Abstract
Background Sotrovimab, a monoclonal antibody against SARS-CoV-2, is used as a pre-exposition prophylaxis (PrEP) against COVID-19, but monitoring strategies using routine test systems have not been defined. Methods Twenty kidney transplant recipients without antibodies after vaccination received 500 mg Sotrovimab. Antibody levels were quantified over eight weeks using live-virus neutralization (BA1 and BA2), antibody binding assays (TrimericS, Elecsys, QuantiVAC) and surrogate virus neutralization tests (sVNTs; TECOmedical, cPass and NeutraLISA). Results Sotrovimab neutralized both Omicron subvariants (BA1 NT titer 90 (+−50) > BA2 NT titer 33 (+−15) one hour post infusion). Sotrovimab was measurable on all used immunoassays, although a prior 1:100 dilution was necessary for Elecsys due to a presumed prozone effect. The best correlation with live-virus neutralization titers was found for QuantiVAC and TrimericS, with a respective R2 of 0.65/0.59 and 0.76/0.57 against BA1/BA2. Elecsys showed an R2 of 0.56/0.54 for BA1/BA2, respectively. sVNT values increased after infusion but had only a poor correlation with live-virus neutralization titers (TECOmedical and cPass) or did not reach positivity thresholds (NeutraLISA). Conclusion Antibody measurements by the used immunoassays showed differences in antibody levels and only a limited correlation with neutralization capacity. We do not recommend sVNTs for monitoring SARS-CoV-2 neutralization by Sotrovimab.
1. Introduction
During the pandemic of severe acute respiratory syndrome coronavirus type 2 (SARS-CoV-2), developing efficient vaccines was the game-changer in mediating protection against severe disease [1]. Nevertheless, not all vaccinated individuals sufficiently responded to the vaccination and produced detectable levels of neutralizing antibodies, even after multiple rounds of vaccination [2]. Such individuals were primarily patients with chronic diseases or on immunosuppressive therapy [3].
Monoclonal antibodies (mAbs) against SARS-CoV-2 were developed as a treatment option for severe SARS-CoV-2 infections and prophylaxis following exposure [4,5]. Selected mAbs were further used as a pre-exposition prophylaxis (PrEP) in an off-label application in high-risk indivudials without sufficient immune response following vaccination [4,6,7]. However, Cilgavimab/tixagevimab (Evusheld, AstraZeneca) remains the only mAb combination that was approved for PrEP.
The majority of these mAbs were less able to neutralize Omicron variants, which displayed significant antigenic changes that inhibited antibody-binding. Thus, a significant reduction in the neutralization capacity against the Omicron BA1 variant (B1.1.529) was observed for most mAbs, including cilgavimab/tixagevimab [8,9,10].
Reductions in antibody-mediated neutralization also resulted in a high rate of breakthrough infections with BA1, including the re-occurrence of clinically severe disease cases following cilgavimab/tixagevimab administration [3,4]. However, Sotrovimab (Xevudy, VIR Biotechnology GlaxoSmithKline (Brentford, UK)) retained substantial neutralizing capacities against BA1 and, together with a long half-life of 48.8 days, this made it a suitable PreP candidate in high-risk individuals following the emergence of Omicron BA.1 [7].
However, soon the question arose as to which antibody assays were best-suited to quantifying the immediate and long-term efficacy of Sotrovimab infusion. In a previous study, we applied an in-house live-virus neutralization test (NT) and showed that the administration of Sotrovimab resulted in detectable levels of neutralizing antibodies against the Omicron BA1 variant for at least eight weeks [8].
Although live-virus NTs are considered the gold standard for measuring antibodies against SARS-CoV-2, these assays are laborious and require high-biosafety-level laboratories [11,12,13,14]. To evaluate other diagnostic tools to quantify antibody levels after Sotrovimab infusion in a PrEP setting, which could also guide re-dosing, we analyzed the antibody kinetics in 20 kidney transplant reciepients (KTRs) without a sufficient response to previous COVID-19 vaccination for eight weeks after infusion of 500 mg Sotrovimab using Omicron-specific BA.1 and BA.2 live-virus NTs and three commercial surrogate NTs (sVNTs; TECOmedical cPass, NeutraLISA) and three commercial Anti-Spike immunoassays [6].
2. Materials and Methods
2.1. Patients
Twenty KTRs without a sufficient antibody response after multiple vaccinations and no prior infection with SARS-CoV-2 received 500 mg Sotrovimab in a pre-exposure prophylaxis setting. Baseline SARS-CoV-2 antibody levels were all below 15 Binding Antibody Units per milliliter (BAU/mL). Detailed patient characteristics are shown in Table 1. Blood sampling took place before and one hour after infusion, as well as two, four, and eight weeks after infusion. All samples were tested using live-virus NTs, three commercial sVNTs, and three commercial Anti-Spike antibody assays.

Table 1.
Patient characteristics. CNI: calcineurin inhibitor; MPA: mycophenolic acid; Tx: transplant.
