

Detection of High-Risk Human Papillomavirus (HPV), p16 and EGFR in Lung Cancer: Insights from the Mediterranean Region of Turkey
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection and Data Collection
2.2. DNA Extraction
2.3. HPV DNA Detection and Genotyping
2.4. EGFR Mutation Detection
2.5. p16 Immunohistochemical Staining
2.6. Statistical Analysis
3. Results
3.1. Clinicopathological Characteristics of Patients
3.2. HPV Infection, Prevalence of HPV Types, and Their Relationship with Clinicopathologic Parameters
3.3. Presence of EGFR Mutation and Its Relation with HPV
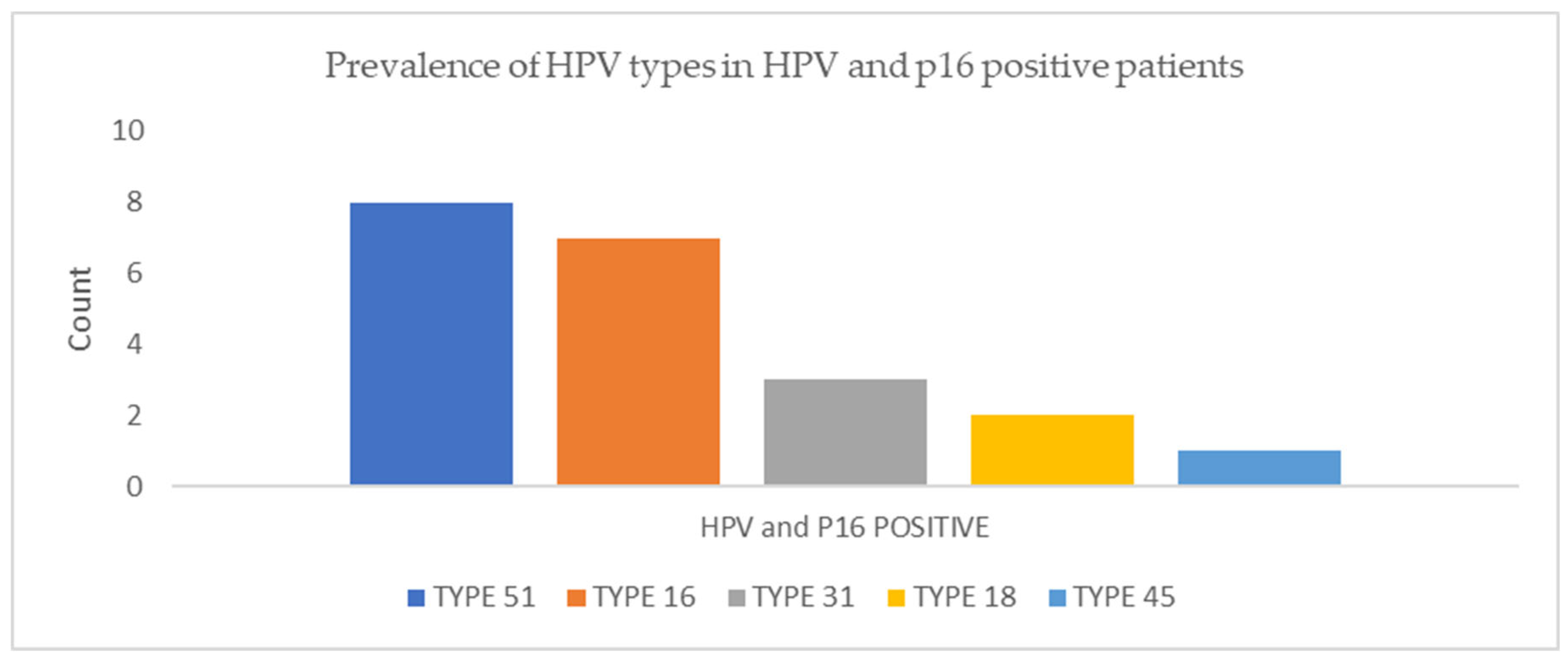
3.4. Detection of p16 by Immunohistochemistry
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sagerup, C.M.T.; Nymoen, D.A.; Halvorsen, A.R.; Iversen, M.L.; Helland, A.; Brustugun, O.T. Human papilloma virus detection and typing in 334 lung cancer patients. Acta Oncol. 2014, 53, 952–957. [Google Scholar] [CrossRef] [PubMed]
- Shikova, E.; Ivanova, Z.; Alexandrova, D.; Shindov, M.; Lekov, A. Human papillomavirus prevalence in lung carcinomas in Bulgaria. Microbiol. Immunol. 2017, 61, 427–432. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, T.H.A.; do Amaral, C.M.; de França São Marcos, B.; Nascimento, K.C.G.; de Miranda Rios, A.C.; Quixabeira, D.C.A.; Muniz, M.T.C.; Silva Neto, J.D.C.; de Freitas, A.C. Presence and activity of HPV in primary lung cancer. J. Cancer Res. Clin. Oncol. 2018, 144, 2367–2376. [Google Scholar] [CrossRef] [PubMed]
- de Freitas, A.C.; Gurgel, A.P.; de Lima, E.G.; de França São Marcos, B.; do Amaral, C.M. Human papillomavirus and lung cancinogenesis: An overview. J. Cancer Res. Clin. Oncol. 2016, 142, 2415–2427. [Google Scholar] [CrossRef] [PubMed]
- Klein, F.; Amin Kotb, W.F.; Petersen, I. Incidence of human papilloma virus in lung cancer. Lung Cancer 2009, 65, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Kotb, W.F.; Petersen, I. Morphology, DNA ploidy and HPV in lung cancer and head and neck cancer. Pathol. Res. Pract. 2012, 208, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.S.; Lundine, D.; Leeman, J.E.; Higginson, D.S. Genomic Signatures in HPV- Associated Tumors. Viruses 2021, 13, 1998. [Google Scholar] [CrossRef] [PubMed]
