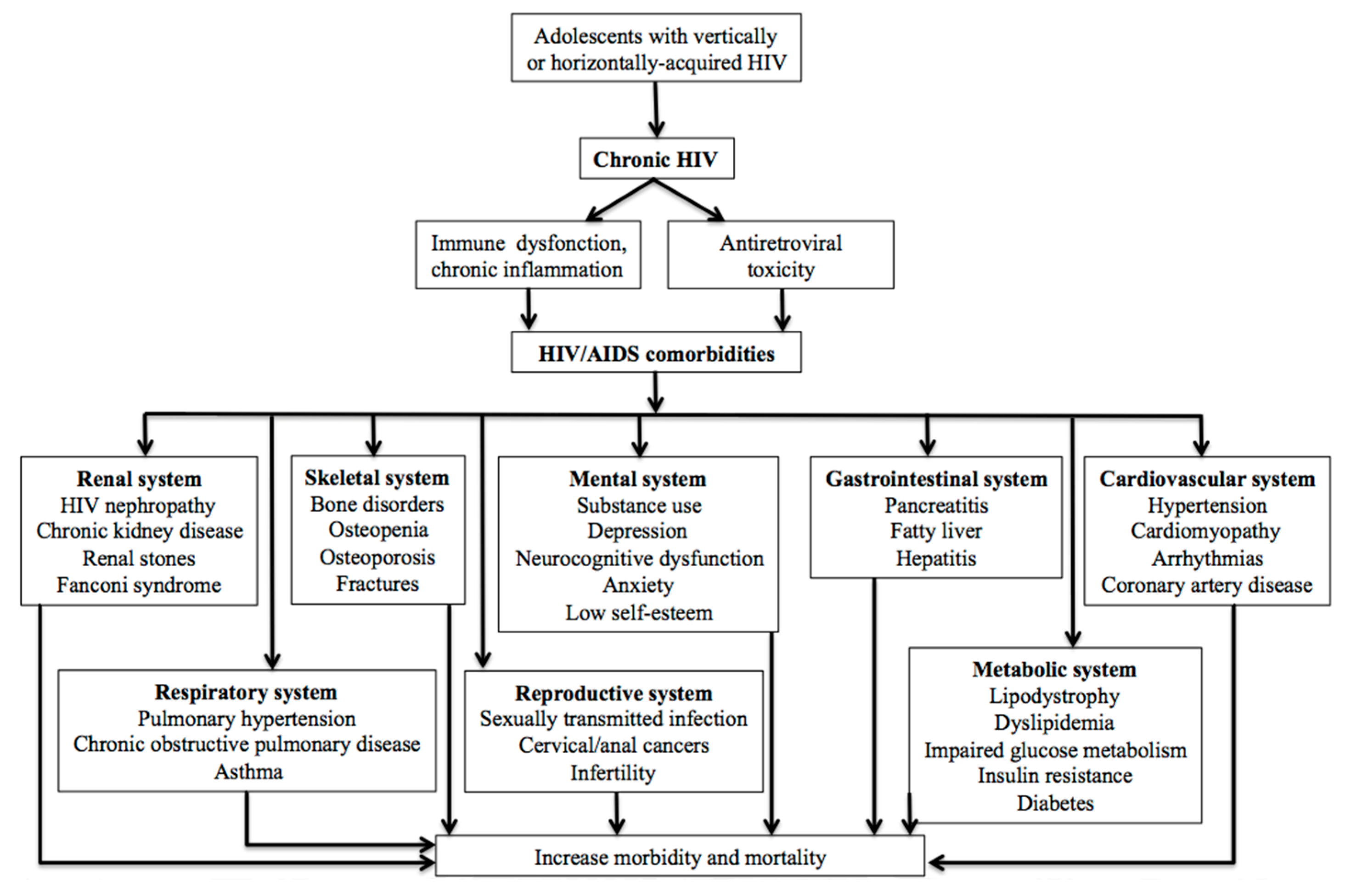
5. Key Complications Affecting Adolescents Living with HIV
6. Neurodevelopmental Issues and Mental Health
7. Opportunistic Infections
8. Sexual Development and Contraception Counseling
9. Adherence Barriers
10. Particularities of ALHIV Living in Low- and Middle-Income Countries
11. Approaches to Optimize Care for ALHIV
11.1. Dual Therapy Regimens
11.2. Intermittent Antiretroviral Therapy
11.3. Long-Acting Antiretrovirals
12. Peer-to-Peer Support
13. Transition to Adult Care
14. Impact of COVID 19 Pandemic
15. Summary
Author Contributions
Funding
Conflicts of Interest
References
- Shorey, S.; Chan, V.; Rajendran, P.; Ang, E. Learning Styles, Preferences and Needs of Generation Z Healthcare Students: Scoping Review. Nurse Educ. Pract. 2021, 57, 103247. [Google Scholar] [CrossRef]
- UNICEF. 2021 HIV and AIDS Global Snapshot: Pregnant Women, Children and Adolescents. Available online: https://www.childrenandaids.org/sites/default/files/2021-11/211130_HIV%20Global%20Snapshot%20(Final).pdf (accessed on 22 June 2023).