2.2. Live-Virus Neutralization Test
The live-virus NTs were performed as described previously [15]. In brief, serum samples were incubated at 37 °C with 50–100 tissue culture infectious doses of either Omicron BA1 or BA2 virus strains for one hour. Then, this mixture was applied to a monolayer of VeroE6 cells (ECACC 85020206). After 5 days, the NT titers were assessed by microscope as the reciprocal dilution factor at which serum antibodies prevented a virus cytopathic effect. Serial dilutions ranged from 1:10 to 1:10,240. NT titers ≥ 10 were considered positive.
2.3. Surrogate Virus Neutralization Tests (sVNTs)
All samples were further tested using the following three commercial sVNTs: the cPass (GenScript Biotech, Piscataway Township, NJ, USA), the SARS-CoV-2-NeutraLISA (Euroimmun, Lübeck, Germany), and the TECO SARS-CoV-2 Neutralization Antibody Assay (TECOmedical, Sissach, Switzerland). All these tests were conducted following the manufacturers’ instructions and cut-off values, strictly adhering to the respective protocol and only performing the dilution steps recommended by the manufacturers [11]. sVNTs quantify the antibody-mediated binding inhibition (in %) between angiotensin-converting enzyme 2 (ACE2), the host receptor of SARS-CoV-2, and the viral Receptor Binding Domain (RBD) as a surrogate for the antibodies’ neutralizing abilities [11].
2.4. Anti-Spike Immunoassays
Measurements for spike-specific antibodies quantified as BAU/mL were performed using the Anti-SARS-CoV-2 QuantiVAC ELISA (Euroimmun, Lübeck, Germany), the LIAISON® SARS-CoV-2 TrimericS IgG CLIA (DiaSorin, Saluggia, Italy), and the Elecsys Anti-SARS-CoV-2 S (Roche Diagnostics GmbH, Mannheim, Germany). The tests were used following the manufacturers’ recommendations, along with the initially recommended protocols, dilution steps, and cut-off values the manufacturers [11]. Additional dilution steps (1:20, 1:40, 1:60, 1:80, and 1:100) were performed for the LIAISON® SARS-CoV-2 TrimericS IgG CLIA and a single dilution (1:100) for the Elecsys Anti-SARS-CoV-2 S. In principle, these assays measure Spike-specific IgG (QuantiVAC, LIAISON® SARS-CoV-2 TrimericS) or RBD-specific antibodies of all immunoglobulin classes (Elecsys Anti-SARS-CoV-2 S) after binding to the respective target antigen in the assay, either by an enzymatic colorimetric reaction (QuantiVAC) or through (electro)-chemoluminescence (LIAISON® SARS-CoV-2 TrimericS, Elecsys Anti-SARS-CoV-2 S).
2.5. Statistical Analysis
The mean, standard deviation and confidence interval were calculated for all antibody levels, and sensitivity and specificity were calculated for the antibody cut-off levels. Ordinary least square (OLS) regression analysis was used for correlation. Due to the lognormal distribution of BA1 and BA2 test results, these data were transformed for regression analysis by logarithm (base 10) before use in regression analysis.
3. Results
3.1. Omicron BA1 and BA2 Neutralization Titers for Serum Samples after Sotrovimab Infusion
Before the infusion of Sotrovimab, all KTRs tested negative in the Omicron-BA1- and BA2-specific live-virus NTs (all titers < 10). As shown in Figure 1, one hour after infusion, mean neutralization titers against BA1 peaked at 88 (SD: +−51) and decreased to 40 (SD: +−26), 33 (SD: +−10.60) and 25 (SD: +−16) at two, four and eight weeks, respectively. Overall, live-virus NT titers against BA2 were lower compared to BA1 peaking at 33 (SD: +−15), one hour after infusion. Titers subsequently decreased to 20 (SD: +−9) at week two, and were already negative at week four in all but two patients.
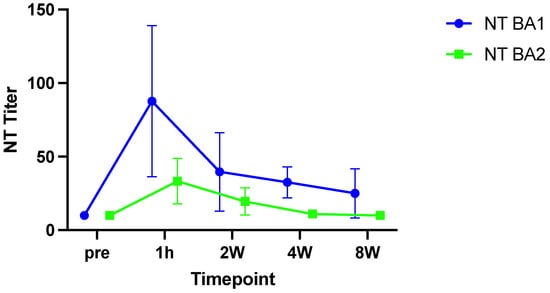
Figure 1.
Live virus neutralization tests for BA1 (blue) and BA2 (green). Reduced neutralization capacity is observed for Sotrovimab against the BA2 subvariant. Mean and standard deviation are shown. NT: neutralization test.
3.2. Kinetics of Anti-Spike Antibodies Quantified in BAU/mL
Although the Anti-SARS-CoV-2 QuantiVAC ELISA and the LIAISON® SARS-CoV-2 TrimericS IgG CLIA measured Spike-specific IgG antibodies, both antibody assays showed significant variation in the measured antibody levels in BAU/mL over time after infusion with Sotrovimab.
