
Metformin and Hepatocellular Carcinoma Risk Reduction in Diabetic Patients with Chronic Hepatitis C: Fact or Fiction?




Abstract
:1. Introduction
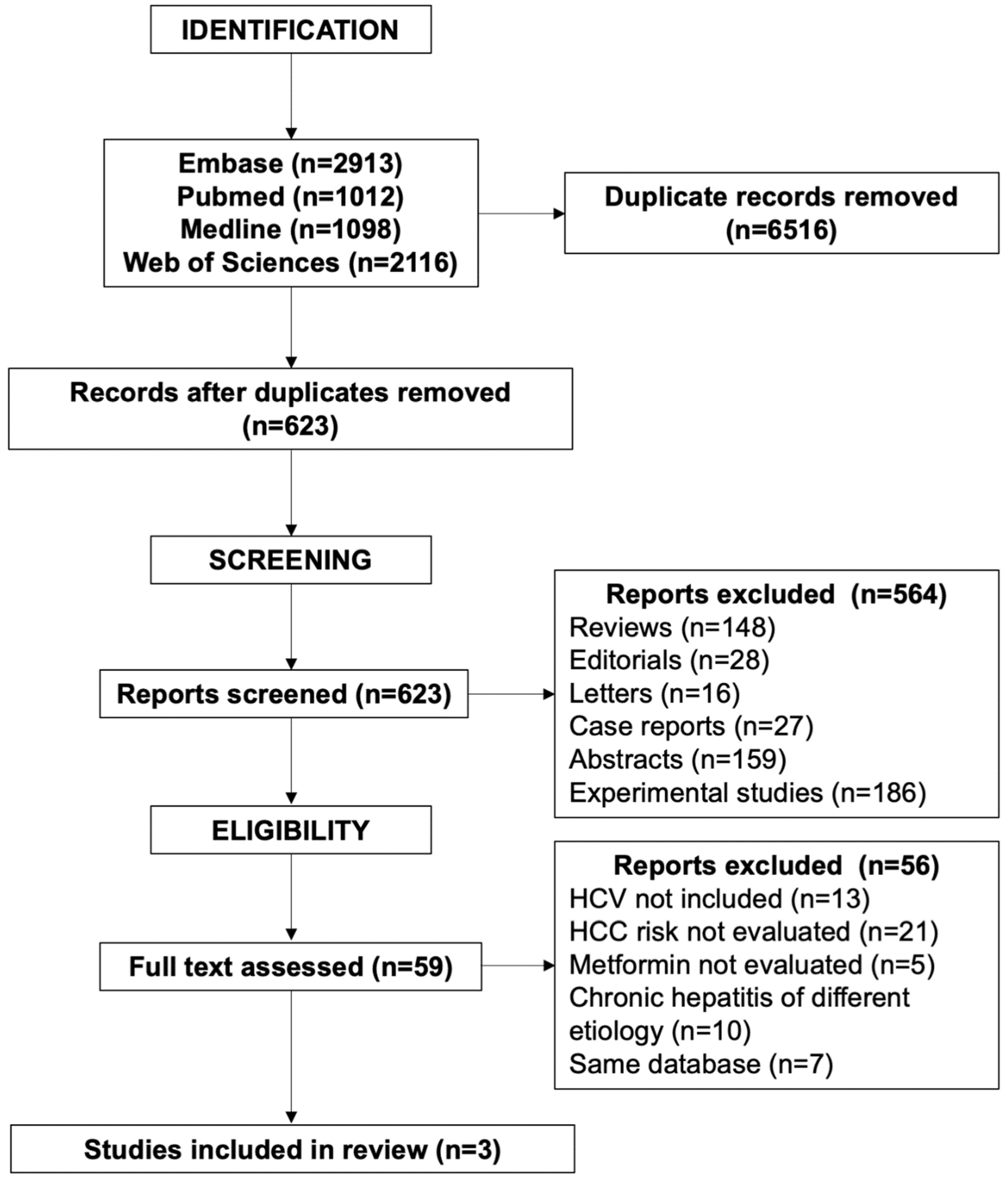
2. Methods
3. Results
3.1. Diabetic Patients with Untreated CHC or Non-Responders to Antiviral Therapy
3.2. Diabetic Patients with CHC Successfully Treated with Antiviral Therapy
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Davila, J.A.; Morgan, R.O.; Shaib, Y.; McGlynn, K.A.; El-Serag, H.B. Diabetes increases the risk of hepatocellular carcinoma in the United States: A population based case control study. Gut 2005, 54, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Van der Meer, A.J.; Feld, J.J.; Hofer, H.; Almasio, P.L.; Calvaruso, V.; Fernandez-Rodriguez, C.M.; Aleman, S.; Ganne-Carrié, N.; D’Ambrosio, R.; Pol, S.; et al. Risk of cirrhosis-related complications in patients with advanced fibrosis following hepatitis C virus eradication. J. Hepatol. 2017, 66, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Nahon, P.; Bourcier, V.; Layese, R.; Audureau, E.; Cagnot, C.; Marcellin, P.; Guyader, D.; Fontaine, H.; Larrey, D.; De Lédinghen, V.; et al. Eradication of hepatitis C virus infection in patients with cirrhosis reduces risk of liver and non-liver complications. Gastroenterology 2017, 152, 142–156. [Google Scholar] [CrossRef] [PubMed]
- Toyoda, H.; Kumada, T.; Tada, T.; Kiriyama, S.; Tanikawa, M.; Hisanaga, Y.; Kanamori, A. Risk factors of hepatocellular carcinoma development in non-cirrhotic patients with sustained virologic response for chronic hepatitis C virus infection. J. Gastroenterol. Hepatol. 2015, 30, 1163–1189. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.F.; Yeh, M.L.; Huang, C.Y.; Tsai, P.C.; Ko, Y.M.; Chen, K.Y.; Lin, Z.Y.; Chen, S.C.; Dai, C.Y.; Chuang, W.L.; et al. Pretreatment glucose status determines HCC development in HCV patients with mild liver disease after curative antiviral therapy. Medicine 2016, 95, e4157. [Google Scholar] [CrossRef] [PubMed]
- Hung, C.H.; Lee, C.M.; Wang, J.H.; Hu, T.H.; Chen, C.H.; Lin, C.Y.; Lu, S.N. Impact of diabetes mellitus on incidence of hepatocellular carcinoma in chronic hepatitis C patients treated with interferon-based antiviral therapy. Int. J. Cancer 2011, 128, 2344–2352. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, H.B.; Kanwal, F.; Richardson, P.; Kramer, J. Risk of hepatocellular carcinoma after sustained virological response in veterans with hepatitis C virus infection. Hepatology 2016, 64, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Hedenstierna, M.; Nangarhari, A.; Weiland, O.; Aleman, S. Diabetes and cirrhosis are risk factors for hepatocellular carcinoma after successful treatment of chronic hepatitis C. Clin. Infect. Dis. 2016, 63, 723–729. [Google Scholar] [CrossRef]
