
Parvovirus B19 Outbreak in Israel: Retrospective Molecular Analysis from 2010 to 2023
 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Samples
2.2. Molecular Analysis
2.3. Phylogenetic Analysis
3. Results
3.1. B19V Positive Rates, 2010–2023
3.2. Demographics of B19V Infections
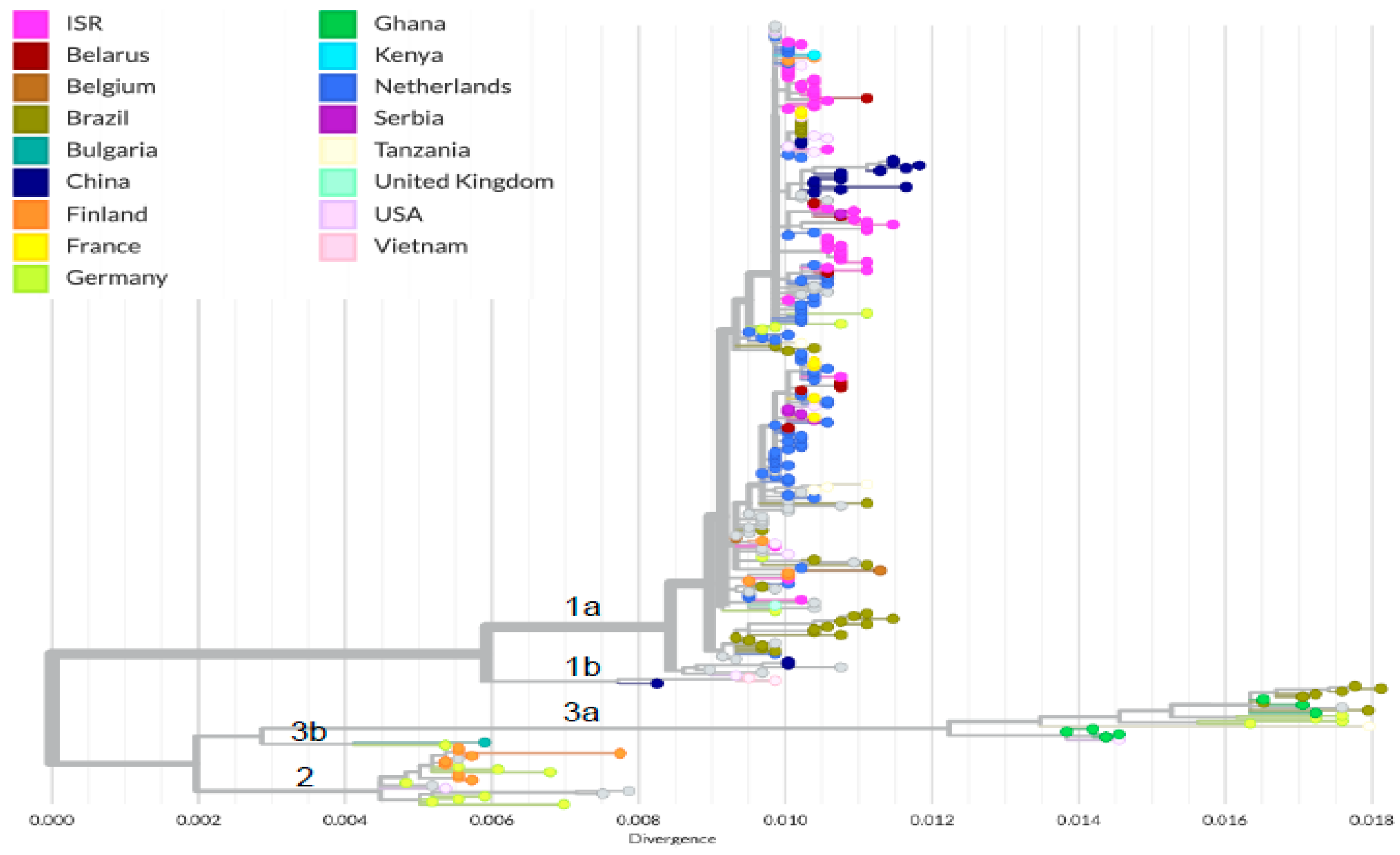
3.3. Phylogenetic Analysis of Circulating B19V
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heegaard, E.D.; Brown, K.E. Human parvovirus B19. Clin. Microbiol. Rev. 2002, 15, 485–505. [Google Scholar] [CrossRef]
- Bichicchi, F.; Guglietta, N.; Rocha Alves, A.D.; Fasano, E.; Manaresi, E.; Bua, G.; Gallinella, G. Next Generation Sequencing for the Analysis of Parvovirus B19 Genomic Diversity. Viruses 2023, 15, 217. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.K.C.; Lam, J.M.; Barankin, B.; Leong, K.F.; Hon, K.L. Erythema Infectiosum: A Narrative Review. Curr. Pediatr. Rev. 2023, 28, 1573396320666230428104619. [Google Scholar] [CrossRef]
- Cnc Garcia, R.; Leon, L.A. Human parvovirus B19: A review of clinical and epidemiological aspects in Brazil. Future Microbiol. 2021, 16, 37–50. [Google Scholar] [CrossRef]
- de Jong, E.P.; Walther, F.J.; Kroes, A.C.; Oepkes, D. Parvovirus B19 infection in pregnancy: New insights and management. Prenat. Diagn. 2011, 31, 419–425. [Google Scholar] [CrossRef]
- Enders, M.; Schalasta, G.; Baisch, C.; Weidner, A.; Pukkila, L.; Kaikkonen, L.; Lankinen, H.; Hedman, L.; Soderlund-Venermo, M.; Hedman, K. Human parvovirus B19 infection during pregnancy—Value of modern molecular and serological diagnostics. J. Clin. Virol. 2006, 35, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Landry, M.L. Parvovirus B19. Microbiol. Spectr. 2016, 4, 297–310. [Google Scholar] [CrossRef] [PubMed]
- Adamson-Small, L.A.; Ignatovich, I.V.; Laemmerhirt, M.G.; Hobbs, J.A. Persistent parvovirus B19 infection in non-erythroid tissues: Possible role in the inflammatory and disease process. Virus Res. 2014, 190, 8–16. [Google Scholar] [CrossRef]
- Nicolay, N.; Cotter, S. Clinical and epidemiological aspects of parvovirus B19 infections in Ireland, January 1996–June 2008. Euro Surveill 2009, 14, 19249. [Google Scholar] [CrossRef]
- Mor, O.; Ofir, I.; Pavel, R.; Bassal, R.; Kra-Oz, Z.; Cohen, D.; Shohat, T.; Mendelson, E. Parvovirus B19V infection in Israel: Prevalence and occurrence of acute infection between 2008 and 2013. Epidemiol. Infect. 2016, 144, 207–214. [Google Scholar] [CrossRef]
- Patalon, T.; Saciuk, Y.; Trotzky, D.; Pachys, G.; Ben-Tov, A.; Segal, Y.; Gazit, S. An Outbreak of Parvovirus B19 in Israel. Viruses 2023, 15, 2261. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, A.; Yoto, Y.; Tsugawa, T.; Tsutsumi, H. Quantitation of human parvovirus B19 DNA in erythema infectiosum and aplastic crisis. J. Med. Virol. 2014, 86, 2102–2106. [Google Scholar] [CrossRef] [PubMed]