- Van der Linden, D.; Lapointe, N.; Kakkar, F.; Ransy, D.G.; Motorina, A.; Maurice, F.; Soudeyns, H.; Lamarre, V. The Young and the Resistant: HIV-Infected Adolescents at t Time of Transfer to Adult Care. J. Pediatr. Infect. Dis. Soc. 2013, 2, 382–385. [Google Scholar] [CrossRef]
- Soumah, A.; Avettand-Fenoel, V.; Veber, F.; Moshous, D.; Mahlaoui, N.; Blanche, S.; Frange, P. High Rates of Antiretroviral Coverage and Virological Suppression in HIV-1-Infected Children and Adolescents. Med. Mal. Infect. 2020, 50, 269–273. [Google Scholar] [CrossRef]
- Collins, I.J.; Foster, C.; Tostevin, A.; Tookey, P.; Riordan, A.; Dunn, D.; Gibb, D.M.; Judd, A.; Hiv, C.; Study, P. Clinical Status of Adolescents with Perinatal HIV at Transfer to Adult Care in the UK/Ireland. Clin. Infect. Dis. 2017, 64, 1105–1112. [Google Scholar] [CrossRef]
- Wood, S.M.; Dowshen, N.; Lowenthal, E. Time to Improve the Global Human Immunodeficiency Virus/ AIDS Care Continuum for Adolescents: A Generation at Stake Sarah. JAMA Pediatr. 2015, 169, 619–620. [Google Scholar] [CrossRef]
- Nachega, J.B.; Hislop, M.; Nguyen, H.; Dowdy, D.W.; Chaisson, R.E.; Regensberg, L.; Cotton, M.; Maartens, G. Antiretroviral Therapy Adherence, Virologic and Immunologic Outcomes in Adolescents Compared with Adults in Southern Africa. J. Acquir. Immune Defic. Syndr. 2009, 51, 65–71. [Google Scholar] [CrossRef]
- Lamb, M.R.; Fayorsey, R.; Nuwagaba-Biribonwoha, H.; Viola, V.; Mutabazi, V.; Alwar, T.; Casalini, C.; Elul, B. High Attrition before and after ART Initiation among Youth (15–24 Years of Age) Enrolled in HIV Care. AIDS 2014, 28, 559–568. [Google Scholar] [CrossRef]
- Judd, A.; Doerholt, K.; Tookey, P.A.; Sharland, M.; Riordan, A.; Menson, E.; Novelli, V.; Lyall, E.G.H.; Masters, J.; Tudor-Williams, G.; et al. Morbidity, Mortality, and Response to Treatment by Children in the United Kingdom and Ireland with Perinatally Acquired HIV Infection during 1996–2006: Planning for Teenage and Adult Care. Clin. Infect. Dis. 2007, 45, 918–924. [Google Scholar] [CrossRef]
- Auld, A.F.; Agolory, S.G.; Shiraishi, R.W.; Wabwire-Mangen, F.; Kwesigabo, G.; Mulenga, M.; Hachizovu, S.; Asadu, E.; Tuho, M.Z.; Ettiegne-Traore, V.; et al. Centers for Disease Control and Prevention MMWR Editorial and Production Staff (Weekly) MMWR Editorial Board. Morb. Mortal. Wkly. Rep. 2019, 8, 4–9. [Google Scholar]
- National Institutes of Health. Clinical Info HIV. Guidelines for the Use of Antretroviral Agents in Adults and Adolescents with HIV. Available online: https://clinicalinfo.hiv.gov/en/guidelines/hiv-clinical-guidelines-adult-and-adolescent-arv/overview?view=full (accessed on 1 May 2023).
- Cardenas, M.C.; Farnan, S.; Hamel, B.L.; Mejia Plazas, M.C.; Sintim-Aboagye, E.; Littlefield, D.R.; Behl, S.; Punia, S.; Enninga, E.A.; Johnson, E.; et al. Prevention of the Vertical Transmission of HIV; A Recap of the Journey so Far. Viruses 2023, 15, 849. [Google Scholar] [CrossRef]
- Connor, E.M.; Sperling, R.S.; Gelber, R.; Kiselev, P.; Scott, G.; O’Sullivan, M.J.; VanDyke, R.; Bey, M.; Shearer, W.; Jacobson, R.L.; et al. Reduction of maternal-infant transmission of human immunodeficiency virus type 1 with zidovudine treatment. Pediatric AIDS Clinical Trials Group Protocol 076 Study Group. N. Engl. J. Med. 1994, 331, 1173–1180. [Google Scholar] [CrossRef]
- Ryom, L.; De Miguel, R.; Cotter, A.G.; Podlekareva, D.; Beguelin, C.; Waalewijn, H.; Arribas, J.R.; Mallon, P.W.; Marzolini, C.; Kirk, O.; et al. Major revision version 11.0 of the European AIDS Clinical Society Guidelines 2021. HIV Med. 2022, 23, 849–858. [Google Scholar] [CrossRef]
- World Health Organization. Consolidated Guidelines on HIV Prevention, Testing, Treatment, Service Delivery and Monitoring: Recommendations for a Public Health Approach; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Gandhi, R.T.; Bedimo, R.; Hoy, J.F.; Landovitz, R.J.; Smith, D.M.; Eaton, E.F.; Lehmann, C.; Springer, S.A.; Sax, P.E.; Thompson, M.A.; et al. Antiretroviral Drugs for Treatment and Prevention of HIV Infection in Adults: 2022 Recommendations of the International Antiviral Society-USA Panel. JAMA 2023, 329, 63–84. [Google Scholar] [CrossRef]
- Turkova, A.; White, E.; Mujuru, H.A.; Kekitiinwa, A.R.; Kityo, C.M.; Violari, A.; Lugemwa, A.; Cressey, T.R.; Musoke, P.; Variava, E.; et al. Dolutegravir as First- or Second-Line Treatment for HIV-1 Infection in Children. N. Engl. J. Med. 2021, 385, 2531–2543. [Google Scholar] [CrossRef]
