Abstract
Background: Four vaccines have been authorized by the European Medicines Agency (EMA): viral vector-based vaccines (AstraZeneca; AZD1222 and Johnson & Johnson; Ad26.COV2. and 2 mRNA-based vaccines (Pfizer/BioNTech; BNT162b2 and Moderna; mRNA-1273). Adverse events (AEs) related to vaccination have been described in the literature. The main aim of the dermatological practice was to avoid the diffusion of COVID-19, allowing the continuity of care for patients. Objective: The aim of this review article is to investigate current literature regarding cutaneous reactions following COVID-19 vaccination, mainly inflammatory dermatological diseases. Materials and methods: Investigated manuscripts included metanalyses, reviews, letters to the editor, real-life studies, case series, and reports. Results: We selected a total of 234 articles involving more than 550 patients. We have divided the results section into various sub-sections to ensure greater understanding for readers. Conclusions: Clinicians should keep in mind the possibility of new onsets or the worsening of several dermatoses following vaccination in order to promptly recognize and treat these AEs. Certainly, vaccination should not be discouraged.
1. Introduction
The spreading of the Coronavirus disease 2019 (COVID-19) at the beginning of the 2020 was a worldwide challenge, strongly affecting overall health, the global economy, and lifestyles [1]. In this scenario, several measures were adopted to reduce the spread of the infection [2,3]. The main aim of the dermatological practice was to avoid the diffusion of COVID-19, allowing the continuity of care for patients [3]. This outcome led to a deep change of daily clinical practice. In particular, telemedicine represented a break of the daily routine, leading to the transition from face-to-face visits to teleconsultations in order to limit the access to hospital only for severe forms of diseases as well as to reduce the risk of infection [4,5,6]. Among the several strategies adopted, a vaccination campaign was the main one. However, several doubts were raised, regarding, for example, the quick development, the slower-than-hoped-for rollout and the uncertain duration of protection [7,8,9]. Moreover, concerns were also expressed about the mechanism of action of vaccines. Indeed, vaccines for COVID-19 are based on nucleic acid-based vaccination platforms, such as viral vector platforms, messenger ribonucleic acid and inactivated viruses [7,8,9]. Currently, four vaccines have been authorized by the European Medicines Agency (EMA): viral-vector based vaccines (AstraZeneca; AZD1222 and Johnson & Johnson; Ad26.COV2.) and two mRNA-based vaccines (Pfizer/BioNTech; BNT162b2 and Moderna; mRNA-1273) [10]. Furthermore, other countries approved other vaccines such as “CoronaVac” (Sinovac), “Convidecia” (CanSino Biologics), and “Sputnik V” (Gamaleya Research Institute) [10]. Nevertheless, the vaccination campaign was a success, allowing the COVID-19 pandemic period to be overcome, and was shown to be the most efficient weapon to control and prevent the COVID-19 pandemic, the progression of the disease, hospitalization, and mortality [11]. Currently, according to the WHO COVID-19 dashboard accessed on 11 May 2023, more than 676 million cases of COVID-19 have been reported [12,13]. Similar to other vaccines, adverse events (AEs) related to vaccination have been described, including headache, diarrhea, muscle aches, fatigue, pain or redness at the injection site, fever, chills, etc. [14]. Globally, most of these AEs were limited, self-resolving and with a duration of a few days [14]. Several cutaneous reactions have been reported following vaccination [15,16,17,18,19]. Of interest, these forms of AEs have been rarely collected in clinical trials. Indeed, global mass vaccination led to the reporting of several dermatologic reactions which were not initially recognized, getting dermatologists involved in knowing how to recognize and treat them. It is of interest that a wide spectrum of cutaneous reactions has been described [15,16,17,18,19]. However, the clinical significance of these reactions as well as the pathogenetic mechanism underlying this AE is still unknown. The aim of this review article is to investigate the current literature regarding cutaneous reactions following COVID-19 vaccination, mainly inflammatory dermatological diseases, in order to provide an overview of all the cutaneous reactions following a COVID-19 vaccine and to help clinicians to better recognize and understand these dermatological conditions.
2. Material and Methods
For this review article, research of the current literature was carried out in the EBSCO, PubMed, Google Scholar, Embase, MEDLINE, and Cochrane Skin databases (until 20 April 2023). The examination was performed by searching and matching the following terms: “COVID-19”, “cutaneous reactions”, “adverse events”, “vaccination”, “lichen planus”, “psoriasis”, “atopic dermatitis”, “hidradenitis suppurativa”, “bullous disorders”, “urticaria”, “atopic eczema”, “alopecia areata”, “biologics”, “biological drugs”, “rash”, “herpes”, “chilblains”, “pityriasis rosea”, “vitiligo”, “erythematous eruption” and “inflammatory skin diseases”. Manuscripts regarding other diseases such as delayed cutaneous reactions and injection site reactions were excluded. Examined manuscripts contained reviews, metanalyses, letters to the editor, case series, real-life studies, and case reports. Manuscripts were recognized, screened, and extracted for pertinent data, following the PRISMA (preferred reporting items for systematic reviews and meta-analyses) guidelines [20]. All the references were also investigated to include articles that could have been missed. Only English-language manuscripts were evaluated in our work (Figure 1).
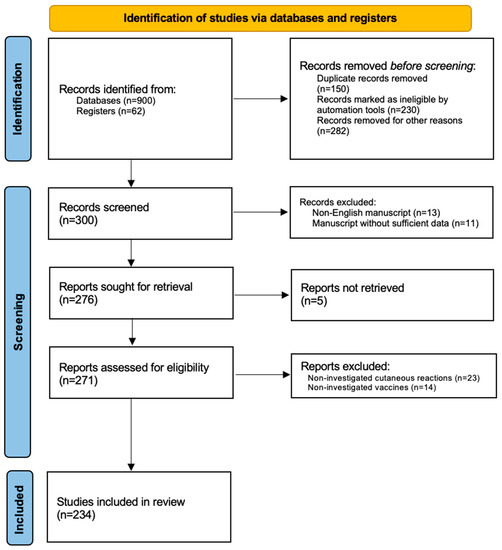
Figure 1.
PRISMA flow-chart.
In our review, we described dermatological reactions to COVID-19 vaccination, focusing mainly on inflammatory dermatological diseases such as psoriasis, lichen planus, atopic eczema, hidradenitis suppurativa, alopecia areata, also considering other cutaneous diseases (pityriasis rosea, herpes zoster, morphea, chilblains, pityriasis lichenoides et varioliformis acuta, Henoch–Schönlein purpura, lichen striatus and Rowell syndrome).
3. Results
The first research led to the discovery of 962 articles. The second research led to a skimming of 662 articles for various reasons: duplicate articles, articles not written in English. A total of 300 reports were initially found by searching the literature. Therefore, the literature review was completed by following the inclusion and exclusion criteria that we indicated in the Section 2. In the last review, in conclusion, we selected a total of 234 articles involving more than 600 patients. We have divided the Section 3 into various sub-sections to ensure greater understanding for readers; therefore, each dermatological disease will have a dedicated sub-paragraph, for example psoriasis, atopic dermatitis, hidradenitis suppurativa, lichen planus, alopecia areata, and vitiligo. Finally, we have chosen to also include a sub-paragraph with the wording “miscellaneous” where we have enclosed other dermatological pathologies found in the literature related to COVID-19 vaccination, such as morphea, chilblains, pityriasis lichenoides et varioliformis acuta, Henoch–Schönlein purpur, lichen striatus and Rowell syndrome.
3.1. Psoriasis
Psoriasis is a commonly occurring inflammatory skin disease that affects up to 3% of the adult population worldwide. A complex pathogenic mechanism is linked to several immune cells and cytokines, including tumor necrosis factors, interleukin (IL)-17, IL-22, and IL-23 [21,22,23,24]. Various psoriasis subtypes have been defined, including plaque, guttate, pustular, and nail psoriasis and psoriatic arthritis (PsA) [25,26,27,28]. The introduction of biologic treatments led to the development of new effective drugs [29,30,31,32,33]. Three years after the COVID-19 pandemic, the safety and efficacy of COVID-19 vaccines have been demonstrated for patients with psoriasis treated with systemic therapies [34,35,36,37]; guidelines have been drawn up that establish the vaccination times for people being treated with immunomodulatory drugs so as not to cause interference between the COVID-19 vaccine and the treatment [38]. What is increased are reports in the literature of new onsets or exacerbations of psoriasis. A distinction should be made in the case of psoriasis in that both new onsets of the condition and flare-ups of pre-existing psoriasis are reported for a total of 98 cases; 81 cases [39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57] involved flare-ups while the remaining 17 cases involved new onsets of psoriasis [58,59,60,61,62,63,64,65,66,67,68,69,70]. Several phenotypes have been described, such as erythrodermic, nail psoriasis, pustular psoriasis, but the plaque and guttate forms are definitely the most frequent [71,72]. Regarding the type of vaccine, most of the cases are attributed to the BNT162b2 vaccine compared to the others available; however, this data does not have much validity, as it should be emphasized that this type of vaccination was the most widely used; therefore, there is a greater risk of association of any post-vaccine dermatologic reactions. Finally, Burlando et al. reported the results of a study investigating if patients under biologics have a lower risk of psoriasis flares after COVID-19 vaccination than other psoriatic patients; their results showed that, under biologic treatment, they developed fewer psoriasis flares after COVID-19 vaccination (33.3%) than patients not under biologic treatment (66.6%) (p = 0.0207) [73]. Table 1 shows the characteristics of psoriatic reactions, the number of cases and the vaccines used.

Table 1.
Features of Psoriasis after COVID-19 vaccination.
3.2. Lichen Planus
Lichen planus (LP) is an inflammatory disease involving the skin and mucous membranes with no known cause. The lesions are pruritic, purplish papules and plaques that are mostly located on the wrists, back, and ankles [74]. To date, to the best of our knowledge, 13 cases of new onsets of the disease have been reported in the literature [75,76,77,78,79,80,81,82,83,84,85], while worsening of lichen planus after COVID-19 vaccination has been reported in three cases [84,85,86]. The underlying mechanism is certainly not known; there have been reports of new onsets of lichen planus after other vaccinations, such as that for HBV. The authors to date speculate that vaccination induces a Th1 cell response and a subsequent secretion of various cytokines that may play a key role in the development of this condition [75,76,77,78,79,80,81,82,83,84,85,86,87,88]. All articles cited with the vaccines used are given in Table 2.
Table 2.
Features of Lichen Planus after COVID-19 vaccination.
3.3. Atopic Dermatitis/Eczema
Atopic dermatitis (AD) is a chronic inflammation that causes itchy skin with a subsequent psychosocial impact on patients and family members [89,90,91]. The most frequent clinical phenotypes in adults and adolescents are flexural eczema, head and neck eczema, and hand eczema (84.9% and 84.2%, respectively); there may also be other possible presentations, such as portrait-like dermatitis (20.1%), diffuse eczema (6.5%), nummular eczema (5.8%), prurigo nodularis (2.1%), and erythroderma (0.7%) [92,93,94]. There are very few reports in the literature linking atopic dermatitis and COVID-19 vaccination. In total there are seven reports of new onsets and 14 reports of atopic dermatitis flare or eczema [95,96,97,98,99,100,101]. Eczematous reactions, particularly those localized at the injection site, were the most misdiagnosed at the beginning of the vaccination campaign. Often, injection-site reactions began with edematous or follicular phases and then evolved into urticarial or eczematous reactions; COVID-arm became a definite entity among these reaction types [102,103,104].
There were no phenotypes described that worsened with vaccination [105,106,107,108], and there were no correlations reported between patients’ current treatments with biotech drugs such as Dupilumab that could have exacerbated atopic dermatitis. Finally, there was no correlation with a particular type of COVID-19 vaccine. All data are shown in Table 3.
Table 3.
Features of Atopic Dermatitis/Eczema following COVID-19 vaccination.
3.4. Hidradenitis Suppurativa
Hidradenitis Suppurativa (HS) is a chronic, inflammatory, and debilitating disease of the skin.
The lesions are mainly nodules, fistulas, and/or abscesses of an inflammatory and painful nature affecting areas of the body rich in apocrine glands.
They usually occur after puberty, although there are reports in children and the elderly [109,110,111,112]. Our research found only one case of a new onset of HS associated with COVID-19 vaccination; specifically, Alexander et al. described the case of a 63-year-old patient who after the second dose of AstraZeneca COVID-19 vaccine developed abscesses in the left axilla, left side of the abdomen, and left groin [113].
The authors report that the AstraZeneca COVID-19 vaccine stimulates innate immune responses by involving multiple pattern recognition receptors, particularly Toll-like receptor 9; this could explain the correlation along with the timing of lesion appearance. Martora et al. described a case series of five patients, two men and three women, with a worsening of HS following COVID-19 vaccination: three patients with Moderna vaccine and two patients with Pfizer vaccine [114].
