
Impact of Nonpharmaceutical Interventions during the COVID-19 Pandemic on the Prevalence of Respiratory Syncytial Virus in Hospitalized Children with Lower Respiratory Tract Infections: A Systematic Review and Meta-Analysis

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
2.2. Data Analysis
3. Results
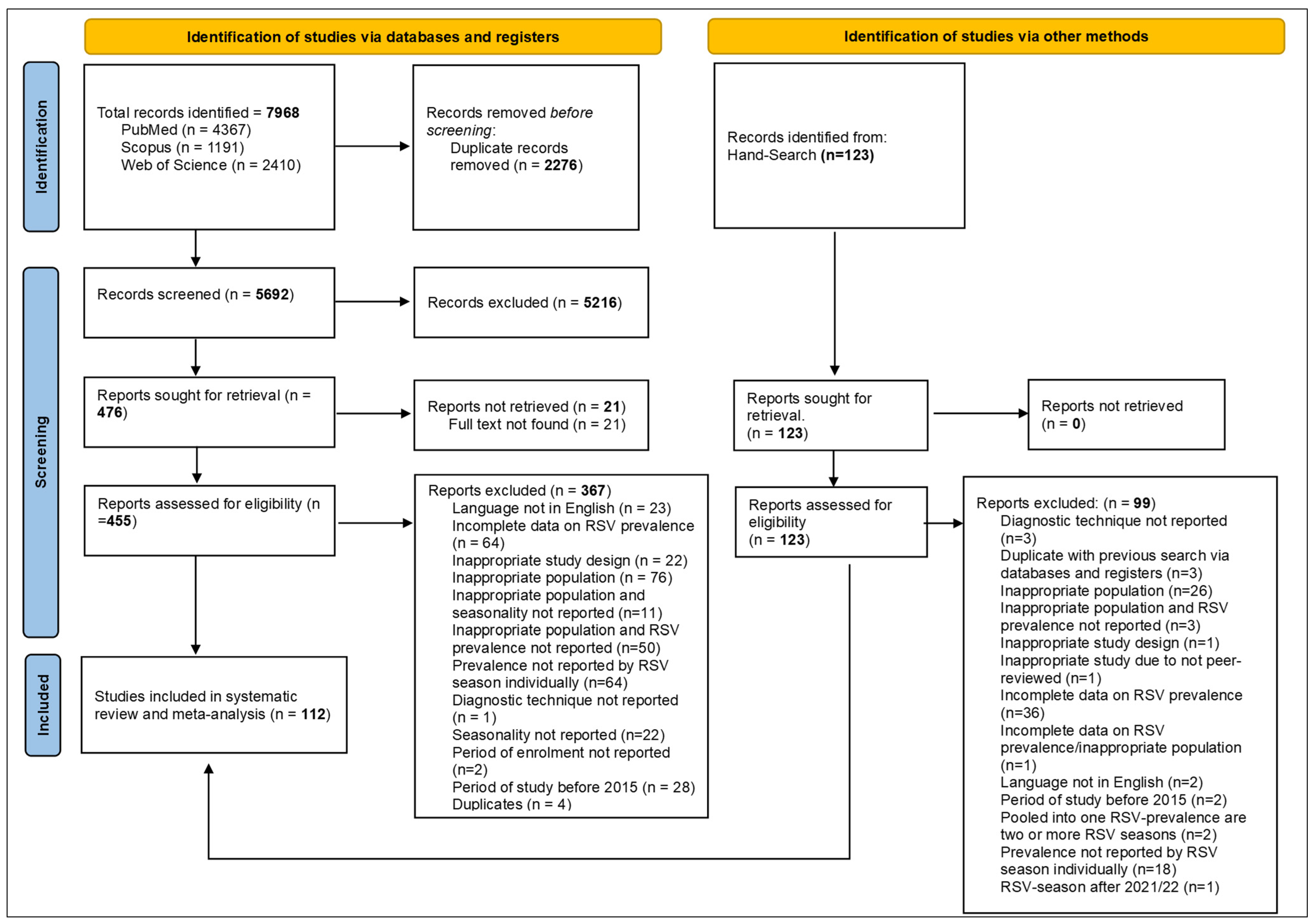
3.1. Search Results
3.2. Characteristics of the Included Articles
3.3. Subgroup Analysis
3.4. Sensitivity Analysis
3.5. Stratified Analysis by World Health Organizations Regions, Countries, and Age Stratum
3.6. Meta-Regression Model Analysis
3.7. Analysis of Intensive Care Unit Admissions and Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, Y.; Wang, X.; Blau, D.M.; Caballero, M.T.; Feikin, D.R.; Gill, C.J.; Madhi, S.A.; Omer, S.B.; Simões, E.A.F.; Campbell, H.; et al. Global, Regional, and National Disease Burden Estimates of Acute Lower Respiratory Infections Due to Respiratory Syncytial Virus in Children Younger Than 5 Years in 2019: A Systematic Analysis. Lancet 2022, 399, 2047–2064. [Google Scholar] [CrossRef] [PubMed]
- Obando-Pacheco, P.; Justicia-Grande, A.J.; Rivero-Calle, I.; Rodríguez-Tenreiro, C.; Sly, P.; Ramilo, O.; Mejías, A.; Baraldi, E.; Papadopoulos, N.G.; Nair, H.; et al. Respiratory Syncytial Virus Seasonality: A Global Overview. J. Infect. Dis. 2018, 217, 1356–1364. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Reeves, R.M.; Wang, X.; Bassat, Q.; Brooks, W.A.; Cohen, C.; Moore, D.P.; Nunes, M.; Rath, B.; Campbell, H.; et al. Global Patterns in Monthly Activity of Influenza Virus, Respiratory Syncytial Virus, Parainfluenza Virus, and Metapneumovirus: A Systematic Analysis. Lancet Glob. Health 2019, 7, e1031–e1045. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019?adgroupsurvey={adgroupsurvey}&gclid=Cj0KCQiAgribBhDkARIsAASA5bsTI4_S1sMrB-dkdzOLNVFioBBozFxhlOz3V1XNgYAq7_OlBxqzluYaAgBGEALw_wcB (accessed on 11 November 2022).