- Agwu, A.L.; Fairlie, L. Antiretroviral treatment, management challenges and outcomes in perinatally HIV-infected adolescents. J. Int. AIDS Soc. 2013, 16, 18579. [Google Scholar] [CrossRef]
- Paton, N.I.; Musaazi, J.; Kityo, C.; Walimbwa, S.; Hoppe, A.; Balyegisawa, A.; Kaimal, A.; Mirembe, G.; Tukamushabe, P.; Ategeka, G.; et al. Dolutegravir or Darunavir in Combination with Zidovudine or Tenofovir to Treat HIV. N. Engl. J. Med. 2021, 385, 330–341. [Google Scholar] [CrossRef]
- Fortuny, C.; Deyà-Martínez, Á.; Chiappini, E.; Galli, L.; De Martino, M.; Noguera-Julian, A. Metabolic and Renal Adverse Effects of Antiretroviral Therapy in HIV-Infected Children and Adolescents. Pediatr. Infect. Dis. J. 2015, 34, S36–S43. [Google Scholar] [CrossRef]
- Hill, A.; Waters, L.; Pozniak, A. Are new antiretroviral treatments increasing the risks of clinical obesity? J. Virus Erad. 2019, 5, 41–43. [Google Scholar] [CrossRef]
- Jebeile, H.; Kelly, A.S.; O’Malley, G.; Baur, L.A. Obesity in children and adolescents: Epidemiology, causes, assessment, and management. Lancet Diabetes Endocrinol. 2022, 10, 351–365. [Google Scholar] [CrossRef]
- Sax, P.E.; Erlandson, K.M.; Lake, J.E.; McComsey, G.A.; Orkin, C.; Esser, S.; Brown, T.T.; Rockstroh, J.K.; Wei, X.; Carter, C.C.; et al. Weight Gain Following Initiation of Antiretroviral Therapy: Risk Factors in Randomized Comparative Clinical Trials. Clin. Infect. Dis. 2020, 71, 1379–1389. [Google Scholar] [CrossRef]
- Dupont, E.; Cyr-Yombi, J. Antiretroviral therapy and weight gain in naive HIV-1 infected patient: A narrative review. AIDS Rev. 2022, 25, 122–132. [Google Scholar] [CrossRef]
- Dupont, E.; Yombi, J.C. Antiretroviral therapy and weight gain in antiretroviral treatment-experienced HIV patients: A review. AIDS Rev. 2023, 25, 54–64. [Google Scholar] [CrossRef]
- Yusuf, H.E.; Griffith, D.; Agwu, A.L. Preventing and diagnosing HIV-related comorbidities in adolescents. Top. Antivir. Med. 2022, 30, 537–544. [Google Scholar]
- Ivanov, A.V.; Valuev-Elliston, V.T.; Ivanova, O.N.; Kochetkov, S.N.; Starodubova, E.S.; Bartosch, B.; Isaguliants, M.G. Oxidative stress during HIV infection: Mechanisms and consequences. Oxid. Med. Cell. Longev. 2016, 2016, 8910396. [Google Scholar] [CrossRef]
- Heany, S.J.; Levine, A.J.; Lesosky, M.; Phillips, N.; Fouche, J.-P.; Myer, L.; Zar, H.J.; Stein, D.J.; Horvath, S.; Hoare, J. Persistent accelerated epigenetic ageing in a longitudinal cohort of vertically infected HIV-positive adolescents. J. Neurovirol. 2023, 29, 272–282. [Google Scholar] [CrossRef]
- Dimock, D.; Thomas, V.; Cushing, A.; Purdy, J.B.; Worrell, C.; Kopp, J.B.; Hazra, R.; Hadigan, C. Longitudinal assessment of metabolic abnormalities in adolescents and young adults with HIV-infection acquired perinatally or in early childhood. Metabolism 2010, 60, 874–880. [Google Scholar] [CrossRef]
- Monge, M.C.; Samples, C.L. Primary care for children and adolescents living with HIV. Curr. Opin. Pediatr. 2012, 24, 453–461. [Google Scholar] [CrossRef]
- Idris, N.S.; Grobbee, D.E.; Burgner, D.; Cheung, M.M.; Kurniati, N.; Sastroasmoro, S.; Uiterwaal, C.S. Cardiovascular manifestations of HIV infection in children. Eur. J. Prev. Cardiol. 2015, 22, 1452–1461. [Google Scholar] [CrossRef]
- Melvin, A.J.; Montepiedra, G.; Aaron, L.; Meyer, W.A.I.; Spiegel, H.M.; Borkowsky, W.; Abzug, M.J.; Best, B.M.; Crain, M.J.; Borum, P.R.; et al. Safety and Efficacy of Atorvastatin in Human Immunodeficiency Virus-infected Children, Adolescents and Young Adults with Hyperlipidemia. Pediatr. Infect. Dis. J. 2017, 36, 53–60. [Google Scholar] [CrossRef]
- Chastain, D.B.; Stover, K.R.; Riche, D.M. Evidence-based review of statin use in patients with HIV on antiretroviral therapy. J. Clin. Transl. Endocrinol. 2017, 8, 6–14. [Google Scholar] [CrossRef]
- Grinspoon, S.K.; Fitch, K.V.; Zanni, M.V.; Fichtenbaum, C.J.; Umbleja, T.; Aberg, J.A.; Overton, E.T.; Malvestutto, C.D.; Bloomfield, G.S.; Currier, J.S.; et al. Pitavastatin to Prevent Cardiovascular Disease in HIV Infection. N. Engl. J. Med. 2023, 389, 687–699. [Google Scholar] [CrossRef] [PubMed]
- Laughton, B.; Cornell, M.; Boivin, M.; Van Rie, A. Neurodevelopment in Perinatally HIV-Infected Children: A Concern for Adolescence. J. Int. AIDS Soc. 2013, 16, 18603. [Google Scholar] [CrossRef] [PubMed]