- Matsuura, K.; Sawai, H.; Ikeo, K.; Ogawa, S.; Iio, E.; Isogawa, M.; Shimada, N.; Komori, A.; Toyoda, H.; Kumada, T.; et al. Genome-wide association study identifies TLL1 variant associated with development of hepatocellular carcinoma after eradication of hepatitis C virus infection. Gastroenterology 2017, 152, 1383–1394. [Google Scholar] [CrossRef]
- Arase, Y.; Kobayashi, M.; Suzuki, F.; Suzuki, Y.; Kawamura, Y.; Akuta, N.; Kobayashi, M.; Sezaki, H.; Saito, S.; Hosaka, T.; et al. Effect of type 2 diabetes on risk for malignancies includes hepatocellular carcinoma in chronic hepatitis C. Hepatology 2013, 57, 964–973. [Google Scholar] [CrossRef]
- Yen, Y.H.; Lin, M.T.; Kuo, F.Y.; Chang, K.C.; Tsai, M.C.; Tseng, P.L.; Wu, C.K.; Lin, J.T.; Hu, T.H.; Lu, S.N.; et al. The association between steatosis and diabetes with hepatocellular carcinoma in non-genotype 3 chronic hepatitis C patients. Liver Intern. 2018, 38, 1064–1073. [Google Scholar] [CrossRef] [PubMed]
- Lockart, I.; Yeo, M.G.H.; Hajarizadeh, B.; Dore, G.J.; Danta, M. HCC incidence after hepatitis C cure among patients with advanced fibrosis or cirrhosis: A meta-analysis. Hepatology 2022, 76, 139–154. [Google Scholar] [CrossRef] [PubMed]
- Doyle, M.A.; Galanakis, C.; Mulvihill, E.; Crawley, A.; Cooper, C.L. Hepatitis C direct acting antivirals and ribavirin modify lipid but not glucose parameters. Cells 2019, 8, 252. [Google Scholar] [CrossRef] [PubMed]
- Di Marco, V.; Calvaruso, V.; Ferraro, D.; Bavetta, M.G.; Cabibbo, G.; Conte, E.; Cammà, C.; Grimaudo, S.; Pipitone, R.M.; Simone, F.; et al. Effects of eradicating hepatitis C virus infection in patients with cirrhosis differ with stage of portal hypertension. Gastroenterology 2016, 151, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Kozbial, K.; Moser, S.; Al-Zoairy, R.; Schwarzer, R.; Datz, C.; Stauber, R.; Laferl, H.; Strasser, M.; Beinhardt, S.; Stättermayer, A.F.; et al. Follow-up of sustained virological responders with hepatitis C and advanced liver disease after interferon/ribavirin-free treatment. Liver Intern. 2018, 38, 1028–1035. [Google Scholar] [CrossRef] [PubMed]
- Calvaruso, V.; Cabibbo, G.; Cacciola, I.; Petta, S.; Madonia, S.; Bellia, A.; Tinè, F.; Distefano, M.; Licata, A.; Giannitrapani, L.; et al. Incidence of hepatocellular carcinmoma in patients with HCV-associated cirrhosis treated with direct-acting antiviral agents. Gastroenterology 2018, 155, 411–421. [Google Scholar] [CrossRef] [PubMed]
- Marino, Z.; Darnell, A.; Lens, S.; Sapena, V.; Diaz, A.; Belmonte, E.; Perellò, C.; Calleja, J.L.; Varela, M.; Rodriguez, M.; et al. Time association between hepatitis C therapy and hepatocellular carcinoma emergence in cirrhosis: Relevance of non-characterized nodules. J. Hepatol. 2019, 70, 874–884. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, E.; Furusyo, N.; Nomura, H.; Dohmen, K.; Higashi, N.; Takahashi, K.; Kawano, A.; Azuma, K.; Satoh, T.; Nakamuta, M.; et al. Short-term risk of hepatocellular carcinoma after hepatitis C virus eradication following direct-acting anti-viral treatment. Aliment. Pharmacol. Ther. 2018, 47, 104–113. [Google Scholar] [CrossRef]