- Bardsley, M.; Morbey, R.A.; Hughes, H.E.; Beck, C.R.; Watson, C.H.; Zhao, H.; Ellis, J.; Smith, G.E.; Elliot, A.J. Epidemiology of Respiratory Syncytial Virus in Children Younger than 5 Years in England during the COVID-19 Pandemic, Measured by Laboratory, Clinical, and Syndromic Surveillance: A Retrospective Observational Study. Lancet Infect. Dis. 2023, 23, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Pruccoli, G.; Castagno, E.; Raffaldi, I.; Denina, M.; Barisone, E.; Baroero, L.; Timeus, F.; Rabbone, I.; Monzani, A.; Terragni, G.M.; et al. The Importance of RSV Epidemiological Surveillance: A Multicenter Observational Study of RSV Infection during the COVID-19 Pandemic. Viruses 2023, 15, 280. [Google Scholar] [CrossRef]
- Ravkin, H.D.; Yom-Tov, E.; Nesher, L. The Effect of Nonpharmaceutical Interventions Implemented in Response to the COVID-19 Pandemic on Seasonal Respiratory Syncytial Virus: Analysis of Google Trends Data. J. Med. Internet Res. 2022, 24, e42781. [Google Scholar] [CrossRef]
- Morawska, L.; Cao, J. Airborne Transmission of SARS-CoV-2: The World Should Face the Reality. Environ. Int. 2020, 139, 105730. [Google Scholar] [CrossRef]
- Lavoie, P.M.; Reicherz, F.; Solimano, A.; Langley, J.M. Potential Resurgence of Respiratory Syncytial Virus in Canada. CMAJ 2021, 193, E1140–E1141. [Google Scholar] [CrossRef]
- Foley, D.A.; Phuong, L.K.; Peplinski, J.; Lim, S.M.; Lee, W.H.; Farhat, A.; Minney-Smith, C.A.; Martin, A.C.; Mace, A.O.; Sikazwe, C.T.; et al. Examining the Interseasonal Resurgence of Respiratory Syncytial Virus in Western Australia. Arch. Dis. Child. 2022, 107, e7. [Google Scholar] [CrossRef] [PubMed]
- McNab, S.; Ha Do, L.A.; Clifford, V.; Crawford, N.W.; Daley, A.; Mulholland, K.; Cheng, D.; South, M.; Waller, G.; Barr, I.; et al. Changing Epidemiology of Respiratory Syncytial Virus in Australia-Delayed Re-Emergence in Victoria Compared to Western Australia/New South Wales (WA/NSW) after Prolonged Lock-Down for Coronavirus Disease 2019 (COVID-19). Clin. Infect Dis. 2021, 73, 2365–2366. [Google Scholar] [CrossRef] [PubMed]
- Curatola, A.; Graglia, B.; Ferretti, S.; Covino, M.; Pansini, V.; Eftimiadi, G.; Chiaretti, A.; Gatto, A. The Acute Bronchiolitis Rebound in Children after COVID-19 Restrictions: A Retrospective, Observational Analysis. Acta Biomed. 2023, 94, e2023031. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- Noyola, D.E.; Esparza-Miranda, L.A.; Leija-Martínez, J.J.; Rivera-Alfaro, G. Impact of Non-Pharmaceutical Interventions During the COVID-19 Pandemic on the Prevalence and Severity of Respiratory Syncytial Virus Lower Respiratory Tract Infections in Pediatric Patients: A Systematic Review. PROSPERO 2022, CRD42022376951. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022376951 (accessed on 11 November 2022).
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Chapter 10: Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022); Cochrane: London, UK, 2022; Available online: www.training.cochrane.org/handbook (accessed on 11 November 2022).
- Hoy, D.; Brooks, P.; Woolf, A.; Blyth, F.; March, L.; Bain, C.; Baker, P.; Smith, E.; Buchbinder, R. Assessing Risk of Bias in Prevalence Studies: Modification of an Existing Tool and Evidence of Interrater Agreement. J. Clin. Epidemiol. 2012, 65, 934–939. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A Critical Appraisal Tool for Systematic Reviews That Include Randomised or Non-Randomised Studies of Healthcare Interventions, or Both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef]