The important finding from this case series was that all patients regularly completed the vaccine course; the authors conclude that the mechanism is unknown, but it can be hypothesized that COVID-19 vaccine may inhibit the T helper 2 cell pathway and at the same time promote the T helper 1 cell pathway [114,115].
The researchers’ attention was directed toward the safety of the COVID-19 vaccine, particularly in patients with HS being treated with the only drug approved for the condition to date, adalimumab (anti TNF-alpha) [116,117].
Pakhchanian et al. conducted a large-scale study where they evaluated the efficacy and safety of COVID-19 vaccination in HS patients. The study involved the sampling of more than 3000 patients, and the authors conclude that patients with HS are not at any higher risk for any vaccine-related adverse outcomes [117].
Other studies were conducted with smaller samplings, where the authors’ findings described above were confirmed [118,119,120,121,122].
3.5. Alopecia Areata
There have been several reports of COVID-19 post-vaccination alopecia areata in recent years available in the literature [123,124,125,126,127,128,129,130,131,132,133,134,135].
There are no particular data on the type of vaccine received associated with alopecia areata; the only study in the literature on a large scale was conducted by Nguyen et al. [135]; the authors reported a total of 77 post-vaccination alopecia areata, of which 39 were new onsets and 38 were a worsening of pre-existing disease. The authors concluded their study by stating that the number was very low compared to the vaccinated population; therefore, vaccination should not be considered a risk factor in any way, and the authors urged all patients with this condition to perform the scheduled vaccination cycles [135].
3.6. Pemphigus Vulgaris and Bullous Pemphigoids
Rare diseases are defined by the European Community as diseases with a frequency ≤1 case per 2000 people (five cases per 10,000 people) [136]. Certainly, among these, autoimmune bullous diseases (pemphigus vulgaris and bullous pemphigoid) represent the most common. The management of these diseases during the pandemic has been very important in order not to abandon this type of patients; therefore, we can say that the role of the dermatologist in therapeutic management has been crucial [136].
In total, there are 66 reports in the literature of these two diseases. Precisely 26 concern pemphigus vulgaris [137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152], and 40 concern bullous pemphigoid [120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135]. These include reports of new onsets and reports of worsening of pre-existing disease [153,154,155,156,157,158,159,160,161,162,163,164,165,166,167,168]. All characteristics including the vaccine used are shown in Table 4.
Table 4.
Features of Pemphigus Vulgaris and Bullous Pemphigoid after COVID-19 vaccination.
The underlying mechanism is not known yet, but most authors write that vaccination may activate B- and T-cell immunity, triggering an autoimmune response in genetically predisposed individuals, and that this may be the most likely mechanism underlying this association. However, surely further studies are needed to confirm this hypothesis [162].
What has been crucial has been the management of these cases, where the dermatologist has been able to control these diseases without affecting the vaccine course in most cases.
3.7. Pityriasis Rosea
Pityriasis rosea (PR) is an exanthematous disease due to the endogenous systemic reactivation of human herpesvirus-6 (HHV-6) and/or -7 (HHV-7) [169].
Drago et al. have distinguished two different reactions: pityriasis rosea (PR) and PR-like eruptions (PR-LE) after COVID-19 vaccination [170,171]. PR-LE is not associated with human herpesvirus (HHV) 6 and/or 7 systemic reactivations, but it has a pathogenesis more similar to that of drug eruptions, for example, of captopril, barbiturates, isotretinoin [171].
Several clinical differences that have been proposed by the authors. Notably, itching is mild or absent in PR, while it is present and often intense in PR-LE; prodromal symptoms are absent in PR, while they are present in PR; herald patch is present in PR while they are in 25% of cases in PR-LE. Another differentiation concerns eosinophilia, which presents in about 42% of cases in PR-LE. The distribution of lesions involves the Christmas tree pattern on the trunk for PR, while the lesions are more confluent and distributed to the trunk, limbs and face in PR-LE [172,173]. Therapy is symptomatic for PR, while drug withdrawal is therapy for PR-LE [173].
There are 40 post COVID-19 vaccination reports in the literature [174,175,176,177,178,179,180,181,182,183,184,185,186,187,188,189,190,191]. Among them, 33 are reported after BNT162b2 vaccine, four after mRNA-1273 vaccine, three after AZD1222 vaccine, and one after Ad26.COV2 vaccine. The higher number associated with the Pfizer vaccine arises from the large number of vaccinations with this vaccine; there is no scientific correlation with this finding. Data in the literature have shown that SARS-CoV-2 infection may have played a role in the reactivation of HHV-6, -7 and EBV and, consequently, caused skin manifestations typical of pityriasis rosea [170].
The proposed hypothesis could confirm how vaccination could cause an immunosuppressive state secondary to a decrease in the amount of T lymphocytes, so a reactivation of some viruses would be explained, including pityriasis rosea [170].
Finally, a recent review showed that the association between pityriasis rosea and pityriasis rosea-like eruptions after COVID-19 vaccination is possible, but given the scarcity of studies, more studies are required to confirm this association as well as the etiology and mechanism of the disease [192].
3.8. Urticaria
In our review, 98 cases have been collected, also during treatment with omalizumab [95,96,101,193,194,195,196,197,198,199,200,201,202,203,204,205,206]. Of note, two types of urticaria may be distinguished: immediate and delayed, with the first as the most common, as reported by Wang et al. in their monocentric real-life study investigating cutaneous manifestations following vaccination [207] (Table 5).
Table 5.
Features of urticarial rashes after COVID-19 vaccination.
3.9. Herpes Zoster
Varicella zoster virus (VZV) is a commonly encountered infectious disease in dermatology presenting as varicella/chickenpox or herpes zoster. Reactivation is most common in the elderly population, most commonly in individuals aged 60 years and older, the main triggers being decreased cell-mediated immunity often caused by factors such as vaccinations that lead to an aggravation of the immune system [208].
Reviewing the literature, there are 55 reports of herpes zoster post-vaccination, among them 33 post-BNT162b2 vaccine, five post-mRNA-1273 vaccine, while 19 were reported post-AZD1222 vaccine [208,209,210,211,212,213,214,215,216,217]. All authors conclude that, again, the risk of possible development of this reaction is far lower than the safety and efficacy of COVID-19 vaccination, so it is not a contraindication for the first dose or subsequent booster doses [208,209,210,211,212,213,214,215,216,217].
3.10. Miscellaneous
Regarding other cutaneous diseases developed following COVID-19 vaccination available or reported in literature, we have found nine cases of morphea [218,219,220,221,222,223], and 11 cases of vitiligo [224,225,226,227,228,229,230,231,232,233,234]. Other dermatoses have been described, such as chilblains, pityriasis lichenoides et varioliformis acuta, Henoch–Schönlein purpur, lichen striatus or Rowell syndrome, Sweet Syndrome, dermatomyositis, and exanthematous pustulosis. Nevertheless, these are reports of a few cases suggesting this association with the COVID-19 vaccination. Therefore, we believe that unlike the other reactions we have reported, where both the numbers and the mechanisms proposed at the base are valid, in these cases certainly further studies will be necessary to establish the true correlation [235,236,237,238,239,240,241,242,243,244].
4. Discussion
The COVID-19 pandemic revolutionized medical routine dermatological clinical practice [245]. Indeed, several measures were adopted to contain the spread of the infection as well as to guarantee the continuity of care, particularly for the oncodermatological field [246,247,248,249,250,251] as well as for patients undergoing biological treatments [252]. In this scenario, dermatologists were involved and forced to change their clinical routine to guarantee the continuity of care for patients with chronic inflammatory disease undergoing biological or other systemic treatments as well as to avoid the reduction in the diagnosis and treatment of several conditions, mainly melanoma and non-melanoma skin cancer [251,252,253,254]. Teledermatological services were shown to be a useful tool in this context, allowing clinicians to continuously assist patients’ diseases with promising results in terms of clinical outcomes, patient satisfaction, and treatment adherence [255,256]. Subsequently, COVID-19 vaccines were developed to overcome the pandemic period. Vaccination campaigns were successful, showing excellent results in terms of safety and efficacy [257]. Even if several concerns were raised about the effective and safe profile of vaccines, the diffusion of vaccinations allowed every doubt to be clarified [34,258]. However, several AEs were described following vaccination. Among these, several cutaneous diseases (lichen planus, psoriasis, atopic dermatitis, hidradenitis suppurativa, bullous disorders, eczema, urticaria, atopic eczema, alopecia areata, chilblains, pityriasis rosea, vitiligo, etc.) developed or exacerbated after COVID-19 vaccination have been described. Globally, most of these reactions were mild and self-limited, not requiring medical attention. For the same reason, most of these cutaneous AEs were not reported, as patients tended to self-medicate, without seeking medical advice. To date, dermatologic reports after the first vaccination are at one case in a million. At the same time, it is still unclear whether repeated doses of vaccination according to the schedule can affect the decrease in these events. In this context, we performed a review article with the aim of reporting data on cutaneous reactions described following COVID-19 vaccination in order to offer a wide perspective as well as trying to underline possible pathogenetic factors. As regards their pathogenesis, cutaneous reactions were reported following vaccination with both viral vector-based and mRNA vaccines, suggesting that the pathogenetic mechanism underlying the cutaneous reaction is not directly connected with the mechanism of action of the vaccine itself. Certainly, mRNA vaccines seem to be more commonly related to cutaneous reactions. However, mRNA vaccines have been the more used, as they were previously authorized and administered worldwide. Moreover, cutaneous reactions were reported following the first, the second and the third dose of vaccines, highlighting that each dose may be related to the development of AEs. Thus, more studies are required to recognize the pathogenetic mechanisms related to cutaneous reactions following COVID-19 vaccination in order to identify “at-risk” patients and to adopt preventive strategies. Certainly, further epidemiological studies will help to clarify if the percentage of cutaneous reactions following vaccination is significantly higher in one of the two types of vaccines, with clinical implications. Despite not being specifically investigated, local injection-site reactions were the commonest cutaneous vaccine-related AEs collected. As regards cutaneous inflammatory disease, there are several reports of their new onset or worsening following COVID-19 vaccination. However, the chronic relapsing course of these diseases does not allow the casual correlation to be excluded in most of the cases. Thus, the exact link between vaccination and cutaneous AE has not been elucidated. Of interest, viral reactivations (e.g., EBV reactivation, other herpesviruses) have also been reported in a minority of cases following COVID-19 vaccination [258,259,260,261].
To sum up, our review manuscript investigated several dermatoses developed or exacerbated following COVID-19 vaccination. However, the causality of the temporal association between the administration of the vaccine and the development of skin reactions cannot be ruled out. As regards the dose of vaccine, cutaneous reactions were described following both the first and the second dose of vaccine, while cutaneous AEs were also reported after the third (booster) dose of vaccination. In our opinion, clinicians should keep in mind the possibility of the development or new onset of cutaneous AEs following vaccination, regardless of the dose and the mechanism of action of the vaccine.
Strengths and Limitations
The main strengths of this review article are the systematic method used for the literature research as well as the elevated number of investigated articles and analyzed cutaneous reactions. However, the main limitations must be discussed. First of all, only the four vaccines approved by EMA have been considered in this manuscript, excluding cutaneous reactions related to other COVID-19 vaccines. Furthermore, many manuscripts reporting registry-based studies did not allow direct correlations to be established between cutaneous reactions and the type of vaccine. Post-vaccination dermatology reports often contain case reports or small case series; there is a lack of guidelines for the management of these manifestations, as each case certainly needs to be treated according to the pathology, and treatment may depend on various factors. In addition, the causal temporal correlation between cutaneous reaction and vaccination cannot be ruled out in most of the cases.
Moreover, dermatological conditions exacerbated or developed following COVID-19 vaccines are usually mild, and patients do not seek medical attention, reducing the possibility to point out the exact incidence of these reactions.
Finally, our assumptions, mainly in the discussion, must be taken simply as suggestions and not as definite proposals, as our work has not had the support of meta-analysis, which may allow our results to be generalized.
5. Conclusions
Vaccination campaigns were the main weapon to overcome the COVID-19 pandemic period. With the progress of vaccination programs, several cutaneous reactions have been reported; most of these were not previously assessed in clinical trials. Fortunately, the percentage of these AEs is extremely low if compared with the number of vaccines administered. In our opinion, other cutaneous reactions related to COVID-19 vaccination will be described. Furthermore, the pathogenetic mechanisms linking vaccination and skin reactions should be investigated to identify “at-risk” patients and adopt preventative measures. To sum up, clinicians should keep in mind the possibility of new onsets or the worsening of several dermatoses following vaccination in order to promptly recognize and treat these AEs. Certainly, vaccination should not be discouraged.