Antibody levels measured with the QuantiVAC ELISA peaked at 5244 BAU/mL (SD: +−2292) one hour after infusion, and subsequently decreased to 1808.34 BAU/mL (SD: +−526.12) after two weeks, to 1537 BAU/mL (SD: +−459) after four, and to 1048.45 BAU/mL (SD: +−373.30) after eight weeks, respectively (Figure 2A).
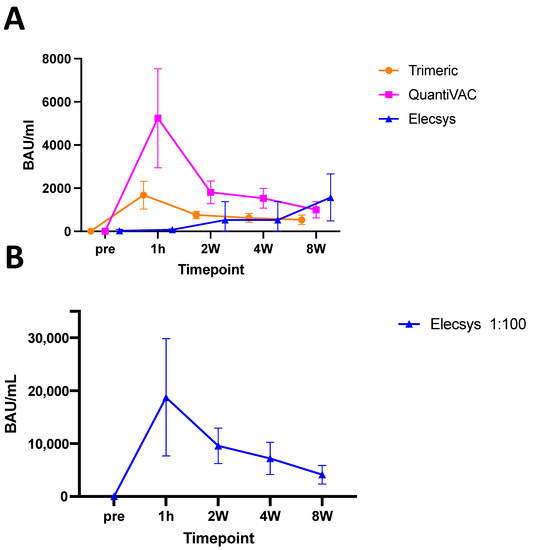
Figure 2.
Antibody measurements by (A) TrimericS CLIA (Orange), QuantiVAC ELISA (pink), Elecsys systems (blue) and (B) Elecsys after 1:100 dilution. Initial increase after infusion is followed by reduced antibodies over time, as expected. For the Elecsys system, a prior 1:100 dilution is necessary due to a presumed prozone effect. Shown are mean and standard deviation.
Spike-specific IgG antibody levels assessed with the LIAISON® SARS-CoV-2 TrimericS IgG CLIA showed similar kinetics to the antibody levels quantified with the QuantiVAC ELISA, but reached a maximum of 1680.92 BAU/mL (SD: +−643.41) one hour after infusion and decreased to 762 BAU/mL (SD: +−168), 634 BAU/mL (SD: 204) and 536 (SD: +−220) two, four and eight weeks after application.
Notably, the Elecsys Anti-SARS-CoV-2 S ECLIA were measured to have significantly lower antibody levels than the other assays. One hour after Sotrovimab application, the Elecsys Anti-SARS-CoV-2 S ECLIA quantified a mean of 77 BAU/mL (SD: +−39), slightly increasing over time and reaching levels of 530 BAU/mL (SD: +−849) two weeks, 999 BAU/mL (SD: +−597) four weeks, and 1572 BAU/mL (SD: +−1089) eight weeks post-infusion.
The antibody measurements with the Elecsys Anti-SARS-CoV-2-2 S ECLIA showed high variability between individuals, ranging from >2500 to 145 BAU/mL at two weeks and >2500 BAU/mL to 221 BAU/mL at eight weeks after sotrovimab infusion. Since these measurements were not plausible, we speculated that a prozone effect occurred. Therefore, we performed additional dilution series of the patient serum samples. After an additional 1:100 dilution, the antibody kinetics measured with Elecsys Anti-SARS-CoV-2-2 S ECLIA were similar to the other two assays, with peak values of 18,750 BAU/mL one hour after infusion (SD: +−11,078) followed by a decrease to 9585 BAU/mL (SD: +−3358), 7197 U/mL (SD: +−3049) and 4120 U/mL (SD: +−1767) two, four, and eight weeks after infusion, respectively (Figure 2B).
3.3. Antibody Kinetics as Measured by Surrogate Virus Neutralization Tests
Next, we tested the KTRs samples after Sotrovimab PrEP infusion with multiple sVNTs (ACE2-RBD-binding-inhibition assays). As shown in Figure 3, the cPass and the TECO SARS-CoV-2 Neutralization Antibody Assay showed similar kinetics with an increase in ACE2-RBD-binding-inhibition (in %). However, the individual levels of % binding inhibition significantly varied among the two assays. From baseline (pre-infusion) to one-hour post Sotrovimab infusion, the increase was from a mean of 7.43% (SD: +−6.65) to 57.27% (SD: 14.86) for the TECO SARS-CoV-2 Neutralization Antibody Assay and from −13.52% (SD: 10.58) to 42.50% (SD: 11.31) for the cPass, respectively (Figure 3). In consecutive measurements at two, four and eight weeks after Sotrovimab infusion, the levels of ACE2-RBD-inhibition measured by cPass were lower than the ones measured with the TECO SARS-CoV-2 Neutralization Antibody Assay with a median level of 55.80% (SD: 12.15) and 41.08% (SD: 9.40) at week two, 57.56% (SD: 13.49) compared to 41.55% (SD: 9.90) at week four and 56.99% (SD: 15.41) and 41.71% (SD: 11.50) at week eight for the TECO SARS-CoV-2 Neutralization Antibody Assay and cPass, respectively.