- Lin, L.; Chu, H. Meta-Analysis of Proportions Using Generalized Linear Mixed Models. Epidemiology 2020, 31, 713–717. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Varela, F.H.; Sartor, I.T.S.; Polese-Bonatto, M.; Azevedo, T.R.; Kern, L.B.; Fazolo, T.; de David, C.N.; Zavaglia, G.O.; Fernandes, I.R.; Krauser, J.R.M.; et al. Rhinovirus as the Main Co-Circulating Virus During the COVID-19 Pandemic in Children. J. Pediatr. 2022, 98, 579–586. [Google Scholar] [CrossRef]
- Lucion, M.F.; Del Valle Juárez, M.; Pejito, M.N.; Orqueda, A.S.; Romero Bollón, L.; Mistchenko, A.S.; Gentile, Á. Impact of COVID-19 on the Circulation of Respiratory Viruses in a Children’s Hospital: An Expected Absence. Arch. Argent. Pediatr. 2022, 120, 99–105. [Google Scholar] [CrossRef]
- Diesner-Treiber, S.C.; Voitl, P.; Voitl, J.J.M.; Langer, K.; Kuzio, U.; Riepl, A.; Patel, P.; Mühl-Riegler, A.; Mühl, B. Respiratory Infections in Children During a Covid-19 Pandemic Winter. Front. Pediatr. 2021, 9, 740785. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Delaney, M.; Shah, R.K.; Campos, J.M.; Wessel, D.L.; DeBiasi, R.L. Common Seasonal Respiratory Viral Infections in Children Before and During the Coronavirus Disease 2019 (COVID-19) Pandemic. Infect. Control Hosp. Epidemiol. 2022, 43, 1454–1458. [Google Scholar] [CrossRef] [PubMed]
- Ippolito, G.; La Vecchia, A.; Umbrello, G.; Di Pietro, G.; Bono, P.; Scalia Catenacci, S.; Pinzani, R.; Tagliabue, C.; Bosis, S.; Agostoni, C.; et al. Disappearance of Seasonal Respiratory Viruses in Children Under Two Years Old During COVID-19 Pandemic: A Monocentric Retrospective Study in Milan, Italy. Front. Pediatr. 2021, 9, 721005. [Google Scholar] [CrossRef] [PubMed]
- Stera, G.; Pierantoni, L.; Masetti, R.; Leardini, D.; Biagi, C.; Buonsenso, D.; Pession, A.; Lanari, M. Impact of SARS-CoV-2 Pandemic on Bronchiolitis Hospitalizations: The Experience of an Italian Tertiary Center. Children 2021, 8, 556. [Google Scholar] [CrossRef] [PubMed]
- Regassa, B.T.; Gebrewold, L.A.; Mekuria, W.T.; Kassa, N.A. Molecular Epidemiology of Respiratory Syncytial Virus in Children with Acute Respiratory Illnesses in Africa: A Systematic Review and Meta-Analysis. J. Glob. Health 2023, 13, 04001. [Google Scholar] [CrossRef] [PubMed]
- Pratt, M.T.G.; Abdalla, T.; Richmond, P.C.; Moore, H.C.; Snelling, T.L.; Blyth, C.C.; Bhuiyan, M.U. Prevalence of Respiratory Viruses in Community-Acquired Pneumonia in Children: A Systematic Review and Meta-Analysis. Lancet Child. Adolesc. Health 2022, 6, 555–570. [Google Scholar] [CrossRef] [PubMed]
- Vittucci, A.C.; Piccioni, L.; Coltella, L.; Ciarlitto, C.; Antilici, L.; Bozzola, E.; Midulla, F.; Palma, P.; Perno, C.F.; Villani, A. The Disappearance of Respiratory Viruses in Children During the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 9550. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, L.; Sheppard, M.; Smith, A.; Dietz, S.; Jayanthi, P.; Yuan, Y.; Bull, L.; Wotiz, S.; Schwarze, T.; Azondekon, R.; et al. Changes in Seasonal Respiratory Illnesses in the United States During the Coronavirus Disease 2019 (COVID-19) Pandemic. Clin. Infect. Dis. 2021, 73, S100–S107. [Google Scholar] [CrossRef] [PubMed]
- Billard, M.N.; Bont, L.J. Quantifying the RSV Immunity Debt Following COVID-19: A Public Health Matter. Lancet Infect. Dis. 2023, 23, 3–5. [Google Scholar] [CrossRef]
- Hatter, L.; Eathorne, A.; Hills, T.; Bruce, P.; Beasley, R. Respiratory Syncytial Virus: Paying the Immunity Debt with Interest. Lancet Child. Adolesc. Health 2021, 5, e44–e45. [Google Scholar] [CrossRef]