- Laughton, B.; Cornell, M.; Kidd, M.; Springer, P.E.; Dobbels, E.F.M.T.; Van Rensburg, A.J.; Otwombe, K.; Babiker, A.; Gibb, D.M.; Violari, A.; et al. Five Year Neurodevelopment Outcomes of Perinatally HIV-Infected Children on Early Limited or Deferred Continuous Antiretroviral Therapy. J. Int. AIDS Soc. 2018, 21, e25106. [Google Scholar] [CrossRef] [PubMed]
- Bucek, A.; Leu, C.S.; Benson, S.; Warne, P.; Abrams, E.J.; Elkington, K.S.; Dolezal, C.; Wiznia, A.; Mellins, C.A. Psychiatric Disorders, Antiretroviral Medication Adherence and Viremia in a Cohort of Perinatally HIV-Infected Adolescents and Young Adults. Pediatr. Infect. Dis. J. 2018, 37, 673–677. [Google Scholar] [CrossRef] [PubMed]
- Woods, S.P.; Moore, D.J.; Weber, E.; Grant, I. Cognitive neuropsychology of HIV-associated neurocognitive disorders. Neuropsychol. Rev. 2009, 19, 152–168. [Google Scholar] [CrossRef] [PubMed]
- Sumari-de Boer, M.; Schellekens, A.; Duinmaijer, A.; Lalashowi, J.M.; Swai, H.J.; de Mast, Q.; van der Ven, A.; Kinabo, G. Efavirenz Is Related to Neuropsychiatric Symptoms among Adults, but Not among Adolescents Living with Human Immunodeficiency Virus in Kilimanjaro, Tanzania. Trop. Med. Int. Health 2018, 23, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Scheper, H.; van Holten, N.; Hovens, J.G.F.M.; de Boer, M.G.J. Severe Depression as a Neuropsychiatric Side Effect Induced by Dolutegravir. HIV Med. 2018, 19, e58–e59. [Google Scholar] [CrossRef] [PubMed]
- Yombi, J.C. Dolutegravir Neuropsychiatric Adverse Events: Specific Drug Effect or Class Effect. AIDS Rev. 2018, 20, 14–26. [Google Scholar]
- Bhana, A.; Abas, M.A.; Kelly, J.; van Pinxteren, M.; Mudekunye, L.A.; Pantelic, M. Mental health interventions for adolescents living with HIV or affected by HIV in low- and middle-income countries: Systematic review. BJPsych Open 2020, 6, e104. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health. Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV. National Institutes of Health, Centers for Disease Control and Prevention, HIV Medicine Association, and Infectious Diseases Society of America. Available online: https://clinicalinfo.hiv.gov/en/guidelines/adult-and-adolescent-opportunistic-infection (accessed on 10 May 2023).
- Marais, B.J.; Gie, R.P.; Hesseling, A.H.; Beyers, N. Adult-type pulmonary tuberculosis in children 10–14 years of age. Pediatr. Infect. Dis. J. 2005, 24, 743–744. [Google Scholar] [CrossRef] [PubMed]
- Ferrand, R.A.; Bandason, T.; Musvaire, P.; Larke, N.; Nathoo, K.; Mujuru, H.; Ndhlovu, C.E.; Munyati, S.; Cowan, F.M.; Gibb, D.M.; et al. Causes of acute hospitalization in adolescence: Burden and spectrum of HIV-related morbidity in a country with an early-onset and severe HIV epidemic: A prospective survey. PLoS Med. 2010, 7, e1000178. [Google Scholar] [CrossRef] [PubMed]
- Meiring, S.T.; Quan, V.C.; Cohen, C.; Dawood, H.; Karstaedt, A.S.; McCarthy, K.M.; Whitelaw, A.C.; Govender, N.P.; Group for Enteric, Respiratory and Meningeal Disease Surveillance in South Africa (GERMS-SA). A comparison of cases of paediatric-onset and adultonset cryptococcosis detected through population-based surveillance, 2005–2007. AIDS 2012, 26, 2307–2314. [Google Scholar] [CrossRef] [PubMed]
- Marais, B.J.; Gie, R.P.; Schaaf, H.S.; Hesseling, A.C.; Obihara, C.C.; Nelson, L.J.; Enarson, D.; Donald, P.R.; Beyers, N. The clinical epidemiology of childhood pulmonary tuberculosis: A critical review of literature from the pre-chemotherapy era. Int. J. Tuberc. Lung Dis. 2004, 8, 278–285. [Google Scholar] [PubMed]
- Wood, R.; Racow, K.; Bekker, L.G.; Morrow, C.; Middelkoop, K.; Mark, D.; Lawn, S.D. Indoor social networks in a South African township: Potential contribution of location to tuberculosis transmission. PLoS ONE 2012, 7, e39246. [Google Scholar] [CrossRef] [PubMed]
- Buchacz, K.; Rogol, A.D.; Lindsey, J.C.; Wilson, C.M.; Hughes, M.D.; Seage, G.R., III; Oleske, J.M.; Rogers, A.S.; Pediatric AIDS Clinical Trials Group 219 Study Team. Delayed onset of pubertal development in children and adolescents with perinatally acquired HIV infection. J. Acquir. Immune Defic. Syndr. 2003, 33, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Kourtis, A.P.; Mirza, A.; Committee on Pediatric Aids. Contraception for HIV-Infected Adolescents. Pediatrics 2016, 138, e20161892. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Medical Eligibility Criteria for Contraceptive Use Executive Summary, 5th ed.; World Health Organization: Geneva, Switzerland, 2015; Available online: https://www.who.int/reproductivehealth/publications/family_planning/Ex-Summ-MEC-5/en/ (accessed on 1 May 2023).
