
The Cascade of Care for Hepatitis C Treatment in Rwanda: A Retrospective Cohort Study of the 2017–2019 Mass Screening and Treatment Campaign

 , , ,
, , ,
Abstract
1. Background
2. Materials and Methods
2.1. Study Context
2.2. Study Design
2.3. Study Sites and Population
2.4. Data Sources
2.5. Cascade of Care
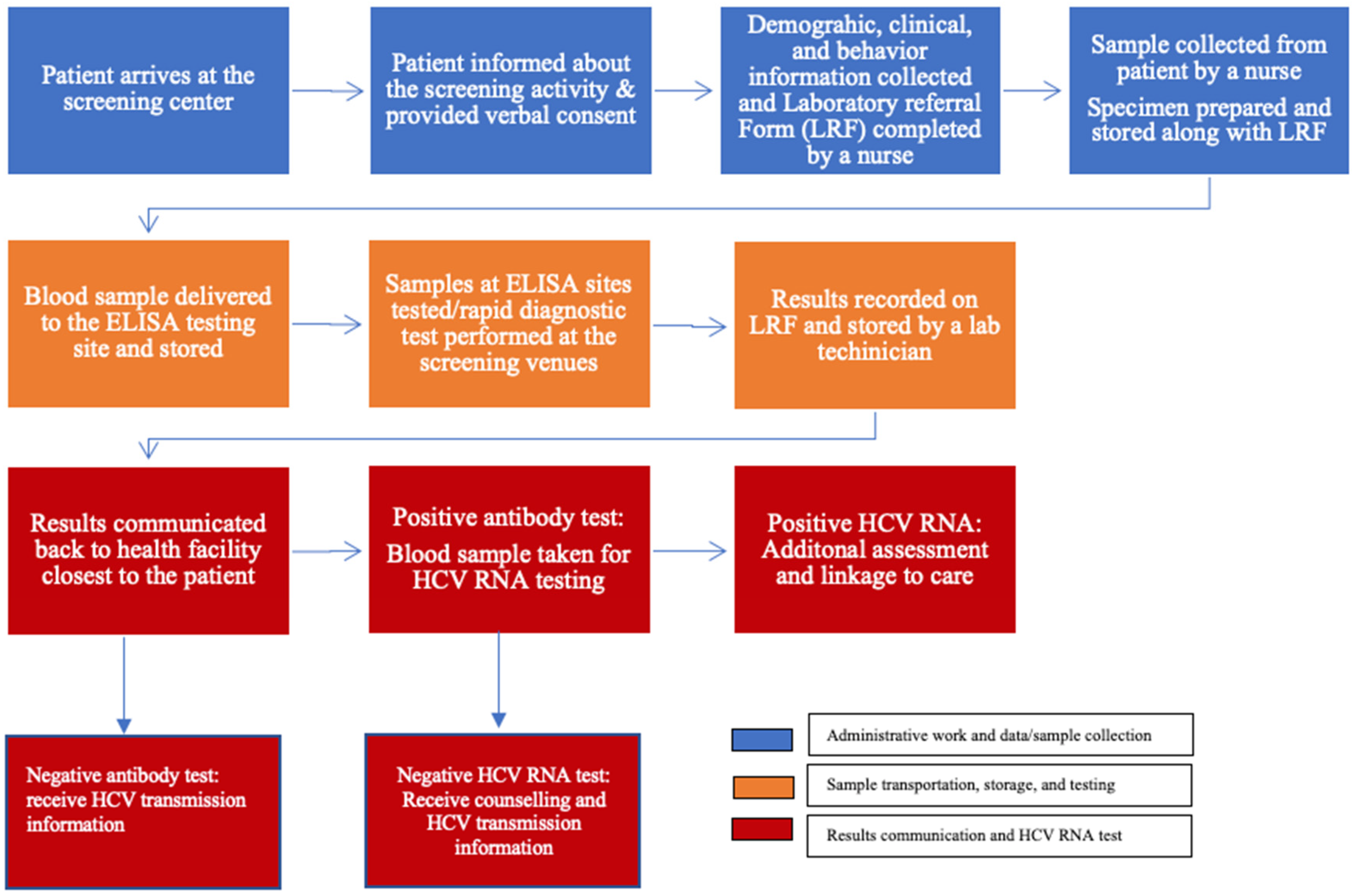
2.5.1. Screening
2.5.2. HCV RNA Testing
2.5.3. Treatment
2.6. Outcome Variables
2.7. Other Variables
2.8. Data Analysis
3. Results
3.1. Descriptive Characteristics
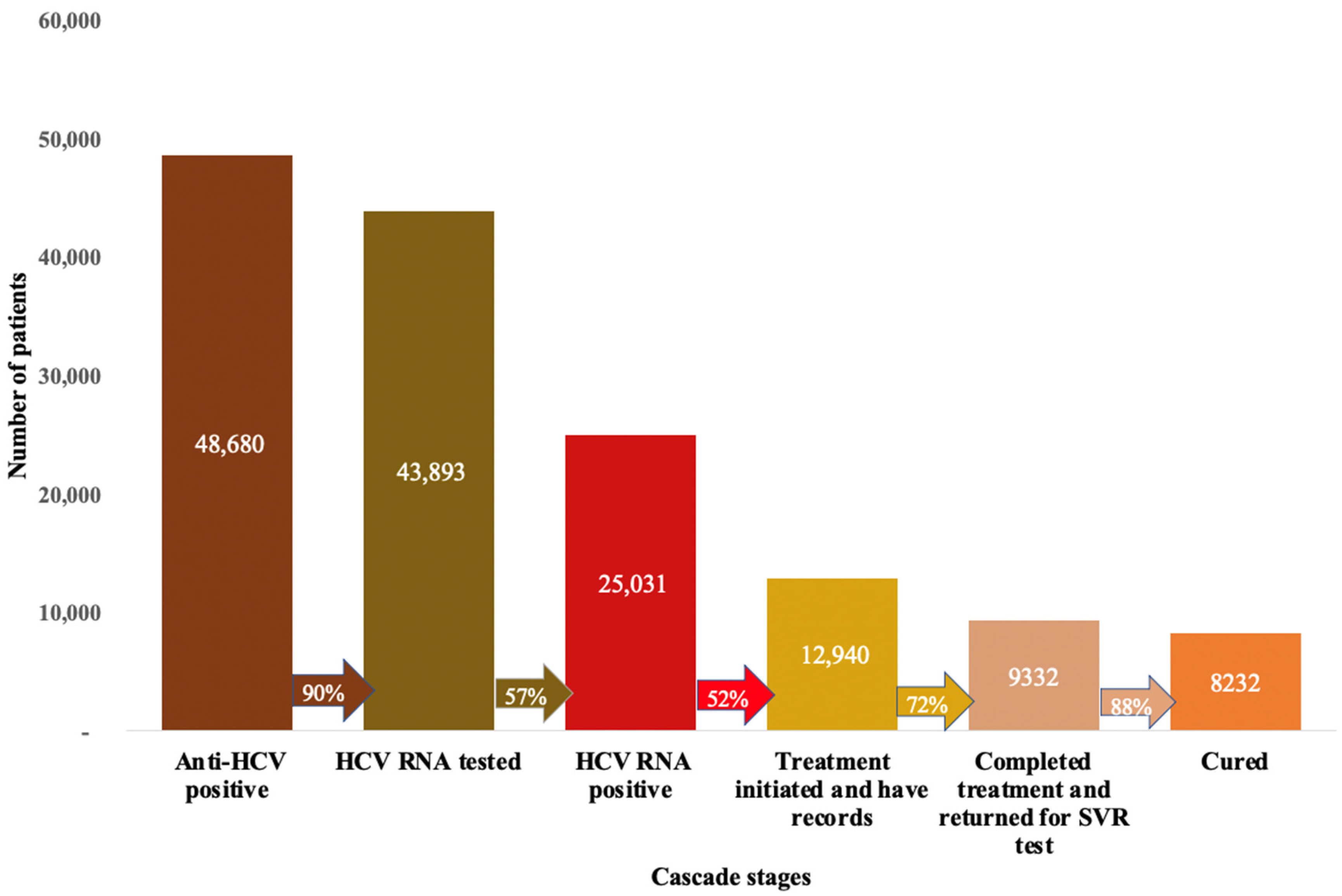
3.2. Cascade of Care
3.3. Anti-HCV Seroprevalence
3.4. HCV RNA Testing
3.5. Dropout at HCV RNA Testing
3.6. Treatment Success (Achieving SVR)
3.7. Dropout at Final SVR Test
4. Discussion
4.1. Anti-HCV Screening and HCV RNA Testing
4.2. Treatment Initiation and Success
4.3. HCV RNA and SVR Testing Dropout
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marinho, R.T.; Vitor, S.; Velosa, J. Benefits of Curing Hepatitis C Infection. J. Gastrointest. Liver Dis. 2014, 23, 85–90. [Google Scholar] [CrossRef]
- Mohd Hanafiah, K.; Groeger, J.; Flaxman, A.D.; Wiersma, S.T. Global epidemiology of hepatitis C virus infection: New estimates of age-specific antibody to HCV seroprevalence. Hepatology 2013, 57, 1333–1342. [Google Scholar] [CrossRef] [PubMed]
- Madhava, V.; Burgess, C.; Drucker, E. Epidemiology of chronic hepatitis C virus infection in sub-Saharan Africa. Lancet Infect. Dis. 2002, 2, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Turner, S.J.; Brown, J.; Paladino, J.A. Protease inhibitors for hepatitis C: Economic implications. PharmacoEconomics 2013, 31, 739–751. [Google Scholar] [CrossRef] [PubMed]
- Global Progress Report on HIV, Viral Hepatitis and Sexually Transmitted Infections. 2021. Available online: https://www.who.int/publications-detail-redirect/9789240027077 (accessed on 19 December 2022).
- World Health Organization. Global Hepatitis Report; World Health Organization: Geneva, Switzerland, 2017; ISBN 978-92-4-156545-5. [Google Scholar]
- World Health Organization. The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 19 December 2022).
- Thongsawat, S.; Piratvisuth, T.; Pramoolsinsap, C.; Chutaputti, A.; Tanwandee, T.; Thongsuk, D. Resource Utilization and Direct Medical Costs of Chronic Hepatitis C in Thailand: A Heavy but Manageable Economic Burden. Value Health Reg. Issues 2014, 3, 12–18. [Google Scholar] [CrossRef]