- Ewels, P.; Magnusson, M.; Lundin, S.; Käller, M. MultiQC: Summarize analysis results for multiple tools and samples in a single report. Bioinformatics 2016, 32, 3047–3048. [Google Scholar] [CrossRef] [PubMed]
- Bolger, A.M.; Lohse, M.; Usadel, B. Trimmomatic: A flexible trimmer for Illumina sequence data. Bioinformatics 2014, 30, 2114–2120. [Google Scholar] [CrossRef]
- Li, H.; Durbin, R. Fast and accurate short read alignment with Burrows-Wheeler transform. Bioinformatics 2009, 25, 1754–1760. [Google Scholar] [CrossRef]
- Li, H.; Handsaker, B.; Wysoker, A.; Fennell, T.; Ruan, J.; Homer, N.; Marth, G.; Abecasis, G.; Durbin, R. The Sequence Alignment/Map format and SAMtools. Bioinformatics 2009, 25, 2078–2079. [Google Scholar] [CrossRef]
- Grubaugh, N.D.; Gangavarapu, K.; Quick, J.; Matteson, N.L.; De Jesus, J.G.; Main, B.J.; Tan, A.L.; Paul, L.M.; Brackney, D.E.; Grewal, S.; et al. An amplicon-based sequencing framework for accurately measuring intrahost virus diversity using PrimalSeq and iVar. Genome Biol. 2019, 20, 8. [Google Scholar] [CrossRef]
- Hadfield, J.; Megill, C.; Bell, S.M.; Huddleston, J.; Potter, B.; Callender, C.; Sagulenko, P.; Bedford, T.; Neher, R.A. Nextstrain: Real-time tracking of pathogen evolution. Bioinformatics 2018, 34, 4121–4123. [Google Scholar] [CrossRef]
- Nguyen, L.T.; Schmidt, H.A.; von Haeseler, A.; Minh, B.Q. IQ-TREE: A fast and effective stochastic algorithm for estimating maximum-likelihood phylogenies. Mol. Biol. Evol. 2015, 32, 268–274. [Google Scholar] [CrossRef]
- Sagulenko, P.; Puller, V.; Neher, R.A. TreeTime: Maximum-likelihood phylodynamic analysis. Virus Evol. 2018, 4, vex042. [Google Scholar] [CrossRef]
- Jiang, H.; Qiu, Q.; Zhou, Y.; Zhang, Y.; Xu, W.; Cui, A.; Li, X. The epidemiological and genetic characteristics of human parvovirus B19 in patients with febrile rash illnesses in China. Sci. Rep. 2023, 13, 15913. [Google Scholar] [CrossRef]
- Mengyi, Z.; Yuhui, L.; Zhan, G.; Anqing, L.; Yujia, L.; Shilin, L.; Lei, G.; Yue, L.; Mei, H.; Jianhua, W.; et al. Plasma metagenomics reveals regional variations of emerging and re-emerging pathogens in Chinese blood donors with an emphasis on human parvovirus B19. One Health 2023, 17, 100602. [Google Scholar] [CrossRef]
- Sengupta, S.; Ince, L.; Sartor, F.; Borrmann, H.; Zhuang, X.; Naik, A.; Curtis, A.; McKeating, J.A. Clocks, Viruses, and Immunity: Lessons for the COVID-19 Pandemic. J. Biol. Rhythm. 2021, 36, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Chow, E.J.; Uyeki, T.M.; Chu, H.Y. The effects of the COVID-19 pandemic on community respiratory virus activity. Nat. Rev. Microbiol. 2023, 21, 195–210. [Google Scholar] [CrossRef] [PubMed]
