

Respiratory Syncytial Virus Reinfections in Children in Western Australia
 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Location and RSV Seasonality
2.2. Data Sources
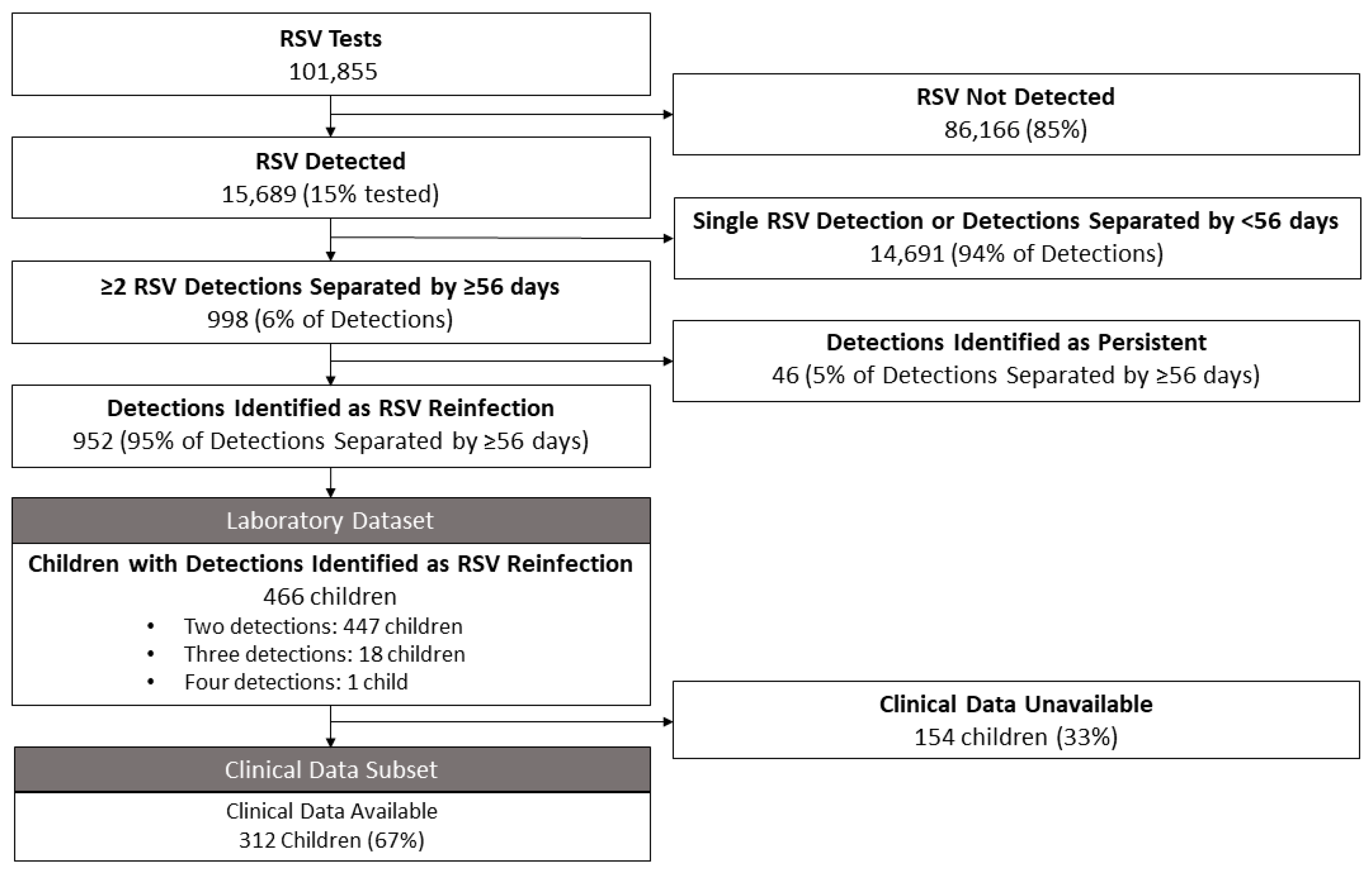
2.2.1. Laboratory Data
2.2.2. Clinical Data Subset
2.3. Definitions
2.3.1. Persistent Detection
2.3.2. Predisposing Factors
2.3.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Subtyping Data
3.2. Clinical Data Subset
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saravanos, G.L.; Sheel, M.; Homaira, N.; Dey, A.; Brown, E.; Wang, H.; Macartney, K.; Wood, N.J. Respiratory syncytial virus-associated hospitalisations in Australia, 2006–2015. Med. J. Aust. 2019, 210, 447–453. [Google Scholar] [CrossRef]
- Li, Y.; Wang, X.; Blau, D.M.; Caballero, M.T.; Feikin, D.R.; Gill, C.J.; Madhi, S.A.; Omer, S.B.; Simões, E.A.; Campbell, H. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: A systematic analysis. Lancet 2022, 399, 2047–2064. [Google Scholar] [CrossRef]
- Na’amnih, W.; Kassem, E.; Tannous, S.; Kagan, V.; Jbali, A.; Hanukayev, E.; Freimann, S.; Obolski, U.; Muhsen, K. Incidence and risk factors of hospitalisations for respiratory syncytial virus among children aged less than 2 years. Epidemiol. Infect. 2022, 150, e45. [Google Scholar] [CrossRef]
- Noble, M.; Khan, R.A.; Walker, B.; Bennett, E.; Gent, N. Respiratory syncytial virus-associated hospitalisation in children aged ≤5 years: A scoping review of literature from 2009 to 2021. ERJ Open Res. 2022, 8, 00593–02021. [Google Scholar] [CrossRef]
- Russell, C.D.; Unger, S.A.; Walton, M.; Schwarze, J. The Human Immune Response to Respiratory Syncytial Virus Infection. Clin. Microbiol. Rev. 2017, 30, 481–502. [Google Scholar] [CrossRef]
- Barnes, M.V.C.; Openshaw, P.J.M.; Thwaites, R.S. Mucosal Immune Responses to Respiratory Syncytial Virus. Cells 2022, 11, 1153. [Google Scholar] [CrossRef]
- Nduaguba, S.O.; Tran, P.T.; Choi, Y.; Winterstein, A.G. Respiratory syncytial virus reinfections among infants and young children in the United States, 2011–2019. PLoS ONE 2023, 18, e0281555. [Google Scholar] [CrossRef]
