
Comparative Performance of Serological (IgM/IgG) and Molecular Testing (RT-PCR) of COVID-19 in Three Private Universities in Cameroon during the Pandemic

 ,
,  , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
- A.
- Study Design and Population
- B.
- Ethics Approval and Consent
- C.
- Determination of Minimum Sample Size
- D.
- Sample Collection and Conservation
- Blood Sampling
- Nasopharyngeal sampling
- Samples Transportation
- COVID-19 Testing
- E.
- Data Analysis
3. Results
3.1. Determination of Baseline Characteristics of the Study Population
3.2. Prevalence of SARS-CoV-2 in Students and Associated Risk Factors
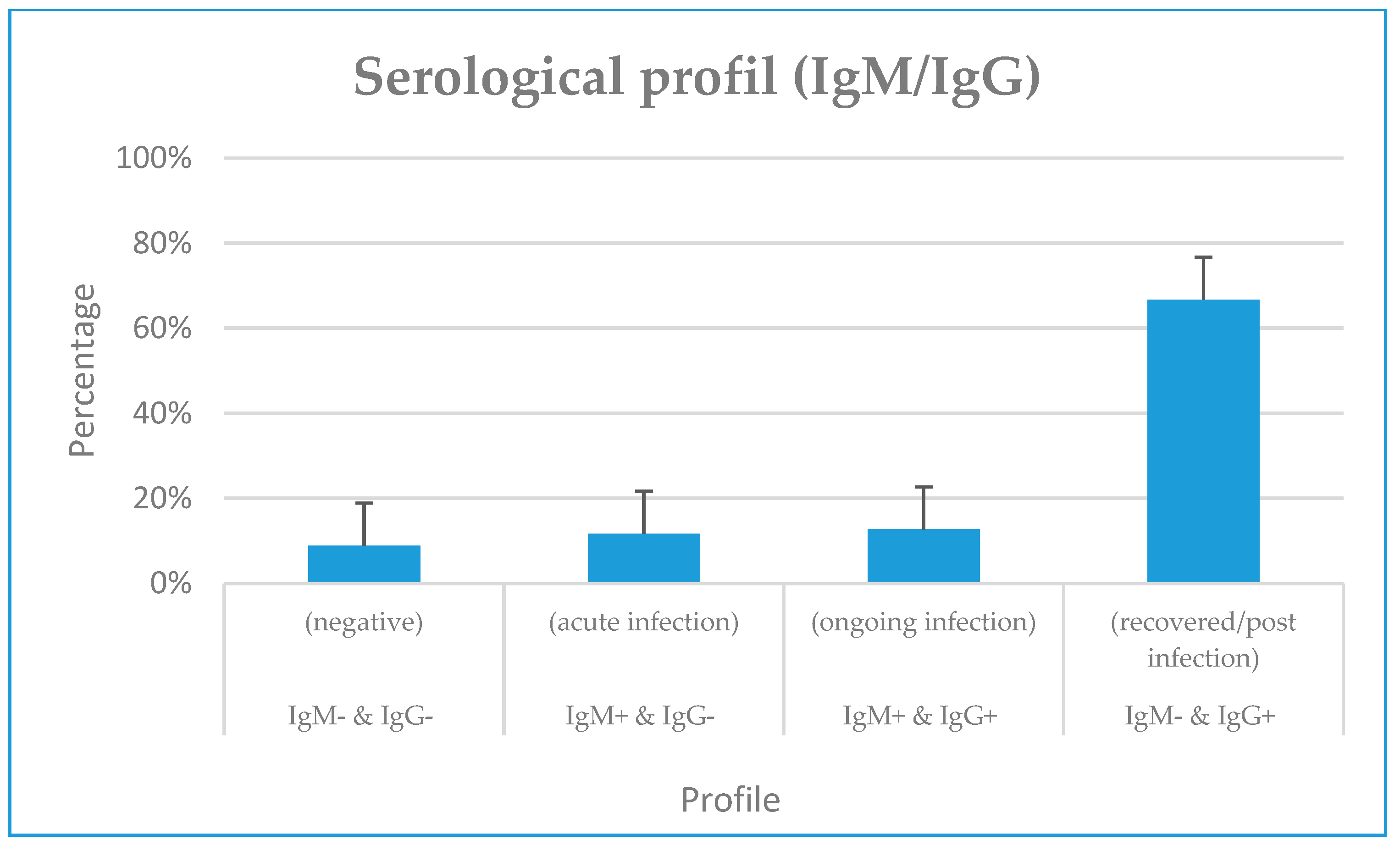
3.3. IgM/IgG Serological Profile and Their Associated Factors
3.4. IgM/IgG Serological Profile and SARS-CoV-2 RNA Detection
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Caeseele, P.; Bailey, D.; Forgie, S.E.; Dingle, T.C.; Krajden, M. SARS-CoV-2 (COVID-19) serology: Implications for clinical practice, laboratory medicine and public health. Can. Med. Assoc. J. 2020, 192, E973. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Zhao, J.; Yuan, Q.; Wang, H.; Liu, W.; Liao, X.; Su, Y.; Wang, X.; Yuan, J.; Li, T.; Li, J.; et al. Antibody Responses to SARS-CoV-2 in Patients With Novel Coronavirus Disease 2019. Clin. Infect. Dis. 2020, 71, 2027–2034. [Google Scholar] [CrossRef]
- Oran, D.P.; Topol, E.J. Prevalence of asymptomatic SARS-CoV-2 infection: A narrative review. Ann. Intern. Med. 2020, 173, 362–367. [Google Scholar] [CrossRef] [PubMed]
- WHO. Weekly Epidemiological Update on COVID-19-30 November 2022, Edition 120, 30 November 2022, Emergency Situational Updates. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---30-november-2022 (accessed on 16 January 2023).
- Johns Hopkins University of Medicine, Mortality Analyses, Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/data/mortality (accessed on 16 January 2023).