- Reicherz, F.; Xu, R.Y.; Abu-Raya, B.; Majdoubi, A.; Michalski, C.; Golding, L.; Stojic, A.; Vineta, M.; Granoski, M.; Cieslak, Z.; et al. Waning Immunity Against Respiratory Syncytial Virus During the Coronavirus Disease 2019 Pandemic. J. Infect. Dis. 2022, 226, 2064–2068. [Google Scholar] [CrossRef]
- den Hartog, G.; van Kasteren, P.B.; Schepp, R.M.; Teirlinck, A.C.; van der Klis, F.R.M.; van Binnendijk, R.S. Decline of RSV-Specific Antibodies During the COVID-19 Pandemic. Lancet Infect. Dis. 2023, 23, 23–25. [Google Scholar] [CrossRef]
- Piret, J.; Boivin, G. Viral Interference between Respiratory Viruses. Emerg. Infect. Dis. 2022, 28, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Abu-Raya, B.; Viñeta Paramo, M.; Reicherz, F.; Lavoie, P.M. Why Has the Epidemiology of RSV Changed During the COVID-19 Pandemic? EClinicalMedicine 2023, 61, 102089. [Google Scholar] [CrossRef] [PubMed]
- Stamm, P.; Sagoschen, I.; Weise, K.; Plachter, B.; Münzel, T.; Gori, T.; Vosseler, M. Influenza and RSV Incidence during COVID-19 Pandemic—An Observational Study from In-Hospital Point-of-Care Testing. Med. Microbiol. Immunol. 2021, 210, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Groves, H.E.; Piché-Renaud, P.P.; Peci, A.; Farrar, D.S.; Buckrell, S.; Bancej, C.; Sevenhuysen, C.; Campigotto, A.; Gubbay, J.B.; Morris, S.K. The Impact of the COVID-19 Pandemic on Influenza, Respiratory Syncytial Virus, and Other Seasonal Respiratory Virus Circulation in Canada: A Population-Based Study. Lancet Reg. Health Am. 2021, 1, 100015. [Google Scholar] [CrossRef] [PubMed]
- Suleiman-Martos, N.; Caballero-Vázquez, A.; Gómez-Urquiza, J.L.; Albendín-García, L.; Romero-Béjar, J.L.; Cañadas-De la Fuente, G.A. Prevalence and Risk Factors of Respiratory Syncytial Virus in Children under 5 Years of Age in the WHO European Region: A Systematic Review and Meta-Analysis. J. Pers. Med. 2021, 11, 416. [Google Scholar] [CrossRef] [PubMed]
- Johannesen, C.K.; van Wijhe, M.; Tong, S.; Fernández, L.V.; Heikkinen, T.; van Boven, M.; Wang, X.; Bøås, H.; Li, Y.; Campbell, H.; et al. Age-Specific Estimates of Respiratory Syncytial Virus-Associated Hospitalizations in 6 European Countries: A Time Series Analysis. J. Infect. Dis. 2022, 226, S29–S37. [Google Scholar] [CrossRef]
- Billard, M.N.; van de Ven, P.M.; Baraldi, B.; Kragten-Tabatabaie, L.; Bont, L.J.; Wildenbeest, J.G. International Changes in Respiratory Syncytial Virus (RSV) Epidemiology during the COVID-19 Pandemic: Association with School Closures. Influenza Other Respir. Viruses. 2022, 16, 926–936. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Morgenstern, C.; Kelly, J.; Lowe, R.; CMMID COVID-19 Working Group; Jit, M. The impact of non-pharmaceutical interventions on SARS-CoV-2 transmission across 130 countries and territories. BMC Med. 2021, 19, 40. [Google Scholar] [CrossRef]
- Suryanarayanan, P.; Tsou, C.H.; Poddar, A.; Mahajan, D.; Dandala, B.; Madan, P.; Agrawal, A.; Wachira, C.; Samuel, O.M.; Bar-Shira, O.; et al. AI-Assisted Tracking of Worldwide Non-Pharmaceutical Interventions for COVID-19. Sci. Data. 2021, 8, 94. [Google Scholar] [CrossRef]
- Onwuchekwa, C.; Atwell, J.; Moreo, L.M.; Menon, S.; Machado, B.; Siapka, M.; Agarwal, N.; Rubbrecht, M.; Aponte-Torres, Z.; Rozenbaum, M.; et al. Pediatric Respiratory Syncytial Virus Diagnostic Testing Performance: A Systematic Review and Meta-analysis. J. Infect. Dis. 2023, 228, 1516–1527. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, D.I.; Mejias, A.; Rath, B.; Woods, C.W.; Deeter, J.P. Summarizing Study Characteristics and Diagnostic Performance of Commercially Available Tests for Respiratory Syncytial Virus: A Scoping Literature Review in the COVID-19 Era. J. Appl. Lab. Med. 2023, 8, 353–371. [Google Scholar] [CrossRef]