- Ohuma, E.O.; Okiro, E.A.; Ochola, R.; Sande, C.J.; Cane, P.A.; Medley, G.F.; Bottomley, C.; Nokes, D.J. The natural history of respiratory syncytial virus in a birth cohort: The influence of age and previous infection on reinfection and disease. Am. J. Epidemiol. 2012, 176, 794–802. [Google Scholar] [CrossRef]
- Bont, L.; Versteegh, J.; Swelsen, W.T.; Heijnen, C.J.; Kavelaars, A.; Brus, F.; Draaisma, J.M.; Pekelharing-Berghuis, M.; van Diemen-Steenvoorde, R.A.; Kimpen, J.L. Natural reinfection with respiratory syncytial virus does not boost virus-specific T-cell immunity. Pediatr. Res. 2002, 52, 363–367. [Google Scholar] [CrossRef]
- Kutsaya, A.; Teros-Jaakkola, T.; Kakkola, L.; Toivonen, L.; Peltola, V.; Waris, M.; Julkunen, I. Prospective clinical and serological follow-up in early childhood reveals a high rate of subclinical RSV infection and a relatively high reinfection rate within the first 3 years of life. Epidemiol. Infect. 2016, 144, 1622–1633. [Google Scholar] [CrossRef] [PubMed]
- Mazur, N.I.; Terstappen, J.; Baral, R.; Bardají, A.; Beutels, P.; Buchholz, U.J.; Cohen, C.; Crowe, J.E.; Cutland, C.L.; Eckert, L. Respiratory syncytial virus prevention within reach: The vaccine and monoclonal antibody landscape. Lancet Infect. Dis. 2023, 23, e2–e21. [Google Scholar] [CrossRef] [PubMed]
- Sparrow, E.; Adetifa, I.; Chaiyakunapruk, N.; Cherian, T.; Fell, D.B.; Graham, B.S.; Innis, B.; Kaslow, D.C.; Karron, R.A.; Nair, H.; et al. WHO preferred product characteristics for monoclonal antibodies for passive immunization against respiratory syncytial virus (RSV) disease in infants—Key considerations for global use. Vaccine 2022, 40, 3506–3510. [Google Scholar] [CrossRef] [PubMed]
- Minney-Smith, C.A.; Foley, D.A.; Sikazwe, C.T.; Levy, A.; Smith, D.W. The seasonality of respiratory syncytial virus in Western Australia prior to implementation of SARS-CoV-2 non-pharmaceutical interventions. Influenza Other Respir. Viruses 2023, 17, e13117. [Google Scholar] [CrossRef] [PubMed]
- Foley, D.A.; Yeoh, D.K.; Minney-Smith, C.A.; Martin, A.C.; Mace, A.O.; Sikazwe, C.T.; Le, H.; Levy, A.; Moore, H.C.; Blyth, C.C. The Interseasonal Resurgence of Respiratory Syncytial Virus in Australian Children Following the Reduction of Coronavirus Disease 2019-Related Public Health Measures. Clin. Infect. Dis. 2021, 73, e2829–e2830. [Google Scholar] [CrossRef] [PubMed]
