Abstract
Viral respiratory diseases place a heavy burden on the healthcare system, with children making up a significant portion of related hospitalizations. While comorbidities increase the risk of complications and poor outcomes, many hospitalized children lack clear risk factors. As new vaccines for respiratory viral diseases emerge, this study examined pediatric respiratory hospitalizations, focusing on viral etiology, complication rates, and the impact of comorbidities to guide future policy. Data were analyzed from eight pre-COVID influenza seasons (2011/2012–2018/2019) involving patients under 18 years hospitalized with respiratory complaints across 4–10 hospitals in Valencia, Spain. Respiratory specimens were tested for eight viral targets using multiplex real-time reverse-transcription polymerase chain reaction. Demographics, clinical outcomes, discharge diagnoses, and laboratory results were examined. Among the hospitalized children, 26% had at least one comorbidity. These children had higher rates of pneumonia, asthma exacerbation, and pneumothorax, and were twice as likely to require ICU admission, though mechanical ventilation and length of stay were similar to those without comorbidities. Respiratory syncytial virus (RSV) was the most common virus detected (23.1%), followed by rhinovirus/enterovirus (9.5%) and influenza (7.2%). Viral codetection decreased with age, occurring in 4.6% of cases. Comorbidities increase the risk of complications in pediatric respiratory illnesses, however, healthcare utilization is driven largely by otherwise healthy children. Pediatric viral vaccines could reduce this burden and should be further evaluated.
1. Introduction
Acute respiratory illnesses are an important cause of pediatric morbidity and mortality, with pneumonia being the main cause of death among children <5 years worldwide [1]. Viruses have been identified as the most common etiology of pneumonia in children [2], with those with comorbidities being at highest risk for complications [3]. For this reason, public health officials and policymakers have often prioritized people with comorbidities in health interventions and prevention measures [4,5,6,7]. Nonetheless, data among children with influenza, RSV, and more recently COVID-19, indicate that many children hospitalized with respiratory illness associated with these pathogens are otherwise healthy [5,8,9,10,11,12,13,14], contributing nonetheless to considerable healthcare utilization [15]. With the success of mRNA and adenovirus vaccine platforms [16], new vaccines against respiratory illnesses combining various viral targets have been discussed or are under development [17,18]. Young children, for instance, could potentially benefit from vaccines that target viruses, leading to medically attended illness. Investigating the impact of chronic medical conditions in children hospitalized with respiratory illness can improve our understanding of associated clinical outcomes and provide an evidence base to support policymakers on the prioritization of interventions.
We used data from a prospective active surveillance study conducted before the COVID-19 pandemic to investigate the characteristics of pediatric patients hospitalized with respiratory illness in healthcare district reference hospitals in the Valencia region, Spain. We describe the frequency of severe outcomes and complications by presence of comorbidities and explore associations with viral etiologies.
2. Materials and Methods
2.1. Population
We analyzed the data of patients aged <18 years hospitalized with respiratory complaints during the respiratory seasons 2011/12 to 2018/19. The respiratory season was defined as November to March/April for most seasons, except in 2017/18 where surveillance was extended from September to June and in 2018/19 where surveillance was year-round. This analysis used data collected from 4–10 hospitals (covering between 21% and 46% of the total population of the Valencia region of Spain, which is around 5 million) from a prospective hospital-based active surveillance study for acute respiratory illness [19,20,21,22,23]. Data collected during the 2019/20 and 2020/21 seasons were not included in our analysis as the preventive measures implemented during the COVID-19 pandemic impacted both healthcare seeking behavior and the circulation of respiratory viruses [24,25].
2.2. Inclusion Criteria
Children hospitalized with an acute respiratory illness, with an onset of <7 days from admission and resident in one of the participating hospitals’ catchment areas, were eligible for enrolling [26]. Patients discharged 30 days prior to the present admission were excluded to remove multiple enrolments during what have might been the same illness episode and to avoid the inclusion of nosocomial infections. Institutionalized patients and those who were not local residents were also excluded from the study.
2.3. Laboratory Methods
Enrolled patients had oropharyngeal and nasopharyngeal swabs if aged ≥14 years, or nasal and oropharyngeal swabs if aged <14 years, collected within 8–48 h of admission. Both swabs were combined in one tube of viral transport media (Copan, Brescia, Italy) and kept frozen at −50° to −20 °C until shipped refrigerated to a centralized virology laboratory at Fisabio-Public Health. One third of the viral transport media volume was used for the extraction of total nucleic acids using an automated silica-based method (Nuclisens e-Mag, BioMérieux, Lyon, France). Extracted nucleic acids (50 µL) were tested by five in-house multiplex real-time reverse transcription polymerase chain reaction (RT-PCR) screening assays for influenza, RSV, rhinovirus/enterovirus, adenovirus, coronavirus, bocavirus, metapneumovirus, and parainfluenza. Laboratory procedures to prevent RT-PCR contamination were strictly followed, and positive (purified viral nucleic acids Vircell, Granada, Spain) and negative controls (without sample and/or nucleic acid) were included. Positive results were defined, overall, by cycle threshold values up to 35 together with negativity of the negative controls. Negative results for viruses were only considered if the human ribonucleoprotein gene amplification was positive.
2.4. Data Sources and Categorization
Data were collected by interviewing parents/legal tutors and from the patients’ medical record on demographic characteristics, the presence of comorbidities, clinical course, and outcomes (including admission to the intensive care unit (ICU), need for mechanical ventilation (collected from the 2014/15 season), death during hospitalization, and length of hospital stay (LOS)—all considered markers of disease severity). We also captured three International Classification of Diseases Ninth or Tenth Revision (ICD-9 or ICD-10) codes assigned to the patient at discharge. The ICD codes were used to identify complications that were associated with the reason for admission (e.g., viral infection that could have evolved to pneumonia or triggered the worsening of underlying conditions) or occurred during hospitalization (e.g., sepsis). Among the children hospitalized with viral infections, complications involving the respiratory tract such as pneumonia and exacerbations of chronic lung disease as well as outside the respiratory tract such as febrile seizures and encephalopathy have been reported. Therefore, we defined complication as any diagnosis of an acute disease process such as pneumonia or bacteremia/sepsis that was grouped in broad categories (Supplementary Table S1). Codes associated with symptoms or signs and laboratory abnormalities were not considered. We also used ICD codes to complement information on the presence of comorbidities (Supplementary Tables S2 and S3). Underlying medical conditions included recurrent wheezing/asthma, heart disease, anemia, neurological/neuromuscular diseases, chronic lung disease, chronic renal disease, chronic autoimmune disease, endocrine system disease other than diabetes, diabetes, recent cerebrovascular disease, chronic liver disease, neoplastic disease, and prematurity. Finally, ICD codes were used to identify potential etiologic agents for the condition associated with the hospitalization (Supplementary Table S4). We compared them with the results from the multiplex RT-PCR, which was conducted as part of the prospective investigation. The viral multiplex results were not available for patient management nor shared with administrative staff and therefore were not used to guide discharge diagnosis coding. The LOS was recorded as the number of nights spent on the hospital. In case a child was admitted in several wards, the LOS was the sum of the lengths spent in the different wards. We divided age into four categories, namely <6 months, 6 months to <1 year, 1 to <5 years, and 5 to 17 years based on their age at the day of admission.
2.5. Statistical Method
Categorical data were described using proportions and compared using Chi-square tests or Fisher tests when the Chi-square hypotheses were not met. Continuous data were compared using t-Student tests or Wilcoxon tests when the conditions of the application of a t-Student test were not met. Confidence intervals for single proportions were calculated using the exact binomial method (Clopper–Pearson method). Logistic regression models were used to determine the odds of complications associated with the presence of at least one comorbidity. A p-value < 0.05 was indicative of statistical significance. All analyses were performed using R software.