- WHO. Africa, The Future of WHO Covid-19 Response Operations in Africa in 2022. Available online: https://www.afro.who.int/publications/future-who-covid-19-response-operations-africa-2022 (accessed on 16 January 2023).
- Rabi, F.A.; Al Zoubi, M.S.; Kasasbeh, G.A.; Salameh, D.M.; Al-Nasser, A.D. SARS-CoV-2 and Coronavirus Disease 2019: What We Know So Far. Pathogens 2020, 9, 231. [Google Scholar] [CrossRef] [PubMed]
- Bonny, V.; Maillard, A.; Mousseaux, C.; Plaçais, L.; Richier, Q. COVID-19: Physiopathologie d’une maladie à plusieurs visages. La Rev. De Médecine Interne 2020, 41, 375–389. [Google Scholar] [CrossRef] [PubMed]
- CDC COVID-19 Science Briefs, Science Brief: Transmission of SARS-CoV-2 in K-12 Schools and Early Care and Education Programs—Updated, 17 December 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK570438/ (accessed on 17 January 2023).
- Ravens-Sieberer, U.; Kaman, A.; Erhart, M.; Devine, J.; Schlack, R.; Otto, C. Impact of the COVID-19 pandemic on quality of life and mental health in children and adolescents in Germany. Eur. Child Adolesc. Psychiatry 2021, 31, 879–889. [Google Scholar] [CrossRef]
- Goldstein, E.; Lipsitch, M.; Cevik, M. On the Effect of Age on the Transmission of SARS-CoV-2 in Households, Schools, and the Community. J. Infect. Dis. 2021, 223, 362–369. [Google Scholar] [CrossRef]
- National Centre for Immunisation Research and Surveillance. COVID-19 in Schools and Early Childhood Education and Care Services—The Term 3 Experience in NSW. Report from National Centre for Immunisation Research and Surveillance. 9 October 2020. Available online: https://www.ncirs.org.au/sites/default/files/2020-10/COVID-19%20Transmission%20in%20educational%20settings%20in%20NSW%20Term%203%20report_0.pdf (accessed on 30 June 2021).