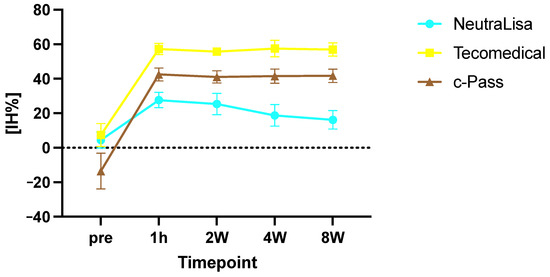
Figure 3.
Surrogat neutralization test results determined with the NeutraLISA (blue), Teicomedical (yellow) and cPass system (brown). Signal inhibition (IH%) increased after infusion and remained high over the entire observational time. Shown are mean and standard deviation.
Notably, the SARS-CoV-2-NeutraLISA measured significantly lower levels of ACE2-RBD-binding inhibition in the same samples, with median levels of 27.88% (SD: 8.40) one hour after infusion, 25.23% (SD: 8.21) at two weeks, 18.97% (SD: 7.50) at four weeks, and 16.15% (SD: 6.80) at eight weeks after infusion. When using the cut-off levels provided by the manufacturer, these results would be interpreted as negative for neutralizing antibodies (cut-off level of 35%).
3.4. Correlation of Titers of Neutralizing Antibodies with Levels of Commercial Assays
Subsequently, the titers of neutralizing antibodies determined in the live-virus NTs of the samples were correlated with the antibody levels measured by the commercial antibody assays. The LIAISON® SARS-CoV-2 TrimericS IgG CLIA and QuantiVAC ELISA Q had the best correlation with NT titers against the BA1 variant and, to a lesser extent, against the BA2 variant (R2: 0.65 and 0.59 for QuantiVAC and 0.76 and 0.57 for the TrimericS IgG assay for BA1 and BA2, respectively; Figure 4). Following additional dilution, the correlation between NT titers and the BAU/mL levels measured from the Elecsys Anti-SARS-CoV-2 S ECLIA was weaker, with an R2 of 0.56 and 0.54 for BA1 and BA2, respectively.
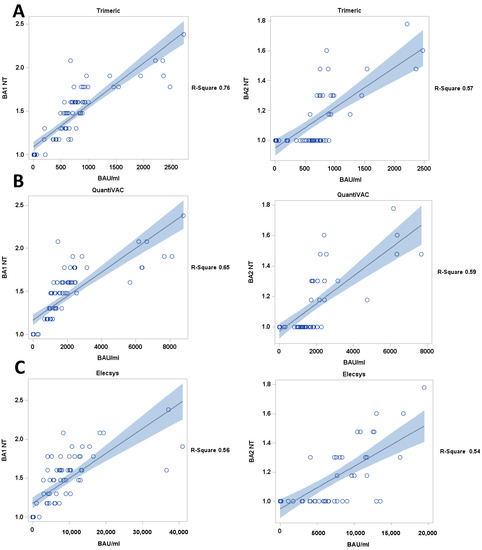
Figure 4.
Correlation of antibody levels (BAU/mL) and live-virus BA1 and BA2 NT titers, (A) TrimericS and (B) QuantiVAC an (C) Elecsys (diluted samples) assay. black line: regression line, blue: confidence limits; Y axis = BA1 NT titers, BA2 NT titers.
Importantly, the correlation between live-virus NT titers and levels of ACE2-RBD-binding inhibition after Sotrovimab infusion was very weak for cPass and TECO SARS-CoV-2 Neutralization Antibody Assay, with an R2 of 0.46 and 0.10 and 0.46 and 0.11 for BA1 and BA2 for each test respectively. Of note, the NeutraLISA sVNT showed a higher R2 of 0.58 and 0.27 for BA1 and BA2, respectively, but the results were all negative, as defined by the manufacturer (Figure 5).
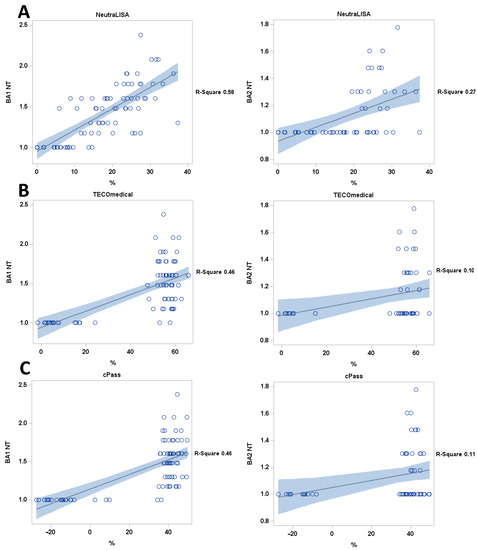
Figure 5.
Correlation of sVNTs (A) NeutraLISA, (B) TECOmedical and (C) cPass with live-virus NT titers. All sVNTs show poor correlation with live-virus NT results. black line: regression line, blue: confidence limits; blue dotted blue lines: prediction limits; Y axis = BA1 NT titers, BA2 NT titers.