3. Results
3.1. Demographic Characteristics and Underlying Health Status of Hospitalized Children
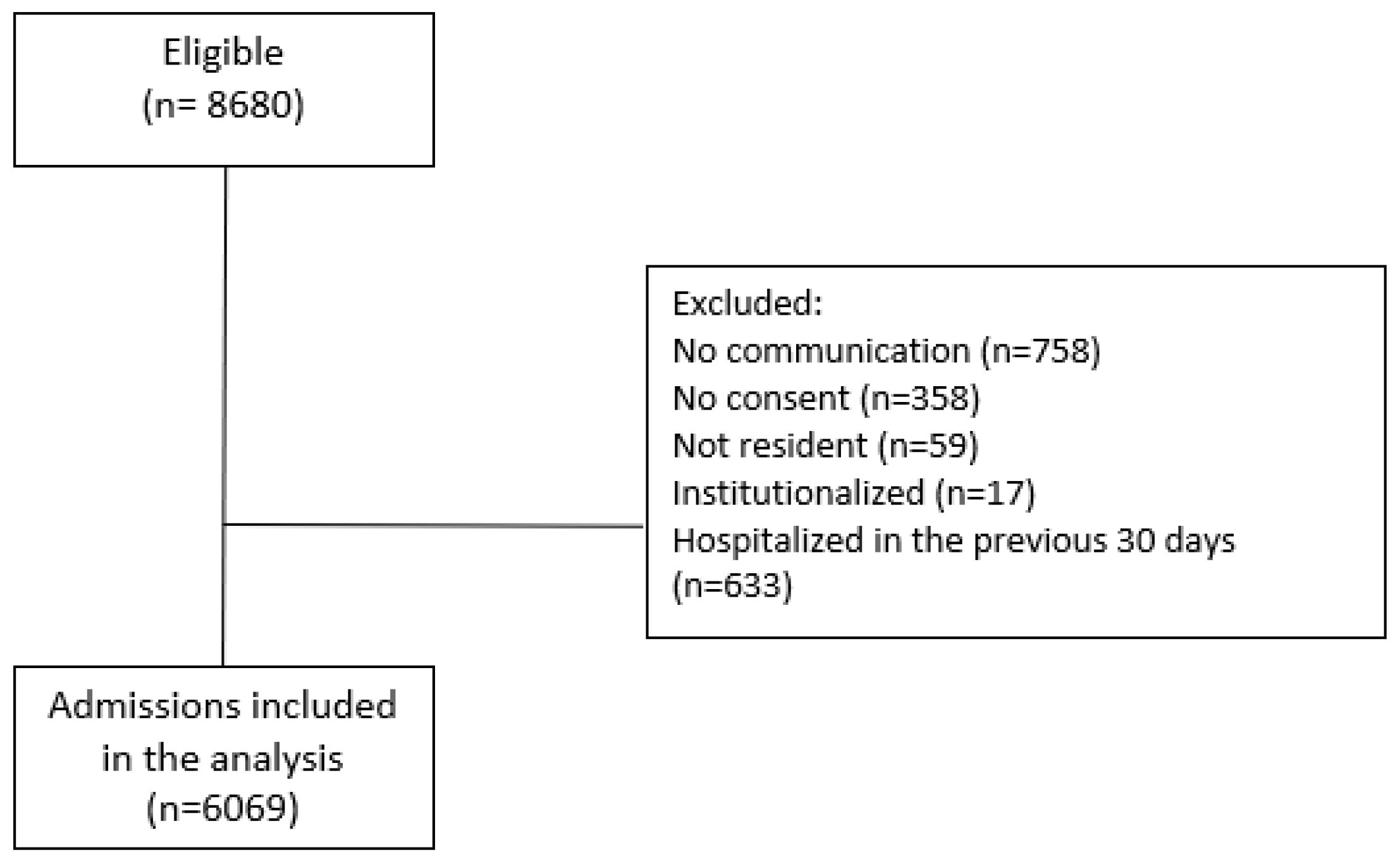
From 8680 eligible patients <18 years admitted to the study hospitals from November 2011 through July 2019, 6069 patients were included in the analysis after applying the exclusion criteria (Figure 1).
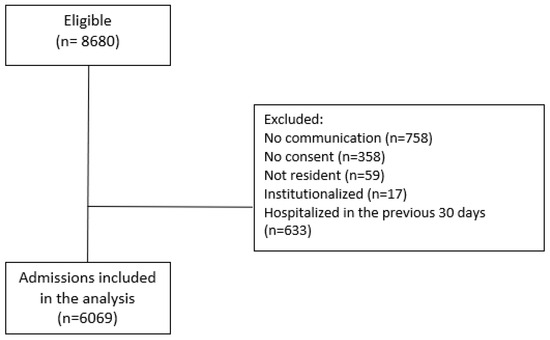
Figure 1.
Patient selection process.
Almost half of them were <1 year of age (38.9% were <6 months and 11.1% were 6 months to <1 year), and 56.8% were male. The median age among patients <1 year was 2.4 months (interquartile range [IQR], in months: 1.2–4.8) and was 2 years (IQR, in years: 1.6–4.0) for those aged ≥1 year. A total of 1600 patients (26.4%) reported at least one comorbidity, with the majority having only one comorbidity. Prematurity, lung disease, recurrent wheezing/asthma, heart disease, anemia, and neurological/neuromuscular diseases were reported in 10.5%, 8.8%, 4.7%, 2.5%, 2.1%, and 1.4% of cases, respectively. Other comorbidities were reported in less than 1% of patients (Table 1).

Table 1.
General characteristics of children at admission, Valencia region, Spain, 2011/12–2018/19.
3.2. Impact of Comorbidities on the Presence of Complications and Disease Severity
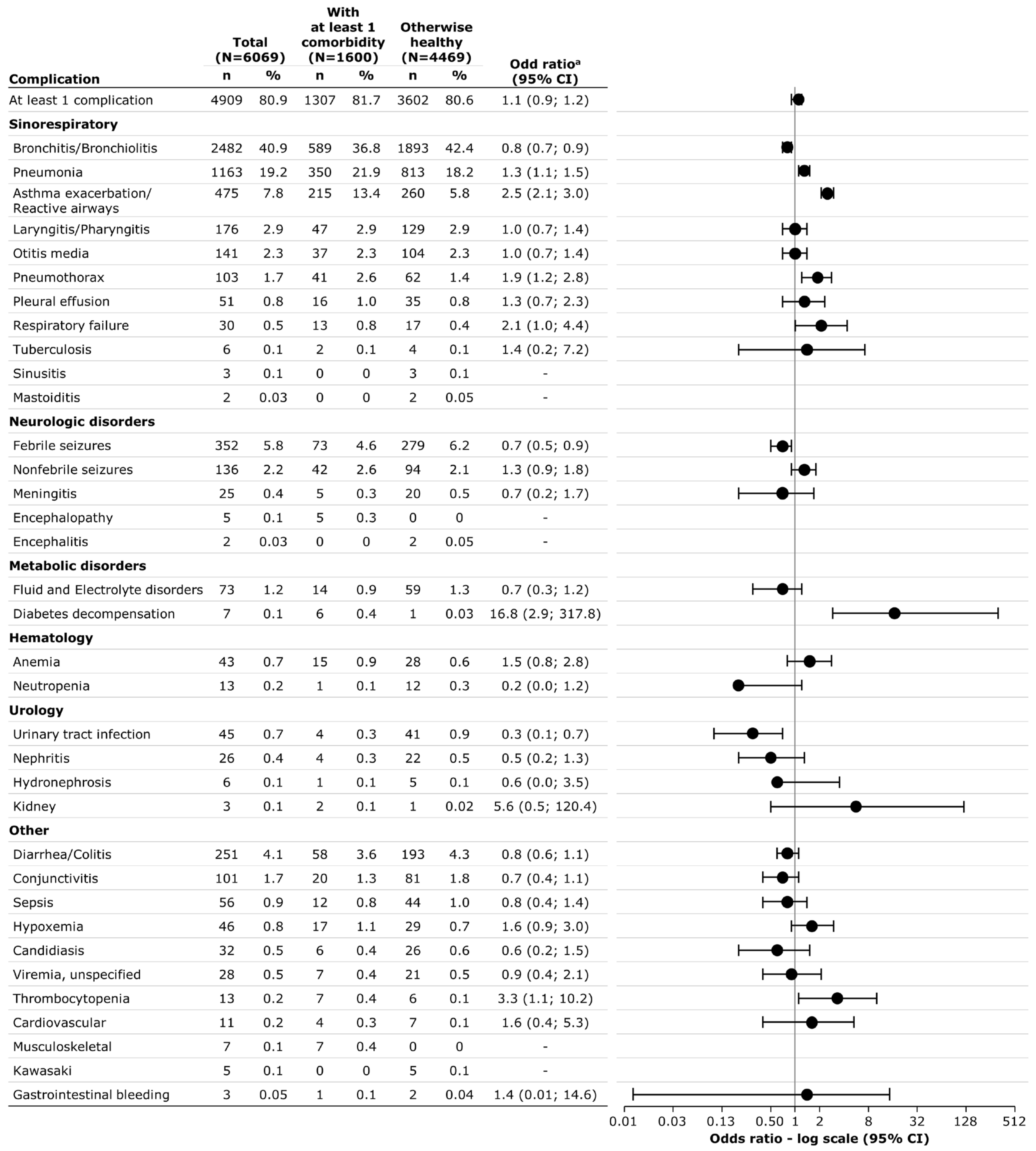
In total, 4909 patients (80.9%) had at least one complication associated with their respiratory illness hospitalization. This proportion was similar between patients with and without comorbidities. Overall and per presence of comorbidity, complications were mostly associated with sinorespiratory diagnoses. Pneumonia (21.9% vs. 18.2%), asthma exacerbation/reactive airways (13.4% vs. 5.8%), pneumothorax (2.6% vs. 1.4%), diabetes decompensation (0.4% vs.0.03%), thrombocytopenia (0.4% vs. 0.1%), and musculoskeletal diagnosis (0.4% vs. 0%) were significantly more frequently reported among those with comorbidity than those without, whereas bronchitis/bronchiolitis (42.4% vs. 36.8%), febrile seizures (6.2% vs. 4.6%), and urinary tract infections (0.9% vs. 0.3%) were more often reported among those otherwise healthy (Figure 2). Overall, the median length of hospitalization was 4 days (IQR: 3–6). Very few patients were admitted to the ICU (n = 78, 