- Kenmoe, S.; Kengne-Nde, C.; Ebogo-Belobo, J.T.; Mbaga, D.S.; Fatawou Modiyinji, A.; Njouom, R. Systematic Review and Meta-analysis of the Prevalence of Common Respiratory Viruses in Children < 2 Years with Bronchiolitis in the Pre-COVID-19 Pandemic Era. PLoS ONE 2020, 15, e0242302. [Google Scholar] [CrossRef]
- Umuhoza, T.; Bulimo, W.D.; Oyugi, J.; Musabyimana, J.P.; Kinengyere, A.A.; Mancuso, J.D. Prevalence of Human Respiratory Syncytial Virus, Parainfluenza and Adenoviruses in East Africa Community Partner States of Kenya, Tanzania, and Uganda: A Systematic Review and Meta-analysis (2007–2020). PLoS ONE 2021, 16, e0249992. [Google Scholar] [CrossRef]
- Kenmoe, S.; Bigna, J.J.; Well, E.A.; Simo, F.B.N.; Penlap, V.B.; Vabret, A.; Njouom, R. Prevalence of Human Respiratory Syncytial Virus Infection in People with Acute Respiratory Tract Infections in Africa: A Systematic Review and Meta-analysis. Influenza Other Respir. Viruses 2018, 12, 793–803. [Google Scholar] [CrossRef]
- Nygaard, U.; Hartling, U.B.; Nielsen, J.; Vestergaard, L.S.; Dungu, K.H.S.; Nielsen, J.S.A.; Sellmer, A.; Matthesen, A.T.; Kristensen, K.; Holm, M. Hospital admissions and need for mechanical ventilation in children with respiratory syncytial virus before and during the COVID-19 pandemic: A Danish nationwide cohort study. Lancet Child. Adolesc. Health 2023, 7, 171–179. [Google Scholar] [CrossRef] [PubMed]
- ÓhAiseadha, C.; Quinn, G.A.; Connolly, R.; Wilson, A.; Connolly, M.; Soon, W.; Hynds, P. Unintended Consequences of COVID-19 Non-Pharmaceutical Interventions (NPIs) for Population Health and Health Inequalities. Int. J. Environ. Res. Public Health 2023, 20, 5223. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | N = 112 | % |
|---|---|---|
| Age range | ||
| 35 | 31.3 |
| 22 | 19.6 |
| 4 | 3.6 |
| 20 | 17.9 |
| 27 | 24.1 |
| 4 | 3.6 |
| Male range (%) | 39.1–73.8% | |
| Period of inclusion of participants; range | January 2015–December 2022 | |
| Year of publication; range | 2017–2023 | |
| Study design | ||
| 75 | 67 |
| 37 | 33 |
| Sampling method | ||
| 110 | 98.2 |
| 2 | 1.8 |
| Timing of data collection | ||
| 4 | 3.6 |
| 58 | 51.8 |
| 50 | 44.6 |
| Study bias | ||
| 71 | 63.4 |
| 41 | 36.6 |
| WHO region | ||
| 7 | 6.3 |
| 13 | 11.6 |
| 3 | 2.7 |
| 47 | 42 |
| 8 | 7.1 |
| 34 | 30.4 |
| Type of assay | ||
| 22 | 19.6 |
| 85 | 75.9 |
| 5 | 4.5 |
| Diagnostic technique $ | ||
| 6 | 5.4 |
| 16 | 14.3 |
| 5 | 4.5 |
| 14 | 12.5 |
| 18 | 16.1 |
| 16 | 14.3 |
| 2 | 1.8 |
| 31 | 27.7 |
| 4 | 3.6 |
| Sample type | ||
| 7 | 6.3 |
| 9 | 8 |
| 62 | 55.4 |
| 11 | 9.8 |
| 8 | 7.1 |
| 7 | 6.3 |
| 3 | 2.7 |
| 5 | 4.5 |
| Groups | Studies (n) | RSV-Positive (n) | Total (n) | Pooled Prevalence (95% CI) | Q-Value | I2 (%) | p Value Heterogeneity | p Value Egger Test | p Value Subgroup Difference |
|---|---|---|---|---|---|---|---|---|---|
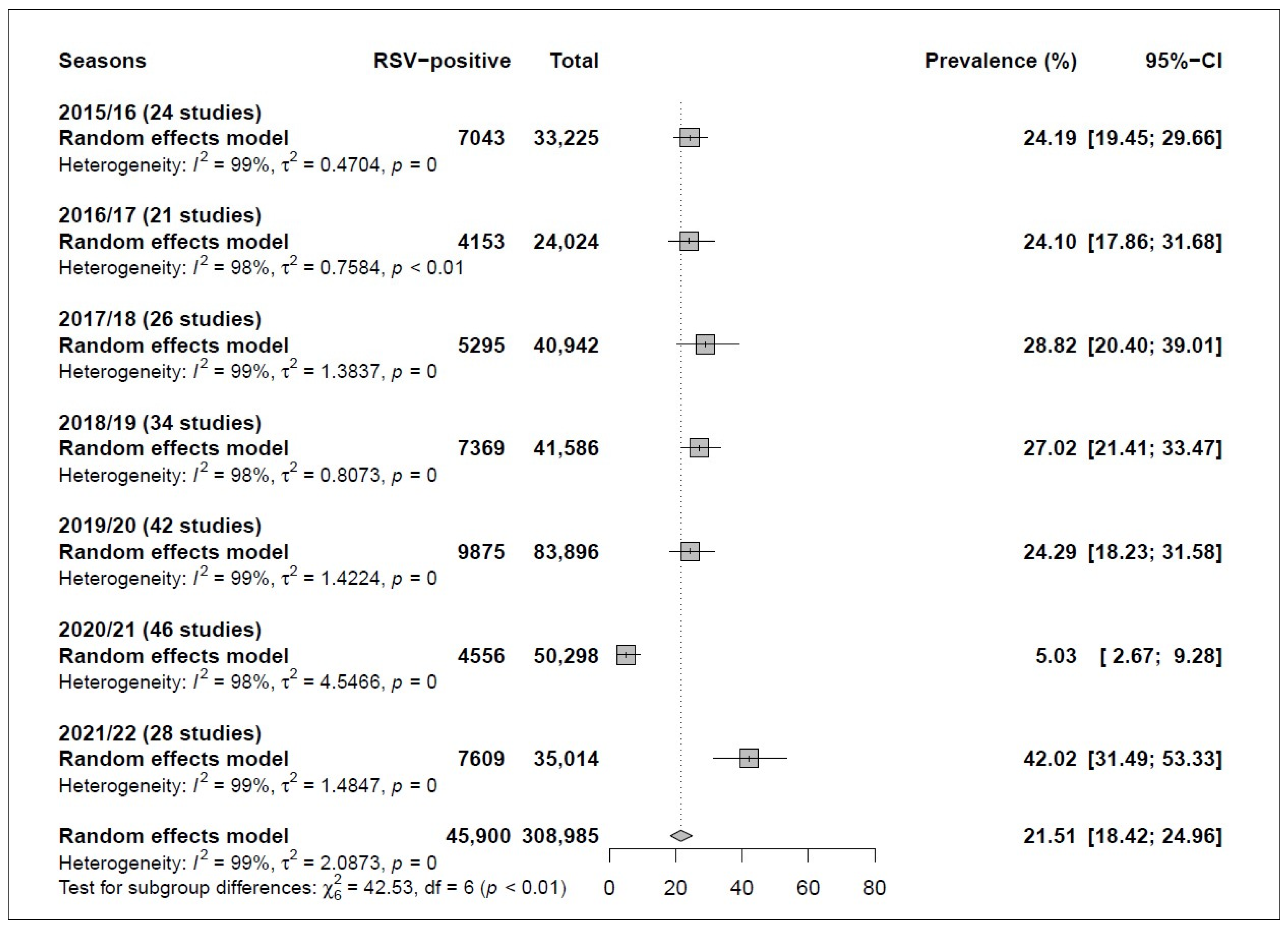
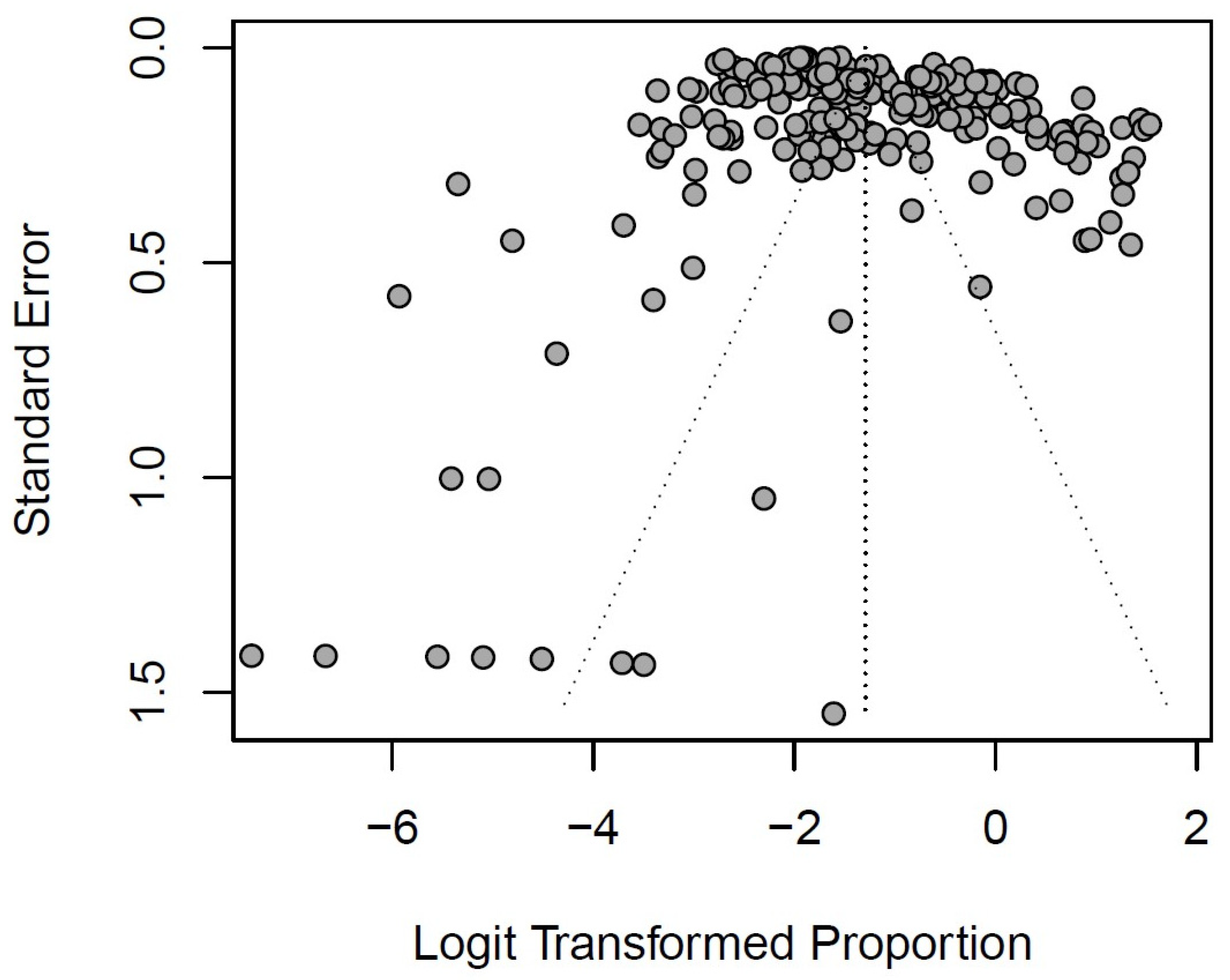
| Overall | 112 | 45,900 | 308,985 | 21.51 [18.42; 24.96] | 22,893.65 | 99.0 | <0.0001 | <0.0001 | NA |
| Subgroup analyses | |||||||||
| Period | <0.0001 | ||||||||
| Pre-pandemic (2015/20) | 83 | 33,735 | 223,673 | 25.60 [22.57; 28.88] | 15,032.9 | 99.0 | <0.0001 | <0.0001 | |
| Lockdown (2020/21) | 46 | 4556 | 50,298 | 5.03 [2.67; 9.28] | 2581.79 | 98.3 | <0.0001 | 0.5569 | |
| Post-lockdown (2021/22) | 28 | 7609 | 35,014 | 42.02 [31.49; 53.33] | 3765.28 | 99.3 | <0.0001 | <0.0001 | |
| Seasons | <0.0001 | ||||||||