- Tapper, E.B.; Catana, A.M.; Sethi, N.; Mansuri, D.; Sethi, S.; Vong, A.; Afdhal, N.H. Direct costs of care for hepatocellular carcinoma in patients with hepatitis C cirrhosis. Cancer 2016, 122, 852–858. [Google Scholar] [CrossRef]
- Estes, C.; Abdel-Kareem, M.; Abdel-Razek, W.; Abdel-Sameea, E.; Abuzeid, M.; Gomaa, A.; Osman, W.; Razavi, H.; Zaghla, H.; Waked, I. Economic burden of hepatitis C in Egypt: The future impact of highly effective therapies. Aliment. Pharmacol. Ther. 2015, 42, 696–706. [Google Scholar] [CrossRef]
- Nevens, F.; Colle, I.; Michielsen, P.; Robaeys, G.; Moreno, C.; Caekelbergh, K.; Lamotte, M.; Wyffels, V. Resource use and cost of hepatitis C-related care. Eur. J. Gastroenterol. Hepatol. 2012, 24, 1191–1198. [Google Scholar] [CrossRef]
- Hellard, M.; Thompson, A.; Scott, N.; Iser, D.; Doyle, J.S. Cost-effectiveness of treating chronic hepatitis C virus with direct-acting antivirals in people who inject drugs in Australia. J. Gastroenterol. Hepatol. 2016, 31, 872–882. [Google Scholar] [CrossRef]
- Ford, N.; Swan, T.; Beyer, P.; Hirnschall, G.; Easterbrook, P.; Wiktor, S. Simplification of antiviral hepatitis C virus therapy to support expanded access in resource-limited settings. J. Hepatol. 2014, 61, S132–S138. [Google Scholar] [CrossRef]
- Gupta, N.; Kabahizi, J.; Mukabatsinda, C.; Walker, T.D.; Musabeyezu, E.; Kiromera, A.; Van Nuil, J.I.; Steiner, K.; Mukherjee, J.; Nsanzimana, S.; et al. “Waiting for DAAs”: A retrospective chart review of patients with untreated hepatitis C in Rwanda. PLoS ONE 2017, 12, e0174148. [Google Scholar] [CrossRef]
- Layden, J.E.; Phillips, R.; Opare-Sem, O.; Akere, A.; Salako, B.L.; Nelson, K.; Dugas, L.; Luke, A.; Tayo, B.O.; Cooper, R.S. Hepatitis C in Sub-Saharan Africa: Urgent Need for Attention. Open Forum Infect. Dis. 2014, 1, ofu065. [Google Scholar] [CrossRef]
- Assefa, Y.; Hill, P.S.; Ulikpan, A.; Williams, O.D. Access to medicines and hepatitis C in Africa: Can tiered pricing and voluntary licencing assure universal access, health equity and fairness? Glob. Health 2017, 13, 73. [Google Scholar] [CrossRef]
- Nsanzimana, S.; Kirik, C.M.; Uwizihiwe, J.P.; Bucher, H.C. Increasing Access to Hepatitis C Treatment in Rwanda: The Promise of Rwanda: Existing HIV Infrastructure. J. Infect. Dis. Ther. 2015, 3, 5–6. [Google Scholar] [CrossRef]
- How Rwanda Is Eliminating Hepatitis C and What Canada Can Learn from Its Successes. Available online: https://blog.catie.ca/2021/11/18/how-rwanda-is-eliminating-hepatitis-c-and-what-canada-can-learn-from-its-successes/ (accessed on 26 July 2022).