- Foley, D.A.; Phuong, L.K.; Peplinski, J.; Lim, S.M.J.; Lee, W.H.; Keane, A.; Wong, J.W.S.; Minney-Smith, C.A.; Martin, A.C.; Mace, A.O.; et al. Examining the entire delayed respiratory syncytial virus season in Western Australia. Arch. Dis. Child. 2022, 107, 517–519. [Google Scholar] [CrossRef] [PubMed]
- WAtch, V. Virus Watch—Week Ending 10th September 2023; Communicable Disease Control Directorate: Perth, Australia, 2023. [Google Scholar]
- Chidlow, G.R.; Harnett, G.B.; Shellam, G.R.; Smith, D.W. An economical tandem multiplex real-time PCR technique for the detection of a comprehensive range of respiratory pathogens. Viruses 2009, 1, 42–56. [Google Scholar] [CrossRef]
- CAHS. CAHS Annual Report 2020–2021. Available online: https://www.cahs.health.wa.gov.au/~/media/HSPs/CAHS/Documents/About-us/Annual-Reports/CAHS-2020-21-Annual-Report.pdf (accessed on 25 March 2023).
- Hospital, F.S. Record Day for Paediatric Emergency Department. Available online: https://www.fsh.health.wa.gov.au/About-us/News/Record-day-for-Paediatric-Emergency-Department (accessed on 17 July 2023).
- Munywoki, P.K.; Koech, D.C.; Agoti, C.N.; Kibirige, N.; Kipkoech, J.; Cane, P.A.; Medley, G.F.; Nokes, D.J. Influence of age, severity of infection, and co-infection on the duration of respiratory syncytial virus (RSV) shedding. Epidemiol. Infect. 2015, 143, 804–812. [Google Scholar] [CrossRef]
- Cheng, F.W.; Lee, V.; Shing, M.M.; Li, C.K. Prolonged shedding of respiratory syncytial virus in immunocompromised children: Implication for hospital infection control. J. Hosp. Infect. 2008, 70, 383–385. [Google Scholar] [CrossRef]
- Foley, D.A.; Phuong, L.K.; Peplinski, J.; Lim, S.M.; Lee, W.H.; Farhat, A.; Minney-Smith, C.A.; Martin, A.C.; Mace, A.O.; Sikazwe, C.T.; et al. Examining the interseasonal resurgence of respiratory syncytial virus in Western Australia. Arch. Dis. Child. 2022, 107, e7. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics Australian Demographic Statisitics. Available online: https://www.abs.gov.au/AUSSTATS/abs@.nsf/Latestproducts/3101.0Main%20Features3Dec%202019?opendocument&tabname=Summary&prodno=3101.0&issue=Dec%202019&num=&view= (accessed on 1 February 2023).
- SankeyMATIC. Available online: https://sankeymatic.com/build/ (accessed on 1 July 2023).