- National Institutes of Health. Recommendations for Use of Antiretroviral Drugs in Pregnant HIV-1-Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV Transmission in the United States. Available online: https://aidsinfo.nih.gov/guidelines/html/3/perinatalguidelines/0 (accessed on 1 May 2023).
- Sevinsky, H.; Eley, T.; Persson, A.; Garner, D.; Yones, C.; Nettles, R.; Krantz, K.; Bertz, R.; Zhang, J. The effect of efavirenz on the pharmacokinetics of an oral contraceptive containing ethinyl estradiol and norgestimate in healthy HIV-negative women. Antivir. Ther. 2011, 16, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Landolt, N.K.; Phanuphak, N.; Ubolyam, S.; Pinyakorn, S.M.; Kerr, S.; Ahluwalia, J.; Thongpaeng, P.; Thammajaruk, N.M.; Cremers, S.; Thomas, T.; et al. Significant decrease of ethinylestradiol with nevirapine, and of etonogestrel with efavirenz in HIV-positive women. J. Acquir. Immune Defic. Syndr. 2014, 66, e50–e52. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Hormonal Contraceptive Methods for Women at High Risk for HIV and Living with HIV: 2014 Guidance Statement; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Centers for Disease Control and Prevention. US. medical eligibility criteria for contraceptive use. MMWR Recomm. Rep. 2010, 59, 1–86. [Google Scholar]
- World Health Organization. Providing Contraceptive Services in the Context of HIV Treatment Programmes; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Ott, M.A.; Sucato, G.S.; Committee on Adolescence. Contraception for adolescents. Pediatrics 2014, 134, e1257-81. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, J.N.; Green, M.; Weaver, M.A.; Mpangile, G.; Kohi, T.W.; Mujaya, S.N.; Lasway, C. Integrating family planning services into HIV care and treatment clinics in Tanzania: Evaluation of a facilitated referral model. Health Policy Plan. 2014, 29, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Kidman, R.; Violari, A. Growing up positive: Adolescent HIV disclosure to sexual partners and others. AIDS Care 2020, 32, 1565–1572. [Google Scholar] [CrossRef] [PubMed]
- Mkumba, L.S.; Nassali, M.; Benner, J.; Ritchwood, T.D. Sexual and reproductive health needs of young people living with HIV in low- and middle-income countries: A scoping review. Reprod. Health. 2021, 18, 219. [Google Scholar] [CrossRef] [PubMed]
- Vanthournout, B.; Van Der Kelen, E.; Elate, D.; Goetghebuer, T.; Hainaut, M.; Levy, J. Clinical Evaluation of Adherence to Antiretroviral Therapy in Adolescents Infected by HIV since Infancy. Arch. Pédiatr. 2013, 20, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Chesney, M.A. Factors Affecting Adherence to Antiretroviral Therapy. Clin. Infect. Dis. 2000, 30, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Hudelson, C.; Cluver, L. Factors Associated with Adherence to Antiretroviral Therapy among Adolescents Living with HIV/AIDS in Low- and Middle-Income Countries: A Systematic Review. AIDS Care Psychol. Socio-Med. Asp. AIDS/HIV 2015, 27, 805–816. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Gerver, S.M.; Fidler, S.; Ward, H. Adherence to Antiretroviral Therapy in Adolescents Living with HIV: Systematic Review and Meta-Analysis. AIDS 2014, 28, 1945–1956. [Google Scholar] [CrossRef] [PubMed]
- Kakkar, F.; Van der Linden, D.; Valois, S.; Maurice, F.; Onnorouille, M.; Lapointe, N.; Soudeyns, H.; Lamarre, V. Health Outcomes and the Transition Experience of HIV-Infected Adolescents after Transfer to Adult Care in Québec, Canada. BMC Pediatr. 2016, 16, 109. [Google Scholar] [CrossRef] [PubMed]
- Ridgeway, K.; Dulli, L.S.; Murray, K.R.; Silverstein, H.; Santo, L.D.; Olsen, P.; Darrow de Mora, D.; McCarraher, D.R. Interventions to Improve Antiretroviral Therapy Adherence among Adolescents in Low- and Middle-Income Countries: A Systematic Review of the Literature. PLoS ONE 2018, 13, e0189770. [Google Scholar] [CrossRef] [PubMed]
- Mills, E.J.; Nachega, J.B.; Bangsberg, D.R.; Singh, S.; Rachlis, B.; Wu, P.; Wilson, K.; Buchan, I.; Gill, C.J.; Cooper, C. Adherence to HAART: A systematic review of developed and developing nation patient-reported barriers and facilitators. PLoS Med. 2006, 3, e438. [Google Scholar] [CrossRef] [PubMed]
- Cahn, P.; Madero, J.S.; Arribas, J.R.; Antinori, A.; Ortiz, R.; Clarke, A.E.; Hung, C.C.; Rockstroh, J.K.; Girard, P.M.; Sievers, J.; et al. Durable Efficacy of Dolutegravir Plus Lamivudine in Antiretroviral Treatment-Naive Adults With HIV-1 Infection: 96-Week Results From the GEMINI-1 and GEMINI-2 Randomized Clinical Trials. J. Acquir. Immune Defic. Syndr. 2020, 83, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Dupont, E.; Yombi, J.C. Is Antiretroviral Two-Drug Regimen the New Standard for HIV Treatment in Naive Patients? AIDS Rev. 2019, 21, 143–156. [Google Scholar] [CrossRef] [PubMed]