- Larosa, E.; Djuric, O.; Cassinadri, M.; Cilloni, S.; Bisaccia, E.; Vicentini, M.; Venturelli, F.; Rossi, P.G.; Pezzotti, P.; Bedeschi, E.; et al. Secondary transmission of COVID-19 in preschool and school settings in northern Italy after their reopening in September 2020: A population-based study. Eurosurveillance 2020, 25, 2001911. [Google Scholar] [CrossRef]
- Murillo-Llorente, M.T.; Perez-Bermejo, M. COVID-19: Social Irresponsibility of Teenagers Towards the Second Wave in Spain. J. Epidemiol. 2020, 30, 483. [Google Scholar] [CrossRef]
- Zhu, Y.; Bloxham, C.J.; Hulme, K.D.; Sinclair, J.E.; Tong, Z.W.M.; Steele, L.E.; Noye, E.C.; Lu, J.; Xia, Y.; Chew, K.Y.; et al. A Meta-analysis on the Role of Children in Severe Acute Respiratory Syndrome Coronavirus 2 in Household Transmission Clusters. Clin. Infect. Dis. 2021, 72, e1146–e1153. [Google Scholar] [CrossRef]
- Hobbs, C.V.; Drobeniuc, J.; Kittle, T.; Williams, J.; Byers, P.; Satheshkumar, P.S.; Inagaki, K.; Stephenson, M.; Kim, S.S.; Patel, M.M.; et al. Estimated SARS-CoV-2 Seroprevalence Among Persons Aged <18 Years-Mississippi, May-September 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 312–315. [Google Scholar] [PubMed]
- Kim, D.H.; Kim, D.; Moon, J.W.; Chae, S.-W.; Rhyu, I.J. Complications of Nasopharyngeal Swabs and Safe Procedures for COVID-19 Testing Based on Anatomical Knowledge. J. Korean Med. Sci. 2022, 37, e88. [Google Scholar] [CrossRef]
- Marty, F.M.; Chen, K.; Verrill, K.A. How to Obtain a Nasopharyngeal Swab Specimen. N. Engl. J. Med. 2020, 383, e14. [Google Scholar] [CrossRef] [PubMed]
- Di Maio, P.; Iocca, O.; Cavallero, A.; Giudice, M. Performing the nasopharyngeal and oropharyngeal swab for 2019-novel coronavirus (SARS-CoV-2) safely: How to dress, undress, and technical notes. Head Neck 2020, 42, 1548–1551. [Google Scholar] [CrossRef]
- Batra, R.; Olivieri, L.G.; Rubin, D.; Vallari, A.; Pearce, S.; Olivo, A.; Prostko, J.; Nebbia, G.; Douthwaite, S.; Rodgers, M.; et al. A comparative evaluation between the Abbott PanbioTM COVID-19 IgG/IgM rapid test device and Abbott ArchitectTM SARS CoV-2 IgG assay. J. Clin. Virol. 2020, 132, 104645. [Google Scholar] [CrossRef] [PubMed]
- Yamada, S.; Fukushi, S.; Kinoshita, H.; Ohnishi, M.; Suzuki, T.; Fujimoto, T.; Saijo, M.; Maeda, K. Virus Diagnosis Group (NIID Toyama. Assessment of SARS-CoV-2 infectivity of upper respiratory specimens from COVID-19 patients by virus isolation using VeroE6/TMPRSS2 cells. BMJ Open Respir. Res. 2021, 8, e000830. [Google Scholar] [CrossRef]
- Kim, Y.I.; Casel, M.A.B.; Kim, S.M.; Kim, S.G.; Park, S.J.; Kim, E.H.; Jeong, H.W.; Poo, H.; Choi, Y.K. Development of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) thermal inactivation method with preservation of diagnostic sensitivity. J. Microbiol. 2020, 58, 886–891. [Google Scholar] [CrossRef]
- Pratha, S.; Meagan, C.F.; Zimmer, C.F.; Abdollahi, E.; Juden-Kelly, L.; Moghadas, S.M.; Singer Burton, H.; Galvani, A.P. Asymptomatic SARS-CoV-2 infection: A systematic review and meta-analysis. Proc. Natl. Acad. Sci. USA 2021, 118, e2109229118. [Google Scholar] [CrossRef]
- Esso, L.; Epée, E.; Bilounga, C.; Abah, A.; Hamadou, A.; Dibongue, E.; Kamga, Y.; Belinga, S.; Eyangoh, S.; Okomo, M.C.; et al. Cameroon’s bold response to the COVID-19 pandemic during the first and second waves. Lancet Infect. Dis. 2021, 21, 1064–1065. [Google Scholar] [CrossRef]