Author Contributions
F.M.—Conceptualization, validation, visualization, writing-original draft preparation, writing—review & editing. L.P.—Conceptualization, validation, visualization, writing-original draft preparation, writing—review & editing. M.S.—Conceptualization, validation, visualization, writing-review & editing, supervision. validation, visualization. A.R.—Conceptualization, validation, visualization, writing-review & editing, supervision. T.B.—Conceptualization, validation, visualization, writing-original draft preparation, writing—review & editing. M.M.—Conceptualization, validation, visualization, writing-original draft preparation, writing—review & editing. A.V.—Conceptualization, validation, visualization, writing-original draft preparation, writing—review & editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent has been obtained from the patient(s) to publish this paper. Patient’s gave the consent for photo acquisition and publication.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Shivalkar, S.; Pingali, M.S.; Verma, A.; Singh, A.; Singh, V.; Paital, B.; Das, D.; Varadwaj, P.K.; Samanta, S.K. Outbreak of COVID-19: A Detailed Overview and Its Consequences. Adv. Exp. Med. Biol. 2021, 1353, 23–45. [Google Scholar] [CrossRef]
- De Lucia, M.; Potestio, L.; Costanzo, L.; Fabbrocini, G.; Gallo, L. Scabies outbreak during COVID-19: An Italian experience. Int. J. Dermatol. 2021, 60, 1307–1308. [Google Scholar] [CrossRef]
- Ibrahim, A.E.; Magdy, M.; Khalaf, E.M.; Mostafa, A.; Arafa, A. Teledermatology in the time of COVID-19. Int. J. Clin. Pract. 2021, 75, e15000. [Google Scholar] [CrossRef] [PubMed]
- Megna, M.; Camela, E.; Villani, A.; Tajani, A.; Fabbrocini, G.; Potestio, L. Teledermatology: A useful tool also after COVID-19 era? J. Cosmet. Dermatol. 2022, 21, 2309–2310. [Google Scholar] [CrossRef] [PubMed]
- McKoy, K.; Halpern, S.; Mutyambizi, K. International Teledermatology Review. Curr. Dermatol. Rep. 2021, 10, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Marasca, C.; Annunziata, M.C.; Camela, E.; Di Guida, A.; Fornaro, L.; Megna, M.; Napolitano, M.; Patruno, C.; Potestio, L.; Fabbrocini, G. Teledermatology and Inflammatory Skin Conditions during COVID-19 Era: New Perspectives and Applications. J. Clin. Med. 2022, 11, 1511. [Google Scholar] [CrossRef]
- Olusanya, O.A.; Bednarczyk, R.A.; Davis, R.L.; Shaban-Nejad, A. Addressing Parental Vaccine Hesitancy and Other Barriers to Child-hood/Adolescent Vaccination Uptake During the Coronavirus (COVID-19) Pandemic. Front. Immunol. 2021, 12, 663074. [Google Scholar] [CrossRef]
- Hudson, A.; Montelpare, W.J. Predictors of Vaccine Hesitancy: Implications for COVID-19 Public Health Messaging. Int. J. Environ. Res. Public Health 2021, 18, 8054. [Google Scholar] [CrossRef]
- Sharif, N.; Alzahrani, K.J.; Ahmed, S.N.; Dey, S.K. Efficacy, Immunogenicity and Safety of COVID-19 Vaccines: A Systematic Review and Meta-Analysis. Front. Immunol. 2021, 12, 714170. [Google Scholar] [CrossRef]
- European Medicines Agency. COVID-19 Vaccines: Authorised. Available online: https://www.ema.europa.eu/en/human-regulatory/overview/public-health-threats/coronavirus-disease-COVID-19/treatments-vaccines/vaccines-COVID-19/COVID-19-vaccines-authorised (accessed on 18 May 2023).
- Martora, F.; Battista, T.; Marasca, C.; Genco, L.; Fabbrocini, G.; Potestio, L. Cutaneous Reactions Following COVID-19 Vaccination: A Review of the Current Literature. Clin. Cosmet. Investig. Dermatol. 2022, 15, 2369–2382. [Google Scholar] [CrossRef]
- COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Available online: https://coronavirus.jhu.edu/map.html (accessed on 8 June 2020).
- COVID-19 Vaccine Tracker and Landscape. Available online: https://www.who.int/publications/m/item/draft-landscape-of-COVID-19-candidate-vaccines (accessed on 18 May 2023).
- Klein, N.P.; Lewis, N.; Goddard, K.; Fireman, B.; Zerbo, O.; Hanson, K.E.; Donahue, J.G.; Kharbanda, E.O.; Naleway, A.; Nelson, J.C.; et al. Surveillance for Adverse Events after COVID-19 mRNA Vaccination. JAMA 2021, 326, 1390. [Google Scholar] [CrossRef]
- Potestio, L.; Fabbrocini, G.; D’Agostino, M.; Piscitelli, I.; Martora, F. Cutaneous reactions following COVID-19 vaccination: The evidence says “less fear”. J. Cosmet. Dermatol. 2023, 22, 28–29. [Google Scholar] [CrossRef] [PubMed]
- Martora, F.; Villani, A.; Marasca, C.; Fabbrocini, G.; Potestio, L. Skin reaction after SARS-CoV-2 vaccines Reply to ‘cutaneous adverse reactions following SARS-CoV-2 vaccine booster dose: A real-life multicentre experience’. J. Eur. Acad. Dermatol. Venereol. 2022, 37, e43–e44. [Google Scholar] [CrossRef] [PubMed]
- Martora, F.; Villani, A.; Battista, T.; Fabbrocini, G.; Potestio, L. COVID-19 vaccination and inflammatory skin diseases. J. Cosmet. Dermatol. 2022, 22, 32–33. [Google Scholar] [CrossRef]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based COVID-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, A.; Martora, F.; Fabbrocini, G.; Villani, A.; Marasca, C.; Megna, M.; Fornaro, L.; Comune, R.; Potestio, L. The Role of Teledermatology During the COVID-19 Pandemic: A Narrative Review. Clin. Cosmet. Investig. Dermatol. 2022, 15, 2785–2793. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 2021, 372, n71. [Google Scholar] [CrossRef]
- Wu, P.-C.; Huang, I.-H.; Wang, C.-W.; Tsai, C.-C.; Chung, W.-H.; Chen, C.-B. New Onset and Exacerbations of Psoriasis Following COVID-19 Vaccines: A Systematic Review. Am. J. Clin. Dermatol. 2022, 23, 775–799. [Google Scholar] [CrossRef]
- Ruggiero, A.; Martora, F.; Picone, V.; Potestio, L.; Camela, E.; Battista, T.; Fabbrocini, G.; Megna, M. The impact of COVID-19 infection on patients with psoriasis treated with biologics: An Italian experience. Clin. Exp. Dermatol. 2022, 47, 2280–2282. [Google Scholar] [CrossRef]
- Ruggiero, A.; Picone, V.; Martora, F.; Fabbrocini, G.; Megna, M. Guselkumab, Risankizumab, and Tildrakizumab in the Management of Psoriasis: A Review of the Real-World Evidence. Clin. Cosmet. Investig. Dermatol. 2022, 15, 1649–1658. [Google Scholar] [CrossRef]
- Marasca, C.; Fornaro, L.; Martora, F.; Picone, V.; Fabbrocini, G.; Megna, M. Onset of vitiligo in a psoriasis patient on ixekizumab. Dermatol. Ther. 2021, 34, e15102. [Google Scholar] [CrossRef] [PubMed]
- Pathmarajah, P.; Benjamin-Laing, Z.; Abdurrahman, M.; Grunova, A.; Sinclair, C. Generalized vitiligo in a psoriatic patient treated with ixekizumab. Dermatol. Ther. 2022, 35, e15872. [Google Scholar] [CrossRef] [PubMed]
- Coates, L.C.; Helliwell, P.S. Psoriatic arthritis: State of the art review. Clin. Med. 2017, 17, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Megna, M.; Potestio, L.; Fabbrocini, G.; Camela, E. Treating psoriasis in the elderly: Biologics and small molecules. Expert Opin. Biol. Ther. 2022, 22, 1503–1520. [Google Scholar] [CrossRef] [PubMed]
- Megna, M.; Camela, E.; Battista, T.; Genco, L.; Martora, F.; Noto, M.; Picone, V.; Ruggiero, A.; Monfrecola, G.; Fabbrocini, G.; et al. Efficacy and safety of biologics and small molecules for psoriasis in pediatric and geriatric populations. Part I: Focus on pediatric patients. Expert Opin. Drug Saf. 2023, 22, 25–41. [Google Scholar] [CrossRef]
- Megna, M.; Ruggiero, A.; Battista, T.; Marano, L.; Cacciapuoti, S.; Potestio, L. Long-Term Efficacy and Safety of Risankizumab for Moderate to Severe Psoriasis: A 2-Year Real-Life Retrospective Study. J. Clin. Med. 2023, 12, 3233. [Google Scholar] [CrossRef]
- Megna, M.; Potestio, L.; Camela, E.; Fabbrocini, G.; Ruggiero, A. Ixekizumab and brodalumab indirect comparison in the treatment of moderate to severe psoriasis: Results from an Italian single-center retrospective study in a real-life setting. Dermatol. Ther. 2022, 35, e15667. [Google Scholar] [CrossRef]
- Ruggiero, A.; Potestio, L.; Cacciapuoti, S.; Gallo, L.; Battista, T.; Camela, E.; Fabbrocini, G.; Megna, M. Tildrakizumab for the treatment of moderate to severe psoriasis: Results from a single center preliminary real-life study. Dermatol. Ther. 2022, 35, e15941. [Google Scholar] [CrossRef]
- Ruggiero, A.; Camela, E.; Potestio, L.; Fabbrocini, G.; Megna, M. Drug safety evaluation of tildrakizumab for psoriasis: A review of the current knowledge. Expert Opin. Drug Saf. 2022, 21, 1445–1451. [Google Scholar] [CrossRef]
- Megna, M.; Camela, E.; Battista, T.; Genco, L.; Martora, F.; Noto, M.; Picone, V.; Ruggiero, A.; Monfrecola, G.; Fabbrocini, G.; et al. Efficacy and safety of biologics and small molecules for psoriasis in pediatric and geriatric populations. Part II: Focus on elderly patients. Expert Opin. Drug Saf. 2023, 22, 43–58. [Google Scholar] [CrossRef]
- Wack, S.; Patton, T.; Ferris, L.K. COVID-19 vaccine safety and efficacy in patients with immune-mediated inflammatory disease: Review of available evidence. J. Am. Acad. Dermatol. 2021, 85, 1274–1284. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Geat, D.; Naldi, L.; Piaserico, S. Insights into SARS-CoV-2 vaccination in patients with chronic plaque psoriasis on systemic treatments. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e361–e362. [Google Scholar] [CrossRef] [PubMed]
- Skroza, N.; Bernardini, N.; Tolino, E.; Proietti, I.; Mambrin, A.; Marchesiello, A.; Marraffa, F.; Rossi, G.; Volpe, S.; Potenza, C. Safety and impact of anti-COVID-19 vaccines in psoriatic patients treated with bio-logics: A real life experience. J. Clin. Med. 2021, 10, 3355. [Google Scholar] [CrossRef] [PubMed]
- Furer, V.; Eviatar, T.; Zisman, D.; Peleg, H.; Paran, D.; Levartovsky, D.; Zisapel, M.; Elalouf, O.; Kaufman, I.; Meidan, R.; et al. Immunogenicity and safety of the BNT162b2 mRNA COVID-19 vaccine in adult patients with autoimmune inflammatory rheumatic diseases and in the general population: A multicentre study. Ann. Rheum. Dis. 2021, 80, 1330–1338. [Google Scholar] [CrossRef] [PubMed]
- Potestio, L.; Martora, F.; Fabbrocini, G.; Battista, T.; Megna, M. Safety and Efficacy of COVID-19 Vaccination in Patients Undergoing Biological Treatments for Psoriasis. Psoriasis (Auckl) 2023, 13, 11–18. [Google Scholar] [CrossRef]
- Huang, Y.-W.; Tsai, T.-F. Exacerbation of Psoriasis Following COVID-19 Vaccination: Report from a Single Center. Front. Med. 2021, 8, 812010. [Google Scholar] [CrossRef]