- WHO|Combating Hepatitis B and C to Reach Elimination by 2030. Available online: http://www.who.int/hepatitis/publications/hep-elimination-by-2030-brief/en/ (accessed on 7 February 2019).
- Gupta, N.; Nsanzimana, S. Is hepatitis C elimination possible in sub-Saharan Africa? The case of Rwanda. Lancet Gastroenterol. Hepatol. 2018, 3, 302–303. [Google Scholar] [CrossRef]
- Umutesi, G.; Shumbusho, F.; Kateera, F.; Serumondo, J.; Kabahizi, J.; Musabeyezu, E.; Ngwije, A.; Gupta, N.; Nsanzimana, S. Rwanda launches a 5-year national hepatitis C elimination plan: A landmark in sub-Saharan Africa. J. Hepatol. 2019, 70, 1043–1045. [Google Scholar] [CrossRef]
- Kronfli, N.; Dussault, C.; Klein, M.B.; Lebouché, B.; Sebastiani, G.; Cox, J. The hepatitis C virus cascade of care in a Quebec provincial prison: A retrospective cohort study. Can. Med. Assoc. Open Access J. 2019, 7, E674–E679. [Google Scholar] [CrossRef]
- Yousafzai, M.T.; Bajis, S.; Alavi, M.; Grebely, J.; Dore, G.J.; Hajarizadeh, B. Global cascade of care for chronic hepatitis C virus infection: A systematic review and meta-analysis. J. Viral Hepat. 2021, 28, 1340–1354. [Google Scholar] [CrossRef]
- Karoney, M.J.; Siika, A.M. Hepatitis C virus (HCV) infection in Africa: A review. Pan Afr. Med. J. 2013, 14, 44. [Google Scholar] [CrossRef]
- Kamali, I.; Shumbusho, F.; Barnhart, D.A.; Nyirahabihirwe, F.; Gakuru, J.P.; Dusingizimana, W.; Nizeyumuremyi, E.; Habinshuti, P.; Walker, S.; Makuza, J.D.; et al. Time to complete hepatitis C cascade of care among patients identified during mass screening campaigns in rural Rwanda: A retrospective cohort study. BMC Infect. Dis. 2022, 22, 272. [Google Scholar] [CrossRef]
- Binagwaho, A.; Farmer, P.; Nsanzimana, S.; Karema, C.; Gasana, M.; de Dieu Ngirabega, J.; Ngabo, F.; Wagner, C.; Nutt, C.; Nyatanyi , T.; et al. Thierry Nyatanyi 20 years on: Investing in life. Lancet 2014, 384, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Nsanzimana, S.; Penkunas, M.; Liu, C.; Sebuhoro, D.; Ngwije, A.; Remera, E.; Umutesi, J.; Ntirenganya, C.; Mugeni, S.; Serumondo, J. THU-411-Effectiveness of direct: Acting antivirals for the treatment of viral hepatitis C in Rwanda. J. Hepatol. 2019, 70, e337. [Google Scholar] [CrossRef]
- Universal Health Coverage: How Rwanda Is Moving forward with Healthcare for All|Innovations in Healthcare. Available online: https://www.innovationsinhealthcare.org/universal-health-coverage-how-rwanda-is-moving-forward-with-healthcare-for-all/ (accessed on 19 December 2022).
- Makuza, J.D.; Rwema, J.O.T.; Ntihabose, C.K.; Dushimiyimana, D.; Umutesi, J.; Nisingizwe, M.P.; Serumondo, J.; Semakula, M.; Riedel, D.J.; Nsanzimana, S. Prevalence of hepatitis B surface antigen (HBsAg) positivity and its associated factors in Rwanda. BMC Infect. Dis. 2019, 19, 381. [Google Scholar] [CrossRef] [PubMed]
- Umutesi, J.; Simmons, B.; Makuza, J.D.; Dushimiyimana, D.; Mbituyumuremyi, A.; Uwimana, J.M.; Ford, N.; Mills, E.J.; Nsanzimana, S. Prevalence of hepatitis B and C infection in persons living with HIV enrolled in care in Rwanda. BMC Infect. Dis. 2017, 17, 315. [Google Scholar] [CrossRef]
- Martínez, J.D.; Garzón, M.A.; Arteaga, J.M.; Hernández, G.; Manrique, C.; Hormaza, N.; Lizarazo, J.; Marulanda, J.; Molano, J.C.; Rey, M.H.; et al. The SD BIOLINE Rapid Test for Detection of Antibodies to HCV among High-Risk Patients. Rev. Colomb. Gastroenterol. 2015, 30, 273–278. [Google Scholar] [CrossRef][Green Version]
- Sonderup, M.W.; Afihene, M.; Ally, R.; Apica, B.; Awuku, Y.; Cunha, L.; Dusheiko, G.; Gogela, N.; Lohouès-Kouacou, M.-J.; Lam, P.; et al. Hepatitis C in sub-Saharan Africa: The current status and recommendations for achieving elimination by 2030. Lancet Gastroenterol. Hepatol. 2017, 2, 910–919. [Google Scholar] [CrossRef]
- Ezeanya, C. Home-Grown and Grassroots-Based Strategies for Determining Inequality towards Policy Action: Rwanda’s Ubudehe Approach in Perspective. Available online: https://www.wider.unu.edu/sites/default/files/wp2015-008.pdf (accessed on 19 December 2022).