- Van Wyk, J.; Ajana, F.; Bisshop, F.; De Wit, S.; Osiyemi, O.; Sogorb, J.P.; Routy, J.-P.; Wyen, C.; Ait-Khaled, M.; Nascimento, M.C.; et al. Efficacy and Safety of Switching to Dolutegravir/Lamivudine Fixed-Dose 2-Drug Regimen vs Continuing a Tenofovir Alafenamide-Based 3- or 4-Drug Regimen for Maintenance of Virologic Suppression in Adults Living with Human Immunodeficiency Virus Type 1: Phase 3, Randomized, Noninferiority TANGO Study. Clin. Infect. Dis. 2020, 71, 1920–1929. [Google Scholar] [PubMed]
- Llibre, J.M.; Brites, C.; Cheng, C.Y.; Osiyemi, O.; Galera, C.; Hocqueloux, L.; Maggiolo, F.; Degen, O.; Taylor, S.; Blair, E.; et al. Efficacy and Safety of Switching to the 2-Drug Regimen Dolutegravir/Lamivudine Versus Continuing a 3- or 4-Drug Regimen for Maintaining Virologic Suppression in Adults Living with Human Immunodeficiency Virus 1 (HIV-1): Week 48 Results from the Phase 3, Noninferiority SALSA Randomized Trial. Clin. Infect. Dis. 2023, 76, 720–729. [Google Scholar] [PubMed]
- Compagnucci, A.; Chan, M.; Saïdi, Y.; Cressey, T.; Bamford, A.; Riault, Y.; Coelho, A.; Nolan, A.; Chalermpantmetagul, S.; Amuge, P.; et al. Once-Daily Integrase Inhibitor (INSTI) with Boosted Darunavir Is Non-Inferior to Standard of Care in Virologically Suppressed Children, Week 48 Results of the SMILE PENTA-17 TRIAL (ABSTRACT 1079). Available online: https://theprogramme.ias2021.org/Abstract/Abstract/1079 (accessed on 23 June 2023).
- Butler, K.; Inshaw, J.; Ford, D.; Bernays, S.; Scott, K.; Kenny, J.; Klein, N.; Turkova, A.; Harper, L.; Nastouli, E.; et al. BREATHER (PENTA 16) short-cycle therapy (SCT) (5 days on/2 days off) in young people with chronic human immunodeficiency virus infection: An open, randomised, parallel-group Phase II/III trial. Health Technol. Assess. 2016, 20, 1. [Google Scholar] [CrossRef] [PubMed]
- Landman, R.; de Truchis, P.; Assoumou, L.; Lambert, S.; Bellet, J.; Amat, K.; Lefebvre, B.; Allavena, C.; Katlama, C.; Yazdanpanah, Y.; et al. A 4-days-on and 3-days-off maintenance treatment strategy for adults with HIV-1 (ANRS 170 QUATUOR): A randomised, open-label, multicentre, parallel, non-inferiority trial. Lancet HIV 2022, 9, e79–e90. [Google Scholar] [CrossRef] [PubMed]
- Roland, T.; Yombi, J.C. Is intermittent antiretroviral therapy a satisfactory strategy for the management of patients living with HIV? AIDS Rev. 2021, 23, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Haberer, J.; Mellins, C. Pediatric Adherence to HIV Antiretroviral Therapy. Curr. HIV/AIDS Rep. 2009, 6, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Thoueille, P.; Choong, E.; Cavassini, M.; Buclin, T.; Decosterd, L.A. Long-Acting Antiretrovirals: A New Era for the Management and Prevention of HIV Infection. J. Antimicrob. Chemother. 2022, 77, 290–302. [Google Scholar] [CrossRef] [PubMed]
- Margolis, D.A.; Gonzalez-Garcia, J.; Stellbrink, H.J.; Eron, J.J.; Yazdanpanah, Y.; Podzamczer, D.; Lutz, T.; Angel, J.B.; Richmond, G.J.; Clotet, B.; et al. Long-Acting Intramuscular Cabotegravir and Rilpivirine in Adults with HIV-1 Infection (LATTE-2): 96-Week Results of a Randomised, Open-Label, Phase 2b, Non-Inferiority Trial. The Lancet 2017, 390, 1499–1510. [Google Scholar] [CrossRef] [PubMed]
- Orkin, C.; Arasteh, K.; Górgolas Hernández-Mora, M.; Pokrovsky, V.; Overton, E.T.; Girard, P.-M.; Oka, S.; Walmsley, S.; Bettacchi, C.; Brinson, C.; et al. Long-Acting Cabotegravir and Rilpivirine after Oral Induction for HIV-1 Infection. N. Engl. J. Med. 2020, 382, 1124–1135. [Google Scholar] [CrossRef] [PubMed]
- Swindells, S.; Andrade-Villanueva, J.-F.; Richmond, G.J.; Rizzardini, G.; Baumgarten, A.; Masiá, M.; Latiff, G.; Pokrovsky, V.; Bredeek, F.; Smith, G.; et al. Long-Acting Cabotegravir and Rilpivirine for Maintenance of HIV-1 Suppression. N. Engl. J. Med. 2020, 382, 1112–1123. [Google Scholar] [CrossRef] [PubMed]
- Garris, C.P.; Czarnogorski, M.; Dalessandro, M.; D’Amico, R.; Nwafor, T.; Williams, W.; Merrill, D.; Wang, Y.Y.; Stassek, L.; Wohlfeiler, M.B.; et al. Perspectives of People Living with HIV-1 on Implementation of Long-Acting Cabotegravir plus Rilpivirine in US Healthcare Settings: Results from the CUSTOMIZE Hybrid III Implementation-Effectiveness Study. J. Int. AIDS Soc. 2022, 25, e26006. [Google Scholar] [CrossRef] [PubMed]
- Queen Mary University of London Implementing Long-Acting Novel Antiretrovirals—The ILANA Study. Available online: https://clinicaltrials.gov/ct2/show/NCT05294159 (accessed on 15 July 2023).