- Shi, T.; Balsells, E.; Wastnedge, E.; Singleton, R.; Rasmussen, Z.A.; Zar, H.J.; Rath, B.A.; Madhi, S.A.; Campbell, S.; Vaccari, L.C.; et al. Risk factors for respiratory syncytial virus associated with acute lower respiratory infection in children under five years: Systematic review and meta-analysis. J. Glob. Health 2015, 5, 020416. [Google Scholar] [CrossRef]
- Rose, E.B.; Dahl, R.M.; Havers, F.P.; Peacock, G.; Langley, G.E. Respiratory Syncytial Virus-Associated Hospitalizations in Children With Neurological Disorders, 2006–2015. J. Pediatr. Infect. Dis. Soc. 2021, 10, 951–957. [Google Scholar] [CrossRef] [PubMed]
- Tan, D.; Goff, Z.; MacDonald, B.; Blyth, C.C.; Foley, D.A. The Loss of Respiratory Syncytial Virus Seasonality and the Effects on Palivizumab Administration. Pediatr. Infect. Dis. J. 2022, 41, e407–e408. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Group | N | Median Age (IQR) | Comparison With Reinfection Group |
|---|---|---|---|
| All RSV First Detections | 15,689 | 12 months (4–26) | p = 0.5 |
| Reinfection Group | N | Median Age (IQR) | Median Interval (IQR) to Subsequent Detection |
| 466 | 9 months (3.6 to 20) | 460 days (324 to 812) |
| 466 | 29 months (18 to 50) | 447 days (369 to 852) |
| 19 | 52 months (34 to 73) | 530 days |
| 1 | 48 months | - |
| Age Group at 1st Detection | N | Median Age (IQR) | Median Interval (IQR) to Subsequent Detection |
| 178 | 3 months (2 to 4) | 470 days (333 to 877) |
| 190 | 12 months (8 to 17) | 393 days (282 to 707) |
| 98 | 37 months (30 to 50) | 644 days (368 to 1047) |
| Number | % with Predisposing Factors (N) |
|---|---|
| 54 (159) |
| 100 (15) |
| 100 (1) |
| Predisposing Factor | % (N) |
| Any risk factor | 56 (175) |
| Prematurity (<37 weeks) | 29 (89) |
| 12 (38) |
| Respiratory Condition | 24 (76) |
| 12 (37) |
| 10 (31) |
| 5 (15) |
| 3 (8) |
| Significant Heart Disease | 5 (16) |
| Neurology/neuromuscular/syndromes | 17 (53) |
| 2 (8) |
| Immunodeficiency | 4 (14) |
| All | Predisposing Factors | No Predisposing Factors | p-Value | |
|---|---|---|---|---|
| Median Age at First Detection, Months (IQR) | 9 months | 12.8 months | 5.5 months | <0.0001 |
| (3.5–21.3) | (5.2 to 27.7) | (2.3 to 14.4) | ||
| % First Detection Admitted (N) | 85% | 89% | 80% | 0.03 |
| (265) | (156) | (109) | ||
| Length of Stay, Days (IQR) | 3.2 days | 4 days | 2.6 days | <0.0001 |
| (1.7 to 6) | (2.1 to 7.2) | (1 to 4.7) | ||
| Median Interval to Second Detection, Days (IQR) | 458 days | 462 days | 456 days | >0.05 |
| (325 to 812) | (335 to 951) | (314 to 692) | ||
| Median Age at Second detection, Years (IQR) | 2.3 years | 3 years | 1.9 years | <0.0001 |
| (1.5 to 4.3) | (1.8 to 4.8) | (1.3 to 3.3) | ||
| % Second Detection Admitted (N) | 79% | 83% | 70% | 0.007 |
| (242) | (146) | (96) | ||
| Length of Stay for Second Detection, Days (IQR) | 1.8 days | 2.5 days | 0.9 days | <0.0001 |
| (0.8 to 3.4) | (1.4 to 4.7) | (0.6 to 1.8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Foley, D.A.; Minney-Smith, C.A.; Lee, W.H.; Oakes, D.B.; Hazelton, B.; Ford, T.J.; Wadia, U.; Sikazwe, C.; Moore, H.C.; Nicol, M.P.; et al. Respiratory Syncytial Virus Reinfections in Children in Western Australia. Viruses 2023, 15, 2417. https://doi.org/10.3390/v15122417
Foley DA, Minney-Smith CA, Lee WH, Oakes DB, Hazelton B, Ford TJ, Wadia U, Sikazwe C, Moore HC, Nicol MP, et al. Respiratory Syncytial Virus Reinfections in Children in Western Australia. Viruses. 2023; 15(12):2417. https://doi.org/10.3390/v15122417
Chicago/Turabian StyleFoley, David A., Cara A. Minney-Smith, Wei Hao Lee, Daniel B. Oakes, Briony Hazelton, Timothy J. Ford, Ushma Wadia, Chisha Sikazwe, Hannah C. Moore, Mark P. Nicol, and et al. 2023. "Respiratory Syncytial Virus Reinfections in Children in Western Australia" Viruses 15, no. 12: 2417. https://doi.org/10.3390/v15122417
APA StyleFoley, D. A., Minney-Smith, C. A., Lee, W. H., Oakes, D. B., Hazelton, B., Ford, T. J., Wadia, U., Sikazwe, C., Moore, H. C., Nicol, M. P., Levy, A., & Blyth, C. C. (2023). Respiratory Syncytial Virus Reinfections in Children in Western Australia. Viruses, 15(12), 2417. https://doi.org/10.3390/v15122417