1.3%) or required mechanical ventilation (n = 21, 0.6%). No patient died during hospitalization. Children with comorbidities were more often admitted to the ICU (2.3% vs. 1.0%), but there was no significant difference regarding the need for mechanical ventilation (1.0% vs. 0.4%), and the length of stay in the hospital did not differ by presence of comorbidity (Table 2).
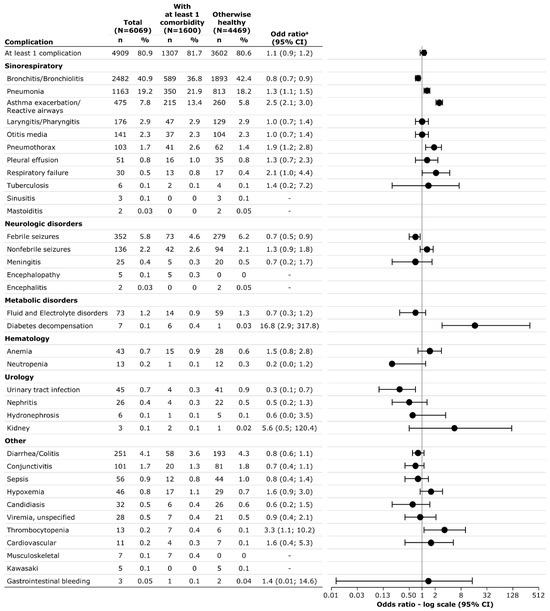
Figure 2.
Complications by presence of comorbidity. a Odd ratio for complication when presenting at least one underlying conditions at admission (otherwise healthy as reference). Abbreviation: CI, confidence interval.
Table 2.
Severity of patients by presence of comorbidities.
3.3. Impact of Comorbidities Associated with Selected Viral Pathogens
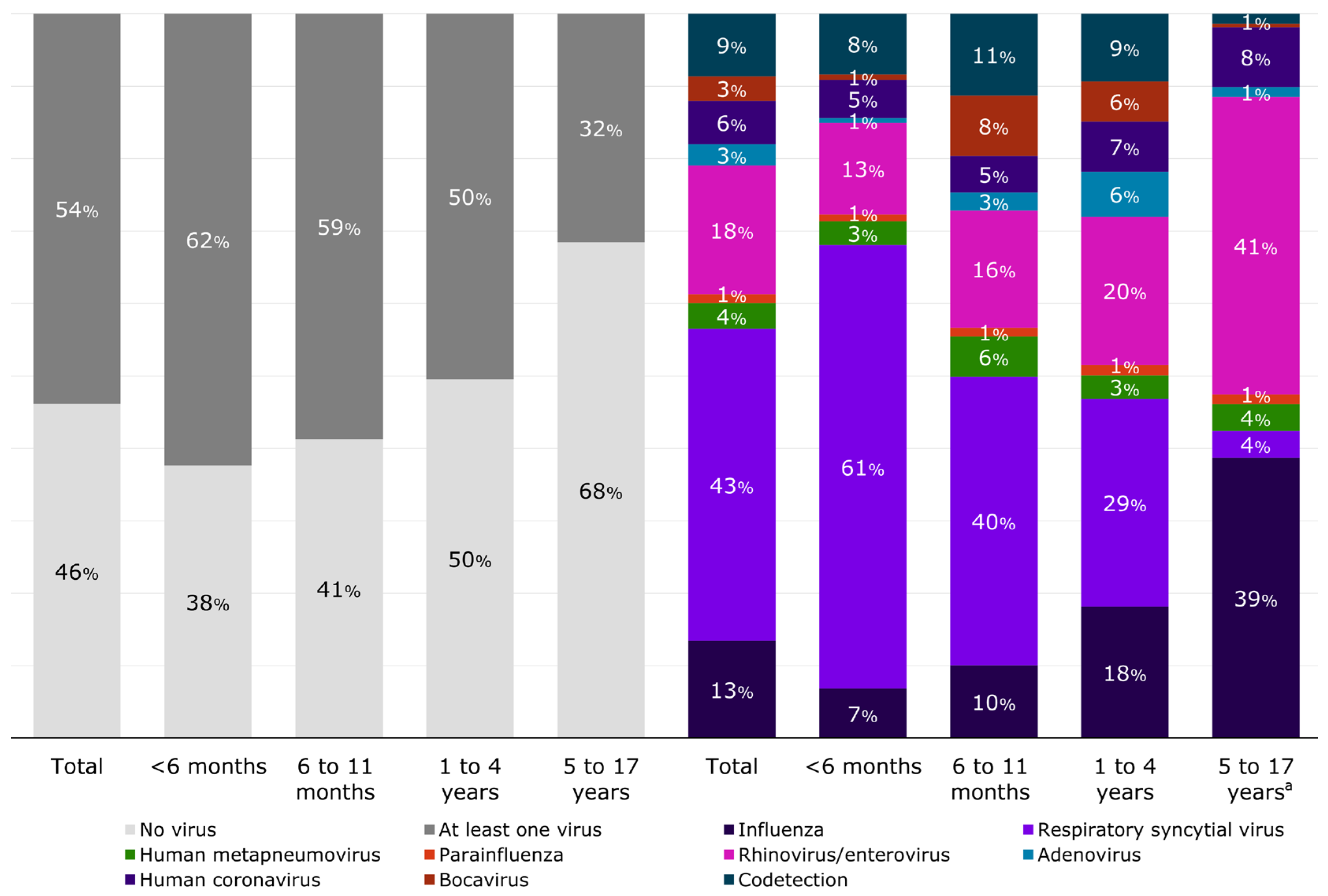
In total, 46% of patients (n = 2790) had no respiratory virus detected by RT-PCR (based on the viral panel used, Table 3), with a slightly higher proportion of negatives among patients without comorbidities compared to those with (50.0% vs. 44.5%, Supplementary Table S5). In general, the most frequently detected viruses were RSV (23.1%), followed by rhinovirus/enterovirus (9.5%) and influenza (7.2%). RSV was detected in a slightly higher proportion among patients without comorbidity than those with (24.3% vs. 19.8%, respectively, Supplementary Table S5), but there was no other pattern observed among virus-specific detection by comorbidity. Codetection corresponded to 4.6% of the patients and was more frequent in patients without comorbidity than in the patients with comorbidities (5.1% vs. 3.3%, Supplementary Table S5). The percentage of codetection was 5.2% among those <6 months, 6.7% among 6–11 months, 4.7% among 1–4 years, and 0.4% among those 5–17 years (Supplementary Table S6). Most of the codetections observed were between RSV and rhinovirus/enterovirus, RSV and human seasonal coronavirus, and RSV and bocavirus, with few detections including more than two different viruses (Supplementary Table S7). RSV was the most frequently detected virus among those <1 year of age whereas rhinovirus/enterovirus and influenza were the most frequent viral pathogen among school-aged children (i.e., 5 to 17 years—Figure 3 and Supplementary Table S6).