- Moore, C.B.; Capparelli, E.; Calabrese, K.; Best, B.M.; Ward, S.; McCoig, C.; Crauwels, H.; Agwu, A.; Samson, P.; Heckman, B.; et al. Safety and Pk of Long-Acting Cabotegravir. In Proceedings of the 29th CROI Conference on Retroviruses and Opportunistic Infections, Virtual, 12–16 February 2022. [Google Scholar]
- Lowenthal, E.D.; Chapman, J.; Calabrese, K.; Milligan, R.; Agwu, A.; Camacho-Gonzalez, A.; Smith-Anderson, C.; Kneebone, J.; McCoig, C.; Harrington, C.M.; et al. Adolescent and Parent Experiences with Long-Acting Injectables in the MOCHA Study. In Proceedings of the CROI Conference on Retroviruses and Opportunistic Infections, Virtual, 12–16 February 2022. [Google Scholar]
- Orkin, C.; Bernal Morell, E.; Tan, D.H.S.; Katner, H.; Stellbrink, H.-J.; Belonosova, E.; DeMoor, R.; Griffith, S.; Thiagarajah, S.; Van Solingen-Ristea, R.; et al. Initiation of long-acting cabotegravir plus rilpivirine as direct-to-injection or with an oral lead-in in adults with HIV-1 infection: Week 124 results of the open-label phase 3 FLAIR study. Lancet HIV 2021, 8, e668–e678. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, M.; Salazar, J.; Hickey, M.; Christopoulos, K.; Oskarsson, J.; Shiels, M.; Szumowski, J.; Grochowski, J.; Munoz-Mayorga, F.; Sauceda, J.; et al. High virologic suppression rates on long-acting ART in a safety-net clinic population. In Proceedings of the CROI Conference on Retroviruses and Opportunistic Infections, Virtual, 20–23 February 2023. [Google Scholar]
- Maturo, D.; Powell, A.; Major-Wilson, H.; Sanchez, K.; De Santis, J.P.; Friedman, L.B. Transitioning Adolescents and Young Adults with HIV Infection to Adult Care: Pilot Testing the “Movin’ Out” Transitioning Protocol. J. Pediatr. Nurs. 2015, 30, e29–e35. [Google Scholar] [CrossRef] [PubMed]
- Campbell, F.; Biggs, K.; Aldiss, S.K.; O’Neill, P.M.; Clowes, M.; McDonagh, J.; While, A.; Gibson, F. Transition of care for adolescents from paediatric services to adult health services. Cochrane Database Syst. Rev. 2016, 4, CD009794. [Google Scholar] [CrossRef] [PubMed]
- Dahourou, D.L.; Gautier-Lafaye, C.; Teasdale, C.A.; Renner, L.; Yotebieng, M.; Desmonde, S.; Ayaya, S.; Davies, M.-A.; Leroy, V. Transition from paediatric to adult care of adolescents living with HIV in sub-Saharan Africa: Challenges, youth-friendly models, and outcomes. J. Int. AIDS Soc. 2017, 20 (Suppl. S3), 21528. [Google Scholar] [CrossRef] [PubMed]
- Mbiya, B.; Goetghebuer, T.; Tshibangu, E.; Van der Linden, D. Immunological and Virological Outcome of HIV-Infected Adolescents after Their Transfer to Adult Care Services in Belgium. Malmo, Sweden, 28 May–2 June 2018. [Google Scholar]
- Zanoni, B.C.; Archary, M.; Sibaya, T.; Musinguzi, N.; Haberer, J.E. Transition from pediatric to adult care for adolescents living with HIV in South Africa: A natural experiment and survival analysis. PLoS ONE 2020, 15, e0240918. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Progress Report on HIV, Viral Hepatitis and Sexually Transmitted Infections, 2021; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Dorward, J.; Khubone, T.; Gate, K.; Ngobese, H.; Sookrajh, Y.; Mkhize, S.; Jeewa, A.; Bottomley, C.; Lewis, L.; Baisley, K.; et al. The Impact of the COVID-19 Lockdown on HIV Care in 65 South African Primary Care Clinics: An Interrupted Time Series Analysis. Lancet HIV 2021, 8, e158–e165. [Google Scholar] [CrossRef] [PubMed]
- McFall, A.M.; Menezes, N.P.; Srikrishnan, A.K.; Solomon, S.S.; Anand, S.; Baishya, J.J.; Lucas, G.M.; Celentano, D.D.; Mehta, S.H. Impact of the COVID-19 Pandemic on HIV Prevention and Care Services among Key Populations across 15 Cities in India: A Longitudinal Assessment of Clinic-Based Data. J. Int. AIDS Soc. 2022, 25, e25960. [Google Scholar] [CrossRef] [PubMed]
- Kuehn, B.M. News from the Centers for Disease Control and Prevention. JAMA J. Am. Med. Assoc. 2022, 327, 711. [Google Scholar] [CrossRef]
- WHO. Technical Report: Assessment of HIV Testing Services and Antiretroviral Therapy Service Disruptions in the Context of COVID-19: Lessons Learned and Way Forward in Sub-Saharan Africa; World Health Organization: Geneva, Switzerland, 2021; pp. 1–8. [Google Scholar]
- Traub, A.M.; Medley, A.; Gross, J.; Sloan, M.; Amzel, A.; Gleason, M.M.; Fernando, N.B.; Wong, V.; Grillo, M.P.; Wolf, H.T.; et al. Pediatric HIV Case Identification Across 22 PEPFAR-Supported Countries During the COVID-19 Pandemic, October 2019–September 2020. MMWR. Morb. Mortal. Wkly. Rep. 2022, 71, 894–898. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. Turning the Tide against AIDS Will Require More Concentrated Focus on Adolescents and Young People. Available online: https://data.unicef.org/topic/hiv-aids/ (accessed on 16 July 2023).