- Abate, B.B.; Kassie, A.M.; Kassaw, M.W.; Aragie, T.G.; Masresha, S.A. Sex difference in coronavirus disease (COVID-19): A systematic review and meta-analysis. BMJ Open 2020, 10, e040129. [Google Scholar] [CrossRef]
- Doerre, A.; Doblhammer, G. The influence of gender on COVID-19 infections and mortality in Germany: Insights from age and gender-specific modeling of contact rates, infections, and deaths in the early phase of the pandemic. PLoS ONE 2022, 17, e0268119. [Google Scholar] [CrossRef] [PubMed]
- Griffith, D.M.; Sharma, G.; Holliday, C.S.; Enyia, O.K.; Valliere, M.; Semlow, A.R.; Stewart, E.C.; Blumenthal, R.S. Men and COVID-19: A Biopsychosocial Approach to Understanding Sex Differences in Mortality and Recommendations for Practice and Policy Interventions. Prev. Chronic Dis. 2020, 17, E63. [Google Scholar] [CrossRef] [PubMed]
- Perlis, R.H.; Santillana, M.; Ognyanova, K.; Safarpour, A.; Trujillo, K.L.; Simonson, M.D.; Green, J.; Quintana, A.; Druckman, J.; Baum, M.A.; et al. Prevalence and Correlates of Long COVID Symptoms Among US Adults. JAMA Netw. Open 2022, 5, e2238804. [Google Scholar] [CrossRef]
- Jin, J.M.; Bai, P.; He, W.; Wu, F.; Liu, X.F.; Han, D.M.; Liu, S.; Yang, J.K. Gender Differences in Patients With COVID-19: Focus on Severity and Mortality. Front. Public Health 2020, 8, 152. [Google Scholar] [CrossRef]
- Muller, C.P. Do asymptomatic carriers of SARS-COV-2 transmit the virus? Lancet Reg. Health–Eur. 2021, 4, 100082. [Google Scholar] [CrossRef]
- Chang, S.E.; Feng, A.; Meng, W.; Apostolidis, A.S.; Mack, E.; Artandi, M.; Barman, L.; Bennett, K.; Chakraborty, S.; Chang, I.; et al. New-onset IgG autoantibodies in hospitalized patients with COVID-19. Nat. Commun. 2021, 12, 5417. [Google Scholar] [CrossRef]
- Nguwoh, P.S.; Mboringong, A.B.; Fokam, J.; Ngounouh Taheu, C.; Halilou, I.; Djieudeu Nouwe, S.H.; Moussa, N.I.; Younouss, A.A.M.B.; Likeng, J.L.N.; Tchoffo, D.; et al. Seroprevalence of SARS-CoV-2 (COVID-19) among Health Care Workers in Three Health Facilities of Yaounde, Center Region of Cameroon. Eur. J. Med. Heal. Sci. 2021, 3, 89–94. [Google Scholar] [CrossRef]
- Nwosu, K.; Fokam, J.; Wanda, F.; Mama, L.; Orel, E.; Ray, N.; Meke, J.; Tassegning, A.; Takou, D.; Mimbe, E.; et al. SARS-CoV-2 antibody seroprevalence and associated risk factors in an urban district in Cameroon. Nat. Commun. 2021, 12, 5851. [Google Scholar] [CrossRef]
- Ndongo, F.A.; Guichet, E.; Mimbé, E.D.; Ndié, J.; Pelloquin, R.; Varloteaux, M.; Esemu, L.; Mpoudi-Etame, M.; Lamare, N.; Edoul, G.; et al. Rapid Increase of Community SARS-CoV-2 Seroprevalence during Second Wave of COVID-19, Yaoundé, Cameroon. Emerg. Infect. Dis. 2022, 28, 1233–1236. [Google Scholar] [CrossRef] [PubMed]
- Lobaloba Ingoba, L.; Djontu, J.C.; Mfoutou Mapangui, C.C.; Mouziga, F.; Diafouka, K.S.; Vouvoungui, C.; Kuisma, E.; Nguimbi, E.; Ntoumi, F. Seroprevalence of anti-SARS-CoV-2 antibodies in a population living in Bomassa village, Republic of Congo. IJID Reg. 2022, 2, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Lone, K.S.; Khan, S.M.S.; Qurieshi, M.A.; Majid, S.; Pandit, M.I.; Haq, I.; Ahmad, J.; Bhat, A.A.; Bashir, K.; Bilquees, S.; et al. Seroprevalence of SARS-CoV-2-specific anti-spike IgM, IgG, and anti-nucleocapsid IgG antibodies during the second wave of the pandemic: A population-based cross-sectional survey across Kashmir, India. Front. Public Heal. 2022, 10, 967447. [Google Scholar] [CrossRef] [PubMed]