Table 3.
RT-PCR results compared to most commonly identified pathogens by ICD code.
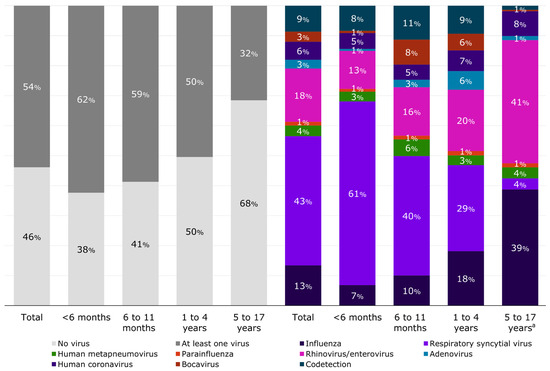
Figure 3.
Distribution of respiratory viral pathogens detected by RT-PCR by age group. a Bocavirus represents 0.5% of the detected viruses in this age group. Influenza includes influenza A(H1N1)pdm09, influenza A(H3N2), influenza B/Yamagata-lineage, influenza B/Victoria-lineage, and influenza not subtyped or with no lineage.
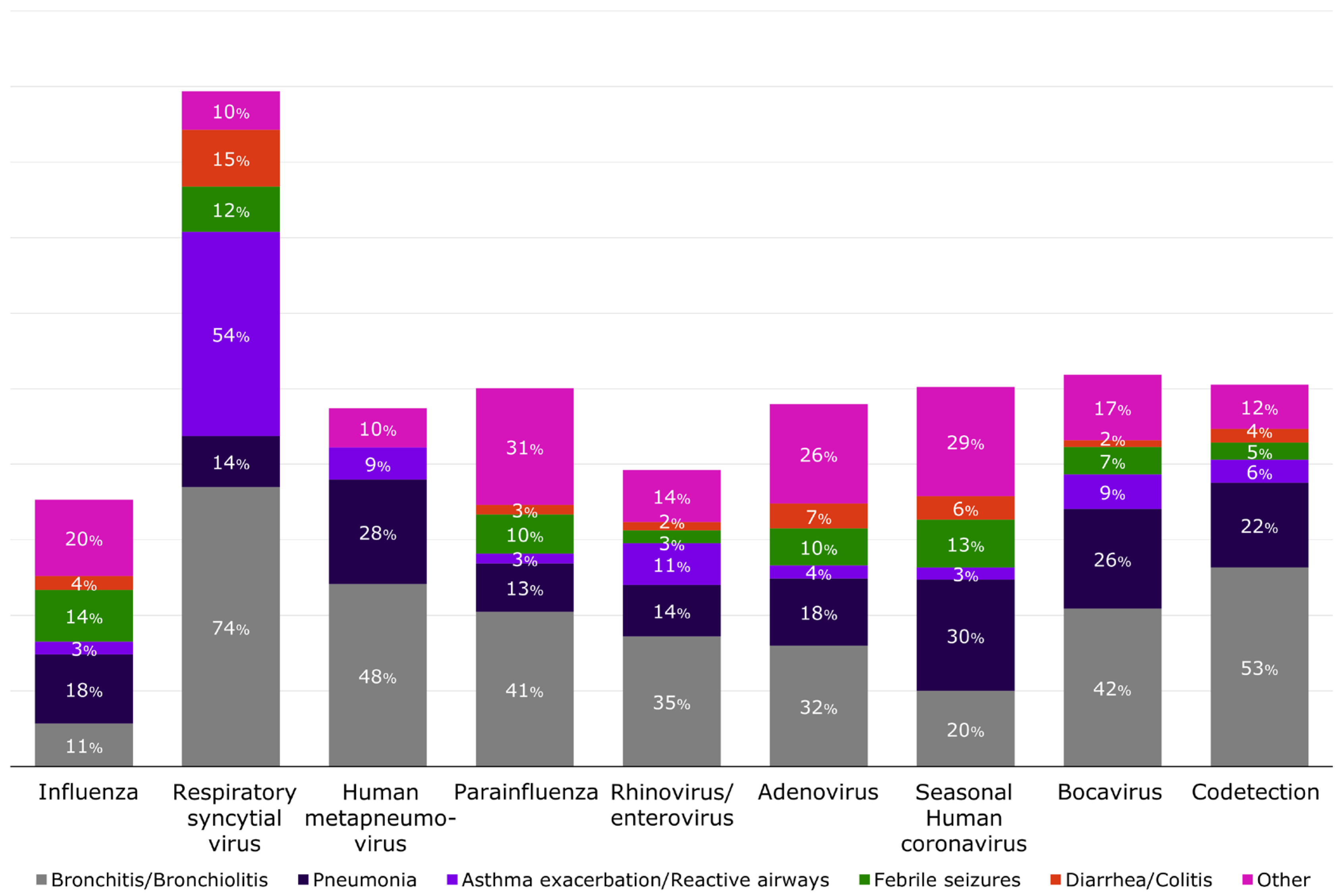
Complications by virus varied substantially, as can be seen in Figure 4, with laboratory-confirmed RSV patients mostly presenting with bronchitis/bronchiolitis (74%). Bronchitis/bronchiolitis was also present among cases with human metapneumovirus, parainfluenza, and bocavirus (>40% of cases) and in >50% of those with codetection. The most frequent complications identified among children with laboratory-confirmed influenza were pneumonia (18.3%), febrile seizures (13.7%), and bronchitis/bronchiolitis (11%). Among patients with no respiratory viruses detected by RT-PCR, the most commonly identified complications were also bronchitis/bronchiolitis (30%) and pneumonia (22.1%), with no differences by presence of comorbidity (Supplementary Table S8).
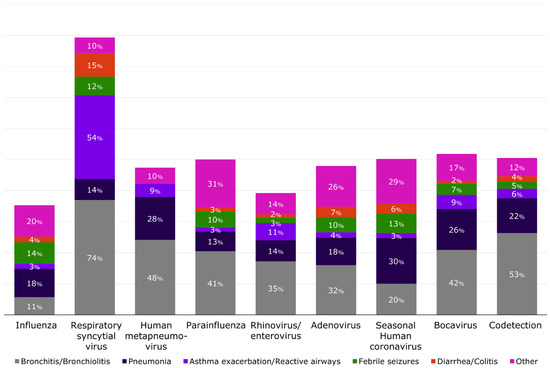
Figure 4.
Distribution of selected complications by respiratory viral pathogens detected by RT-PCR, Valencia, Spain 2011/12 through 2018/19. Complications were not mutually exclusive, and the same patient may have developed more than one complication. Influenza includes influenza A(H1N1)pdm09, influenza A(H3N2), influenza B/Yamagata-lineage, influenza B/Victoria-lineage, and influenza not subtyped or with no lineage.