- Song, M.; Zhou, X.; Pazaris, M.; Spiegelman, D. The Missing Covariate Indicator Method Is Nearly Valid Almost Always 2021. Available online: https://doi.org/10.48550/arXiv.2111.00138 (accessed on 19 December 2022). [CrossRef]
- Rwanda Population (2023)—Worldometer. Available online: https://www.worldometers.info/world-population/rwanda-population/ (accessed on 19 December 2022).
- Nsanzimana, S.; Rwibasira, G.N.; Malamba, S.S.; Musengimana, G.; Kayirangwa, E.; Jonnalagadda, S.; Fazito Rezende, E.; Eaton, J.W.; Mugisha, V.; Remera, E.; et al. HIV incidence and prevalence among adults aged 15–64 years in Rwanda: Results from the Rwanda Population-based HIV Impact Assessment (RPHIA) and District-level Modeling, 2019. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2022, 116, 245–254. [Google Scholar] [CrossRef]
- Makuza, J.D.; Liu, C.Y.; Ntihabose, C.K.; Dushimiyimana, D.; Umuraza, S.; Nisingizwe, M.P.; Umutesi, J.; Serumondo, J.; Mugeni, S.D.; Semakula, M.; et al. Risk factors for viral hepatitis C infection in Rwanda: Results from a nationwide screening program. BMC Infect. Dis. 2019, 19, 688. [Google Scholar] [CrossRef]
- 2005-2020 Rates of Acute Hepatitis C Cases by Age|Center for Disease Control. 10 October 2022. Available online: https://www.cdc.gov/hepatitis/statistics/2020surveillance/hepatitis-c/figure-3.4.htm (accessed on 19 December 2022).
- Umutesi, J.; Liu, C.Y.; Penkunas, M.J.; Makuza, J.D.; Ntihabose, C.K.; Umuraza, S.; Niyikora, J.; Serumondo, J.; Gupta, N.; Nsanzimana, S. Screening a nation for hepatitis C virus elimination: A cross-sectional study on prevalence of hepatitis C and associated risk factors in the Rwandan general population. BMJ Open 2019, 9, e029743. [Google Scholar] [CrossRef]
- Hutin, Y.J.; Duclos, P.; Hogerzeil, H.; Ball, A.; Carr, R. Unsterile injections and emergence of human pathogens. Lancet 2002, 359, 2280. [Google Scholar] [CrossRef]
- Mohamed, Z.; Rwegasha, J.; Kim, J.U.; Shimakawa, Y.; Poiteau, L.; Chevaliez, S.; Bhagani, S.; Taylor-Robinson, S.D.; Thursz, M.R.; Mbwambo, J.; et al. The hepatitis C cascade of care in people who inject drugs in Dar es Salaam, Tanzania. J. Viral Hepat. 2018, 25, 1438–1445. [Google Scholar] [CrossRef]
- Awadalla, H.I.; Ragab, M.H.; Nassar, N.A.; Osman, M.A.H. Risk factors of hepatitis C infection among Egyptian blood donors. Cent. Eur. J. Public Health 2011, 19, 217–221. [Google Scholar] [CrossRef]
- Saleh, D.A.; Shebl, F.; Abdel-Hamid, M.; Narooz, S.; Mikhail, N.; El-Batanony, M.; El-Kafrawy, S.; El-Daly, M.; Sharaf, S.; Hashem, M.; et al. Incidence and risk factors for hepatitis C infection in a cohort of women in rural Egypt. Trans. R. Soc. Trop. Med. Hyg. 2008, 102, 921–928. [Google Scholar] [CrossRef][Green Version]
- Quinn, S.C.; Kumar, S. Health Inequalities and Infectious Disease Epidemics: A Challenge for Global Health Security. Biosecurity Bioterrorism Biodefense Strategy Pract. Sci. 2014, 12, 263–273. [Google Scholar] [CrossRef]
- Platt, L.; Easterbrook, P.; Gower, E.; McDonald, B.; Sabin, K.; McGowan, C.; Yanny, I.; Razavi, H.; Vickerman, P. Prevalence and burden of HCV co-infection in people living with HIV: A global systematic review and meta-analysis. Lancet Infect. Dis. 2016, 16, 797–808. [Google Scholar] [CrossRef]
- Baden, R.; Rockstroh, J.K.; Buti, M. Natural History and Management of Hepatitis C: Does Sex Play a Role? J. Infect. Dis. 2014, 209, S81–S85. [Google Scholar] [CrossRef]
- Baha, W.; Foullous, A.; Dersi, N.; They-they, T.P.; Alaoui, K.E.; Nourichafi, N.; Oukkache, B.; Lazar, F.; Benjelloun, S.; Ennaji, M.M.; et al. Prevalence and risk factors of hepatitis B and C virus infections among the general population and blood donors in Morocco. BMC Public Health 2013, 13, 50. [Google Scholar] [CrossRef]
- Serumondo, J.; Penkunas, M.J.; Niyikora, J.; Ngwije, A.; Kiromera, A.; Musabeyezu, E.; Umutesi, J.; Umuraza, S.; Musengimana, G.; Nsanzimana, S. Patient and healthcare provider experiences of hepatitis C treatment with direct-acting antivirals in Rwanda: A qualitative exploration of barriers and facilitators. BMC Public Health 2020, 20, 946. [Google Scholar] [CrossRef]
- Gupta, N.; Kabahizi, J.; Muvunyi, C.; Mbituyumuremyi, A.; Van Nuil, J.; Shumbusho, F.; Ntaganda, F.; Damascene, M.J.; Mukabatsinda, C.; Musabeyezu, E.; et al. Direct-acting antiviral treatment in sub-Saharan Africa: A prospective trial of Ledipasvir/Sofosbuvir for chronic Hepatitis C infection in Rwanda (the SHARED study). J. Hepatol. 2018, 68, S50. [Google Scholar] [CrossRef]