- Nahon, P.; Layese, R.; Bourcier, V.; Cagnot, C.; Marcellin, P.; Guyader, D.; Pol, S.; Larrey, D.; De Lédinghen, V.; Ouzan, D.; et al. Incidence of hepatocellular carcinoma after direct antiviral therapy for HCV in patients with cirrhosis included in surveillance programs. Gastroenterology 2018, 155, 1436–1450. [Google Scholar] [CrossRef]
- Innes, H.; Barclay, S.T.; Hayes, P.C.; Fraser, A.; Dillon, J.F.; Stanley, A.; Bathgate, A.; McDonald, S.A.; Goldberg, D.; Valerio, H.; et al. The risk of hepatocellular carcinoma in cirrhotic patients with hepatitis C and sustained viral response: The role of the treatment regimen. J. Hepatol. 2018, 68, 646–654. [Google Scholar] [CrossRef]
- Kanwal, F.; Kramer, J.; Asch, S.M.; Cao, Y.; Li, L.; El-Serag, H.B. Long-term risk of hepatocellular carcinoma in HCV patients treated with direct acting antiviral agents. Hepatology 2020, 71, 44–55. [Google Scholar] [CrossRef] [PubMed]
- Shiha, G.; Mousa, N.; Soliman, R.; Mikhail, N.N.; Adel Elbasiony, M.; Khattab, M. Incidence of HCC in chronic hepatitis C patients with advanced hepatic fibrosis who achieved SVR following DAAs: A prospective study. J. Viral Hepat. 2020, 27, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Azzi, J.; Dorival, C.; Cagnot, C.; Fontaine, H.; Lusivika-Nzinga, C.; Leroy, V.; De Ledinghen, V.; Tran, A.; Zoulim, F.; Alric, L.; et al. Prediction of hepatocellular carcinoma in hepatitis C patients with advanced fibrosis after sustained virologic response. Clin. Res. Hepatol. Gastroenterol. 2022, 46, 101923. [Google Scholar] [CrossRef] [PubMed]
- Tahata, Y.; Sakamori, R.; Yamada, R.; Kodama, T.; Hikita, H.; Nozaki, Y.; Oshita, M.; Hiramatsu, N.; Miyazaki, M.; Mita, E.; et al. Risk of hepatocellular carcinoma after sustained virologic response in hepatitis C virus patients without advanced liver fibrosis. Hepatol. Res. 2022, 52, 824–832. [Google Scholar] [CrossRef] [PubMed]
- Romano, A.; Angeli, P.; Piovesan, S.; Noventa, F.; Anastassopoulos, G.; Chemello, L.; Cavalletto, L.; Gambato, M.; Russo, F.P.; Burra, P.; et al. Newly diagnosed hepatocellular carcinoma in patients with advanced hepatitis C treated with DAAs: A prospective population study. J. Hepatol. 2018, 69, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Singer, A.W.; Reddy, K.R.; Telep, L.E.; Osinusi, A.O.; Brainard, D.M.; Buti, M.; Chokkalingam, A.P. Direct-acting antiviral treatment for hepatitis C virus infection and risk of incident liver cancer: A retrospective cohort study. Aliment. Pharmacol. Ther. 2018, 47, 1278–1287. [Google Scholar] [CrossRef] [PubMed]