- Borges, L.P.; Martins, A.F.; de Melo, M.S.; de Oliveira, M.G.B.; Neto, J.M.D.R.; Dósea, M.B.; Cabral, B.C.M.; Menezes, R.F.; Santos, A.A.; Matos, I.L.S.; et al. Seroprevalence of SARS-CoV-2 IgM and IgG antibodies in an asymptomatic population in Sergipe, Brazil. Rev. Panam. Salud. Publica. 2020, 44, e108. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Tanoira, R.; Lledó García, L.; Torralba González de Suso, M.; Rodríguez Zapata, M.; Arroyo Serrano, T.; Giménez Pardo, C.; Rodríguez Pedrosa, M.I.; Romero Badía, M.N.; Pérez-García, F.; González López, P.; et al. High Seroprevalence Against SARS-CoV-2 Among Faculty of Medicine and Health Sciences Personnel and Students of the University of Alcalá, Spain: Contributing Factors. Int. J. Gen. Med. 2021, 14, 7017–7024. [Google Scholar] [CrossRef] [PubMed]
- Machado, B.A.S.; Hodel, K.V.S.; Barbosa-Júnior, V.G.; Soares, M.B.P.; Badaró, R. The Main Molecular and Serological Methods for Diagnosing COVID-19: An Overview Based on the Literature. Viruses 2020, 13, 40. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Shi, H.; Han, X.; Jiang, N.; Cao, Y.; Alwalid, O.; Gu, J.; Fan, Y.; Zheng, C. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: A descriptive study. Lancet Infect. Dis. 2020, 20, 425–434. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan. China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Nakano, Y.; Kurano, M.; Morita, Y.; Shimura, T.; Yokoyama, R.; Qian, C.; Xia, F.; He, F.; Kishi, Y.; Okada, J.; et al. Time course of the sensitivity and specificity of anti-SARS-CoV-2 IgM and IgG antibodies for symptomatic COVID-19 in Japan. Sci. Rep. 2021, 11, 2776. [Google Scholar] [CrossRef]
- Lighter, J.; Phillips, M.; Hochman, S.; Sterling, S.; Johnson, D.; Francois, F.; Stachel, A. Profile of IgG and IgM antibodies against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Clin. Infect. Dis. 2020, 71, 896–897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, D.; Wu, T.; Liu, Q.; Yang, Z. The SARS-CoV-2 outbreak: What we know. Int. J. Infect. Dis. 2020, 94, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Li, L.Q.; Huang, T.; Wang, Y.Q.; Wang, Z.P.; Liang, Y.; Huang, T.B.; Zhang, H.Y.; Sun, W.M.; Wang, Y.P. novel coronavirus patients’ clinical characteristics, discharge rate and fatality rate of meta-analysis. J. Med. Virol. 2020, 92, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Sun, P.; Lu, X.; Xu, C.; Sun, W.; Pan, B. Understanding of COVID-19 based on current evidence. J. Med. Virol. 2020, 92, 548–551. [Google Scholar] [CrossRef] [PubMed]
- Pascarella, G.; Strumia, A.; Piliego, C.; Bruno, F.; Del Buono, R.; Costa, F.; Scarlata, S.; Agrò, F.E. COVID-19 diagnosis and management: A comprehensive review. J. Intern. Med. 2020, 288, 192–206. [Google Scholar] [CrossRef]
- CDC. Interim Guidelines for COVID-19 Antibody Testing in Clinical and Public Health Settings. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/testing/antibody-tests-guidelines.html (accessed on 16 December 2022).