| 2015/16 | 24 | 7043 | 33,225 | 24.19 [19.45; 29.66] | 1620.84 | 98.60 | <0.0001 | 0.2232 | |
| 2016/17 | 21 | 4153 | 24,024 | 24.10 [17.86; 31.68] | 1298.39 | 98.50 | <0.0001 | 0.035 | |
| 2017/18 | 26 | 5295 | 40,942 | 28.82 [20.40; 39.01] | 2855.18 | 99.10 | <0.0001 | 0.0003 | |
| 2018/19 | 34 | 7369 | 41,586 | 27.02 [21.41; 33.47] | 2139.94 | 98.50 | <0.0001 | 0.0011 | |
| 2019/20 | 42 | 9875 | 83,896 | 24.29 [18.23; 31.58] | 5676.49 | 99.30 | <0.0001 | 0.0003 | |
| 2020/21 | 46 | 4556 | 50,298 | 5.03 [2.67; 9.28] | 2581.79 | 98.30 | <0.0001 | 0.5569 | |
| 2021/22 | 28 | 7609 | 35,014 | 42.02 [31.49; 53.33] | 3765.28 | 99.30 | <0.0001 | <0.0001 | |
| WHO Region | 0.0004 | ||||||||
| African | 7 | 837 | 3602 | 19.42 [14.19; 25.98] | 224.25 | 96.0 | <0.0001 | 0.0276 | |
| Americas | 13 | 2029 | 6370 | 11.17 [2.19; 41.42] | 194.76 | 93.3 | <0.0001 | 0.7522 | |
| Eastern Mediterranean | 3 | 151 | 568 | 26.53 [15.66; 41.25] | 33.53 | 94.0 | <0.0001 | NA | |
| European | 47 | 14,877 | 70,357 | 28.90 [22.73; 35.98] | 7570.45 | 98.7 | <0.0001 | 0.0004 | |
| South–East Asia | 8 | 1283 | 5987 | 24.85 [14.25; 39.67] | 758.49 | 98.7 | <0.0001 | 0.6948 | |
| Western Pacific | 34 | 26,723 | 222,101 | 14.71 [12.28; 17.52] | 8245.53 | 99.0 | <0.0001 | 0.1071 | |
| Age | <0.0001 | ||||||||
| <2 years | 35 | 6815 | 17,696 | 43.54 [35.56; 51.87] | 1972.43 | 96.7 | <0.0001 | 0.0017 | |
| <5 years | 22 | 7223 | 36,599 | 25.59 [21.03; 30.76] | 2760.33 | 98.8 | <0.0001 | 0.0781 | |
| <10 years | 4 | 7706 | 65,262 | 17.34 [11.89; 24.58] | 1267.48 | 99.0 | <0.0001 | 0.1347 | |
| <15 years | 20 | 5745 | 40,646 | 17.58 [12.82; 23.64] | 4016.97 | 99.1 | <0.0001 | 0.7428 | |
| <18 years | 27 | 17,408 | 139,980 | 10.17 [7.29; 14.02] | 5,380.77 | 99.0 | <0.0001 | 0.9850 | |
| Not reported | 4 | 1003 | 8802 | 9.94 [5.19; 18.18] | 276.85 | 95.7 | <0.0001 | 0.3230 | |
| Design | 0.0840 | ||||||||
| Cross-sectional | 75 | 35,091 | 263,251 | 19.64 [16.55; 23.15] | 15,271.27 | 98.9 | <0.0001 | <0.0001 | |
| Longitudinal | 37 | 10,809 | 45,734 | 27.34 [19.47; 36.94] | 4589.11 | 98.8 | <0.0001 | 0.0379 | |
| Timing of data collection | 0.5983 | ||||||||
| Ambispective | 4 | 1449 | 11,714 | 15.30 [4.70; 39.82] | 657.29 | 98.8 | <0.0001 | NA | |
| Prospective | 58 | 12,676 | 66,479 | 23.44 [18.63; 29.05] | 7496.05 | 98.9 | <0.0001 | 0.1370 | |
| Retrospective | 50 | 31,775 | 230,792 | 20.82 [16.90; 25.37] | 12,692.16 | 99.0 | <0.0001 | 0.0007 | |
| Risk of bias | 0.1453 | ||||||||
| Low risk | 71 | 31,179 | 222,366 | 23.29 [19.18; 27.98] | 17,585.49 | 99.2 | <0.0001 | <0.0001 | |
| Moderate risk | 41 | 14,721 | 86,619 | 18.49 [14.32; 23.54] | 5058.52 | 98.5 | <0.0001 | 0.0752 | |
| Type of assay | 0.0007 | ||||||||
| Immune assays ¥ | 22 | 19,476 | 180,647 | 13.94 [10.65; 18.04] | 4163.17 | 98.9 | <0.0001 | 0.5255 | |
| Molecular assays ¥¥ | 85 | 22,523 | 103,157 | 24.96 [20.77; 29.69] | 10,441.27 | 98.5 | <0.0001 | 0.0350 | |
| Mixed assays ¥¥¥ | 5 | 3901 | 25,181 | 14.74 [8.27; 24.91] | 872.62 | 96.3 | <0.0001 | 0.3155 | |
| Diagnostic technique $ | 0.0016 | ||||||||
| Antigen testing | 6 | 8018 | 75,112 | 17.78 [10.71; 28.05] | 1187.05 | 98.9 | <0.0001 | 0.4242 | |
| Direct immunofluorescence | 16 | 11,458 | 105,535 | 12.46 [9.14; 16.77] | 2892.56 | 99.0 | <0.0001 | 0.8831 | |
| Mixed assays ¥¥¥ | 5 | 3901 | 25,181 | 14.74 [8.27; 24.91] | 1187.05 | 98.9 | <0.0001 | 0.3155 | |
| Multiplex PCR | 14 | 2083 | 10,831 | 27.32 [14.57; 45.30] | 2965.49 | 99.0 | <0.0001 | 0.0439 | |
| Multiplex RT–PCR | 18 | 2215 | 7385 | 30.89 [22.03; 41.42] | 872.62 | 98.3 | <0.0001 | 0.3490 | |