- Sotiriou, E.; Tsentemeidou, A.; Bakirtzi, K.; Lallas, A.; Ioannides, D.; Vakirlis, E. Psoriasis exacerbation after COVID-19 vaccination: A report of 14 cases from a single centre. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e857–e859. [Google Scholar] [CrossRef]
- Koumaki, D.; Krueger-Krasagakis, S.; Papadakis, M.; Katoulis, A.; Gkiaouraki, I.; Zografaki, K.; Mylonakis, D.; Krasagakis, K. Psoriasis flare-up after AZD1222 and BNT162b2 COVID-19 mRNA vaccines: Report of twelve cases from a single centre. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e411–e415. [Google Scholar] [CrossRef]
- Megna, M.; Potestio, L.; Gallo, L.; Caiazzo, G.; Ruggiero, A.; Fabbrocini, G. Reply to “Psoriasis exacerbation after COVID-19 vaccination: Report of 14 cases from a single centre” by Sotiriou E et al. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e11–e13. [Google Scholar] [CrossRef]
- Durmaz, I.; Turkmen, D.; Altunisik, N.; Toplu, S.A. Exacerbations of generalized pustular psoriasis, palmoplantar psoriasis, and psoriasis vulgaris after mRNA COVID-19 vaccine: A report of three cases. Dermatol. Ther. 2022, 35, e15331. [Google Scholar] [CrossRef]
- Tran, T.B.; Pham, N.T.; Phan, H.N.; Nguyen, H.T. Generalized erythrodermic psoriasis triggered by vaccination against severe acute res-piratory syndrome coronavirus 2. Dermatol. Ther. 2022, 35, e15464. [Google Scholar] [CrossRef]
- Nagrani, P.; Jindal, R.; Goyal, D. Onset/flare of psoriasis following the ChAdOx1 nCoV-19 Corona virus vaccine (Ox-ford-AstraZeneca/Covishield): Report of two cases. Dermatol. Ther. 2021, 34, e15085. [Google Scholar] [CrossRef] [PubMed]
- Piccolo, V.; Russo, T.; Mazzatenta, C.; Bassi, A.; Argenziano, G.; Cutrone, M.; Darlington, M.E.S.D.; Grimalt, R. COVID vaccine-induced pustular psoriasis in patients with previous plaque type psoriasis. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e330–e332. [Google Scholar] [CrossRef]
- Bostan, E.; Elmas, L.; Yel, B.; Yalici-Armagan, B. Exacerbation of plaque psoriasis after inactivated and BNT162b2 mRNA COVID-19 vaccines: A report of two cases. Dermatol. Ther. 2021, 34, e15110. [Google Scholar] [CrossRef]
- Pavia, G.; Gargiulo, L.; Spinelli, F.; Avagliano, J.; Valenti, M.; Borroni, R.G.; Costanzo, A.; Narcisi, A. Generalized pustular psoriasis flare in a patient affected by plaque psoriasis after BNT162b2 mRNA COVID-19 vaccine, successfully treated with risankizumab. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e502–e505. [Google Scholar] [CrossRef] [PubMed]
- Durmus, O.; Akdogan, N.; Karadag, O.; Gokoz, O. Erythroderma related with the first dose of Pfizer-BioNTech BNT16B2b2 COVID-19 mRNA vaccine in a patient with psoriasis. Dermatol Ther. 2022, 35, e15363. [Google Scholar] [CrossRef] [PubMed]
- Fang, W.C.; Chiu, L.W.; Hu, S.C. Psoriasis exacerbation after first dose of AstraZeneca coronavirus disease 2019 vaccine. J Dermatol. 2021, 48, e566–e567. [Google Scholar] [CrossRef] [PubMed]
- Krajewski, P.K.; Szepietowski, J.C. Psoriasis flare-up associated with second dose of Pfizer-BioNTech BNT16B2b2 COVID-19 mRNA vaccine. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e632–e634. [Google Scholar] [CrossRef]
- Trepanowski, N.; Coleman, E.L.; Melson, G.; Brem, C.E.; Lam, C.S. Erythrodermic psoriasis after COVID-19 vaccination. JAAD Case Rep. 2022, 28, 123–126. [Google Scholar] [CrossRef]
- Mieczkowska, K.; Kaubisch, A.; McLellan, B.N. Exacerbation of psoriasis following COVID-19 vaccination in a patient previously treated with PD-1 inhibitor. Dermatol. Ther. 2021, 34, e15055. [Google Scholar] [CrossRef]
- Lopez, E.D.; Javed, N.; Upadhyay, S.; Shekhar, R.; Sheikh, A.B. Acute exacerbation of psoriasis after COVID-19 Pfizer vaccination. Bayl. Univ. Med. Cent. Proc. 2021, 35, 199–201. [Google Scholar] [CrossRef] [PubMed]
- Perna, D.; Jones, J.; Schadt, C.R. Acute generalized pustular psoriasis exacerbated by the COVID-19 vaccine. JAAD Case Rep. 2021, 17, 1–3. [Google Scholar] [CrossRef]
- Tsunoda, K.; Watabe, D.; Amano, H. Exacerbation of psoriasis following vaccination with the Pfizer-BioNTech BTN162b2 mRNA COVID-19 vaccine during risankizumab treatment. J. Dermatol. 2022, 50, e79–e80. [Google Scholar] [CrossRef] [PubMed]
- Lamberti, A.; Lora, V.; Graceffa, D.; Bonifati, C.; Cota, C. Nail psoriasis: A rare mRNA COVID-19 vaccine reaction. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e745–e746. [Google Scholar] [CrossRef]
- Tran, T.N.; Nguyen, T.T.; Pham, N.N.; Pham, N.T.; Vu, T.T.; Nguyen, H.T. New onset of psoriasis following COVID-19 vaccination. Dermatol. Ther. 2022, 35, e15590. [Google Scholar] [CrossRef] [PubMed]
- Frioui, R.; Chamli, A.; Zaouak, A.; Hlel, I.; Khanchel, F.; Fenniche, S.; Hammami, H. A case of new-onset acute generalized pustular psoriasis following Pfizer-BioNTech COVID-19 vaccine. Dermatol. Ther. 2022, 35, e15444. [Google Scholar] [CrossRef]
- Cortonesi, G.; Orsini, C.; Rubegni, P.; Trovato, E. New-onset psoriasis after Comirnaty (BNT162b2, BioNTech/Pfizer) vaccine successfully treated with ixekizumab. Dermatol. Ther. 2022, 35, e15606. [Google Scholar] [CrossRef]
- Wei, N.; Kresch, M.; Elbogen, E.; Lebwohl, M. New onset and exacerbation of psoriasis after COVID-19 vaccination. JAAD Case Rep. 2022, 19, 74–77. [Google Scholar] [CrossRef]
- Lehmann, M.; Schorno, P.; Hunger, R.; Heidemeyer, K.; Feldmeyer, L.; Yawalkar, N. New onset of mainly guttate psoriasis after COVID-19 vaccination: A case report. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e752–e755. [Google Scholar] [CrossRef]
- Elamin, S.; Hinds, F.; Tolland, J. De novo generalized pustular psoriasis following Oxford-AstraZeneca COVID-19 vaccine. Clin. Exp. Dermatol. 2022, 47, 153–155. [Google Scholar] [CrossRef]
- Song, W.J.; Lim, Y.; Jo, S.J. De novo guttate psoriasis following coronavirus disease 2019 vaccination. J. Dermatol. 2021, 49, e30–e31. [Google Scholar] [CrossRef] [PubMed]
- Ouni, N.; Korbi, M.; Chahed, F.; Ben Fadhel, N.; Bellalah, A.; Belhadjali, H.; Aouam, K.; Zili, J. New-onset guttate psoriasis following coronavirus disease 2019 vaccination: About two cases. Dermatol. Ther. 2022, 35, e15617. [Google Scholar] [CrossRef] [PubMed]
- Romagnuolo, M.; Pontini, P.; Muratori, S.; Marzano, A.V.; Moltrasio, C. De novo annular pustular psoriasis following mRNA COVID-19 vaccine. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e603–e605. [Google Scholar] [CrossRef] [PubMed]
- Nia, A.M.; Silva, M.M.; Spaude, J.; Gonzalez-Fraga, J.D. Erythrodermic psoriasis eruption associated with SARS-CoV-2 vaccination. Dermatol. Ther. 2022, 35, e15380. [Google Scholar] [CrossRef]
- Lamberti, A.; Lora, V.; Graceffa, D.; Bonifati, C.; Cota, C. Reply to ‘Nail psoriasis: A rare mRNA COVID-19 vaccine reaction’ by Lamberti A et al. J. Eur. Acad. Dermatol. Venereol. 2023, 37, e41–e42. [Google Scholar]
- Ricardo, J.W.; Lipner, S.R. Case of de novo nail psoriasis triggered by the second dose of Pfizer-BioNTech BNT162b2 COVID-19 messenger RNA vaccine. JAAD Case Rep. 2021, 17, 18–20. [Google Scholar] [CrossRef]
- Pesqué, D.; Lopez-Trujillo, E.; Marcantonio, O.; Giménez-Arnau, A.M.; Pujol, R.M. New-onset and exacerbations of psoriasis after mRNA COVID-19 vaccines: Two sides of the same coin? J. Eur. Acad. Dermatol. Venereol. 2022, 36, e80–e81. [Google Scholar] [CrossRef]
- Megna, M.; Potestio, L.; Fabbrocini, G.; Cinelli, E. Tildrakizumab: A new therapeutic option for erythrodermic psoriasis? Dermatol. Ther. 2021, 34, e15030. [Google Scholar] [CrossRef]
- Megna, M.; Ocampo-Garza, S.S.; Potestio, L.; Fontanella, G.; Gallo, L.; Cacciapuoti, S.; Ruggiero, A.; Fabbrocini, G. New-Onset Psoriatic Arthritis under Biologics in Psoriasis Patients: An Increasing Challenge? Biomedicines 2021, 9, 1482. [Google Scholar] [CrossRef]
- Burlando, M.; Herzum, A.; Cozzani, E.; Parodi, A. Psoriasis flares after COVID-19 vaccination: Adherence to biologic therapy reduces psoriasis exacerbations: A case-control study. Clin. Exp. Vaccine Res. 2023, 12, 80–81. [Google Scholar] [CrossRef]
- Arnold, D.L.; Krishnamurthy, K. Lichen Planus. In StatPearls; StatPearls Publishing: Tampa, FL, USA, 2022. [Google Scholar]
- Merhy, R.; Sarkis, A.S.; Kaikati, J.; El Khoury, L.; Ghosn, S.; Stephan, F. New-onset cutaneous lichen planus triggered by COVID-19 vaccination. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e729–e730. [Google Scholar] [CrossRef] [PubMed]
- Gamonal, S.B.; Gamonal, A.C.; Marques, N.C.; Adário, C.L. Lichen planus and vitiligo occurring after ChAdOx1 nCoV-19 vaccination against SARS-CoV-2. Dermatol. Ther. 2022, 35, e15422. [Google Scholar] [CrossRef]
- Alrawashdeh, H.M.; Al-Habahbeh, O.; Naser, A.Y.; Serhan, H.A.; Hamdan, O.; Sweiss, K.; Aldalameh, Y.; Alrawashdeh, H.; Hamdan, O.K. Lichen planus eruption following oxford-AstraZeneca COVID-19 vaccine administration: A case report and review of literature. Cureus 2022, 14, e22669. [Google Scholar] [CrossRef] [PubMed]
- Shakoei, S.; Kalantari, Y.; Nasimi, M.; Tootoonchi, N.; Ansari, M.S.; Razavi, Z.; Etesami, I. Cutaneous manifestations following COVID-19 vaccination: A report of 25 cases. Dermatol. Ther. 2022, 35, e15651. [Google Scholar] [CrossRef] [PubMed]
- Hiltun, I.; Sarriugarte, J.; Martínez-De-Espronceda, I.; Garcés, A.; Llanos, C.; Vives, R.; Yanguas, J. Lichen planus arising after COVID-19 vaccination. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e414–e415. [Google Scholar] [CrossRef] [PubMed]
- Herzum, A.; Burlando, M.; Molle, M.F.; Micalizzi, C.; Cozzani, E.; Parodi, A. Lichen planus flare following COVID-19 vaccination: A case report. Clin. Case Rep. 2021, 9, e05092. [Google Scholar] [CrossRef]
- Kato, J.; Kamiya, T.; Handa, T.; Kobayashi, E.; Hida, T.; Yamashita, T.; Uhara, H. Linear lichen planus after COVID-19 vaccination. Australas. J. Dermatol. 2022, 63, e385–e387. [Google Scholar] [CrossRef]
- Diab, R.; Araghi, F.; Gheisari, M.; Kani, Z.A.; Moravvej, H. Lichen planus and lichen planopilaris flare after COVID-19 vaccination. Dermatol. Ther. 2022, 35, e15283. [Google Scholar] [CrossRef]
- Zagaria, O.; Villani, A.; Ruggiero, A.; Potestio, L.; Fabbrocini, G.; Gallo, L. New-onset lichen planus arising after COVID-19 vaccination. Dermatol Ther. 2022, 35, e15374. [Google Scholar] [CrossRef]