- Mecci, A.J.; Kemos, P.; Leen, C.; Lawson, A.; Richardson, P.; Khakoo, S.I.; Agarwal, K.; Mutimer, D.; Rosenberg, W.M.; Foster, G.R.; et al. The association between hepatocellular carcinoma and direct-acting anti-viral treatment in patients with decompensated cirrhosis. Aliment. Pharmacol. Ther. 2019, 50, 204–214. [Google Scholar] [CrossRef] [PubMed]
- Degasperi, E.; D’Ambrosio, R.; Iavarone, M.; Sangiovanni, A.; Aghemo, A.; Soffredini, R.; Borghi, M.; Lunghi, G.; Colombo, M.; Lampertico, P. Factors associated with increased risk of de novo or recurrent hepatocellular carcinoma in patients with cirrhosis treated with direct-acting antivirals for HCV infection. Clin. Gastroenterol. Hepatol. 2019, 17, 1183–1191. [Google Scholar] [CrossRef]
- Rinaldi, L.; Perrella, A.; Guarino, M.; De Luca, M.; Piai, G.; Coppola, N.; Pafundi, P.C.; Ciardiello, F.; Fasano, M.; Martinelli, E. Incidence and risk factors of early HCC occurrence in HCV patients treated with direct-acting antivirals: A prospective multicentre study. J. Transl. Med. 2019, 17, 292. [Google Scholar] [CrossRef]
- Abe, K.; Wakabayashi, H.; Nakayama, H.; Suzuki, T.; Kuroda, M.; Yoshida, N.; Tojo, J.; Kogure, A.; Rai, T.; Saito, H.; et al. Factors associated with hepatocellular carcinoma occurrence after HCV eradication in patients without cirrhosis or with compensated cirrhosis. PLoS ONE 2020, 12, e0243473. [Google Scholar] [CrossRef]
- Ciancio, A.; Ribaldone, D.; Dotta, A.; Giordanino, C.; Sacco, M.; Fagoonee, S.; Pellicano, R.; Saracco, G.M. Long-term follow-up of diabetic and non-diabetic patients with chronic hepatitis C successfully treated with direct-acting antiviral agents. Liver Intern. 2021, 41, 276–287. [Google Scholar] [CrossRef] [PubMed]
- Kumada, T.; Toyoda, H.; Yasuda, S.; Ito, T.; Tsuji, K.; Fujioka, S.; Hiraoka, A.; Kariyama, K.; Nouso, K.; Ishikawa, T.; et al. Factors linked to hepatocellular carcinoma development beyond 10 years after viral eradication in patients with hepatitis C virus. J. Viral Hepat. 2022, 29, 919–929. [Google Scholar] [CrossRef] [PubMed]
- Kramer, J.R.; Cao, Y.; Li, L.; Smith, D.; Chhatwal, J.; El-Serag, H.; Kanwal, F. Longitudinal association of risk factors and hepatocellular carcinoma in patients with cured Hepatitis C Virus infection. Am. J. Gastroenterol. 2022, 117, 1834–1844. [Google Scholar] [CrossRef]
- Nkontchou, G.; Cosson, E.; Aout, M.; Mahmoudi, A.; Bourcier, V.; Charif, I.; Ganne-Carrie, N.; Grando-Lemaire, V.; Vicaut, E.; Trinchet, J.C.; et al. Impact of metformin on the prognosis of cirrhosis induced by viral hepatitis C in diabetic patients. J. Clin. Endocrinol. Metab. 2011, 96, 2601–2608. [Google Scholar] [CrossRef] [PubMed]