| PCR | 16 | 7247 | 32,319 | 24.91 [16.89; 35.12] | 1756.55 | 98.7 | <0.0001 | 0.8591 | |
| qPCR | 2 | 52 | 140 | 38.93 [21.17; 60.20] | 828.23 | 97.0 | 0.0008 | NA | |
| RT–PCR | 31 | 9193 | 46,668 | 22.15 [16.57; 28.95] | 3648.00 | 99.1 | <0.0001 | 0.0936 | |
| RT–qPCR | 4 | 1733 | 5814 | 17.82 [3.59; 55.79] | 11.32 | 91.2 | <0.0001 | NA | |
| Sample type | 0.0023 | ||||||||
| Mixed specimens * | 7 | 3091 | 14,765 | 18.35 [8.59; 34.98] | 1408.90 | 99.0 | <0.0001 | 0.7840 | |
| Nasal secretions | 9 | 1209 | 3493 | 21.39 [6.94; 49.83] | 263.44 | 95.8 | <0.0001 | 0.5521 | |
| Nasopharyngeal secretions | 62 | 21,542 | 114,495 | 26.25 [21.48; 31.66] | 9150.13 | 98.7 | <0.0001 | <0.0001 | |
| Nasopharyngeal secretions or BLF | 11 | 4374 | 52,107 | 12.12 [8.34; 17.28] | 1848.89 | 98.6 | <0.0001 | 0.0770 | |
| Not reported | 8 | 10,981 | 85,775 | 21.26 [10.99; 37.13] | 2581.81 | 99.3 | <0.0001 | 0.0036 | |
| Oropharyngeal secretions | 7 | 2663 | 20,375 | 15.48 [12.23; 19.39] | 778.85 | 97.7 | <0.0001 | 0.2721 | |
| Sputum | 3 | 549 | 2063 | 25.23 [18.38; 33.58] | 44.03 | 95.5 | <0.0001 | NA | |
| Throat secretions | 5 | 1491 | 15,912 | 16.79 [7.88; 32.26] | 1097.90 | 99.3 | <0.0001 | NA |
| Groups | Studies (n) | RSV-Positive (n) | Total (n) | Pooled Prevalence (95% CI) | Q-Value | I2 (%) | p Value Heterogeneity | p Value Egger Test | p Value Subgroup Difference |
|---|---|---|---|---|---|---|---|---|---|
| WHO Region ## | |||||||||
| European | 47 | 14,877 | 70,357 | 28.90 [22.73; 35.98] | 7570.45 | 98.7 | <0.0001 | 0.0004 | |
| Period | <0.0001 | ||||||||
| Pre-pandemic (2015/20) | 28 | 10,348 | 48,140 | 34.81 [29.47; 40.56] | 3905.86 | 98.50 | <0.0001 | 0.0001 | |
| Lockdown (2020/21) | 23 | 1028 | 12,898 | 4.89 [1.68; 13.39] | 853.67 | 97.40 | <0.0001 | 0.7463 | |
| Post-lockdown (2021/22) | 18 | 3501 | 9319 | 55.18 [42.96; 66.80] | 1479.62 | 98.90 | <0.0001 | 0.0093 | |
| Western Pacific | 34 | 26,723 | 222,101 | 14.71 [12.28; 17.52] | 8245.53 | 99.0 | <0.0001 | 0.1071 | |
| Period | 0.0024 | ||||||||
| Pre-pandemic (2015/20) | 29 | 19,728 | 162,313 | 16.12 [13.28; 19.43] | 6290.45 | 99.10 | <0.0001 | 0.0424 | |
| Lockdown (2020/21) | 16 | 3215 | 34,966 | 8.03 [4.99; 12.68] | 1240.05 | 98.80 | <0.0001 | 0.5502 | |
| Post-lockdown (2021/22) | 8 | 3780 | 24,822 | 22.83 [15.42; 32.42] | 356.45 | 98.00 | <0.0001 | NA | |
| Countries && | |||||||||
| Italy | 20 | 5437 | 14,928 | 47.14 [37.07; 57.45] | 1877.72 | 97.8 | <0.0001 | 0.0011 | |
| Period | 0.0024 | ||||||||
| Pre-pandemic (2015/20) | 10 | 2955 | 9600 | 51.87 [43.11; 60.51] | 815.15 | 97.40 | <0.0001 | <0.0001 | |
| Lockdown (2020/21) | 8 | 43 | 801 | 5.93 [0.89; 30.68] | 110.71 | 93.70 | <0.0001 | NA | |
| Post-lockdown (2021/22) | 13 | 2439 | 4527 | 63.59 [53.25; 72.81] | 381.83 | 96.90 | <0.0001 | 0.0136 | |
| China | 27 | 23,416 | 211,831 | 11.33 [9.61; 13.30] | 4416.56 | 98.6 | <0.0001 | 0.6889 | |
| Period | 0.0002 | ||||||||
| Pre-pandemic (2015/20) | 23 | 16,898 | 153,351 | 12.04 [10.12; 14.26] | 3350.33 | 98.70 | <0.0001 | 0.79 | |
| Lockdown (2020/21) | 12 | 2868 | 34,012 | 6.64 [4.83; 9.07] | 347.18 | 96.80 | <0.0001 | 0.0314 | |
| Post-lockdown (2021/22) | 6 | 3650 | 24,468 | 19.89 [12.49; 30.15] | 237.17 | 97.90 | <0.0001 | NA |
| Groups | Studies (n) | RSV-positive (n) | Total (n) | Pooled Prevalence (95%CI) | Q-Value | I2 (%) | p Value Heterogeneity | p Value Egger Test | p Value Subgroup Difference |
|---|---|---|---|---|---|---|---|---|---|
| Age stratum | |||||||||
| Age < 2 years | 35 | 6815 | 17,696 | 43.54 [35.56; 51.87] | 1972.43 | 96.7 | <0.0001 | 0.0017 | NA |
| Period | <0.0001 | ||||||||