3.5. Cut-Off Levels of Antibody Measurements and Live-Virus Neutralization
A 100% specificity for in vitro neutralizing capacity against BA1 in patient sera (defined as NT titer ≥ 10) was observed at antibody levels of 750 BAU/mL on the LIAISON® SARS-CoV-2 TrimericS IgG CLIA, 2100 BAU/mL on the QuantiVAC ELISA and 4060 BAU/mL on the Elecsys assay (after 1:100 dilution). At these values, the sensitivity was 58.1% for the LIAISON® SARS-CoV-2 TrimericS IgG CLIA assay, 43.9% for the QuantiVAC ELISA system and 96.2% for the Elecsys assay (Figure 6).
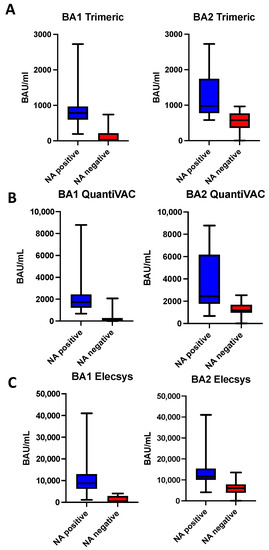
Figure 6.
Measured antibody levels (BAU/mL) with the Elecsys (A), TrimericS (B) and QuantiVAC (C) assays stratified by live-virus NT results. Shown are median, first and third quartile.
For the BA2 variant antibody level, cut-offs with 100% specificity for a positive in-vitro neutralization result were 965 BAU/mL for the LIAISON® SARS-CoV-2 TrimericS IgG CLIA, 2538 BAU/mL for the QuantiVAC ELISA and 13,500 BAU/mL for the Elecsys assay (after 1:100 dilution). The corresponding sensitivity values were 48%, 40.8% and 36% for the LIAISON® SARS-CoV-2 TrimericS IgG CLIA assay, the QuantiVAC ELISA system and the Elecsys assay.
We were not able to define a cut-off value for the surrogate NTs as inhibition percentage values persisted at high levels over the entire observational period after Sotrovimab infusion or did not reach the defined thresholds for positivity (Figure 3).
4. Discussion
In this study, we analyzed the ability of several readily available high-throughput SARS-CoV-2 antibody measurement systems (three platforms to quantify anti-spike protein antibody levels, i.e., QuantiVAC, TrimericS IgG and Elecsys Anti-SARS-CoV-2 S assay; and three surrogate neutralization tests, i.e., TECO SARS-CoV-2 Neutralization Antibody Assay, cPass and NeutraLISA) to determine Sotrovimab antibody levels in serum samples from patients following PrEP with Sotrovimab. We were able to define anti-spike protein antibody cut-off levels associated with 100% specificity with the in vitro virus neutralization of SARS-CoV-2 Omicron sub-variants that could be used to guide the re-dosing of Sotrovimab. However, some of the evaluated systems showed relevant limitations restricting their use in quantifying antibody levels following Sotrovimab infusion in clinical routine diagnostics. Specifically, the Elecsys system requires an additional dilution (1:100) to avoid inadequately low antibody level read-outs due to the presumed prozone effect caused by the high levels of the monoclonal antibody. Furthermore, all surrogate NT-tests showed poor performance and a low correlation with live-virus NT titers and should not be used to guide Sotrovimab dosing in PrEP. Overall, the measured antibody levels showed a high variability across the different commercial antibody quantification assays, probably due to significant differences in the binding of the monoclonal antibodies to the different target antigens incorporated in the test systems.
The commercial test systems were compared to live-virus Omicron BA1 and BA2 NTs that represented the dominant SARS-CoV-2 variants circulating in Austria at the beginning of 2022 (Figure 1). The measured NT titers were in line with the literature, pointing to the reduced effectiveness of Sotrovimab against these subvariants, which showed significant antigenic changes affecting antibody binding compared to the ancestral wild-type [8,9,10].
Since NTs require high biosafety level laboratories and are laborious, we and others aimed to correlate the antibody levels measured with commercial antibody assays to these NT titers [16]. We observed a high level of variability across all three commercial anti-spike antibody assays when quantifying Sotrovimab in patient serum, despite the normalization of antibody concentrations to the WHO-recommended measuring unit BAU/mL.
Multiple studies have demonstrated such variations [11,17,18]. Indeed, when the same samples from individuals after SARS-CoV-2 infections or vaccinations are comparatively tested, the LIAISON® SARS-CoV-2 TrimericS IgG CLIA usually measures higher BAU/mL levels than the QuantiVAC [11,17]. Interestingly, data from this recent study demonstrated a converse pattern in patients after Sotrovimab infusion, probably due to differences in the binding of the mAbs to the epitopes of the assays´ respective target antigens, whose conformation may vary. Additionally, we found a prozone effect for the Elecsys Anti-SARS-CoV-2 S ECLIA, probably caused by the high level of mAb competing for antigen binding at the same site (Figure 2A). Following an additional dilution step, the antibody levels measured by the Elecsys assay showed the expected kinetics over time, correlated with the antibody profiles assessed by the other assays, confirming the hypothesis [19]. In particular, the prozone effect was most pronounced in the samples obtained one hour after infusion and was diminished at later timepoints. In a previous study, a similar dilution was performed before the Elecsys assay measurements in highly concentrated samples [6].