- UNAIDS. Core Epidemiology Slides; UNAIDS: Geneva, Switzerland, 2022. [Google Scholar]
- Racine, N.; McArthur, B.A.; Cooke, J.E.; Eirich, R.; Zhu, J.; Madigan, S. Global Prevalence of Depressive and Anxiety Symptoms in Children and Adolescents during COVID-19: A Meta-Analysis. JAMA Pediatr. 2021, 175, 1142–1150. [Google Scholar] [CrossRef] [PubMed]
- Wyk, B.V.; Mayman, Y. Impact of COVID-19 pandemic in adolescents on HIV treatment. Pan Afr. Med. J. 2022, 42, 120. [Google Scholar] [PubMed]

{kind=link}
| Guideline | PENTA/EACS | WHO Guidelines | NIH Guidelines |
|---|---|---|---|
| Initial regimen | ABC + 3TC + BIC or DTG | TDF + 3TC (or FTC) + DTG | TAF + FTC + DTG or BIC |
| Alternative regimen | TAF + 3TC + BIC or DTG | TDF + 3TC + EFV | ABC + 3TC + DTG or RAL |
| Antiretroviral Class | Combined Hormonal Methods and Progestin-Only Pills | Levonorgestrel IUD | Progestin Implants | Progestin Injectables (DMPA) | Emergency Contraception |
|---|---|---|---|---|---|
| Pis | Interactions with most ritonavir-boosted PIs may decrease hormone contraceptive levels and contraceptive efficacy; alternative or additional contraceptive methods are recommended | No known interactions | Potential interaction, very limited clinical data | No known interactions | Possible interaction of ulipristal with elvitegravir/cobicistat; no clinical data |
| NRTIs | No known interactions | No known interactions | No known interactions | No known interactions | No known interactions |
| NNRTIs | Interactions with efavirenz may decrease hormonal contraceptive levels and contraceptive efficacy; alternative or additional contraceptive methods are recommended | No known interactions | Potential interaction with efavirenz may limit its contraceptive efficacy; more data are needed | No known interactions | Interactions of levonorgestrel emergency contraception with efavirenz may limit efficacy; possible interactions of ulipristal with NNRTIs; no clinical data |
| Integrase inhibitors | Possible interaction with elvitegravir/cobicistat | No known interactions | No known interactions | No known interactions | Possible interaction of ulipristal with elvitegravir/cobicistat |
| Entry/fusion inhibitors | No known interactions | No known interactions | No known interactions | No known interactions | No known interactions |
| Approach | Description |
|---|---|
| Comprehensive Support | Provide comprehensive support services tailored to the unique needs of adolescents living with HIV. Create a dedicated youth HIV clinic. |
| Adherence Counseling | Offer individualized counseling sessions to address adherence challenges and provide strategies for medication adherence. |
| Peer Support | Create support groups or peer networks for adolescents to connect, share experiences, and provide mutual encouragement. |
| Youth-Friendly Services | Design healthcare facilities and services that are teen-friendly, non-judgmental, and accessible for adolescents, with youth-friendly hours (e.g., evening hours). |
| Mental Health Support | Offer mental health services to address psychological and emotional well-being, including counseling and therapy. |
| Medication Reminders | Implement strategies such as mobile apps, SMS alerts, or pillboxes to help adolescents remember to take medications. |
| Treatment Simplification | Novel cART delivery strategies (e.g., long-acting oral or injectable cART), once daily/fixed-dose combinations, regimens to minimize side effects |
| Family Involvement | Involve families/caregivers in the treatment process, providing education and support to ensure adherence at home. |
| Adherence Tools and Resources | Provide educational materials, visual aids, and accessible resources to empower adolescents in managing their own care. |
| Care Transition Planning | Support a smooth transition from pediatric to adult healthcare services, ensuring continuity of care during the transition. |
| Continuous Education | Offer ongoing education and information on HIV, treatment advancements, and sexual health to empower informed decision-making. |
| Sexual and Reproductive Health Education | Provide comprehensive sexuality education, including information on safe sex, contraception, preventing transmission and U=U education. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dufour, I.; Fougère, Y.; Goetghebuer, T.; Hainaut, M.; Mbiya, B.; Kakkar, F.; Yombi, J.C.; Van der Linden, D. Gen Z and HIV—Strategies for Optimizing the Care of the Next Generation of Adolescents Living with HIV. Viruses 2023, 15, 2023. https://doi.org/10.3390/v15102023
Dufour I, Fougère Y, Goetghebuer T, Hainaut M, Mbiya B, Kakkar F, Yombi JC, Van der Linden D. Gen Z and HIV—Strategies for Optimizing the Care of the Next Generation of Adolescents Living with HIV. Viruses. 2023; 15(10):2023. https://doi.org/10.3390/v15102023
Chicago/Turabian StyleDufour, Inès, Yves Fougère, Tessa Goetghebuer, Marc Hainaut, Benoît Mbiya, Fatima Kakkar, Jean Cyr Yombi, and Dimitri Van der Linden. 2023. "Gen Z and HIV—Strategies for Optimizing the Care of the Next Generation of Adolescents Living with HIV" Viruses 15, no. 10: 2023. https://doi.org/10.3390/v15102023