Based on ICD discharge diagnoses, 25.8% ([6069 − 4505]/6069) of patients had a pathogen-specific code (Table 3). The most frequent pathogens coded were RSV (18%) and influenza (4%). No difference was observed between the two groups of patients with and without comorbidities, except for RSV, which was coded in a higher proportion in patients without comorbidity than in patients with comorbidities (19.6% vs. 13.6%). There was a small number of other specific etiologies coded at discharge associated with a variety of pathogens including pneumococcus pneumonia and meningitis, Hemophilus influenzae, rotavirus, and measles (Supplementary Table S9). Overall, 58.9% of RSV and 75.2% of influenza ICD coded cases were confirmed by multiplex RT-PCR conducted as part of our prospective study. Almost 22% ([1402 − 1093]/1402) of laboratory-confirmed RSV cases were missed when considering the ICD codes only. For influenza, 42.3% ([437 − 246]/437) of the laboratory-confirmed influenza cases were missed when considering the ICD codes used. Approximately 20% of patients with ICD codes for Streptococcal pneumoniae and Hemophilus influenzae had multiplex RT-PCR positive for RSV (Table 3).
4. Discussion
In our dataset, most (~75%) of the respiratory-associated hospitalizations were among otherwise healthy children. Nonetheless, children with comorbidities were twice as likely to be admitted to the ICU, even though we did not find differences in other severity markers like mechanical ventilation, death, or LOS by presence of comorbidity. Overall, 80% of children had complications associated with their respiratory illness, and the distribution of certain complications varied by presence of comorbidity. For instance, pneumonia and pneumothorax were more often diagnosed among children with comorbidity. Asthma exacerbation/reactive airways and diabetes decompensation are also a reminder that respiratory illness can trigger the worsening of chronic conditions in children. Nonetheless, our findings corroborate the healthcare burden associated with these infections among children who were otherwise healthy, suggesting that preventive interventions targeting only children with comorbidities would have a lesser impact on reducing healthcare utilization associated with respiratory illnesses.
The role of respiratory viruses on child morbidity and mortality is well-documented [1,2,27,28,29]. More recently, considering the frequency of respiratory viral cocirculation, the association between disease severity and the codetection of respiratory pathogens have been further explored. A study among children <15 years hospitalized with acute respiratory illness described those with viral codetection being more than five times as likely to be admitted to the ICU [30]. Codetection has also been identified as a risk factor for complications among children <5 years hospitalized with COVID-19, where a higher frequency of oxygen support and ICU admissions were described, even after adjusting for the presence of comorbidities [31]. Another study that focused on hospitalized infants with RSV described frequent pathogen codetection with rhinovirus, seasonal coronavirus, Streptococcus, and Hemophilus species, emphasizing the strong contribution of codetection, with Hemophilus being associated with higher overall severity (based on their own severity score) [32]. We did not find any association between codetection and severity in our analysis, which could be due to the small sample size and/or differences in the underlying characteristics of the population or access to care. Moreover, data on pathogens derived from ICD codes are less reliable than medical notes and the direct ascertainment of laboratory test results. The availability of viral diagnostic tools to improve the identification of respiratory illness etiology could become routine care, as this may contribute to improving infection control recommendations, the management of at risk patients, and guide patient care related to therapeutics (antivirals, monoclonal, antibiotics therapy). This may also help reduce pediatric antibiotic use and prevent the spread of antibiotic resistance, especially if these interventions are targeted in children with chronic conditions who may be more likely to be prescribed antibiotics [33,34,35].
Exploring other viral etiologies may be important to further understand their contribution to the burden of respiratory hospitalizations in pediatric populations. For instance, human parechovirus has been described as an important cause of disease in neonates and young children and can lead to fever, sepsis-like syndrome, and/or neurologic illness (seizures, meningitis), which can be difficult to distinguish from other respiratory infections in very young infants [36]. Enterovirus D68 (EVD-68) has also been associated with increased hospitalizations among young children presenting with severe bronchiolitis [37]. EVD-68 targets are not in commercial laboratory tests and were not part of our multiplex. Nonetheless, children with EVD-68 are often detected among those testing positive for rhinovirus/enterovirus, which were the second most detected viruses in our study population, even though our surveillance period focused on the colder months of the year and likely missed rhinovirus/enterovirus circulating during the spring or summer [38,39]. The European Center for Disease Prevention and Control (ECDC) and the World Health Organization (WHO) have recently emphasized the importance of integrated surveillance for influenza, RSV, COVID-19, and potentially other respiratory viruses [40], with year-round monitoring that could inform clinical and public health practices as point-of-care testing may be resource intense.
Influenza is prevented by vaccination in those as young as 6 months of age or through the vaccination of pregnant people to protect those <6 months [41,42]. However, the use of influenza vaccines is limited among young children in many countries, including Spain where policy currently only targets those with comorbidities and the elderly [43]. Our data showed that many children hospitalized with respiratory illness and related complications were otherwise healthy. Studies have suggested that the prevention of influenza through the vaccination of children can reduce influenza-associated hospitalizations in older adults [44], and the spread of influenza in the community [45,46], potentially reducing overall healthcare utilization.
As described in other studies in high income countries [9,47,48], we found RSV to be the most commonly detected viral pathogen in our young children population, being associated with almost a quarter of hospitalizations. The majority of laboratory-confirmed RSV patients had no underlying condition, and the median age of hospitalizations was 2 months. Hospitalization represents just a fraction of all RSV-related healthcare visits and the burden of RSV on primary care is large [47,48]. Long-acting monoclonal antibodies and/or mother/baby vaccination have been approved for use in Europe and the USA and can provide protection from RSV complications including hospitalizations [49,50,51,52,53,54], aiding in reducing the healthcare burden associated with RSV, as influenza and COVID-19 vaccines are already available tools [55].
Our study had several limitations. Despite the large dataset, severe outcomes or some underlying conditions were rare among this pediatric population, reducing our analytical power. Each year, the period of surveillance was defined around the influenza season, which differ from other respiratory viruses, with variations from year to year. We may have underestimated the contribution of some respiratory viruses because we did not document the year-round circulation and because the multiplex RT-PCR we used had limited viral targets. Moreover, the identification of complications among children hospitalized in our study relied on ICD-9 and ICD-10 codes taken from medical records. Some complications may have been missed, since only three codes were collected per patient. The ICD code groupings developed for this analysis have not been previously validated and may misclassify diseases or outcomes, as we documented when comparing coded pathogens from medical records with the multiplex RT-PCR results. Nonetheless, similar analytical approaches to explore complications have been previously published [56,57].
5. Conclusions
In conclusion, our study confirms that comorbidities in children with respiratory illnesses significantly increase the risk of complications and are associated with higher ICU admission rates. However, healthcare utilization is largely driven by otherwise healthy children who can also develop severe complications requiring hospitalization. The contribution of respiratory viruses to healthcare surges during the cold months should be acknowledged when planning interventions for this population. Cost–benefit analyses, considering current vaccination strategies and the potential impact of new respiratory-targeted vaccines, are warranted. Additionally, increased use of point-of-care diagnostic tests and expanded surveillance for respiratory viruses could inform new policies for the prevention and management of pediatric respiratory hospitalizations as well as support research and the development of new vaccines in this field.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/v16101519/s1, Table S1: International Classification of Diseases (ICD) codes used to classify complications; Table S2: International Classification of Diseases (ICD) codes by comorbidity; Table S3: Correspondence between comorbidities identified directly from medical charts and those from ICD discharge codes combined for the analysis; Table S4: International Classification of Diseases (ICD) codes by pathogens; Table S5: Viral pathogens detected by RT-PCR assays by presence of comorbidity; Table S6: RT-PCR results per age group; Table S7: Codetections detected by RT-PCR assays; Table S8: Selected complications by viral pathogens detected by RT-PCR assays; Table S9: Most frequent pathogens identified in ICD codes by presence of comorbidity.