- Gupta, N.; Manirambona, L.; Shumbusho, F.; Kabihizi, J.; Murangwa, A.; Serumondo, J.; Makuza, J.D.; Nsanzimana, S.; Muvunyi, C.M.; Mukabatsinda, C.; et al. Safety and efficacy of sofosbuvir-velpatasvir-voxilaprevir for re-treatment of chronic hepatitis C virus infection in patients with previous direct-acting antiviral treatment failure in Rwanda (SHARED-3): A single-arm trial. Lancet Gastroenterol. Hepatol. 2022, 7, 542–551. [Google Scholar] [CrossRef]
- Sarrazin, C. Treatment failure with DAA therapy: Importance of resistance. J. Hepatol. 2021, 74, 1472–1482. [Google Scholar] [CrossRef] [PubMed]
- Opio, C.K. Direct-acting antiviral regimens and HCV treatment failure and re-treatment in sub-Saharan Africa. Lancet Gastroenterol. Hepatol. 2022, 7, 498–499. [Google Scholar] [CrossRef] [PubMed]
- Nsanzimana, S.; Penkunas, M.J.; Liu, C.Y.; Sebuhoro, D.; Ngwije, A.; Remera, E.; Umutesi, J.; Ntirenganya, C.; Mugeni, S.D.; Serumondo, J. Effectiveness of Direct-Acting Antivirals for the treatment of chronic hepatitis C in Rwanda: A retrospective study. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 73, e3300–e3307. [Google Scholar] [CrossRef] [PubMed]
- Luma, H.N.; Eloumou, S.A.F.B.; Noah, D.N.; Eyenga, B.A.; Nko’Ayissi, G.; Taku, T.S.; Malongue, A.; Donfack-Sontsa, O.; Ditah, I.C. Hepatitis C Continuum of Care in a Treatment Center in Sub-Saharan Africa. J. Clin. Exp. Hepatol. 2018, 8, 335–341. [Google Scholar] [CrossRef]
- Janjua, N.Z.; Kuo, M.; Yu, A.; Alvarez, M.; Wong, S.; Cook, D.; Wong, J.; Grebely, J.; Butt, Z.A.; Samji, H.; et al. The Population Level Cascade of Care for Hepatitis C in British Columbia, Canada: The BC Hepatitis Testers Cohort (BC-HTC). EBioMedicine 2016, 12, 189–195. [Google Scholar] [CrossRef]
- Jankovic, J.; Mirkovic, M.; Jovic-Vranes, A.; Santric-Milicevic, M.; Terzic-Supic, Z. Association between non-communicable disease multimorbidity and health care utilization in a middle-income country: Population-based study. Public Health 2018, 155, 35–42. [Google Scholar] [CrossRef]
- Agrawal, U.; Azcoaga-Lorenzo, A.; Fagbamigbe, A.F.; Vasileiou, E.; Henery, P.; Simpson, C.R.; Stock, S.J.; Shah, S.A.; Robertson, C.; Woolhouse, M.; et al. Association between multimorbidity and mortality in a cohort of patients admitted to hospital with COVID-19 in Scotland. J. R. Soc. Med. 2022, 115, 22–30. [Google Scholar] [CrossRef]
- Screening and Treatment Program to Eliminate Hepatitis C in Egypt|NEJM. Available online: https://www.nejm.org/doi/full/10.1056/NEJMsr1912628 (accessed on 21 July 2022).
- World Bank Poverty Headcount Ratio at National Poverty Lines (% of population)—Rwanda|Data. Available online: https://data.worldbank.org/indicator/SI.POV.NAHC?locations=RW (accessed on 1 November 2022).
- Ha, S.; Timmerman, K. Awareness and knowledge of hepatitis C among health care providers and the public: A scoping review. Can. Commun. Dis. Rep. 2018, 44, 157–165. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Outcome | Numerator | Denominator |
|---|---|---|
| Proportion of patients who were anti-HCV positive | Number of patients with a positive HCV antibody test | Number of patients screened |
| HCV RNA viremia rate | Number of patients who tested HCV RNA positive | Number of patients who screened positive for anti-HCV with HCV RNA test conducted |
| Proportion of patients who dropped out of care before HCV RNA viremia testing | Number of patients who screened positive for anti-HCV and did not return for an HCV RNA test | Number of patients who screened positive for anti-HCV |
| Proportion of patients who initiated treatment | Number of patients who initiated treatment with available records in hospital registers | Number of patients who were confirmed HCV RNA positive |
| Proportion of patients who achieved SVR (treatment success) | Number of patients whose HCV viral load result was below 20 copies/mL within 12–24 weeks post-treatment and returned for SVR test | Number of patients who completed treatment with available records and returned for SVR assessment (excluding those who died) |
| Proportion of patients who did not return for SVR tests | Number of patients who initiated treatment and did not come back for SVR assessment | Number of patients who initiated treatment with available records in the registers (excluding those who died) |
| Total Sample | Anti-HCV Positive | HCV RNA Testing | ||||||
|---|---|---|---|---|---|---|---|---|
| Variables | Total Sample | Total (%) | Total Number Screened Anti-HCV Positive | Anti-HCV Positive (%) | Total Number HCV RNA Tested | HCV RNA Positive (%) | Total Dropouts | Dropout (%) |
| Age | ||||||||
| <44 | 426,186 | 59.4 | 9378 | 19.4 | 3324 | 13.3 | 686 | 15.1 |