- Lai, S.W.; Chen, P.C.; Liao, K.F.; Muo, C.H.; Lin, C.C.; Sung, F.C. Risk of hepatocellular carcinoma in diabetic patients and risk reduction associated with anti-diabetic therapy: A population-based cohort study. Am. J. Gastroenterol. 2012, 107, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H. Metformin and risk of hepatocellular carcinoma in patients with type 2 diabetes. Liver Intern. 2018, 38, 2018–2027. [Google Scholar] [CrossRef]
- Zhang, X.; Harmsen, W.S.; Mettler, T.A.; Kim, W.R.; Roberts, R.O.; Therneau, T.M.; Roberts, L.R.; Chaiteerakij, R. Continuation of metformin use after a diagnosis of cirrhosis significantly improves survival of patients with diabetes. Hepatology 2014, 60, 2008–2016. [Google Scholar] [CrossRef]
- Donadon, V.; Balbi, M.; Mas, M.D.; Casarin, P.; Zanette, G. Metformin and reduced risk hepatocellular carcinoma in diabetic patients with chronic liver disease. Liver Int. 2010, 30, 750–758. [Google Scholar] [CrossRef]
- Hassan, M.M.; Curley, S.A.; Li, D.; Kaseb, A.; Davila, M.; Abdalla, E.K.; Javle, M.; Moghazy, D.M.; Lozano, R.D.; Abbruzzese, J.L.; et al. Association of diabetes duration and diabetes treatment with the risk of hepatocellular carcinoma. Cancer 2010, 116, 1938–1946. [Google Scholar] [CrossRef]
- Ruiter, R.; Visser, L.E.; van Herk-Sukel, M.P.; Coebergh, J.W.; Haak, H.R.; Geelhoed-Duijvestijn, P.H.; Straus, S.M.; Herings, R.M.; Stricker, B.H. Lower risk of cancer in patients on metformin in comparison with those on sulfonylurea derivatives: Results from a large population-based follow-up study. Diabetes Care 2012, 35, 119–124. [Google Scholar] [CrossRef]
- Kasmari, A.J.; Welch, A.; Liu, G.; Leslie, D.; McGarrity, T.; Riley, T. Independent of cirrhosis hepatocellular carcinoma risk is increased with diabetes and metabolic syndrome. Am. J. Med. 2017, 130, 746–747. [Google Scholar] [CrossRef] [PubMed]
- Miele, L.; Bosetti, C.; Turati, F.; Rapaccini, G.; Gasbarrini, A.; La Vecchia, C.; Boccia, S.; Grieco, A. Diabetes and insulin therapy, but not metformin, are related to hepatocellular cancer risk. Gastroenterol. Res. Pract. 2015, 2015, 570356. [Google Scholar] [CrossRef] [PubMed]
- Bosetti, C.; Franchi, M.; Nicotra, F.; Asciutto, R.; Merlino, L.; La Vecchia, C.; Corrao, G. Insulin and other antidiabetic drugs and hepatocellular carcinoma risk: A nested case-control study based on Italian healthcare utilization databases. Pharmacoepidemiol. Drug Saf. 2015, 24, 771–778. [Google Scholar] [CrossRef] [PubMed]
- Cunha, V.; Cotrim, H.P.; Rocha, R.; Carvalho, K.; Lins-Kusterer, L. Metformin in the prevention of hepatocellular carcinoma in diabetic patients: A systematic review. Ann. Hepatol. 2020, 19, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Zeng, R.W.; Yong, J.N.; Tan, D.J.H.; Fu, C.E.; Lim, W.H.; Xiao, J.; Chan, K.E.; Tan, C.; Goh, X.L.; Chee, D.; et al. Meta-analysis: Chemoprevention of hepatocellular carcinoma with statins, aspirin and metformin. Aliment. Pharmacol. Ther. 2023, 57, 600–609. [Google Scholar] [CrossRef] [PubMed]