Notably, we could further show that Sotrovimab strongly affected the results from sVNTs. First, we observed high inter-assay variation that exceeded the variation levels observed in serum samples from convalescent individuals [11]. Furthermore, in contrast to samples from convalescents, we observed higher levels in the TECO SARS-CoV-2 Neutralization Antibody Assay than the cPass [11]. Indeed, while the cPass and TECO SARS-CoV-2 Neutralization Antibody assay provided positive results in all samples, the NeutraLISA failed to detect Sotrovimab neutralization and always tested negative.
Such substantial differences in the results of the sVNTs after Sotrovimab infusion can be explained by the test principle of these assays, which measure the binding inhibition between the viral receptor-binding domain (RBD) and the angiotensin-converting enzyme 2 (ACE2). Since the target binding site of Sotrovimab is a highly conserved epitope outside the ACE2 binding site, this may have significantly affected the readout of these assays [14,20]. Indeed, since sVNTs assess the antibody-mediated RBD-ACE2-binding inhibition, any mismatch between the RBD used in the assay and the epitopes to which the RBD-specific antibodies in the sample are directed can diminish their potential as a substitute assay for live-virus NTs. Similarly to the loss in sensitivity when detecting mAbs after Sotrovimab administration, sVNTs were significantly reduced in their ability to identify the antibody response in individuals after primary Omicron infection, whose antibodies are exclusively directed against the antigenically changed RBD of the Omicron variant [21]. Furthermore, conformational differences in the RBD used as the respective assays´ target antigen could contribute to the inter-assay variations we observed in the present study.
Since Anti-Spike immunoassays (QuantiVAC, TrimericS IgG) use the entire Spike protein as the target antigen, this may explain their improved ability to assess Sotrovimab levels, as indicated by the stronger correlation between the measured BAU/mL levels and the NT titers (Figure 4). However, the evaluated commercial immunoassays still use the ancestral Spike (or RBD) of the ancestral wild-type as the antigen. In principle, such a mismatch could have affected the correlation between the antibody levels quantified by these assays and Omicron-specific NT titers. Thus, further studies should evaluate whether novel immunoassays containing the Omicron variant´s Spike protein display a better correlation. Nonetheless, the significant inter-assay variations we observed exclusively occurred in immunoassays that were not yet adapted to the Omicron variant.
A limitation of this study is that we did not determine the clinical effectiveness of Sotrovimab as PrEP, but rather focused on comparing the measured antibody levels and live-virus NT results. The effectiveness of Sotrovimab against the currently circulating variants has decreased [8,9,10,22]. However, SARS-CoV-2 is currently mutating, so the return of virus variants that are more susceptible to Sotrovimab cannot be excluded, as recent studies suggest for variants BA2.75.2, BQ1.1 and XBB1.5 [22,23,24,25]. Cut-off levels for future variants with increased or similar susceptibility to Sotrovimab can be easily assessed using adapted NTs. In addition, a higher dosing of Sotrovimab is currently being tested in clinical studies and may provide a feasible strategy to overcome their reduced effectiveness, further emphasizing the need for a monitoring strategy, as outlined in this study [26].
In conclusion, this study shows significant variations among commercial antibody assays in measuring Sotrovimab concentration in human serum samples after infusion. Nonetheless, although the correlation of antibody levels measured by immunoassays and live-virus NT titers was limited for certain tests, immunoassays present a viable alternative for guiding Sotrovimab redosing in PrEP, as long as conservative cut-offs are employed. However, as in other fields of laboratory diagnostics, specific SARS-CoV-2 immunoassays have to be carefully selected for the respective application area. In this regard, our study demonstrates that, compared to Spike-specific IgG antibody assays, sVNTs are limited in their ability to guide Sotrovimab redosing in PrEP.