- Katchunga, P.B.; Murhula, A.; Akilimali, P.; Zaluka, J.C.; Karhikalembu, R.; Makombo, M.; Bisimwa, J.; Mubalama, E. Seroprevalence of SARS-CoV-2 antibodies among travellers and workers screened at the Saint Luc Clinic in Bukavu, a city in eastern Democratic Republic of the Congo, from May to August 2020. Pan Afr. Med. J. 2021, 38, 93. [Google Scholar] [CrossRef]
- De Donno, A.; Lobreglio, G.; Panico, A.; Grassi, T.; Bagordo, F.; Bozzetti, M.P.; Massari, S.; Siculella, L.; Damiano, F.; Guerra, F.; et al. IgM and IgG Profiles Reveal Peculiar Features of Humoral Immunity Response to SARS-CoV-2 Infection. Int. J. Environ. Res. Public Health 2021, 18, 1318. [Google Scholar] [CrossRef]
- Meireles, P.; Costa, J.P.; Novais, M.J.; Miranda, D.; Lopes, M.M.; Severo, M.; Barros, H. The SARS-CoV-2 Infection Among Students in the University of Porto: A Cross-Sectional Study. Int. J. Public Health 2022, 67, 1604548. [Google Scholar] [CrossRef]
- Ozturk, T.; Howell, C.; Benameur, K.; Ramonell, R.P.; Cashman, K.; Pirmohammed, S.; Bassit, L.; Roback, J.; Marconi, V.C.; Schinazi, R.F.; et al. Cross-sectional IgM and IgG profiles in SARS-CoV-2 infection. medRxiv 2020. [CrossRef]
- Fernández-Rojas, M.A.; Luna-Ruiz Esparza, M.A.; Campos-Romero, A.; Calva-Espinosa, D.Y.; Moreno-Camacho, J.L.; Mendlovic, F.; Plett-Torres, T.; Alcántar-Fernández, J. Seroconversion dynamic and SARS-CoV-2 seropositivity in unvaccinated population during the first and second outbreaks in Mexico. Sci. Rep. 2022, 12, 5241. [Google Scholar] [CrossRef]
- Munitz, A.; Edry-Botzer, L.; Itan, M.; Tur-Kaspa, R.; Dicker, D.; Marcoviciu, D.; Goren, M.G.; Mor, M.; Lev, S.; Gottesman, T.; et al. Rapid seroconversion and persistent functional IgG antibodies in severe COVID-19 patients correlates with an IL-12p70 and IL-33 signature. Sci. Rep. 2021, 11, 3461. [Google Scholar] [CrossRef] [PubMed]
- Yadav, A.K.; Ghosh, S.; Kotwal, A.; Kaushik, S.K.; Bobdey, S.; Sahu, R.; Kapoor, S.; Faujdar, D.S.; Teli, P.T.; Anand, V. Seroconversion among COVID-19 patients admitted in a dedicated COVID hospital: A longitudinal prospective study of 1000 patients. Med. J. Armed Forces India 2021, 77, S379–S384. [Google Scholar] [CrossRef] [PubMed]
- Mohit, E.; Rostami, Z.; Vahidi, H. A comparative review of immunoassays for COVID-19 detection. Expert Rev. Clin. Immunol. 2021, 17, 573–599. [Google Scholar] [CrossRef] [PubMed]
- Gambino, C.M.; Lo Sasso, B.; Colomba, C.; Giglio, R.V.; Agnello, L.; Bivona, G.; Ciaccio, M. Comparison of a rapid immunochromatographic test with a chemiluminescence immunoassay for detection of anti-SARS-CoV-2 IgM and IgG. Biochem. Med. 2020, 30, 475–479. [Google Scholar] [CrossRef] [PubMed]