| 44–54 | 112,264 | 15.6 | 6165 | 12.8 | 2977 | 11.9 | 265 | 5.8 |
| 55–64 | 100,439 | 14 | 9918 | 20.6 | 5498 | 22 | 340 | 7.5 |
| 64+ | 78,493 | 10.9 | 22,848 | 47.3 | 13,203 | 52.8 | 3252 | 71.6 |
| Sex | ||||||||
| Female | 555,389 | 68.4 | 32,159 | 66.5 | 16,442 | 65.7 | 3259 | 68.1 |
| Male | 256,701 | 31.6 | 16,580 | 33.5 | 8587 | 34.3 | 1528 | 31.9 |
| SES categories | ||||||||
| Category 1 | 104,681 | 12.2 | 8077 | 23.3 | 4971 | 19.9 | 1163 | 25.5 |
| Category 2 | 260,537 | 30.3 | 12,211 | 35.2 | 6854 | 27.4 | 1510 | 33.1 |
| Category 3 or 4 or unknown | 495,583 | 57.6 | 14,456 | 41.6 | 8201 | 52.7 | 1888 | 41.3 |
| Marital status | ||||||||
| Single | 109,552 | 15.1 | 1625 | 4.9 | 910 | 4.8 | 126 | 4.6 |
| Married or in union | 461,231 | 63.6 | 21,522 | 64.9 | 11,911 | 63.4 | 1707 | 62 |
| Separated/divorced/widowed | 153,919 | 21.2 | 9927 | 30.2 | 5972 | 31.8 | 920 | 33.4 |
| Health insurance | ||||||||
| No insurance | 161,853 | 18.8 | 7867 | 15.9 | 172 | 19.3 | 1045 | 21.8 |
| Community insurance | 657,067 | 76.3 | 40,076 | 81.1 | 19,517 | 78 | 3643 | 76.1 |
| Private or other government insurance (RAMA/RSSB) | 41,881 | 4.9 | 1437 | 3 | 694 | 2.8 | 99 | 2.1 |
| Diabetes status | ||||||||
| No | 694,243 | 99 | 32,956 | 98 | 18,681 | 97.5 | 2835 | 98.9 |
| Yes | 7353 | 1 | 676 | 2 | 475 | 2.5 | 32 | 1.1 |
| HTA status | ||||||||
| No | 448,936 | 97.7 | 30,204 | 92.5 | 17,626 | 90.2 | 1845 | 92.4 |
| Yes | 10,653 | 2.3 | 2455 | 7.5 | 1915 | 9.8 | 152 | 7.6 |
| Renal failure status | ||||||||
| No | 453,150 | 98.8 | 30,926 | 98.1 | 18,461 | 98.7 | 2078 | 97.9 |
| Yes | 5365 | 1.2 | 592 | 1.9 | 247 | 1.3 | 44 | 2.1 |
| HIV status | ||||||||
| Negative | 680,082 | 97.1 | 31,789 | 94.6 | 17,719 | 92.8 | 2836 | 98.6 |
| Positive | 20,071 | 2.9 | 1806 | 5.4 | 1371 | 7.2 | 40 | 1.4 |
| HBV result | ||||||||
| Negative | 829,644 | 97 | 42,548 | 97.7 | 20,278 | 98.7 | 4323 | 97.6 |
| Positive | 25,652 | 3 | 984 | 2.3 | 267 | 1.3 | 105 | 2.4 |
| Family History of viral hepatitis C | ||||||||
| No | 837,090 | 97.2 | 32,317 | 95.4 | 17,962 | 96 | 4709 | 98.4 |
| Yes | 23,711 | 2.8 | 1543 | 4.6 | 1006 | 4 | 78 | 1.6 |
| Ever been traditionally operated on | ||||||||
| No | 597,913 | 85.1 | 26,955 | 79.3 | 15,598 | 80.4 | 2312 | 81.7 |
| Yes | 104,688 | 14.9 | 7020 | 20.7 | 3801 | 19.6 | 517 | 18.3 |
| Ever been transfused | ||||||||
| No | 683,769 | 97.3 | 32,931 | 96.9 | 18,770 | 96.8 | 2759 | 97.5 |
| Yes | 18,729 | 2.7 | 1047 | 3.1 | 617 | 3.2 | 70 | 2.5 |
| Ever been medically operated on | ||||||||
| No | 665,094 | 94.7 | 32,108 | 94.3 | 18,430 | 94.7 | 2674 | 94.6 |
| Yes | 37,518 | 5.3 | 1945 | 5.7 | 1022 | 5.3 | 152 | 5.4 |
| Ever been diagnosed with liver disease | ||||||||
| No | 399,965 | 98.3 | 18,211 | 97.58 | 15,000 | 97.9 | 895 | 98.2 |
| Yes | 6947 | 1.7 | 452 | 2.42 | 310 | 2.1 | 16 | 1.8 |
| HBV vaccination | ||||||||
| Partially or fully vaccinated | 53,723 | 6.24 | 5245 | 31.3 | 4519 | 32.8 | 66 | 1.4 |
| Not vaccinated | 807,078 | 93.76 | 43,435 | 68.7 | 20,512 | 67.2 | 4721 | 98.6 |
| Unadjusted Model | Adjusted Model † | ||||
|---|---|---|---|---|---|
| Variables | N | OR | 95% CI | OR | 95% CI |
| Age | |||||
| <44 | 426,186 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| 44–54 | 112,264 | 2.53 | 2.44, 2.61 | 2.41 | 2.33, 2.50 |
| 55–64 | 100,439 | 4.66 | 4.52, 4.80 | 4.45 | 4.31, 4.60 |
| 64+ | 78,493 | 18.1 | 17.64, 18.61 | 15.1 | 14.67, 15.59 |
| Missing | 143,419 | 0.064 | 0.06, 0.07 | 0.0093 | 0.01, 0.01 |
| SES | |||||
| Category 1 | 104,681 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Category 2 | 260,537 | 0.66 | 0.64, 0.68 | 0.84 | 0.81, 0.87 |
| Category 3 or 4 or unknown | 336,580 | 0.59 | 0.58, 0.61 | ||
| Missing | 159,003 | 1.45 | 1.40, 1.50 | ||
| Marital status | |||||
| Single | 109,552 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Married or in union | 461,231 | 2.9 | 2.75, 3.06 | 1.47 | 1.39, 1.55 |
| Separated/divorced/widowed | 153,919 | 3.59 | 3.39, 3.79 | 1.25 | 1.18, 1.33 |
| Missing | 136,099 | 6.69 | 6.33, 7.07 | 6.5 | 5.95, 7.11 |
| HIV | |||||
| No | 680,082 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Yes | 20,071 | 2.2 | 2.09, 2.32 | 1.91 | 1.80, 2.03 |
| Missing | 160,648 | 1.55 | 1.51, 1.59 | 0.91 | 0.76, 1.08 |
| Family history of viral hepatitis | |||||
| No | 677,376 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Yes | 23,711 | 1.27 | 1.21, 1.35 | 1.1 | 1.04, 1.18 |
| Missing | 159,714 | 1.48 | 1.44, 1.52 | 1.51 | 1.20, 1.90 |
| Ever been traditionally operated on | |||||
| No | 597,913 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Yes | 104,688 | 1.52 | 1.48, 1.56 | 1.31 | 1.27, 1.36 |