| Pre-pandemic (2015/20) | 23 | 4844 | 12,939 | 47.82 [42.06; 53.65] | 1019.71 | 96.10 | <0.0001 | <0.0001 | |
| Lockdown (2020/21) | 14 | 261 | 1359 | 6.46 [1.19; 28.29] | 137.86 | 90.60 | <0.0001 | 0.1192 | |
| Post-lockdown (2021/22) | 12 | 1710 | 3398 | 67.61 [57.01; 76.67] | 698.1 | 98.40 | <0.0001 | 0.0004 | |
| Age < 5 years | 22 | 7223 | 36,599 | 25.59 [21.03; 30.76] | 2760.33 | 98.8 | <0.0001 | 0.0781 | NA |
| Period | 0.1193 | ||||||||
| Pre-pandemic (2015/20) | 19 | 5424 | 23,892 | 25.58 [20.94; 30.84] | 1464.93 | 98.10 | <0.0001 | 0.4885 | |
| Lockdown (2020/21) | 3 | 1422 | 11,913 | 17.34 [7.61; 34.84] | 380.63 | 99.50 | <0.0001 | NA | |
| Post-lockdown (2021/22) | 2 | 377 | 794 | 42.69 [24.30; 63.35] | 57.54 | 98.30 | <0.0001 | NA | |
| Age < 10 years | 4 | 7706 | 65,262 | 17.34 [11.89; 24.58] | 1267.48 | 99.0 | <0.0001 | 0.1347 | NA |
| Period | 0.0384 | ||||||||
| Pre-pandemic (2015/20) | 4 | 5554 | 48,007 | 20.48 [13.90; 29.11] | 1249.79 | 99.20 | <0.0001 | 0.1212 | |
| Lockdown (2020/21) | 2 | 795 | 6989 | 7.39 [2.93; 17.40] | 5.34 | 81.30 | 0.0208 | NA | |
| Post-lockdown (2021/22) | 1 | 1357 | 10,266 | 13.22 [12.58; 13.89] | 0 | NA | NA | NA | |
| Age < 15 years | 20 | 5745 | 40,646 | 17.58 [12.82; 23.64] | 4016.97 | 99.1 | <0.0001 | 0.7428 | NA |
| Period | <0.0001 | ||||||||
| Pre-pandemic (2015/20) | 15 | 3963 | 31,279 | 19.46 [14.11; 26.23] | 1939.82 | 98.70 | <0.0001 | 0.0083 | |
| Lockdown (2020/21) | 7 | 304 | 5790 | 6.02 [2.38; 14.39] | 168.99 | 96.40 | <0.0001 | NA | |
| Post-lockdown (2021/22) | 6 | 1478 | 3577 | 31.37 [17.22; 50.12] | 87.88 | 94.30 | <0.0001 | NA | |
| Age < 18 years | 27 | 17,408 | 139,980 | 10.17 [7.29; 14.02] | 5380.77 | 99.0 | <0.0001 | 0.9850 | NA |
| Period | <0.0001 | ||||||||
| Pre-pandemic (2015/20) | 19 | 13,026 | 99,877 | 16.68 [13.29; 20.72] | 3843.26 | 99.20 | <0.0001 | 0.1671 | |
| Lockdown (2020/21) | 17 | 1695 | 23,124 | 2.53 [1.07; 5.85] | 1230.46 | 98.70 | <0.0001 | 0.1565 | |
| Post-lockdown (2021/22) | 7 | 2687 | 16,979 | 17.61 [14.30; 21.51] | 48.9 | 87.70 | <0.0001 | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leija-Martínez, J.J.; Esparza-Miranda, L.A.; Rivera-Alfaro, G.; Noyola, D.E. Impact of Nonpharmaceutical Interventions during the COVID-19 Pandemic on the Prevalence of Respiratory Syncytial Virus in Hospitalized Children with Lower Respiratory Tract Infections: A Systematic Review and Meta-Analysis. Viruses 2024, 16, 429. https://doi.org/10.3390/v16030429
Leija-Martínez JJ, Esparza-Miranda LA, Rivera-Alfaro G, Noyola DE. Impact of Nonpharmaceutical Interventions during the COVID-19 Pandemic on the Prevalence of Respiratory Syncytial Virus in Hospitalized Children with Lower Respiratory Tract Infections: A Systematic Review and Meta-Analysis. Viruses. 2024; 16(3):429. https://doi.org/10.3390/v16030429
Chicago/Turabian StyleLeija-Martínez, José J., Luis A. Esparza-Miranda, Gerardo Rivera-Alfaro, and Daniel E. Noyola. 2024. "Impact of Nonpharmaceutical Interventions during the COVID-19 Pandemic on the Prevalence of Respiratory Syncytial Virus in Hospitalized Children with Lower Respiratory Tract Infections: A Systematic Review and Meta-Analysis" Viruses 16, no. 3: 429. https://doi.org/10.3390/v16030429
APA StyleLeija-Martínez, J. J., Esparza-Miranda, L. A., Rivera-Alfaro, G., & Noyola, D. E. (2024). Impact of Nonpharmaceutical Interventions during the COVID-19 Pandemic on the Prevalence of Respiratory Syncytial Virus in Hospitalized Children with Lower Respiratory Tract Infections: A Systematic Review and Meta-Analysis. Viruses, 16(3), 429. https://doi.org/10.3390/v16030429