- DeFronzo, R.A. Pharmacologic therapy for type 2 diabetes mellitus. Ann. Intern. Med. 1999, 131, 281–303. [Google Scholar] [CrossRef] [PubMed]
- Bhat, A.; Sebastiani, G.; Bhat, M. Systematic review: Preventive and therapeutic applications of metformin in liver disease. World J. Hepatol. 2015, 7, 1652–1659. [Google Scholar] [CrossRef]
- Luo, Z.; Zang, M.; Guo, M. AMPK as a metabolic tumor suppressor: Control of metabolism and cell growth. Future Oncol. 2010, 6, 457–470. [Google Scholar] [CrossRef]
- Schimmak, G.; Defronzo, R.A.; Must, N. AMP-activated protein kinase: Role in metabolism and therapeutic implicatoins. Diabetes Obes. Metab. 2006, 8, 591–602. [Google Scholar] [CrossRef]
- Lin, D.; Reddy, V.; Osman, H.; Lopez, A.; Koksal, A.R.; Rhadhi, S.M.; Dash, S.; Aydin, Y. Additional inhibition of Wnt/β-catenin signalling by metformin in DAA treatments as a novel therapeutic strategy for HCV-infected patients. Cells 2021, 10, 790. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Open Med. 2009, 3, e123–e130. [Google Scholar] [PubMed]
- Tsai, P.C.; Kuo, H.T.; Hung, C.H.; Tseng, K.C.; Lai, H.C.; Peng, C.Y.; Wang, J.H.; Chen, J.J.; Lee, P.L.; Chien, R.N.; et al. Metformin reduces hepatocellular carcinoma incidence after successful antiviral therapy in patients with diabetes and chronic hepatitis C in Taiwan. J. Hepatol. 2023, 78, 281–292. [Google Scholar] [CrossRef] [PubMed]
- Valenti, L.; Pelusi, S.; Aghemo, A.; Gritti, S.; Pasulo, L.; Bianco, C.; Iegri, C.; Cologni, G.; Degasperi, E.; D’Ambrosio, R.; et al. Dysmetabolism, diabetes and clinical outcomes in patients cured of chronic hepatitis C: A real-life cohort study. Hepatol. Commun. 2022, 6, 867–877. [Google Scholar] [CrossRef] [PubMed]
- European Association for the study of the Liver EASL recommendations on treatment of Hepatitis, C. Final update of the series. J. Hepatol. 2020, 73, 1170–1218. [Google Scholar] [CrossRef] [PubMed]
- Donadon, V.; Balbi, M.; Valent, F.; Avogaro, A. Glycated haemoglobin and antidiabetic strategies as risk factors for hepatocellular carcinoma. World J. Gastroenterol. 2010, 16, 3025–3032. [Google Scholar] [CrossRef] [PubMed]
- Caviglia, G.P.; Troshina, G.; Santaniello, U.; Rosati, G.; Bombaci, F.; Birolo, G.; Nicolosi, A.; Saracco, G.M.; Ciancio, A. Long-term hepatocellular carcinoma development and predictive ability of non-invasive scoring systems in patients with HCV-related cirrhosis treated with direct-acting antivirals. Cancers 2022, 14, 828. [Google Scholar] [CrossRef] [PubMed]