| Missing | 158,200 | 1.55 | 1.51, 1.59 | 0.23 | 0.17, 0.32 |
| Unadjusted Model | Adjusted Model † | ||||
|---|---|---|---|---|---|
| Variables | N | OR | 95% CI | OR | 95% CI |
| Age | |||||
| <44 | 8803 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| 44–54 | 5991 | 1.5 | 1.36, 1.58 | 1.65 | 1.51, 1.80 |
| 55–64 | 9744 | 1.8 | 1.69, 1.93 | 1.89 | 1.75, 2.04 |
| >64 | 19,164 | 2.7 | 2.51, 2.82 | 2.88 | 2.67, 3.10 |
| Missing | 191 | 0.2 | 0.11, 0.25 | 0.33 | 0.20, 0.53 |
| Social Economic Status | |||||
| Category 1 | 7061 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Category 2 | 10,957 | 0.7 | 0.67, 0.77 | 0.8 | 0.74, 0.87 |
| Category 3 or 4 or unknown | 12,839 | 0.7 | 0.66, 0.76 | 0.78 | 0.72, 0.85 |
| Missing | 13,036 | 0.3 | 0.32, 0.36 | 0.3 | 0.27, 0.33 |
| Sex | |||||
| Female | 28,834 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Male | 15,059 | 1.1 | 1.04, 1.13 | 1.34 | 1.27, 1.42 |
| Marital status | |||||
| Single | 1528 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Married or in union | 20,191 | 1.3 | 1.12, 1.41 | 0.85 | 0.75, 0.97 |
| Separated/divorced/widowed | 9292 | 1.5 | 1.30, 1.66 | 0.84 | 0.73, 0.97 |
| Missing | 12,882 | 0.7 | 0.59, 0.75 | 1.24 | 1.04, 1.49 |
| Hepatitis B Ag results | |||||
| Negative | 38,922 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Positive | 880 | 0.5 | 0.39, 0.55 | 0.53 | 0.44, 0.65 |
| Missing | 4091 | 15 | 13.29, 16.60 | 109.4 | 95.49, 125.34 |
| HIV | |||||
| No | 29,622 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Yes | 1789 | 2 | 1.80, 2.31 | 2.51 | 2.20, 2.87 |
| Missing | 12,482 | 0.4 | 0.42, 0.46 | 0.49 | 0.41, 0.58 |
| Hypertension | |||||
| No | 29,048 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Yes | 2323 | 2.3 | 1.99, 2.54 | 2.05 | 1.80, 2.34 |
| Missing | 12,522 | 0.4 | 0.33, 0.37 | 0.12 | 0.11, 0.14 |
| Ever been traditionally operated on | |||||
| No | 25,212 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Yes | 6623 | 1 | 0.90, 1.02 | 0.9 | 0.84, 0.97 |
| Missing | 12,058 | 0.4 | 0.41, 0.46 | 0.66 | 0.45, 0.97 |
| Ever been medically operated on | 43,893 | ||||
| No | 30,066 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Yes | 1853 | 0.7 | 0.60, 0.74 | 0.66 | 0.58, 0.74 |
| Missing | 12,755 | 0.4 | 0.41, 0.45 | 1.67 | 0.98, 2.83 |
| HBV vaccination status | |||||
| Partially or fully vaccinated | 5635 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Not vaccinated | 38,258 | 0.3 | 0.29, 0.34 | 0.49 | 0.45, 0.53 |
| Unadjusted Model | Adjusted Model † | ||||
|---|---|---|---|---|---|
| Variables | N | OR | 95% CI | OR | 95% CI |
| Age | |||||
| <44 | 8987 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| 44–54 | 6250 | 0.6 | 0.51, 0.69 | 0.5 | 0.42, 0.59 |
| 55–64 | 10,081 | 0.48 | 0.42, 0.55 | 0.4 | 0.35, 0.47 |
| >64 | 22,927 | 2.53 | 2.31, 2.77 | 4.54 | 4.03, 5.12 |
| Missing | 435 | 14.23 | 10.78, 18.78 | 491 | 328.16, 734.68 |
| Social Economic Status | |||||
| Category 1 | 8224 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Category 2 | 12,462 | 0.66 | 0.60, 0.72 | 0.77 | 0.70, 0.86 |
| Category 3 or 4 or unknown | 14,747 | 0.7 | 0.64, 0.76 | 0.95 | 0.86, 1.05 |
| Missing | 13,247 | 0.066 | 0.06, 0.08 | 0.011 | 0.01, 0.01 |
| Sex | |||||
| Female | 32,100 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Male | 16,580 | 0.86 | 0.81, 0.92 | 0.87 | 0.80, 0.95 |
| Health insurance | |||||
| No insurance | 7867 | 1 | 1 | 1.00, 1.00 | |
| Community insurance | 39,312 | 0.71 | 0.65, 0.76 | 1.7 | 1.40, 2.06 |
| Private or other government insurance (RAMA/RSSB) | 1501 | 0.41 | 0.32, 0.51 | 1.13 | 0.82, 1.56 |
| HIV | |||||
| No | 32,449 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Yes | 1829 | 0.27 | 0.19, 0.37 | 0.37 | 0.25, 0.54 |
| Missing | 14,402 | 1.34 | 1.25, 1.43 | 0.18 | 0.10, 0.31 |
| Diabetes | |||||
| No | 33,611 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Yes | 693 | 0.68 | 0.47, 0.99 | 0.57 | 0.43, 0.76 |
| Missing | 14,376 | 1.43 | 1.34, 1.54 | 1.6 | 1.07, 2.40 |
| Family history of viral hepatitis C | |||||
| No | 32,958 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Yes | 1583 | 0.57 | 0.45, 0.72 | 0.63 | 0.41, 0.98 |
| Missing | 14,139 | 1.44 | 1.35, 1.54 | 0.28 | 0.16, 0.50 |
| HBV vaccination status | |||||
| Partially or fully vaccinated | 5701 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Not vaccinated for hepatitis B | 42,979 | 6.62 | 5.15, 8.51 | 8.77 | 6.66, 11.54 |
| Treatment Failure | Dropout at SVR Assessment Stage | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Unadjusted model | Adjusted model † | Unadjusted model | Adjusted model † | ||||||