- Awada, B.; Abdullah, L.; Kurban, M.; Abbas, O. Inverse lichen planus post Oxford-AstraZeneca COVID-19 vaccine. J. Cosmet. Dermatol. 2022, 21, 883–885. [Google Scholar] [CrossRef]
- Picone, V.; Fabbrocini, G.; Martora, L.; Martora, F. A Case of New-Onset Lichen Planus after COVID-19 Vaccination. Dermatol. Ther. 2022, 12, 801–805. [Google Scholar] [CrossRef]
- Hlaca, N.; Zagar, T.; Kastelan, M.; Peternel, S.; Brajac, I.; Prpic-Massari, L. New-onset lichen planus and lichen planus flare in elderly women after COVID-19 vaccination. J. Cosmet. Dermatol. 2022, 21, 3679–3681. [Google Scholar] [CrossRef] [PubMed]
- Zengarini, C.; Piraccini, B.M.; La Placa, M. Lichen Ruber Planus occurring after SARS-CoV-2 vaccination. Dermatol. Ther. 2022, 35, e15389. [Google Scholar] [CrossRef]
- Masseran, C.; Calugareanu, A.; Caux, F.; Bohelay, G. Extensive cutaneous lichen planus triggered by viral vector COVID-19 vaccination (ChAdOx1 nCoV-19). J. Eur. Acad. Dermatol. Venereol. 2022, 36, e263–e265. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, M.; Fabbrocini, G.; Potestio, L.; Fontanella, G.; Picone, V.; Bennardo, L.; Scalvenzi, M.; Patruno, C. A 24-weeks real-world experience of dupilumab in adolescents with moder-ate-to-severe atopic dermatitis. Dermatol. Ther. 2022, 35, e15588. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, M.; Maffei, M.; Patruno, C.; Leone, C.A.; Di Guida, A.; Potestio, L.; Scalvenzi, M.; Fabbrocini, G. Dupilumab effectiveness for the treatment of patients with concomitant atopic dermatitis and chronic rhinosinusitis with nasal polyposis. Dermatol. Ther. 2021, 34, e15120. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, M.; Fabbrocini, G.; Neri, I.; Stingeni, L.; Boccaletti, V.; Piccolo, V.; Amoruso, G.F.; Malara, G.; De Pasquale, R.; Di Brizzi, E.V.; et al. Dupilumab Treatment in Children Aged 6–11 Years With Atopic Dermatitis: A Multicentre, Real-Life Study. Paediatr. Drugs. 2022, 24, 671–678. [Google Scholar] [CrossRef]
- Napolitano, M.; Fabbrocini, G.; Martora, F.; Picone, V.; Morelli, P.; Patruno, C. Role of Aryl Hydrocarbon Receptor Activation in Inflammatory Chronic Skin Diseases. Cells 2021, 10, 3559. [Google Scholar] [CrossRef]
- Cantelli, M.; Martora, F.; Patruno, C.; Nappa, P.; Fabbrocini, G.; Napolitano, M. Upadacitinib improved alopecia areata in a patient with atopic dermatitis: A case report. Dermatol. Ther. 2022, 35, e15346. [Google Scholar] [CrossRef]
- Napolitano, M.; Fabbrocini, G.; Genco, L.; Martora, F.; Potestio, L.; Patruno, C. Rapid improvement in pruritus in atopic dermatitis patients treated with upadacitinib: A real-life experience. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 1497–1498. [Google Scholar] [CrossRef]
- Rerknimitr, P.; Puaratanaarunkon, T.; Wongtada, C.; Wittayabusarakam, N.; Krithin, S.; Paitoonpong, L.; Kumtornrut, C.; Kerr, S.J.; Asawanonda, P.; Jantarabenjakul, W.; et al. Cutaneous adverse reactions from 35,229 doses of Sinovac and AstraZeneca COVID-19 vaccination: A prospective cohort study in healthcare workers. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e158–e161. [Google Scholar] [CrossRef] [PubMed]
- Holmes, G.A.; Desai, M.; Limone, B.; Love, J.; Tawfik, M.; Wong, L.; Furukawa, B. A case series of cutaneous COVID-19 vaccine reactions at Loma Linda university de-partment of dermatology. JAAD Case Rep. 2021, 16, 53–57. [Google Scholar] [CrossRef]
- Leasure, A.C.; Cowper, S.E.; McNiff, J.; Cohen, J.M. Generalized eczematous reactions to the Pfizer-BioNTech COVID-19 vaccine. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e716–e717. [Google Scholar] [CrossRef] [PubMed]
- Bekkali, N.; Allard, T.; Lengellé, C.; Estève, E. Eczematiform eruption after Pfizer-BioNTech COVID-19 vaccine. Therapie 2021, 76, 364–365. (In French) [Google Scholar] [CrossRef]
- Larson, V.; Seidenberg, R.; Caplan, A.; Brinster, N.K.; Meehan, S.A.; Kim, R.H. Clinical and histopathological spectrum of delayed adverse cutaneous reactions following COVID-19 vaccination. J. Cutan. Pathol. 2022, 49, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Potestio, L.; Napolitano, M.; Bennardo, L.; Fabbrocini, G.; Patruno, C. Atopic dermatitis exacerbation after COVID-19 vaccination in Dupilumab-treated patients. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e409–e411. [Google Scholar] [CrossRef]
- Niebel, D.; Wenzel, J.; Wilsmann-Theis, D.; Ziob, J.; Wilhelmi, J.; Braegelmann, C. Single-Center Clinico-Pathological Case Study of 19 Patients with Cutaneous Adverse Reactions Following COVID-19 Vaccines. Dermatopathology 2021, 8, 463–476. [Google Scholar] [CrossRef] [PubMed]
- Gambichler, T.; Boms, S.; Susok, L.; Dickel, H.; Finis, C.; Abu Rached, N.; Barras, M.; Stücker, M.; Kasakovski, D. Cutaneous findings following COVID-19 vaccination: Review of world literature and own experience. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 172–180. [Google Scholar] [CrossRef]
- Picone, V.; Martora, F.; Fabbrocini, G.; Marano, L. “COVID arm”: Abnormal side effect after Moderna COVID-19 vaccine. Dermatol. Ther. 2022, 35, e15197. [Google Scholar] [CrossRef]
- Wei, N.; Fishman, M.; Wattenberg, D.; Gordon, M.; Lebwohl, M. “COVID arm”: A reaction to the Moderna vaccine. JAAD Case Rep. 2021, 10, 92–95. [Google Scholar] [CrossRef]
- Patruno, C.; Potestio, L.; Napolitano, M. Clinical phenotypes of adult atopic dermatitis and related therapies. Curr. Opin. Allergy Clin. Immunol. 2022, 22, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Ricardo, J.W.; Lipner, S.R. Considerations for safety in the use of systemic medications for psoriasis and atopic dermatitis during theCOVID-19 pandemic. Dermatol. Ther. 2020, 33, e13687. [Google Scholar] [CrossRef] [PubMed]
- Fan, R.; Cohen, J.M. Vaccination Recommendations for Psoriasis and Atopic Dermatitis Patients on Biologic Therapy: A Practical Guide. Yale J. Biol. Med. 2022, 95, 249–255. [Google Scholar] [PubMed]
- Patruno, C.; Potestio, L.; Scalvenzi, M.; Battista, T.; Raia, F.; Picone, V.; Fabbrocini, G.; Napolitano, M. Dupilumab for the treatment of adult atopic dermatitis in special populations. J. Dermatol. Treat. 2022, 33, 3028–3033. [Google Scholar] [CrossRef] [PubMed]
- Martora, F.; Martora, L.; Fabbrocini, G.; Marasca, C. A Case of Pemphigus Vulgaris and Hidradenitis Suppurativa: May Systemic Steroids Be Considered in the Standard Management of Hidradenitis Suppurativa? Ski. Appendage Disord. 2022, 8, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, A.; Martora, F.; Picone, V.; Marano, L.; Fabbrocini, G.; Marasca, C. Paradoxical Hidradenitis Suppurativa during Biologic Therapy, an Emerging Challenge: A Systematic Review. Biomedicines 2022, 10, 455. [Google Scholar] [CrossRef] [PubMed]
- Saunte, D.M.L.; Jemec, G.B.E. Hidradenitis Suppurativa: Advances in Diagnosis and Treatment. JAMA 2017, 318, 2019–2032. [Google Scholar] [CrossRef]
- Wortsman, X. Diagnosis and Treatment of Hidradenitis Suppurativa. JAMA 2018, 319, 1617–1618. [Google Scholar] [CrossRef]
- Alexander, H.; Patel, N.P. Response to Martora et al.’s “Hidradenitis suppurativa flares following COVID-19 vaccination: A case series”. JAAD Case Rep. 2022, 25, 13–14. [Google Scholar] [CrossRef]
- Martora, F.; Picone, V.; Fabbrocini, G.; Marasca, C. Hidradenitis suppurativa flares following COVID-19 vaccination: A case series. JAAD Case Rep. 2022, 23, 42–45. [Google Scholar] [CrossRef]
- Sahin, U.; Muik, A.; Derhovanessian, E.; Vogler, I.; Kranz, L.M.; Vormehr, M.; Baum, A.; Pascal, K.; Quandt, J.; Maurus, D.; et al. COVID-19 vaccine BNT162b1 elicits human antibody and TH1 T cell responses. Nature 2020, 586, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Martora, F.; Megna, M.; Battista, T.; Potestio, L.; Annunziata, M.C.; Marasca, C.; Villani, A.; Fabbrocini, G. Adalimumab, Ustekinumab, and Secukinumab in the Management of Hidradenitis Suppurativa: A Review of the Real-Life Experience. Clin. Cosmet. Investig. Dermatol. 2023, 16, 135–148. [Google Scholar] [CrossRef] [PubMed]
- Ring, H.C.; Maul, J.-T.; Yao, Y.; Wu, J.J.; Thyssen, J.P.; Thomsen, S.F.; Egeberg, A. Drug Survival of Biologics in Patients with Hidradenitis Suppurativa. JAMA Dermatol. 2022, 158, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Martora, F.; Marasca, C.; Battista, T.; Fabbrocini, G.; Ruggiero, A. Management of patients with hidradenitis suppurativa during COVID-19 vaccination: An experience from southern Italy. Comment on: ‘Evaluating the safety and efficacy of COVID-19 vaccination in patients with hidradenitis suppurativa’. Clin. Exp. Dermatol. 2022, 47, 2026–2028. [Google Scholar] [CrossRef]
- Montero-Vilchez, T.; Martinez-Lopez, A.; Salvador-Rodriguez, L.; Molina-Leyva, A.; Arias-Santiago, S. Management of patients with hidradenitis suppurativa during the COVID -19 pandemic. Dermatol. Ther. 2020, 33, e13875. [Google Scholar] [CrossRef]
- Molinelli, E.; Diotallevi, F.; Simonetti, O.; Brisigotti, V.; Sapigni, C.; Radi, G.; Campanati, A.; Offidani, A. Management of patients with hidradenitis suppurativa during the COVID-19 pandemic: Risk and benefit of immunomodulatory therapy. Dermatol. Ther. 2020, 33, e14256. [Google Scholar] [CrossRef]
- Martora, F.; Marasca, C.; Fabbrocini, G.; Ruggiero, A. Strategies adopted in a southern Italian referral centre to reduce adalimumab dis-continuation: Comment on ‘Can we increase the drug survival time of biologic therapies in hidradenitis suppurativa?’. Clin. Exp. Dermatol. 2022, 47, 1864–1865. [Google Scholar] [CrossRef]
- Martora, F.; Scalvenzi, M.; Ruggiero, A.; Potestio, L.; Battista, T.; Megna, M. Hidradenitis Suppurativa and JAK Inhibitors: A Review of the Published Literature. Medicina 2023, 59, 801. [Google Scholar] [CrossRef]
- Scollan, M.E.; Breneman, A.; Kinariwalla, N.; Soliman, Y.; Youssef, S.; Bordone, L.A.; Gallitano, S.M. Alopecia areata after SARS-CoV-2 vaccination. JAAD Case Rep. 2022, 20, 1–5. [Google Scholar] [CrossRef]
- Genco, L.; Cantelli, M.; Noto, M.; Battista, T.; Patrì, A.; Fabbrocini, G.; Vastarella, M. Alopecia Areata after COVID-19 Vaccines. Ski. Appendage Disord. 2023, 9, 141–143. [Google Scholar] [CrossRef]
- Babadjouni, A.; Phong, C.H.; Nguyen, C.; Mesinkovska, N.A. COVID-19 vaccination related exacerbations of hair loss in patients with moderate-to-severe alopecia areata on systemic therapy. JAAD Case Rep. 2022, 29, 181–185. [Google Scholar] [CrossRef]