- Chansaenroj, J.; Yorsaeng, R.; Posuwan, N.; Puenpa, J.; Sudhinaraset, N.; Chirathaworn, C.; Poovorawan, Y. Detection of SARS-CoV-2-specific antibodies via rapid diagnostic immunoassays in COVID-19 patients. Virol. J. 2021, 18, 52. [Google Scholar] [CrossRef]
- Gong, F.; Wei, H.-X.; Li, Q.; Liu, L.; Li, B. Evaluation and Comparison of Serological Methods for COVID-19 Diagnosis. Front. Mol. Biosci. 2021, 8, 682405. [Google Scholar] [CrossRef]
- Andrey, D.O.; Cohen, P.; Meyer, B.; Torriani, G.; Yerly, S.; Mazza, L.; Calame, A.; Arm-Vernez, I.; Guessous, I.; Stringhini, S.; et al. Head-to-Head Accuracy Comparison of Three Commercial COVID-19 IgM/IgG Serology Rapid Tests. J. Clin. Med. 2020, 9, 2369. [Google Scholar] [CrossRef]


{kind=link}
| Variables | n | Percentage (%) | |
|---|---|---|---|
| Age range (year) | 18–21 | 81 | 27.84 |
| 21–24 | 120 | 41.24 | |
| 24–28 | 90 | 30.93 | |
| Gender | Male | 138 | 47.42 |
| Female | 153 | 52.58 | |
| Location | Yaounde | 93 | 31.96 |
| Bangangte | 198 | 68.04 | |
| Clinical status | Symptomatic | 57 | 19.59 |
| Asymptomatic | 234 | 80.41 | |
| Comorbidities | Yes | 12 | 4.12 |
| No | 279 | 95.88 | |
| Case-contact | Yes | 56 | 19.24 |
| No | 235 | 80.76 | |
| Nomadic 1 | Yes | 20 | 6.87 |
| No | 271 | 93.13 | |
| Treatment | Yes | 4 | 1.37 |
| No | 287 | 98.63 | |
| Variables | N | Positive PCR n(%) | ORa | 95%CI | p-Value |
|---|---|---|---|---|---|
| Age range (year) | |||||
| [18–21] | 81 | 15 (18.52) | Ref | ||
| [21–24] | 120 | 31 (25.83) | 1.81 | 0.8–3.7 | 0.11 |
| [24–28] | 90 | 16 (17.78) | 1.09 | 0.4–2.5 | 0.83 |
| Sexe | |||||
| Female | 153 | 44 (28.76) | Ref | ||
| Male | 138 | 18 (13.04) | 2.21 | 1.5–4.5 | 0.0007 |
| Location | |||||
| Bangangte | 198 | 50 (25.25) | Ref | ||
| Yaounde | 93 | 12 (12.90) | 1.95 | 1.2–3.8 | 0.01 |
| Clinical status | |||||
| Asymptomatic | 234 | 53 (22.65) | Ref | ||
| Symptomatic | 57 | 9 (15.79) | 0.64 | 0.3–1.4 | 0.2 |
| Comorbidities | |||||
| No | 279 | 58 (20.79) | Ref | ||
| Yes | 12 | 4 (33.33) | 1.14 | 0.3–4.3 | 0.84 |
| Case-contact | |||||
| No | 235 | 52 (22.13) | Ref | ||
| Yes | 56 | 10 (17.86) | 0.61 | 0.3–1.4 | 0.25 |
| Nomadic | |||||
| No | 271 | 57 (21.03) | Ref | ||
| Yes | 20 | 5 (25) | 1.82 | 0.5–6.1 | 0.33 |
| Treatment | |||||
| No | 287 | 61 (21.25) | Ref | ||
| Yes | 4 | 1 (25) | 1.70 | 0.15–18.7 | 0.66 |
| Variables | Total (N) | IgM+&IgG+ n(%) | p-Value | IgM+&IgG− n(%) | p-Value | IgM−&IgG+ n(%) | p-Value |
|---|---|---|---|---|---|---|---|
| Age range (year) | |||||||
| [18–21] | 81 | 8 (9.88) | Ref | 4 (4.94) | Ref | 13 (16.05) | Ref |
| [21–24] | 120 | 16 (13.33) | 0.26 | 11 (9.17) | 0.5 | 13 (10.83) | 0.31 |
| [24–28] | 90 | 10 (11.11) | 0.61 | 11 (12.22) | 0.21 | 11 (12.22) | 0.63 |
| Gender | |||||||
| Female | 153 | 24 (15.69) | Ref | 12 (7.84) | Ref | 19 (12.42) | Ref |
| Male | 138 | 10 (7.25) | 0.01 | 14 (10.14) | 0.77 | 18 (13.04) | 0.92 |