| OR | 95% CI | OR | 95% CI | N | OR | 95% CI | OR | 95% CI | ||
| Baseline viral load | 9332 | 1.12 | 1.04, 1.39 | 1.14 | 1.02, 1.28 | - | - | - | - | - |
| Age | ||||||||||
| <44 | 1227 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 | 1591 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| 44–54 | 1262 | 1.02 | 0.79, 1.32 | 1.34 | 0.93, 1.91 | 1571 | 1.02 | 0.83, 1.26 | 1.1 | 0.88, 1.39 |
| 55–64 | 2343 | 0.94 | 0.75, 1.18 | 1.18 | 0.86, 1.63 | 2968 | 0.96 | 0.80, 1.15 | 1.11 | 0.91, 1.35 |
| 64+ | 4500 | 0.94 | 0.76, 1.15 | 1.12 | 0.82, 1.53 | 6754 | 1.9 | 1.63, 2.23 | 1.42 | 1.17, 1.72 |
| Sex | ||||||||||
| Female | 5654 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 | 7939 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Male | 3678 | 1.01 | 0.87, 1.16 | 1.1 | 0.90, 1.33 | 4945 | 0.81 | 0.73, 0.90 | 0.76 | 0.67, 0.85 |
| SES | ||||||||||
| Category 1 | 1835 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 | 2573 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Category 2 | 2541 | 0.97 | 0.79, 1.18 | 0.98 | 0.76, 1.25 | 3296 | 0.89 | 0.77, 1.03 | 0.96 | 0.82, 1.14 |
| Category 3 or 4 or unknown | 3224 | 1.15 | 0.95, 1.40 | 1.13 | 0.88, 1.45 | 5174 | 0.64 | 0.56, 0.73 | 0.73 | 0.62, 0.84 |
| Missing | 1732 | 1.41 | 1.12, 1.78 | 0.61 | 0.43, 0.86 | 1841 | 3.58 | 3.01, 4.26 | 2.53 | 2.08, 3.08 |
| HIV positive | ||||||||||
| No | 7795 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 | 11,075 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Yes | 922 | 0.8 | 0.62, 1.03 | 1.09 | 0.81, 1.46 | 1125 | 0.31 | 0.25, 0.38 | 0.3 | 0.24, 0.38 |
| Missing | 615 | 5.92 | 4.73, 7.40 | 0.77 | 0.20, 3.01 | 684 | 0.076 | 0.05, 0.13 | 0.059 | 0.03, 0.11 |
| HBV Ag positive | ||||||||||
| No | 8873 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 | 12,291 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Yes | 140 | 1.27 | 0.79, 2.05 | 1.11 | 0.57, 2.18 | 274 | 0.86 | 0.57, 1.31 | 0.6 | 0.37, 0.99 |
| Missing | 319 | 2.8 | 2.00, 3.92 | 1.48 | 0.84, 2.63 | 319 | 0.73 | 0.54, 0.99 | 0.79 | 0.50, 1.22 |
| Cirrhotic | ||||||||||
| No | 8898 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 | 12,440 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Yes | 434 | 1.12 | 0.81, 1.54 | 1.71 | 1.20, 2.43 | 444 | 0.066 | 0.03, 0.13 | 0.059 | 0.03, 0.12 |
| Family history of viral hepatitis C | ||||||||||
| No | 8220 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 | 11,376 | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 |
| Yes | 437 | 1.57 | 1.17, 2.12 | 1.57 | 1.10, 2.25 | 721 | 0.42 | 0.30, 0.57 | 0.14 | 0.08, 0.24 |
| Missing | 675 | 5.96 | 4.79, 7.42 | 3.62 | 1.07, 12.31 | 787 | 0.66 | 0.53, 0.81 | 0.18 | 0.08, 0.39 |
| Ever been medically operated on | ||||||||||
| No | 8351 | 1 | 1.00, 1.00 | - | - | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 | |
| Yes | 306 | 1.34 | 0.90, 1.97 | - | - | 0.57 | 0.47, 0.68 | 0.39 | 0.27, 0.56 | |
| Missing | 675 | 5.8 | 4.71, 7.29 | - | - | 1.21 | 0.56, 1.40 | 1.44 | 0.89, 2.32 | |
| HBV vaccination status | ||||||||||
| Not vaccinated | 6985 | - | - | - | 1 | 1.00, 1.00 | 1 | 1.00, 1.00 | ||
| Partially or fully vaccinated | 2347 | - | - | - | - | 0.11 | 0.09, 0.13 | 0.14 | 0.11, 0.16 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nisingizwe, M.P.; Makuza, J.D.; Janjua, N.Z.; Bansback, N.; Hedt-Gauthier, B.; Serumondo, J.; Remera, E.; Law, M.R. The Cascade of Care for Hepatitis C Treatment in Rwanda: A Retrospective Cohort Study of the 2017–2019 Mass Screening and Treatment Campaign. Viruses 2023, 15, 661. https://doi.org/10.3390/v15030661
Nisingizwe MP, Makuza JD, Janjua NZ, Bansback N, Hedt-Gauthier B, Serumondo J, Remera E, Law MR. The Cascade of Care for Hepatitis C Treatment in Rwanda: A Retrospective Cohort Study of the 2017–2019 Mass Screening and Treatment Campaign. Viruses. 2023; 15(3):661. https://doi.org/10.3390/v15030661
Chicago/Turabian StyleNisingizwe, Marie Paul, Jean Damascene Makuza, Naveed Z. Janjua, Nick Bansback, Bethany Hedt-Gauthier, Janvier Serumondo, Eric Remera, and Michael R. Law. 2023. "The Cascade of Care for Hepatitis C Treatment in Rwanda: A Retrospective Cohort Study of the 2017–2019 Mass Screening and Treatment Campaign" Viruses 15, no. 3: 661. https://doi.org/10.3390/v15030661
APA StyleNisingizwe, M. P., Makuza, J. D., Janjua, N. Z., Bansback, N., Hedt-Gauthier, B., Serumondo, J., Remera, E., & Law, M. R. (2023). The Cascade of Care for Hepatitis C Treatment in Rwanda: A Retrospective Cohort Study of the 2017–2019 Mass Screening and Treatment Campaign. Viruses, 15(3), 661. https://doi.org/10.3390/v15030661