Author Contributions
All authors contributed to the study conception and the interpretation of the data, and all participated in the drafting and critical revision of this report. All authors read and approved the final version and are accountable for its accuracy and integrity. V.B.C. conducted the analysis and wrote the first draft of the manuscript under the supervision of S.S.C. All authors have read and agreed to the published version of the manuscript.
Funding
This study was partly funded by Sanofi, the Fondation de France, FISABIO-Public Health and CIBER-ESP.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Research Committee of the Dirección General de Salud Pública—Centro Superior de Investigación en Salud Pública (DGSP-CSISP) on the 3 August 2011.
Informed Consent Statement
Informed consent was obtained from all subjects/parents/legal tutors involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the authors upon reasonable request and with the permission of FISABIO-Public Health. Please contact Ainara Mira-Iglesias (ainara.mira@fisabio.es).
Acknowledgments
The authors thank the staff at the Hospital General Universitario de Castellón in Castellón; La Plana in Vila-real; Hospital Universitario y Politécnico La Fe in Valencia; Hospital Universitario Dr Peset in Valencia; Hospital de La Ribera in Alzira; Hospital de San Juan in Alicante; Hospital General de Alicante in Alicante; Hospital General de Elda in Elda, and Hospital del Vinalopó in Elche, for their support. We thank all of the study participants and their families for their support and contribution to the Valencia Hospital Network for the Study of Influenza and Other Respiratory Viruses Disease (VAHNSI) network.
Conflicts of Interest
V.B.C. and S.S.C. are employees of Sanofi and may hold shares and/or stock options in the company. A.M.-I. has received fees for conferences/experts’ meetings from Sanofi, and for educational events from Merck Sharp & Dohme (MSD). J.D.-D. has attended several congresses whose registration, travel, and accommodation costs were covered by MSD, GlaxoSmithKline (GSK), and Sanofi. J.D.-D. and his institution received research grants from Sanofi and GSK related to respiratory syncytial virus preventive strategies. J.D.-D. has acted as an advisor for these immunization strategies for Sanofi. F.X.L.-L., B.M.-C., M.C.-F., M.T.-G., J.M.-M. and J.P.-B. declare no conflicts of interest.
References
- Collaborators GLRI. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory tract infections in 195 countries: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Infect. Dis. 2017, 17, 1133–1161. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Williams, D.J.; Arnold, S.R.; Ampofo, K.; Bramley, A.M.; Reed, C.; Stockmann, C.; Anderson, E.J.; Grijalva, C.G.; Self, W.H.; et al. Community-acquired pneumonia requiring hospitalization among U.S. children. N. Engl. J. Med. 2015, 372, 835–845. [Google Scholar] [CrossRef] [PubMed]
- Derqui, N.; Nealon, J.; Mira-Iglesias, A.; Díez-Domingo, J.; Mahé, C.; Chaves, S.S. Predictors of influenza severity among hospitalized adults with laboratory confirmed influenza: Analysis of nine influenza seasons from the Valencia region, Spain. Influenza Other Respir. Viruses 2022, 16, 862–872. [Google Scholar] [CrossRef] [PubMed]
- Simon, T.D.; Mahant, S.; Cohen, E. Pediatric Hospital Medicine and Children with Medical Complexity: Past, Present, and Future. Curr. Probl. Pediatr. Adolesc. Health Care 2012, 42, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Keren, R. Flu-related hospitalization in children. LDI Issue Brief 2006, 12, 1–4. [Google Scholar] [PubMed]
- American Academy of Pediatrics Committee on Infectious Diseases; American Academy of Pediatrics Bronchiolitis Guidelines Committee. Updated guidance for palivizumab prophylaxis among infants and young children at increased risk of hospitalization for respiratory syncytial virus infection. Pediatrics 2014, 134, e620–e638. [Google Scholar] [CrossRef]
- Gov.UK. Available online: https://www.gov.uk/government/publications/covid-19-vaccination-resources-for-children-aged-5-to-11-years (accessed on 28 March 2022).
- Rha, B.; Curns, A.T.; Lively, J.Y.; Campbell, A.P.; Englund, J.A.; Boom, J.A.; Azimi, P.H.; Weinberg, G.A.; Staat, M.A.; Selvarangan, R.; et al. Respiratory Syncytial Virus-Associated Hospitalizations Among Young Children: 2015–2016. Pediatrics 2020, 146, e20193611. [Google Scholar] [CrossRef]
- Arriola, C.S.; Kim, L.; Langley, G.; Anderson, E.J.; Openo, K.; Martin, A.M.; Lynfield, R.; Bye, E.; Como-Sabetti, K.; Reingold, A.; et al. Estimated Burden of Community-Onset Respiratory Syncytial Virus–Associated Hospitalizations among Children Aged <2 Years in the United States, 2014–2015. J. Pediatr. Infect. Dis. Soc. 2020, 9, 587–595. [Google Scholar] [CrossRef]
- Hall, C.B.; Weinberg, G.A.; Blumkin, A.K.; Edwards, K.M.; Staat, M.A.; Schultz, A.F.; Poehling, K.A.; Szilagyi, P.G.; Griffin, M.R.; Williams, J.V.; et al. Respiratory Syncytial Virus–Associated Hospitalizations Among Children Less Than 24 Months of Age. Pediatrics 2013, 132, e341–e348. [Google Scholar] [CrossRef]
- Hauge, S.H.; Bakken, I.J.; de Blasio, B.F.; Håberg, S.E. Risk conditions in children hospitalized with influenza in Norway, 2017–2019. BMC Infect. Dis. 2020, 20, 769. [Google Scholar] [CrossRef]
- Tsankov, B.K.; Allaire, J.M.; Irvine, M.A.; Lopez, A.A.; Sauvé, L.J.; Vallance, B.A.; Jacobson, K. Severe COVID-19 Infection and Pediatric Comorbidities: A Systematic Review and Meta-Analysis. Int. J. Infect. Dis. 2021, 103, 246–256. [Google Scholar] [CrossRef] [PubMed]
- Farrar, D.S.; Drouin, O.; Hepburn, C.M.; Baerg, K.; Chan, K.; Cyr, C.; Donner, E.J.; Embree, J.E.; Farrell, C.; Forgie, S.; et al. Risk factors for severe COVID-19 in hospitalized children in Canada: A national prospective study from March 2020–May 2021. Lancet Reg. Health Am. 2022, 15, 100337. [Google Scholar] [CrossRef] [PubMed]
- Neuzil, K.M.; Mellen, B.G.; Wright, P.F.; Mitchel, E.F.J.; Griffin, M.R. The Effect of Influenza on Hospitalizations, Outpatient Visits, and Courses of Antibiotics in Children. N. Engl. J. Med. 2000, 342, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Demont, C.; Petrica, N.; Bardoulat, I.; Duret, S.; Watier, L.; Chosidow, A.; Lorrot, M.; Kieffer, A.; Lemaitre, M. Economic and disease burden of RSV-associated hospitalizations in young children in France, from 2010 through 2018. BMC Infect. Dis. 2021, 21, 730. [Google Scholar] [CrossRef]
- Zipkin, M. New Vaccine Approaches Present New Possibilities, But New Challenges. Nat. Biopharma Deal. Mak. News Feature 2021. [Google Scholar] [CrossRef]
- Focosi, D. From Co-Administration to Co-Formulation: The Race for New Vaccines against COVID-19 and Other Respiratory Viruses. Vaccines 2023, 11, 109. [Google Scholar] [CrossRef]
- Belshe, R.B.; Newman, F.K.; Anderson, E.L.; Wright, P.F.; Karron, R.A.; Tollefson, S.; Henderson, F.W.; Meissner, H.C.; Madhi, S.; Roberton, D.; et al. Evaluation of Combined Live, Attenuated Respiratory Syncytial Virus and Parainfluenza 3 Virus Vaccines in Infants and Young Children. J. Infect. Dis. 2004, 190, 2096–2103. [Google Scholar] [CrossRef]