- Rossi, A.; Magri, F.; Michelini, S.; Caro, G.; Di Fraia, M.; Fortuna, M.C.; Pellacani, G.; Carlesimo, M.; Rossi, A. Recurrence of alopecia areata after COVID-19 vaccination: A report of three cases in Italy. J. Cosmet. Dermatol. 2021, 20, 3753–3757. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Chen, Y.; Lan, C.E. Intractable alopecia areata following the second dose of COVID-19 vaccination: Report of two cases. Dermatol. Ther. 2022, 35, e15689. [Google Scholar] [CrossRef] [PubMed]
- Abdalla, H.; Ebrahim, E. Alopecia areata universalis precipitated by SARS-CoV-2 vaccine: A case report and narrative review. Cureus 2022, 14, e27953. [Google Scholar] [CrossRef]
- Gamonal, S.B.; Marques, N.C.; Pereira, H.M.; Gamonal, A.C. New-onset systemic lupus erythematosus after ChAdOX1 nCoV-19 and alopecia areata after BNT162b2 vaccination against SARS-CoV-2. Dermatol. Ther. 2022, 35, e15677. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.D.; McNish, A.; McDonald, L.; Burrell, C.; Smith-Matthews, S. Alopecia universalis with unusual histopathologic features after vaccination with ChAdOx1 nCoV-19 (AZD1222). JAAD Case Rep. 2022, 25, 4–8. [Google Scholar] [CrossRef]
- Su, H.-A.; Juan, C.-K.; Chen, Y.-C. Alopecia areata following ChAdOx1 nCoV-19 vaccination (Oxford/AstraZeneca). J. Formos. Med. Assoc. 2022, 121, 2138–2140. [Google Scholar] [CrossRef]
- Gallo, G.; Mastorino, L.; Tonella, L.; Ribero, S.; Quaglino, P. Alopecia areata after COVID-19 vaccination. Clin. Exp. Vaccine Res. 2022, 11, 129–132. [Google Scholar] [CrossRef]
- May Lee, M.; Bertolani, M.; Pierobon, E.; Lotti, T.; Feliciani, C.; Satolli, F. Alopecia areata following COVID-19 vaccination: Vaccine-induced autoimmunity? Int. J. Dermatol. 2022, 61, 634–635. [Google Scholar] [CrossRef]
- Essam, R.; Ehab, R.; Al-Razzaz, R.; Khater, M.W.; Moustafa, E.A. Alopecia areata after ChAdOx1 nCoV-19 vaccine (Oxford/AstraZeneca): A potential triggering factor? J. Cosmet. Dermatol. 2021, 20, 3727–3729. [Google Scholar] [CrossRef]
- Nguyen, B.; Tosti, A. Alopecia areata after COVID-19 infection and vaccination: A cross-sectional analysis. J. Eur. Acad. Dermatol. Venereol. 2022, 37, e7–e8. [Google Scholar] [CrossRef] [PubMed]
- Martora, F.; Fabbrocini, G.; Nappa, P.; Megna, M. Impact of the COVID-19 pandemic on hospital admissions of patients with rare dis-eases: An experience of a Southern Italy referral center. Int. J. Dermatol. 2022, 61, e237–e238. [Google Scholar] [CrossRef] [PubMed]
- Martora, F.; Fabbrocini, G.; Nappa, P.; Megna, M. Reply to ‘Development of severe pemphigus vulgaris following SARS-CoV-2 vac-cination with BNT162b2′ by Solimani et al. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e750–e751. [Google Scholar] [CrossRef]
- Zou, H.; Daveluy, S. Pemphigus vulgaris after COVID-19 infection and vaccination. J. Am. Acad. Dermatol. 2022, 87, 709–710. [Google Scholar] [CrossRef]
- Gui, H.; Young, P.A.; So, J.Y.; Pol-Rodriguez, M.; Rieger, K.E.; Lewis, M.A.; Winge, M.C.; Bae, G.H. New-onset pemphigus vegetans and pemphigus foliaceus after SARS-CoV-2 vaccination: A report of 2 cases. JAAD Case Rep. 2022, 27, 94–98. [Google Scholar] [CrossRef]
- Rouatbi, J.; Aounallah, A.; Lahouel, M.; Sriha, B.; Belajouza, C.; Denguezli, M. Two cases with new onset of Pemphigus Foliaceus after SARS-CoV-2 vaccination. Dermatol. Ther. 2022, 35, e15827. [Google Scholar] [CrossRef] [PubMed]
- Aryanian, Z.; Balighi, K.; Azizpour, A.; Kamyab Hesari, K.; Hatami, P. Coexistence of pemphigus vulgaris and lichen planus following COVID-19 vac-cination. Case Rep. Dermatol. Med. 2022, 2022, 2324212. [Google Scholar]
- Koutlas, I.G.; Camara, R.; Argyris, P.P.; Davis, M.D.; Miller, D.D. Development of pemphigus vulgaris after the second dose of the mRNA-1273 SARS-CoV-2 vaccine. Oral Dis. 2021, 28, 2612–2613. [Google Scholar] [CrossRef]
- Knechtl, G.V.; Seyed Jafari, S.M.; Berger, T.; Rammlmair, A.; Feldmeyer, L.; Borradori, L. Development of pemphigus vulgaris following mRNA SARS-CoV-19 BNT162b2 vaccination in an 89-year-old patient. J. Eur. Acad. Dermato.l Venereol. 2022, 36, e251–e253. [Google Scholar] [CrossRef]
- Ong, S.K.; Darji, K.; Chaudhry, S.B. Severe flare of pemphigus vulgaris after first dose of COVID-19 vaccine. JAAD Case Rep. 2022, 22, 50–52. [Google Scholar] [CrossRef]
- Yıldırıcı, Ş.; Yaylı, S.; Demirkesen, C.; Vural, S. New onset of pemphigus foliaceus following BNT162b2 vaccine. Dermatol. Ther. 2022, 35, e15381. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Bharadwaj, S.J.; Chirayath, A.G.; Ganguly, S. Development of severe pemphigus vulgaris following ChAdOx1 nCoV-19 vac-cination and review of literature. J. Cosmet. Dermatol. 2022, 21, 2311–2314. [Google Scholar] [CrossRef] [PubMed]
- Norimatsu, Y.; Yoshizaki, A.; Yamada, T.; Akiyama, Y.; Toyama, S.; Sato, S. Pemphigus vulgaris with advanced hypopharyngeal and gastric cancer following SARS-CoV-2 vaccination. J. Dermatol. 2022, 50, e74–e75. [Google Scholar] [CrossRef] [PubMed]
- Agharbi, F.-Z.; Basri, G.; Chiheb, S. Pemphigus vulgaris following second dose of mRNA-(Pfizer-BioNTech) COVID-19 vaccine. Dermatol. Ther. 2022, 35, e15769. [Google Scholar] [CrossRef]
- Almasi-Nasrabadi, M.; Ayyalaraju, R.S.; Sharma, A.; Elsheikh, S.; Ayob, S. New onset pemphigus foliaceus following AstraZeneca COVID-19 vaccination. J. Eur. Acad. Dermatol. Venereol. 2022, 37, e1–e3. [Google Scholar] [CrossRef]
- Corrá, A.; Barei, F.; Genovese, G.; Zussino, M.; Spigariolo, C.B.; Mariotti, E.B.; Quintarelli, L.; Verdelli, A.; Caproni, M.; Marzano, A.V. Five cases of new-onset pemphigus following vaccinations against coronavirus disease 2019. J. Dermatol. 2022, 50, 229–233. [Google Scholar] [CrossRef]
- Solimani, F.; Mansour, Y.; Didona, D.; Dilling, A.; Ghoreschi, K.; Meier, K. Development of severe pemphigus vulgaris following SARS-CoV-2 vaccination with BNT162b2. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e649–e651. [Google Scholar] [CrossRef]
- Martora, F.; Battista, T.; Nappa, P.; Fabbrocini, G.; Megna, M. Pemphigus vulgaris and COVID-19 vaccination: Management and treatment. J. Cosmet. Dermatol. 2022, 22, 30–31. [Google Scholar] [CrossRef]
- Maronese, C.A.; Caproni, M.; Moltrasio, C.; Genovese, G.; Vezzoli, P.; Sena, P.; Previtali, G.; Cozzani, E.; Gasparini, G.; Parodi, A.; et al. Bullous Pemphigoid Associated With COVID-19 Vaccines: An Italian Multicentre Study. Front. Med. 2022, 9, 841506. [Google Scholar] [CrossRef]
- Bostan, E.; Yel, B.; Akdogan, N.; Gokoz, O. Reply to “New-onset bullous pemphigoid after inactivated COVID-19 vaccine: Synergistic effect of the COVID-19 vaccine and vildagliptin”. Dermatol. Ther. 2022, 35, e15496. [Google Scholar] [CrossRef]
- Hali, F.; Araqi, L.; Marnissi, F.; Meftah, A.; Chiheb, S. Autoimmune Bullous Dermatosis Following COVID-19 Vaccination: A Series of Five Cases. Cureus 2022, 14, e23127. [Google Scholar] [CrossRef]
- Gambichler, T.; Hamdani, N.; Budde, H.; Sieme, M.; Skrygan, M.; Scholl, L.; Dickel, H.; Behle, B.; Ganjuur, N.; Scheel, C.; et al. Bullous pemphigoid after SARS-CoV-2 vaccination: Spike-protein-directed im-munofluorescence confocal microscopy and T-cell-receptor studies. Br. J. Dermatol. 2022, 186, 728–731. [Google Scholar] [CrossRef]
- Shanshal, M. Dyshidrosiform Bullous Pemphigoid Triggered by COVID-19 Vaccination. Cureus 2022, 14, e26383. [Google Scholar] [CrossRef]
- Desai, A.D.; Shah, R.; Haroon, A.; Wassef, C. Bullous Pemphigoid Following the Moderna mRNA-1273 Vaccine. Cureus 2022, 14, e24126. [Google Scholar] [CrossRef]
- Fu, P.A.; Chen, C.W.; Hsu, Y.T.; Wei, K.C.; Lin, P.C.; Chen, T.Y. A case of acquired hemophilia A and bullous pemphigoid following SARS-CoV-2 mRNA vaccination. J. Formosan. Med. Assoc. 2022, 121, 1872–1876. [Google Scholar] [CrossRef]
- Alshammari, F.; Abuzied, Y.; Korairi, A.; Alajlan, M.; Alzomia, M.; AlSheef, M. Bullous pemphigoid after second dose of mRNA- (Pfizer-BioNTech) COVID-19 vaccine: A case report. Ann. Med. Surg. 2022, 75, 103420. [Google Scholar] [CrossRef] [PubMed]
- Hung, W.-K.; Chi, C.-C. Incident bullous pemphigoid in a psoriatic patient following mRNA-1273 SARS-CoV-2 vaccination. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e407–e409. [Google Scholar] [CrossRef] [PubMed]
- Pauluzzi, M.; Stinco, G.; Errichetti, E. Bullous pemphigoid in a young male after COVID-19 mRNA vaccine: A report and brief literature review. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e257–e259. [Google Scholar] [CrossRef]
- Dell’Antonia, M.; Anedda, S.; Usai, F.; Atzori, L.; Ferreli, C. Bullous pemphigoid triggered by COVID-19 vaccine: Rapid resolution with cortico-steroid therapy. Dermatol. Ther. 2022, 35, e15208. [Google Scholar]
- Pérez-López, I.; Moyano-Bueno, D.; Ruiz-Villaverde, R. Bullous pemphigoid and COVID-19 vaccine. Med. Clin. 2021, 157, e333–e334. [Google Scholar] [CrossRef] [PubMed]
- Agharbi, F.-Z.; Eljazouly, M.; Basri, G.; Faik, M.; Benkirane, A.; Albouzidi, A.; Chiheb, S. Bullous pemphigoid induced by the AstraZeneca COVID-19 vaccine. Ann. Dermatol. Venereol. 2022, 149, 56–57. [Google Scholar] [CrossRef] [PubMed]
- Young, J.; Mercieca, L.; Ceci, M.; Pisani, D.; Betts, A.; Boffa, M.J. A case of bullous pemphigoid after the SARS-CoV-2 mRNA vaccine. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e13–e16. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Kosano, M.; Sakai, Y.; Saito, N.; Takazawa, Y.; Omodaka, T.; Kiniwa, Y.; Okuyama, R. Case of bullous pemphigoid following coronavirus disease 2019 vaccination. J. Dermatol. 2021, 48, e606–e607. [Google Scholar] [CrossRef] [PubMed]
- Martora, F.; Ruggiero, A.; Battista, T.; Fabbrocini, G.; Megna, M. Bullous pemphigoid and COVID-19 vaccination: Management and treatment reply to ‘Bullous pemphigoid in a young male after COVID-19 mRNA vaccine: A report and brief literature review’ by Pauluzzi et al. J. Eur. Acad. Dermatol. Venereol. 2023, 37, e35–e36. [Google Scholar] [CrossRef]
- Martora, F.; Picone, V.; Fornaro, L.; Fabbrocini, G.; Marasca, C. Can COVID-19 cause atypical forms of pityriasis rosea refractory to conventional therapies? J. Med. Virol. 2022, 94, 1292–1293. [Google Scholar] [CrossRef]
- Drago, F.; Ciccarese, G.; Javor, S.; Parodi, A. Vaccine-induced pityriasis rosea and pityriasis rosea-like eruptions: A review of the liter-ature. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 544–545. [Google Scholar] [CrossRef]