Author Contributions
Conceptualization, R.R.-S., L.W., A.H. and R.O.; methodology: K.S., C.B., J.K., W.W., K.H., C.A. and H.H.; statistical analysis: A.K. and A.H.; writing—original draft preparation: C.A., R.R.-S., A.H., L.W. and R.O.; writing—review and editing: L.W., R.R.-S., A.H., A.K., C.A., K.S., K.H., W.W., J.K., C.B., R.O. and H.H.; visualization: A.K., A.H. and C.A.; supervision: R.R.-S., R.O. and A.H.; funding acquisition: R.R.-S. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by the Medical-Scientific Fund of the Mayor of the Federal Capital of Vienna (Project-Nr. 21182) and the Christine Vranitzky-Stiftung Research Grant 2020.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethics Committee of the medical university of Vienna (1362/2020; 4 July 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study prior to the study.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We thank Jutta Hutecek for technical assistance.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Graña, C.; Ghosn, L.; Evrenoglou, T.; Jarde, A.; Minozzi, S.; Bergman, H.; Buckley, B.S.; Probyn, K.; Villanueva, G.; Henschke, N. Efficacy and safety of COVID-19 vaccines. Cochrane Database Syst. Rev. 2022, 12, CD015477. [Google Scholar]
- Cowan, M.; Chon, W.J.; Desai, A.; Andrews, S.; Bai, Y.; Veguilla, V.; Katz, J.M.; Josephson, M.A.; Wilson, P.C.; Sciammas, R.; et al. Impact of Immunosuppression on Recall Immune Responses to Influenza Vaccination in Stable Renal Transplant Recipients. Transplantation 2014, 97, 846–853. [Google Scholar] [CrossRef] [PubMed]
- Reindl-Schwaighofer, R.; Heinzel, A.; Mayrdorfer, M.; Jabbour, R.; Hofbauer, T.M.; Merrelaar, A.; Eder, M.; Regele, F.; Doberer, K.; Spechtl, P.; et al. Comparison of SARS-CoV-2 Antibody Response 4 Weeks After Homologous vs Heterologous Third Vaccine Dose in Kidney Transplant Recipients: A Randomized Clinical Trial. JAMA Intern. Med. 2022, 182, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Akinosoglou, K.; Rigopoulos, E.-A.; Kaiafa, G.; Daios, S.; Karlafti, E.; Ztriva, E.; Polychronopoulos, G.; Gogos, C.; Savopoulos, C. Tixagevimab/Cilgavimab in SARS-CoV-2 Prophylaxis and Therapy: A Comprehensive Review of Clinical Experience. Viruses 2022, 15, 118. [Google Scholar] [CrossRef] [PubMed]
- Sotrovimab: First Approval—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/35286623/ (accessed on 18 April 2023).
- Totschnig, D.; Augustin, M.; Niculescu, I.; Laferl, H.; Jansen-Skoupy, S.; Lehmann, C.; Wenisch, C.; Zoufaly, A. SARS-CoV-2 Pre-Exposure Prophylaxis with Sotrovimab and Tixagevimab/Cilgavimab in Immunocompromised Patients-A Single-Center Experience. Viruses 2022, 14, 2278. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Gonzalez-Rojas, Y.; Juarez, E.; Crespo Casal, M.; Moya, J.; Rodrigues Falci, D.; Sarkis, E.; Solis, J.; Zheng, H.; Scott, N.; et al. Effect of Sotrovimab on Hospitalization or Death Among High-risk Patients With Mild to Moderate COVID-19, A Randomized Clinical Trial. JAMA 2022, 327, 1236–1246. [Google Scholar] [CrossRef] [PubMed]
- Stiasny, K.; Weseslindtner, L.; Heinzel, A.; Camp, J.V.; Oberbauer, R.; Reindl-Schwaighofer, R. SARS-CoV-2 Omicron BA.1/BA.2 Neutralization up to 8 Weeks After PrEP With Sotrovimab or Cilgavimab/Tixagevimab. Transpl. Int. 2022, 35, 10906. [Google Scholar] [CrossRef]
- Aggarwal, N.R.; Beaty, L.E.; Bennett, T.D.; Carlson, N.E.; Mayer, D.A.; Molina, K.C.; Peers, J.L.; Russell, S.; Wynia, M.K.; Ginde, A.A. Change in effectiveness of sotrovimab for preventing hospitalization and mortality for at-risk COVID-19 outpatients during an Omicron BA.1 and BA.1.1-predominant phase. Int. J. Infect. Dis. 2023, 128, 310–317. [Google Scholar] [CrossRef]
- Cox, M.; Peacock, T.P.; Harvey, W.T.; Hughes, J.; Wright, D.W.; Willett, B.J.; Thomson, E.; Gupta, R.K.; Peacock, S.J.; Robertson, D.L. SARS-CoV-2 variant evasion of monoclonal antibodies based on in vitro studies. Nat. Rev. Microbiol. 2023, 21, 112–124. [Google Scholar] [CrossRef]
- Graninger, M.; Jani, C.M.; Reuberger, E.; Prüger, K.; Gaspar, P.; Springer, D.N.; Borsodi, C.; Weidner, L.; Rabady, S.; Puchhammer-Stöckl, E.; et al. Comprehensive Comparison of Seven SARS-CoV-2-Specific Surrogate Virus Neutralization and Anti-Spike IgG Antibody Assays Using a Live-Virus Neutralization Assay as a Reference. Microbiol. Spectr. 2023, 11, e0231422. [Google Scholar] [CrossRef]