- Puig-Barberà, J.; Tormos, A.; Sominina, A.; Burtseva, E.; Launay, O.; Ciblak, M.A.; Natividad-Sancho, A.; Buigues-Vila, A.; Martínez-Úbeda, S.; Mahé, C. First-year results of the Global Influenza Hospital Surveillance Network: 2012–2013 Northern hemisphere influenza season. BMC Public Health 2014, 14, 564. [Google Scholar] [CrossRef]
- Puig-Barberà, J.; Tormos, A.; Trushakova, S.; Sominina, A.; Pisareva, M.; Ciblak, M.A.; Badur, S.; Yu, H.; Cowling, B.J.; Burtseva, E.; et al. The Global Influenza Hospital Surveillance Network (GIHSN): A new platform to describe the epidemiology of severe influenza. Influ. Other Respir. Viruses 2015, 9, 277–286. [Google Scholar] [CrossRef]
- Mira-Iglesias, A.; López-Labrador, F.X.; García-Rubio, J.; Mengual-Chuliá, B.; Tortajada-Girbés, M.; Mollar-Maseres, J.; Carballido-Fernández, M.; Schwarz-Chavarri, G.; Puig-Barberà, J.; Díez-Domingo, J. Influenza Vaccine Effectiveness and Waning Effect in Hospitalized Older Adults. Valencia Region, Spain, 2018/2019 Season. Int. J. Environ. Res. Public Health 2021, 18, 1129. [Google Scholar] [CrossRef]
- Mira-Iglesias, A.; López-Labrador, F.X.; Baselga-Moreno, V.; Tortajada-Girbés, M.; Mollar-Maseres, J.; Carballido-Fernández, M.; Schwarz-Chavarri, G.; Puig-Barberà, J.; Díez-Domingo, J. Influenza vaccine effectiveness against laboratory-confirmed influenza in hospitalised adults aged 60 years or older, Valencia Region, Spain, 2017/18 influenza season. Euro Surveill. 2019, 24. [Google Scholar] [CrossRef] [PubMed]
- Mira-Iglesias, A.; López-Labrador, F.X.; Guglieri-López, B.; Tortajada-Girbés, M.; Baselga-Moreno, V.; Cano, L.; Mollar-Maseres, J.; Carballido-Fernández, M.; Schwarz-Chavarri, G.; Díez-Domingo, J.; et al. Influenza vaccine effectiveness in preventing hospitalisa-tion of individuals 60 years of age and over with laboratory-confirmed influenza, Valencia Region, Spain, influenza season 2016/17. Euro Surveill 2018, 23. [Google Scholar] [CrossRef] [PubMed]
- Cohen, P.R.; Rybak, A.; Werner, A.; Béchet, S.; Desandes, R.; Hassid, F.; André, J.M.; Gelbert, N.; Thiebault, G.; Kochert, F.; et al. Trends in pediatric ambulatory community acquired infections before and during COVID-19 pandemic: A prospective multicentric sur-veillance study in France. Lancet Reg. Health Eur. 2022, 22, 100497. [Google Scholar] [CrossRef] [PubMed]
- Baker, R.E.; Park, S.W.; Yang, W.; Vecchi, G.A.; Metcalf, C.J.E.; Grenfell, B.T. The impact of COVID-19 nonpharmaceutical interventions on the future dynamics of endemic infections. Proc. Natl. Acad. Sci. USA 2020, 117, 30547–30553. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Commission Implementing Decision (EU) 2018/945 of 22 June 2018 on the Communicable Diseases and Related Health Issues to Be Covered by Epidemiological Surveillance As Well As Relevant Case Definitions; European Centre for Disease Prevention and Control: Solna, Sweden, 2018; Volume 1–74, Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32018D0945 (accessed on 1 July 2024).
- Thompson, M.G.; Levine, M.Z.; Bino, S.; Hunt, D.R.; Al-Sanouri, T.M.; Simões, E.A.F.; Porter, R.M.; Biggs, H.M.; Gresh, L.; Simaku, A.; et al. Underdetection of laboratory-confirmed influenza-associated hospital admissions among infants: A multicentre, prospective study. Lancet Child Adolesc. Health 2019, 3, 781–794. [Google Scholar] [CrossRef] [PubMed]
- Norman, D.A.; Cheng, A.C.; Macartney, K.K.; Moore, H.C.; Danchin, M.; Seale, H.; McRae, J.; Clark, J.E.; Marshall, H.S.; Buttery, J.; et al. Influenza hospitalizations in Australian children 2010-2019: The impact of medical comorbidities on outcomes, vaccine coverage, and effectiveness. Influenza Other Respir Viruses 2022, 16, 316–327. [Google Scholar] [CrossRef]
- Sarna, M.; Lambert, S.B.; Sloots, T.P.; Whiley, D.M.; Alsaleh, A.; Mhango, L.; Bialasiewicz, S.; Wang, D.; Nissen, M.D.; Grimwood, K.; et al. Viruses causing lower respiratory symptoms in young children: Findings from the ORChID birth cohort. Thorax 2017, 73, 969–979. [Google Scholar] [CrossRef]
- Le Corre, N.; Pérez, R.; Vizcaya, C.; Martínez-Valdebenito, C.; López, T.; Monge, M.; Alarcón, R.; Moller, F.; Martínez, M.T.; Massardo, J.M.; et al. Relevance of codetection of respiratory viruses in the severity of acute respiratory infection in hospitalized children. Andes Pediatr. 2021, 92, 349–357. [Google Scholar] [CrossRef]
- Agathis, N.T.; Patel, K.; Milucky, J.; Taylor, C.A.; Whitaker, M.; Pham, H.; Anglin, O.; Chai, S.J.; Alden, N.B.; Meek, J.; et al. Codetections of Other Respiratory Viruses Among Children Hospitalized with COVID-19. Pediatrics 2023, 151. [Google Scholar] [CrossRef]
- Lin, G.-L.; Drysdale, S.; Snape, M.; O’Connor, D.; Brown, A.; MacIntyre-Cockett, G.; Mellado-Gomez, E.; de Cesare, M.; Ansari, A.; Bonsall, D.; et al. Association between disease severity and co-detection of respiratory pathogens in infants with RSV infection. medRxiv 2023. [Google Scholar] [CrossRef]
- Samson, L.; Cooke, C.; MacDonald, N. Analysis of antibiotic use and misuse in children hospitalized with RSV infection. Paediatr. Child Health 1999, 4, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Van Houten, C.B.; Cohen, A.; Engelhard, D.; Hays, J.P.; Karlsson, R.; Moore, E.; Fernández, D.; Kreisberg, R.; Collins, L.V.; de Waal, W.; et al. Antibiotic misuse in respiratory tract infections in children and adults—A prospective, multicentre study (TAILORED Treatment). Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 505–514. [Google Scholar] [CrossRef] [PubMed]
- Han, S.B.; Shin, J.A.; Kim, S.K.; Lee, J.W.; Lee, D.-G.; Chung, N.-G.; Cho, B.; Jeong, D.C.; Kang, J.H. Respiratory viral infections in children and adolescents with hematological malignancies. Mediterr. J. Hematol. Infect. Dis. 2019, 11, e2019006. [Google Scholar] [CrossRef] [PubMed]
- Britton, P.N.; Jones, C.A.; Macartney, K.; Cheng, A.C. Parechovirus: An important emerging infection in young infants. Med. J. Aust. 2018, 208, 365–369. [Google Scholar] [CrossRef]
- Shah, M.M.; Perez, A.; Lively, J.Y.; Avadhanula, V.; Boom, J.A.; Chappell, J.; Englund, J.A.; Fregoe, W.; Halasa, N.B.; Harrison, C.J.; et al. Enterovirus D68-Associated Acute Respiratory Illness—New Vaccine Surveillance Network, United States, July–November 2018–2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1623–1628. [Google Scholar] [CrossRef]
- Monto, A.S. The seasonality of rhinovirus infections and its implications for clinical recognition. Clin. Ther. 2002, 24, 1987–1997. [Google Scholar] [CrossRef]
- Pons-Salort, M.; Oberste, M.S.; Pallansch, M.A.; Abedi, G.R.; Takahashi, S.; Grenfell, B.T.; Grassly, N.C. The seasonality of nonpolio enteroviruses in the United States: Patterns and drivers. Proc. Natl. Acad. Sci. USA 2018, 115, 3078–3083. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control; World Health Organization. Operational Considerations for Respiratory Virus Surveillance in Europe, 18 July 2022. WHO/EURO:2022-5841-45606-65427. 2022. Available online: https://www.who.int/europe/publications/i/item/WHO-EURO-2022-5841-45606-65427 (accessed on 1 July 2024).