| Location | |||||||
| Bangangte | 198 | 28 (14.14) | Ref | 21 (10.61) | 23 (11.62 %) | Ref | |
| Yaounde | 93 | 6 (4.45) | 0.05 | 5 (5.38) | 0.11 | 14 (15.05 %) | 0.74 |
| Clinical status | |||||||
| Asymptomatic | 234 | 30 (12.82) | Ref | 21 (8.97) | Ref | 28 (11.97) | Ref |
| Symptomatic | 57 | 4 (7.02) | 0.15 | 5 (8.77) | 0.67 | 9 (15.79) | 0.6 |
| Comorbidities | |||||||
| No | 279 | 34 (12.19) | Ref | 23 (8.24) | Ref | 34 (12.19) | Ref |
| Yes | 12 | 0 (0.00) | 0.97 | 3 (25.00) | 0.12 | 3 (25.00) | 0.11 |
| Case-contact | |||||||
| No | 235 | 30 (12.77) | Ref | 19 (8.09) | Ref | 32 (13.62) | Ref |
| Yes | 56 | 4 (7.14) | 0.05 | 7 (12.50) | 0.9 | 5 (8.93) | 0.18 |
| Nomad | |||||||
| No | 271 | 30 (11.07) | Ref | 23 (8.49) | Ref | 34 (12.55) | Ref |
| Yes | 20 | 4 (20.00) | 0.01 | 3 (15.00) | 0.3 | 3 (15.00) | 0.21 |
| Treatment | |||||||
| No | 287 | 33 (11.50) | Ref | 25 (8.71) | Ref | 37 (12.89) | Ref |
| Yes | 4 | 1 (25.00) | 0.22 | 1 (25.00) | 0.2 | 0 (0.00) | 0.98 |
| Profil Sérologique | N | PCR | OR | IC 95% | p-Value | |
|---|---|---|---|---|---|---|
| Negative n (%) | Positive n (%) | |||||
| IgM− & IgG− | 194 | 180 (92.98) | 14 (7.22) | Ref | ||
| (negative) | ||||||
| IgM+ & IgG− | 26 | 7 (26.92) | 19 (73.08) | 34.9 | [12.5–97] | <0.0001 |
| (acute infection) | ||||||
| IgM+ & IgG+ | 34 | 6 (17.65) | 28 (82.35) | 60 | [21.3–169] | <0.0001 |
| (ongoing infection) | ||||||
| IgM− & IgG+ | 37 | 36 (97.3) | 1 (2.7) | 0.36 | [0.05–2.8] | 0.33 |
| (recovered/post infection) | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamga Wouambo, R.; Djuikoué, C.I.; Esemu, L.F.; Kagoue Simeni, L.A.; Tchitchoua, M.C.; Djouela Djoulako, P.D.; Fokam, J.; Singwe-Ngandeu, M.; Mpoudi Ngolé, E.; Apalata, T. Comparative Performance of Serological (IgM/IgG) and Molecular Testing (RT-PCR) of COVID-19 in Three Private Universities in Cameroon during the Pandemic. Viruses 2023, 15, 407. https://doi.org/10.3390/v15020407
Kamga Wouambo R, Djuikoué CI, Esemu LF, Kagoue Simeni LA, Tchitchoua MC, Djouela Djoulako PD, Fokam J, Singwe-Ngandeu M, Mpoudi Ngolé E, Apalata T. Comparative Performance of Serological (IgM/IgG) and Molecular Testing (RT-PCR) of COVID-19 in Three Private Universities in Cameroon during the Pandemic. Viruses. 2023; 15(2):407. https://doi.org/10.3390/v15020407
Chicago/Turabian StyleKamga Wouambo, Rodrigue, Cecile Ingrid Djuikoué, Livo Forgu Esemu, Luc Aime Kagoue Simeni, Murielle Chantale Tchitchoua, Paule Dana Djouela Djoulako, Joseph Fokam, Madeleine Singwe-Ngandeu, Eitel Mpoudi Ngolé, and Teke Apalata. 2023. "Comparative Performance of Serological (IgM/IgG) and Molecular Testing (RT-PCR) of COVID-19 in Three Private Universities in Cameroon during the Pandemic" Viruses 15, no. 2: 407. https://doi.org/10.3390/v15020407