- Ciancio, A.; Ribaldone, D.G.; Spertino, M.; Risso, A.; Ferrarotti, D.; Caviglia, G.P.; Carucci, P.; Gaia, S.; Rolle, E.; Sacco, M.; et al. Who should not be surveilled for HCC development after successful therapy with DAAs in advanced chronic hepatitis C? Results of a long-term prospective study. Biomedicines 2023, 11, 166. [Google Scholar] [CrossRef]
- Pons, M.; Rodriguez-Tajes, S.; Esteban, J.I.; Marino, Z.; Vargas, V.; Lens, S.; Buti, M.; Augustin, S.; Forns, X.; Mínguez, B.; et al. Non-invasive prediction of liver-related events in patients with HCV-associated compensated advanced chronic liver disease after oral antivirals. J. Hepatol. 2020, 72, 472–480. [Google Scholar] [CrossRef]
- Semmler, G.; Meyer, E.L.; Kozbial, K.; Schwabl, P.; Hametner-Schreil, S.; Zanetto, A.; Bauer, D.; Chromy, D.; Simbrunner, B.; Scheiner, B.; et al. HCC risk stratification after cure of hepatitis C in patients with compensated advanced chronic liver disease. J. Hepatol. 2022, 76, 812–821. [Google Scholar] [CrossRef]
- Smith, F.C.; Stocker, S.L.; Danta, M.; Carland, J.E.; Kumar, S.S.; Liu, Z.; Greenfield, J.R.; Braithwaite, H.E.; Cheng, T.S.; Graham, G.G.; et al. The safety and pharmacokinetics of metformin in patients with chronic liver disease. Aliment. Pharmacol. Ther. 2020, 51, 565–575. [Google Scholar] [CrossRef]

{kind=link}
| Author, Year (Reference) | Nkontchou, 2011 [34] | Tsai, 2023 [52] | Valenti, 2022 [53] |
|---|---|---|---|
| Type of study | Observational | Observational | Observational |
| Design | Prospective | Retrospective | Retrospective |
| HCV-cured patients | NO | YES | YES |
| Diabetic patients, n | 100 | 781 | 725 |
| Cirrhosis, % | 100% | 10.2% | 78.6% |
| Median follow-up, years | 5.7 | 4.4 | 2.0 |
| MET users, % | 26% | 82.8% | 49.4% |
| HCC incidence MET vs. non-MET users, HR [CI]; p | 0.22 [0.05–0.97]; p = 0.046 | 2.84 [1.49–5.40]; p = 0.002 | 0.24 [0.07–0.87]; p = 0.0029 |
| Propensity score | YES | YES | YES |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sacco, M.; Ribaldone, D.G.; Saracco, G.M. Metformin and Hepatocellular Carcinoma Risk Reduction in Diabetic Patients with Chronic Hepatitis C: Fact or Fiction? Viruses 2023, 15, 2451. https://doi.org/10.3390/v15122451
Sacco M, Ribaldone DG, Saracco GM. Metformin and Hepatocellular Carcinoma Risk Reduction in Diabetic Patients with Chronic Hepatitis C: Fact or Fiction? Viruses. 2023; 15(12):2451. https://doi.org/10.3390/v15122451
Chicago/Turabian StyleSacco, Marco, Davide Giuseppe Ribaldone, and Giorgio Maria Saracco. 2023. "Metformin and Hepatocellular Carcinoma Risk Reduction in Diabetic Patients with Chronic Hepatitis C: Fact or Fiction?" Viruses 15, no. 12: 2451. https://doi.org/10.3390/v15122451
APA StyleSacco, M., Ribaldone, D. G., & Saracco, G. M. (2023). Metformin and Hepatocellular Carcinoma Risk Reduction in Diabetic Patients with Chronic Hepatitis C: Fact or Fiction? Viruses, 15(12), 2451. https://doi.org/10.3390/v15122451