- Fiore, A.E.; Uyeki, T.M.; Broder, K.; Finelli, L.; Euler, G.L.; Singleton, J.A.; Iskander, J.K.; Wortley, P.M.; Shay, D.K.; Bresee, J.S.; et al. Prevention and control of influenza with vaccines: Recommendations of the Advisory Committee on Immunization Practices (ACIP), 2010. MMWR Recomm. Rep. 2010, 59, 1–62. [Google Scholar]
- Mak, T.K.; Mangtani, P.; Leese, J.; Watson, J.M.; Pfeifer, D. Influenza vaccination in pregnancy: Current evidence and selected national policies. Lancet Infect. Dis. 2008, 8, 44–52. [Google Scholar] [CrossRef]
- Morales, K.F.; Brown, D.W.; Dumolard, L.; Steulet, C.; Vilajeliu, A.; Alvarez, A.M.R.; Moen, A.; Friede, M.; Lambach, P. Seasonal influenza vaccination policies in the 194 WHO Member States: The evolution of global influenza pandemic preparedness and the challenge of sustaining equitable vaccine access. Vaccine X 2021, 8, 100097. [Google Scholar] [CrossRef]
- Cohen, S.A.; Chui, K.K.; Naumova, E.N. Influenza Vaccination in Young Children Reduces Influenza-Associated Hospitalizations in Older Adults, 2002–2006. J. Am. Geriatr. Soc. 2011, 59, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Dbaibo, G.; Amanullah, A.; Claeys, C.; Izu, A.; Jain, V.K.; Kosalaraksa, P.; Rivera, L.; Soni, J.; Yanni, E.; Zaman, K.; et al. Quadrivalent Influenza Vaccine Prevents Illness and Reduces Healthcare Utilization Across Diverse Geographic Regions During Five Influenza Seasons: A Randomized Clinical Trial. Pediatr. Infect Dis. J. 2020, 39, e1–e10. [Google Scholar] [CrossRef] [PubMed]
- King, J.C.J.; Stoddard, J.J.; Gaglani, M.J.; Moore, K.A.; Magder, L.; McClure, E.; Rubin, J.D.; Englund, J.A.; Neuzil, K. Effectiveness of School-Based Influenza Vaccination. N. Engl. J. Med. 2006, 355, 2523–2532. [Google Scholar] [CrossRef] [PubMed]
- Gantenberg, J.R.; van Aalst, R.; Zimmerman, N.; Limone, B.; Chaves, S.S.; La Via, W.V.; Nelson, C.B.; Rizzo, C.; Savitz, D.A.; Zullo, A.R. Medically Attended Illness due to Respiratory Syncytial Virus Infection Among Infants Born in the United States Between 2016 and 2020. J. Infect. Dis. 2022, 226 (Suppl. S2), S164–S174. [Google Scholar] [CrossRef] [PubMed]
- Wildenbeest, J.G.; Billard, M.-N.; Zuurbier, R.P.; Korsten, K.; Langedijk, A.C.; van de Ven, P.M.; Snape, M.D.; Drysdale, S.B.; Pollard, A.J.; Robinson, H.; et al. The burden of respiratory syncytial virus in healthy term-born infants in Europe: A prospective birth cohort study. Lancet Respir. Med. 2022, 11, 341–353. [Google Scholar] [CrossRef]
- Domachowske, J.B.; Anderson, E.J.; Goldstein, M. The Future of Respiratory Syncytial Virus Disease Prevention and Treatment. Infect. Dis. Ther. 2021, 10 (Suppl. S1), 47–60. [Google Scholar] [CrossRef]
- Mazur, N.I.; Terstappen, J.; Baral, R.; Bardají, A.; Beutels, P.; Buchholz, U.J.; Cohen, C.; Crowe, J.E.; Cutland, C.L.; Eckert, L.; et al. Respiratory syncytial virus prevention within reach: The vaccine and monoclonal antibody landscape. Lancet Infect. Dis. 2023, in press. [Google Scholar] [CrossRef]
- Hammitt, L.L.; Dagan, R.; Yuan, Y.; Cots, M.B.; Bosheva, M.; Madhi, S.A.; Muller, W.J.; Zar, H.J.; Brooks, D.; Grenham, A.; et al. Nirsevimab for Prevention of RSV in Healthy Late-Preterm and Term Infants. N. Engl. J. Med. 2022, 386, 837–846. [Google Scholar] [CrossRef]
- Griffin, M.P.; Yuan, Y.; Takas, T.; Domachowske, J.B.; Madhi, S.A.; Manzoni, P.; Simões, E.A.F.; Esser, M.T.; Khan, A.A.; Dubovsky, F.; et al. Single-Dose Nirsevimab for Prevention of RSV in Preterm Infants. N. Engl. J. Med. 2020, 383, 415–425. [Google Scholar] [CrossRef]
- Simões, E.A.F.; Madhi, S.A.; Muller, W.J.; Atanasova, V.; Bosheva, M.; Cabañas, F.; Cots, M.B.; Domachowske, J.B.; Garcia-Garcia, M.L.; Grantina, I.; et al. Efficacy of nirsevimab against respiratory syncytial virus lower respiratory tract infections in preterm and term infants, and pharmacokinetic extrapolation to infants with congenital heart disease and chronic lung disease: A pooled analysis of randomised controlled trials. Lancet Child Adolesc. Health 2023, 7, 180–189. [Google Scholar] [CrossRef]
- Aliprantis, A.O.; Wolford, D.; Caro, L.; Maas, B.M.; Ma, H.; Montgomery, D.L.; Sterling, L.M.; Hunt, A.; Cox, K.S.; Vora, K.A.; et al. A Phase 1 Randomized, Double-Blind, Placebo-Controlled Trial to Assess the Safety, Tolerability, and Pharmacokinetics of a Respiratory Syncytial Virus Neutralizing Monoclonal Antibody MK-1654 in Healthy Adults. Clin. Pharmacol. Drug Dev. 2021, 10, 556–566. [Google Scholar] [CrossRef] [PubMed]
- Sah, P.; Vilches, T.N.; Pandey, A.; Schneider, E.C.; Moghadas, S.M.; Galvani, A.P. Estimating the impact of vaccination on reducing COVID-19 burden in the United States: December 2020 to March 2022. J. Glob. Health 2022, 12, 03062. [Google Scholar] [CrossRef] [PubMed]
- Dawood, F.S.; Chaves, S.S.; Pérez, A.; Reingold, A.; Meek, J.; Farley, M.M.; Ryan, P.; Lynfield, R.; Morin, C.; Baumbach, J.; et al. Emerging Infections Program Network. Complications and Associated Bacterial Coinfections Among Children Hospitalized with Seasonal or Pandemic Influenza, United States, 2003–2010. J. Infect. Dis. 2014, 209, 686–694. [Google Scholar] [CrossRef] [PubMed]
- Reed, C.; Chaves, S.S.; Perez, A.; D’Mello, T.; Kirley, P.D.; Aragon, D.; Meek, J.I.; Farley, M.M.; Ryan, P.; Lynfield, R.; et al. Complications Among Adults Hospitalized with Influenza: A Comparison of Seasonal Influenza and the 2009 H1N1 Pandemic. Clin. Infect. Dis. 2014, 59, 166–174. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).