- Harapan, H.; Ryan, M.; Yohan, B.; Abidin, R.S.; Nainu, F.; Rakib, A.; Jahan, I.; Emran, T.B.; Ullah, I.; Panta, K.; et al. COVID-19 and dengue: Double punches for dengue-endemic countries in Asia. Rev. Med. Virol. 2021, 31, 18. [Google Scholar] [CrossRef]
- Molenaar-de Backer, M.W.; Hogema, B.M.; Koppelman, M.H.; van de Laar, T.J.; Slot, E.; Zaaijer, H.L. Lower Incidence of Parvovirus-B19 Infections in Dutch Blood Donors during SARS-CoV-2 Pandemic. Microbiol. Spectr. 2021, 9, e0025321. [Google Scholar] [CrossRef] [PubMed]
- Hayes, L.J.; Uri, H.; Bojkova, D.; Cinatl, J., Jr.; Wass, M.N.; Michaelis, M. Impact of the COVID-19 pandemic on the circulation of other pathogens in England. J. Med. Virol. 2023, 95, e28401. [Google Scholar] [CrossRef]
- Leshem, E.; Afek, A.; Kreiss, Y. Buying Time with COVID-19 Outbreak Response, Israel. Emerg. Infect. Dis. 2020, 26, 2251–2253. [Google Scholar] [CrossRef]
- Ivanova, S.K.; Mihneva, Z.G.; Toshev, A.K.; Kovaleva, V.P.; Andonova, L.G.; Muller, C.P.; Hübschen, J.M. Insights into epidemiology of human parvovirus B19 and detection of an unusual genotype 2 variant, Bulgaria, 2004 to 2013. Euro Surveill 2016, 21, 1560–7917. [Google Scholar] [CrossRef]
- Bua, G.; Marrazzo, P.; Manaresi, E.; Gamberini, C.; Bonsi, L.; Alviano, F.; Gallinella, G. Non-Permissive Parvovirus B19 Infection: A Reservoir and Questionable Safety Concern in Mesenchymal Stem Cells. Int. J. Mol. Sci. 2023, 24, 8204. [Google Scholar] [CrossRef]
- Gigi, C.E.; Anumba, D.O.C. Parvovirus b19 infection in pregnancy—A review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 264, 358–362. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mor, O.; Wax, M.; Arami, S.-S.; Yitzhaki, M.; Kriger, O.; Erster, O.; Zuckerman, N.S. Parvovirus B19 Outbreak in Israel: Retrospective Molecular Analysis from 2010 to 2023. Viruses 2024, 16, 480. https://doi.org/10.3390/v16030480
Mor O, Wax M, Arami S-S, Yitzhaki M, Kriger O, Erster O, Zuckerman NS. Parvovirus B19 Outbreak in Israel: Retrospective Molecular Analysis from 2010 to 2023. Viruses. 2024; 16(3):480. https://doi.org/10.3390/v16030480
Chicago/Turabian StyleMor, Orna, Marina Wax, Shoshana-Shani Arami, Maya Yitzhaki, Or Kriger, Oran Erster, and Neta S. Zuckerman. 2024. "Parvovirus B19 Outbreak in Israel: Retrospective Molecular Analysis from 2010 to 2023" Viruses 16, no. 3: 480. https://doi.org/10.3390/v16030480
APA StyleMor, O., Wax, M., Arami, S.-S., Yitzhaki, M., Kriger, O., Erster, O., & Zuckerman, N. S. (2024). Parvovirus B19 Outbreak in Israel: Retrospective Molecular Analysis from 2010 to 2023. Viruses, 16(3), 480. https://doi.org/10.3390/v16030480