- Kohmer, N.; Rühl, C.; Ciesek, S.; Rabenau, H.F. Utility of Different Surrogate Enzyme-Linked Immunosorbent Assays (sELISAs) for Detection of SARS-CoV-2 Neutralizing Antibodies. J. Clin. Med. 2021, 10, 2128. [Google Scholar] [CrossRef] [PubMed]
- Krüttgen, A.; Lauen, M.; Klingel, H.; Imöhl, M.; Kleines, M. Two novel SARS-CoV-2 surrogate virus neutralization assays are suitable for assessing successful immunization with mRNA-1273. J. Virol. Methods 2022, 299, 114297. [Google Scholar] [CrossRef] [PubMed]
- Münsterkötter, L.; Hollstein, M.M.; Hahn, A.; Kröger, A.; Schnelle, M.; Erpenbeck, L.; Groß, U.; Frickmann, H.; Zautner, A.E. Comparison of the Anti-SARS-CoV-2 Surrogate Neutralization Assays by TECOmedical and DiaPROPH-Med with Samples from Vaccinated and Infected Individuals. Viruses 2022, 14, 315. [Google Scholar] [CrossRef] [PubMed]
- Medits, I.; Springer, D.N.; Graninger, M.; Camp, J.V.; Höltl, E.; Aberle, S.W.; Traugott, M.T.; Hoepler, W.; Deutsch, J.; Lammel, O.; et al. Different Neutralization Profiles After Primary SARS-CoV-2 Omicron BA.1 and BA.2 Infections. Front. Immunol. 2022, 13, 946318. [Google Scholar] [CrossRef]
- Lau, E.H.Y.; Tsang, O.T.Y.; Hui, D.S.C.; Kwan, M.Y.W.; Chan, W.; Chiu, S.S.; Ko, R.L.; Chan, K.H.; Cheng, S.M.; Perera, R.A. Neutralizing antibody titres in SARS-CoV-2 infections. Nat. Commun. 2021, 12, 63. [Google Scholar] [CrossRef] [PubMed]
- Buchta, C.; Springer, D.; Jovanovic, J.; Borsodi, C.; Weidner, L.; Sareban, N.; Radler, U.; Müller, M.M.; Griesmacher, A.; Puchhammer-Stöckl, E. Three rounds of a national external quality assessment reveal a link between disharmonic anti-SARS-CoV-2 antibody quantifications and the infection stage. Clin. Chem. Lab. Med. 2023, 61, 1349–1358. [Google Scholar] [CrossRef]
- Perkmann, T.; Perkmann-Nagele, N.; Koller, T.; Mucher, P.; Radakovics, A.; Marculescu, R.; Wolzt, M.; Wagner, O.F.; Binder, C.J. Anti-Spike Protein Assays to Determine SARS-CoV-2 Antibody Levels: A Head-to-Head Comparison of Five Quantitative Assays. Microbiol. Spectr. 2021, 9, e0024721. [Google Scholar] [CrossRef]
- Van Loghem, J.J.; Kresner, M.; Coombs, R.R.A.; Fulton Roberts, G. Observations on a prozone phenomenon encountered in using the anti-globulin sensitisation test. Lancet 1950, 256, 729–732. [Google Scholar] [CrossRef]
- Magnus, C.L.; Hiergeist, A.; Schuster, P.; Rohrhofer, A.; Medenbach, J.; Gessner, A.; Peterhoff, D.; Schmidt, B. Targeted escape of SARS-CoV-2 in vitro from monoclonal antibody S309, the precursor of sotrovimab. Front. Immunol. 2022, 13, 966236. [Google Scholar] [CrossRef]
- Springer, D.N.; Perkmann, T.; Jani, C.M.; Mucher, P.; Prüger, K.; Marculescu, R.; Reuberger, E.; Camp, J.V.; Graninger, M.; Borsodi, C. Reduced Sensitivity of Commercial Spike-Specific Antibody Assays after Primary Infection with the SARS-CoV-2 Omicron Variant. Microbiol. Spectr. 2022, 10, e0212922. [Google Scholar] [CrossRef]
- Touret, F.; Baronti, C.; Pastorino, B.; Villarroel, P.M.S.; Ninove, L.; Nougairède, A.; de Lamballerie, X. In vitro activity of therapeutic antibodies against SARS-CoV-2 Omicron BA.1, BA.2 and BA.5. Sci. Rep. 2022, 12, 12609. [Google Scholar] [CrossRef]
- Corey, L.; Beyrer, C.; Cohen, M.S.; Michael, N.L.; Bedford, T.; Rolland, M. SARS-CoV-2 variants in immunosuppressed individuals. N. Engl. J. Med. 2021, 385, 562–566. [Google Scholar] [CrossRef] [PubMed]
- Bruel, T.; Vrignaud, L.L.; Porrot, F.; Staropoli, I.; Planas, D.; Guivel-Benhassine, F.; Puech, J.; Prot, M.; Munier, S.; Bolland, W.H. Antiviral activities of sotrovimab against BQ.1.1 and XBB.1.5 in sera of treated patients. medRxiv 2023, medRxiv:2023.05.25.23290512. [Google Scholar]
- Touret, F.; Giraud, E.; Bourret, J.; Donati, F.; Tran-Rajau, J.; Chiaravalli, J.; Lemoine, F.; Agou, F.; Simon-Loriere, E.; Van Der Werf, S. Enhanced neutralization escape to therapeutic monoclonal antibodies by SARS-CoV-2 Omicron sub-lineages. biorxiv 2022, biorxiv:2022.12.22.521201. [Google Scholar] [CrossRef] [PubMed]
- University of Oxford. Randomised Evaluation of COVID-19 Therapy. Clinical Trial Registration 2023. Available online: https://clinicaltrials.gov/study/NCT04381936?tab=results (accessed on 19 March 2020).






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).