- Drago, F.; Ciccarese, G.; Parodi, A. Pityriasis rosea and pityriasis rosea-like eruptions after COVID-19 vaccines. JAAD Int. 2022, 9, 127. [Google Scholar] [CrossRef]
- Drago, F.; Broccolo, F.; Ciccarese, G. Pityriasis rosea, pityriasis rosea–like eruptions, and herpes zoster in the setting of COVID-19 and COVID-19 vaccination. Clin. Dermatol. 2022, 40, 586–590. [Google Scholar] [CrossRef]
- Temiz, S.A.; Abdelmaksoud, A.; Dursun, R.; Durmaz, K.; Sadoughifar, R.; Hasan, A. Pityriasis rosea following SARS-CoV-2 vaccination: A case series. J. Cosmet. Dermatol. 2021, 20, 3080–3084. [Google Scholar] [CrossRef]
- Ramot, Y.; Nanova, K.; Faitatziadou, S.M.; Assab, D.A.; Berkun, Y.; Zlotogorski, A. Six cases of pityriasis rosea following SARS-CoV-2 vaccination with BNT162b2. J. Der Dtsch. Dermatol. Ges. 2022, 20, 1123–1124. [Google Scholar] [CrossRef]
- Martora, F.; Fabbrocini, G.; Marasca, C. Pityriasis rosea after Moderna mRNA-1273 vaccine: A case series. Dermatol. Ther. 2022, 35, e15225. [Google Scholar] [CrossRef] [PubMed]
- Khattab, E.; Christaki, E.; Pitsios, C. Pityriasis Rosea Induced by COVID-19 Vaccination. Eur. J. Case Rep. Intern. Med. 2022, 9, 003164. [Google Scholar] [CrossRef]
- Cyrenne, B.; Al-Mohammedi, F.; DeKoven, J.; Alhusayen, R. Pityriasis rosea-like eruptions following vaccination with BNT162b2 mRNA COVID-19 Vaccine. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e546–e548. [Google Scholar] [CrossRef] [PubMed]
- Valk, B.; Bender, B. Pityriasis rosea associated with COVID-19 vaccination: A common rash following administration of a novel vaccine. Cutis. 2021, 108, 317–318. [Google Scholar] [CrossRef] [PubMed]
- Buckley, J.E.; Landis, L.N.; Rapini, R.P. Pityriasis rosea–like rash after messenger RNA COVID-19 vaccination: A case report and review of the literature. JAAD Int. 2022, 7, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-S.; Chen, H.-H.; Liu, S.-H. Pityriasis Rosea-like eruptions following COVID-19 mRNA-1273 vaccination: A case report and literature review. J. Formosan. Med. Assoc. 2022, 121, 1003–1007. [Google Scholar] [CrossRef]
- Shin, S.H.; Hong, J.K.; Hong, S.A.; Li, K.; Yoo, K.H. Pityriasis Rosea Shortly After mRNA-1273 COVID-19 Vaccination. Int. J. Infect. Dis. 2022, 114, 88–89. [Google Scholar] [CrossRef]
- Bostan, E.; Jarbou, A. Atypical pityriasis rosea associated with mRNA COVID-19 vaccine. J. Med. Virol. 2022, 94, 814–816. [Google Scholar] [CrossRef]
- Leerunyakul, K.; Pakornphadungsit, K.; Suchonwanit, P. Case report: Pityriasis rosea-like Eruption following COVID-19 vac-cination. Front. Med. 2021, 8, 752443. [Google Scholar] [CrossRef]
- Cohen, O.G.; Clark, A.K.; Milbar, H.; Tarlow, M. Pityriasis rosea after administration of Pfizer-BioNTech COVID-19 vaccine. Hum. Vaccin. Immunother. 2021, 17, 4097–4098. [Google Scholar] [CrossRef]
- Dormann, H.; Grummt, S.; Karg, M. Pityriasis Rosea as a Possible Complication of Vaccination Against COVID-19. Dtsch. Arztebl. Int. 2021, 118, 431. [Google Scholar] [CrossRef] [PubMed]
- Rubaian, N.F.; Almuhaidib, S.R.; Aljarri, S.A.; Alamri, A.S.; AlMuhaidib, S.; Aljarri, S.; Alamri, A. Pityriasis rosea following pfizer-BioNTech vaccination in an adolescent girl. Cureus 2022, 14, e27108. [Google Scholar] [CrossRef]
- Fenner, B.; Marquez, J.L.; Pham, M.; Tarbox, M. Inverse pityriasis rosea secondary to COVID-19 vaccination. Bayl. Univ. Med Cent. Proc. 2022, 35, 342–343. [Google Scholar] [CrossRef]
- Cruz, O.M.; Vidal-Navarro, A.; Pesqué, D.; Giménez-Arnau, A.; Pujol, R.; Martin-Ezquerra, G. Pityriasis rosea developing after COVID-19 vaccination. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e721–e722. [Google Scholar] [CrossRef]
- Abdullah, L.; Hasbani, D.; Kurban, M.; Abbas, O. Pityriasis rosea after mRNA COVID-19 vaccination. Int. J. Dermatol. 2021, 60, 1150–1151. [Google Scholar] [CrossRef] [PubMed]
- Carballido Vázquez, A.M.; Morgado, B. Pityriasis rosea-like eruption after Pfizer-BioNTech COVID-19 vaccination. Br. J. Dermatol. 2021, 185, e34. [Google Scholar] [CrossRef] [PubMed]
- Paolino, G.; Di Nicola, M.R.; Cantisani, C.; Mercuri, S.R. Pityriasis rosea infection in a COVID-19 patient successfully treated with systemic steroid and antihistamine via telemedicine: Literature update of a possible prodromal symptom of an underlying SARS-CoV-2 infection. Dermatol. Ther. 2021, 34, e14972. [Google Scholar] [CrossRef] [PubMed]
- Khan, I.; Elsanousi, A.A.; Shareef, A.M.; Tebha, S.S.; Arif, A.; Gul, S. Manifestation of pityriasis rosea and pityriasis rosea-like eruptions after COVID-19 vaccine: A systematic review. Immun. Inflamm. Dis. 2023, 11, e804. [Google Scholar] [CrossRef]
- Magen, E.; Yakov, A.; Green, I.; Israel, A.; Vinker, S.; Merzon, E. Chronic spontaneous urticaria after BNT162b2 mRNA (Pfizer-BioNTech) vaccination against SARS-CoV-2. Allergy Asthma Proc. 2022, 43, 30–36. [Google Scholar] [CrossRef]
- Potestio, L.; Genco, L.; Villani, A.; Marasca, C.; Fabbrocini, G.; Fornaro, L.; Ruggiero, A.; Martora, F. Reply to ‘Cutaneous adverse effects of the available COVID-19 vaccines in India: A questionnaire-based study’ by Bawane J et al. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e863–e864. [Google Scholar] [CrossRef]
- Riad, A.; Pokorná, A.; Attia, S.; Klugarová, J.; Koščík, M.; Klugar, M. Prevalence of COVID-19 vaccine side effects among healthcare workers in the Czech Re-public. J. Clin. Med. 2021, 10, 1428. [Google Scholar] [CrossRef] [PubMed]
- Sidlow, J.S.; Reichel, M.; Lowenstein, E.J. Localized and generalized urticarial allergic dermatitis secondary to SARS-CoV-2 vac-cination in a series of 6 patients. JAAD Case Rep. 2021, 14, 13–16. [Google Scholar] [CrossRef] [PubMed]
- Peigottu, M.F.; Ferreli, C.; Atzori, M.G.; Atzori, L. Skin Adverse Reactions to Novel Messenger RNA Coronavirus Vaccination: A Case Series. Diseases 2021, 9, 58. [Google Scholar] [CrossRef] [PubMed]
- McMahon, D.E.; Kovarik, C.L.; Damsky, W.; Rosenbach, M.; Lipoff, J.B.; Tyagi, A.; Chamberlin, G.; Fathy, R.; Nazarian, R.M.; Desai, S.R.; et al. Clinical and pathologic correlation of cutaneous COVID-19 vaccine reactions including V-REPP: A registry-based study. J. Am. Acad. Dermatol. 2022, 86, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Nieto, D.; Hammerle, J.; Fernandez-Escribano, M.; Moreno-del Real, C.M.; Garcia-Abellas, P.; Carretero-Barrio, I.; Solano-Solares, E.; de-la-Hoz-Caballer, B.; Jimenez-Cauhe, J.; Ortega-Quijano, D.; et al. Skin manifestations of the BNT162b2 mRNA COVID-19 vaccine in healthcare workers. “COVID-arm”: A clinical and histological characterization. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e425–e427. [Google Scholar] [CrossRef]
- Bianchi, L.; Biondi, F.; Hansel, K.; Murgia, N.; Tramontana, M.; Stingeni, L. Skin tests in urticaria/angioedema and flushing to Pfizer-BioNTech SARS-CoV-2 vaccine: Limits of intradermal testing. Allergy 2021, 76, 2605–2607. [Google Scholar] [CrossRef]
- Corbeddu, M.; Diociaiuti, A.; Vinci, M.R.; Santoro, A.; Camisa, V.; Zaffina, S.; El Hachem, M. Transient cutaneous manifestations after administration of Pfizer-BioNTech COVID-19 Vaccine: An Italian single-centre case series. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e483–e485. [Google Scholar] [CrossRef]
- Baraldi, C.; Boling, L.B.; Patrizi, A.; Prodi, C.; Deleonardi, G.; Gaspari, V.; Misciali, C. Unique Case of Urticarial Skin Eruptions After COVID-19 Vaccination. Am. J. Dermatopathol. 2022, 44, 198–200. [Google Scholar] [CrossRef]
- Choi, E.; Liew, C.F.; Oon, H.H. Cutaneous adverse effects and contraindications to COVID -19 vaccination; four cases and an illustrative review from an Asian country. Dermatol. Ther. 2021, 34, e15123. [Google Scholar] [CrossRef]
- Patruno, C.; Napolitano, M.; Stingeni, L.; Fabbrocini, G. Skin rashes after SARS-CoV-2 vaccine: Which relationship if any? Immun. Inflamm. Dis. 2021, 9, 622–623. [Google Scholar] [CrossRef]
- Burlando, M.; Herzum, A.; Cozzani, E.; Parodi, A. Acute urticarial rash after COVID-19 vaccination containing Polysorbate 80. Clin. Exp. Vaccine Res. 2021, 10, 298–300. [Google Scholar] [CrossRef]
- Thomas, J.; Thomas, G.; Chatim, A.; Shukla, P.; Mardiney, M. Chronic Spontaneous Urticaria After COVID-19 Vaccine. Cureus 2021, 13, e18102. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Mathes, S.; Claussen, C.; Biedermann, T.; Brockow, K. Cutaneous reactions following COVID-19 vaccination assessed by dermatologists: A single-institutional study in Germany. J. Dtsch. Dermatol. Ges. 2023, 21, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, S.; Verma, K.; Verma, I.; Gandhi, J. Reactivation of Herpes Zoster Virus After COVID-19 Vaccination: Is There Any Association? Cureus 2022, 14, e25195. [Google Scholar] [CrossRef] [PubMed]
- Naoum, C.; Hartmann, M. Herpes zoster reactivation after COVID-19 vaccination—A retrospective case series of 22 patients. Int. J. Dermatol. 2022, 61, 628–629. [Google Scholar] [CrossRef] [PubMed]
- Monastirli, A.; Pasmatzi, E.; Badavanis, G.; Panagiotopoulou, G.; Apostolidou, A.; Tsambaos, D. Herpes Zoster after mRNA COVID-19 vaccination: A case series. Skinmed 2022, 20, 284–288. [Google Scholar]
- Furer, V.; Zisman, D.; Kibari, A.; Rimar, D.; Paran, Y.; Elkayam, O. Herpes zoster following BNT162b2 mRNA COVID-19 vaccination in patients with auto-immune inflammatory rheumatic diseases: A case series. Rheumatology 2021, 60, SI90–SI95. [Google Scholar] [CrossRef] [PubMed]
- Vastarella, M.; Picone, V.; Martora, F.; Fabbrocini, G. Herpes zoster after ChAdOx1 nCoV-19 vaccine: A case series. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e845–e846. [Google Scholar] [CrossRef]
- Palanivel, J.A. Herpes zoster after COVID-19 vaccination-Can the vaccine reactivate latent zoster virus? J. Cosmet. Dermatol. 2021, 20, 3376–3377. [Google Scholar] [CrossRef]
- Vallianou, N.G.; Tsilingiris, D.; Karampela, I.; Liu, J.; Dalamaga, M. Herpes zoster following COVID-19 vaccination in an immunocompetent and vaccinated for herpes zoster adult: A two-vaccine related event? Metab. Open 2022, 13, 100171. [Google Scholar] [CrossRef]
- Jiang, Z.H.; Wong, L.S.; Lee, C.H.; Hsu, T.J.; Yu, Y.H. Disseminated and localised herpes zoster following Oxford-AstraZeneca COVID-19 vaccination. Indian J. Dermatol. Venereol. Leprol. 2022, 88, 445. [Google Scholar] [CrossRef] [PubMed]
- Martora, F.; Fabbrocini, G.; Picone, V. A case of herpes zoster ophthalmicus after third dose of Comirnaty (BNT162b2 mRNA) vaccine. Dermatol. Ther. 2022, 35, e15411. [Google Scholar] [CrossRef]
- Tanizaki, R.; Miyamatsu, Y. Zoster sine herpete following BNT162b2 mRNA COVID-19 vaccination in an immunocompetent patient. IDCases 2022, 29, e01563. [Google Scholar] [CrossRef] [PubMed]
- Paolino, G.; Campochiaro, C.; Di Nicola, M.; Mercuri, S.; Rizzo, N.; Dagna, L.; Rongioletti, F.; De Luca, G. Generalized morphea after COVID-19 vaccines: A case series. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e680–e682. [Google Scholar] [CrossRef] [PubMed]
- Antoñanzas, J.; Rodríguez-Garijo, N.; Estenaga, Á.; Morelló-Vicente, A.; España, A.; Aguado, L. Generalized morphea following the COVID vaccine: A series of two patients and a bibliographic review. Dermatol. Ther. 2022, 35, e15709. [Google Scholar] [CrossRef] [PubMed]
- Oh, D.A.Q.; Tee, S.-I.; Heng, Y.K. Morphoea following COVID-19 vaccination. Clin. Exp. Dermatol. 2022, 47, 2293–2295. [Google Scholar] [CrossRef]
- Metin, Z.; Celepli, P. A case of morphea following the COVID-19 mRNA vaccine: On the basis of viral spike proteins. Int. J. Dermatol. 2022, 61, 639–641. [Google Scholar] [CrossRef]
- Aryanian, Z.; Balighi, K.; Hatami, P.; Tootoonchi, N.M.; Goodarzi, A.; Mohseni Afshar, Z. Morphea in two patients after being infected to and being vaccinated against SARS-CoV-2 infection. Clin. Case Rep. 2022, 10, e05667. [Google Scholar] [CrossRef]
- Martora, F.; Battista, T.; Ruggiero, A.; Fabbrocini, G.; Potestio, L. Comment on ‘Morphoea following COVID-19 vaccination’. Clin. Exp. Dermatol. 2022, 47, 2312–2313. [Google Scholar] [CrossRef]
- Kaminetsky, J.; Rudikoff, D. New-onset vitiligo following mRNA-1273 (Moderna) COVID-19 vaccination. Clin. Case Rep. 2021, 9, e04865. [Google Scholar] [CrossRef]
- Militello, M.; Ambur, A.B.; Steffes, W. Vitiligo Possibly Triggered by COVID-19 Vaccination. Cureus 2022, 14, e20902. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Cohen, J.L.; Astudillo, M.; Harris, J.E.; Freeman, E.E. Vitiligo of the arm after COVID-19 vaccination. JAAD Case Rep. 2022, 28, 142–144. [Google Scholar] [CrossRef] [PubMed]
- Nicolaidou, E.; Vavouli, C.; Koumprentziotis, I.A.; Gerochristou, M.; Stratigos, A. New-onset vitiligo after COVID-19 mRNA vaccination: A causal asso-ciation? J. Eur. Acad. Dermatol. Venereol. 2023, 37, e11–e12. [Google Scholar] [CrossRef]
- Flores-Terry, M.Á.; García-Arpa, M.; Mateo, J.S.; Aguilera, G.R. Facial vitiligo after SARS-CoV-2 vaccination. Actas Dermosifiliogr. 2022, 113, 721. (In Spanish) [Google Scholar] [CrossRef]
- Bukhari, A.E. New-onset of vitiligo in a child following COVID-19 vaccination. JAAD Case Rep. 2022, 22, 68–69. [Google Scholar] [CrossRef]
- Uğurer, E.; Sivaz, O.; Altunay, İ.K. Newly-developed vitiligo following COVID-19 mRNA vaccine. J. Cosmet. Dermatol. 2022, 21, 1350–1351. [Google Scholar] [CrossRef] [PubMed]
- Ciccarese, G.; Drago, F.; Boldrin, S.; Pattaro, M.; Parodi, A. Sudden onset of vitiligo after COVID-19 vaccine. Dermatol. Ther. 2022, 35, e15196. [Google Scholar] [CrossRef]
- López Riquelme, I.; Fernández Ballesteros, M.D.; Serrano Ordoñez, A.; Godoy Díaz, D.J. COVID-19 and autoimmune phenomena: Vitiligo after AstraZeneca vaccine. Dermatol. Ther. 2022, 35, e15502. [Google Scholar]
- Okan, G.; Vural, P. Worsening of the vitiligo following the second dose of the BNT162B2 mRNA COVID-19 vaccine. Dermatol. Ther. 2022, 35, e15280. [Google Scholar] [CrossRef]
- Caroppo, F.; Deotto, M.L.; Tartaglia, J.; Fortina, A.B. Vitiligo worsened following the second dose of mRNA SARS-CoV-2 vaccine. Dermatol. Ther. 2022, 35, e15434. [Google Scholar] [CrossRef]
- Majid, I.; Mearaj, S. Sweet syndrome after Oxford-AstraZeneca COVID-19 vaccine (AZD1222) in an elderly female. Dermatol. Ther. 2021, 34, e15146. [Google Scholar] [CrossRef] [PubMed]
- Agaronov, A.; Makdesi, C.; Hall, C.S. Acute generalized exanthematous pustulosis induced by Moderna COVID-19 messenger RNA vaccine. JAAD Case Rep. 2021, 16, 96–97. [Google Scholar] [CrossRef] [PubMed]
- Cantisani, C.; Chello, C.; Grieco, T.; Ambrosio, L.; Kiss, N.; Tammaro, A.; Tosti, G.; Paolino, G.; Pellacani, G. Cutaneous Reactions to COVID-19 Vaccines in a Monocentric Study: A Case Series. J. Clin. Med. 2022, 11, 3811. [Google Scholar] [CrossRef] [PubMed]
- Camargo Coronel, A.; Jiménez Balderas, F.J.; Quiñones Moya, H.; Hernández Zavala, M.R.; Mandinabeitia Rodríguez, P.; Hernández Vázquez, J.R.; Zamora Zarco, S.; Aguilar Castillo, S.D. Dermatomyositis post vaccine against SARS-CoV-2. BMC Rheumatol. 2022, 6, 20. [Google Scholar] [CrossRef] [PubMed]
- Martora, F.; Villani, A.; Fabbrocini, G.; Battista, T. COVID-19 and cutaneous manifestations: A review of the published literature. J. Cosmet. Dermatol. 2023, 22, 4–10. [Google Scholar] [CrossRef]
- Hlaca, N.; Zagar, T.; Kastelan, M.; Peternel, S.; Brajac, I.; Dujmovic-Hasanbegovic, K.; Prpic-Massari, L. Pityriasis rubra pilaris following booster dose of mRNA (Pfizer-BioNTech) COVID-19 vaccine. Dermatol Ther. 2022, 35, e15791. [Google Scholar] [CrossRef]
- Martora, F.; Fabbrocini, G.; Guerrasio, G.; Potestio, L. Reply to ‘A case of pityriasis lichenoides et varioliformis acuta developed after first dose of Oxford-AstraZeneca COVID-19 vaccine’. J. Eur. Acad. Dermatol. Venereol. 2022, 37, e141. [Google Scholar] [CrossRef]
- Ruggiero, A.; Megna, M.; Fabbrocini, G.; Martora, F. Video and telephone teledermatology consultations during COVID-19 in compar-ison: Patient satisfaction, doubts and concerns. Clin. Exp. Dermatol. 2022, 47, 1863–1864. [Google Scholar] [CrossRef]
- Liu, Q.; Qin, C.; Liu, M.; Liu, J. Effectiveness and safety of SARS-CoV-2 vaccine in real-world studies: A systematic review and meta-analysis. Infect. Dis. Poverty 2021, 10, 132. [Google Scholar] [CrossRef]
- Gambichler, T.; Scheel, C.H.; Arafat, Y.; Kautz, O.; Boms, S. Erythrodermic pityriasis rubra pilaris after SARS-CoV-2 vaccination with concom-itant COVID-19 infection. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e675–e676. [Google Scholar] [CrossRef]
- Fernandes, Q.; Inchakalody, V.P.; Merhi, M.; Mestiri, S.; Taib, N.; Moustafa Abo El-Ella, D.; Bedhiafi, T.; Raza, A.; Al-Zaidan, L.; Mohsen, M.O.; et al. Emerging COVID-19 variants and their impact on SARS-CoV-2 diagnosis, therapeutics and vaccines. Ann. Med. 2022, 54, 524–540. [Google Scholar] [CrossRef]
- Villani, A.; Potestio, L.; Fabbrocini, G.; Troncone, G.; Malapelle, U.; Scalvenzi, M. The Treatment of Advanced Melanoma: Therapeutic Update. Int. J. Mol. Sci. 2022, 23, 6388. [Google Scholar] [CrossRef]
- Villani, A.; Potestio, L.; Fabbrocini, G.; Scalvenzi, M. New Emerging Treatment Options for Advanced Basal Cell Carcinoma and Squamous Cell Carcinoma. Adv. Ther. 2022, 39, 1164–1178. [Google Scholar] [CrossRef]
- Villani, A.; Ocampo-Garza, S.S.; Potestio, L.; Fabbrocini, G.; Ocampo-Candiani, J.; Ocampo-Garza, J.; Scalvenzi, M. Cemiplimab for the treatment of advanced cutaneous squamous cell carcinoma. Expert Opin. Drug Saf. 2022, 21, 21–29. [Google Scholar] [CrossRef]
- Villani, A.; Scalvenzi, M.; Micali, G.; Lacarrubba, F.; Fornaro, L.; Martora, F.; Potestio, L. Management of Advanced Invasive Melanoma: New Strategies. Adv. Ther. 2023. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, A.; Potestio, L.; Martora, F.; Villani, A.; Comune, R.; Megna, M. Bimekizumab treatment in patients with moderate to severe plaque psoriasis: A drug safety evaluation. Expert Opin. Drug Saf. 2023. [Google Scholar] [CrossRef] [PubMed]
- Camela, E.; Potestio, L.; Fabbrocini, G.; Pallotta, S.; Megna, M. The holistic approach to psoriasis patients with comorbidities: The role of investigational drugs. Expert Opin. Investig. Drugs 2023. [Google Scholar] [CrossRef] [PubMed]
- Elmas, Ö.F.; Demirbaş, A.; Düzayak, S.; Atasoy, M.; Türsen, Ü.; Lotti, T. Melanoma and COVID-19: A narrative review focused on treatment. Dermatol. Ther. 2020, 33, e14101. [Google Scholar] [CrossRef] [PubMed]
- Villani, A.; Scalvenzi, M.; Fabbrocini, G.; Fornaro, L.; Guerrasio, G.; Potestio, L. Effects of COVID-19 pandemic on malignant melanoma diagnosis. J. Eur. Acad. Dermatol. Venereol. 2023, 37, e22–e23. [Google Scholar] [CrossRef]
- Wollina, U. Challenges of COVID-19 pandemic for dermatology. Dermatol. Ther. 2020, 33, e13430. [Google Scholar] [CrossRef]
- Martora, F.; Fabbrocini, G.; Megna, M.; Scalvenzi, M.; Battista, T.; Villani, A.; Potestio, L. Teledermatology for Common Inflammatory Skin Conditions: The Medicine of the Future? Life 2023, 13, 1037. [Google Scholar] [CrossRef] [PubMed]
- Camela, E.; Potestio, L.; Fabbrocini, G.; Ruggiero, A.; Megna, M. New frontiers in personalized medicine in psoriasis. Expert Opin. Biol. Ther. 2022, 22, 1431–1433. [Google Scholar] [CrossRef] [PubMed]
- Potestio, L.; Villani, A.; Fabbrocini, G.; Martora, F. Cutaneous reactions following booster dose of COVID-19 mRNA vaccination: What we should know? J. Cosmet. Dermatol. 2022, 21, 5339–5340. [Google Scholar] [CrossRef] [PubMed]
- Picone, V.; Napolitano, M.; Martora, F.; Guerriero, L.; Fabbrocini, G.; Patruno, C. Urticaria relapse after mRNA COVID-19 vaccines in patients affected by chronic spontaneous urticaria and treated with antihistamines plus omalizumab: A single-center experi-ence. Dermatol. Ther. 2022, 35, e15838. [Google Scholar] [CrossRef]
- Megna, M.; Potestio, L.; Battista, T.; Camela, E.; Genco, L.; Noto, M.; Fabbrocini, G.; Martora, F. Immune response to COVID-19 mRNA vaccination in patients with psoriasis undergoing treatment with biologics. Clin. Exp. Dermatol. 2022, 47, 2310–2312. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Bielsa, A.; Gracia-Cazaña, T.; Aldea-Manrique, B.; Abadías-Granado, I.; Ballano, A.; Bernad, I.; Gilaberte, Y. COVID-19 infection and vaccines: Potential triggers of Herpesviridae reactivation. An. Bras. de Dermatol. 2023, 98, 347–354. [Google Scholar] [CrossRef]
- Herzum, A.; Trave, I.; D’Agostino, F.; Burlando, M.; Cozzani, E.; Parodi, A. Epstein-Barr virus reactivation after COVID-19 vac-cination in a young immunocompetent man: A case report. Clin. Exp. Vaccine Res. 2022, 11, 222–225. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).