- Gatta, L.B.; Balzarini, P.; Tironi, A.; Berenzi, A.; Benetti, A.; Angiero, F.; Grigolato, P.; Dessy, E. Human papillomavirus DNA and p16 gene in squamous cell lung carcinoma. Anticancer Res. 2012, 32, 3085–3089. [Google Scholar]
- Zhou, Y.; Höti, N.; Ao, M.; Zhang, Z.; Zhu, H.; Li, L.; Askin, F.; Gabrielson, E.; Zhang, H.; Li, Q.K. Expression of p16 and p53 in non-small-cell lung cancer: Clinicopathological correlation and potential prognostic impact. Biomark. Med. 2019, 13, 761–771. [Google Scholar] [CrossRef]
- São Marcos, B.F.; de Oliveira, T.H.A.; do Amaral, C.M.C.; Muniz, M.T.C.; Freitas, A.C. Correlation between HPV PCNA, p16, and p21 expression in lung cancer patients. Cell. Microbiol. 2022, 8, 1–13. [Google Scholar] [CrossRef]
- Rubel, L.; Reynolds, R.E. Cytologic description of squamous cell papilloma of the respiratory tract. Acta Cytol. 1979, 23, 227–231. [Google Scholar] [PubMed]
- Syrjänen, K.J. Condylomatous changes in neoplastic bronchial epithelium. Respiration 1979, 38, 299–304. [Google Scholar] [CrossRef]
- Syrjänen, K.J. Epithelial lesions suggestive of a condylomatous origin found closely associated with invasive bronchial squamous cell carcinomas. Respiration 1980, 40, 150–160. [Google Scholar] [CrossRef]
- Hu, Y.; Ren, S.; He, Y.; Wang, L.; Chen, C.; Tang, J.; Liu, W.; Yu, F. Possible Oncogenic Viruses Associated with Lung Cancer. Onco Targets Ther. 2020, 13, 10651–10666. [Google Scholar] [CrossRef]
- Xiong, W.M.; Xu, Q.P.; Li, X.; Xiao, R.D.; Cai, L.; He, F. The association between human papillomavirus infection and lung cancer: A system review and meta-analysis. Oncotarget 2017, 8, 96419–96432. [Google Scholar] [CrossRef]
- Hussen, B.M.; Ahmadi, G.; Marzban, H.; Azar, M.E.F.; Sorayyayi, S.; Karampour, R.; Nahand, J.S.; Hidayat, H.J.; Moghoofei, M. The role of HPV gene expression and selected cellular MiRNAs in lung cancer development. Microb. Pathog. 2021, 150, 104692. [Google Scholar] [CrossRef] [PubMed]
- Carpagnano, G.E.; Koutelou, A.; Natalicchio, M.I.; Martinelli, D.; Ruggieri, C.; Di Taranto, A.; Antonetti, R.; Carpagnano, F.; Foschino-Barbaro, M.P. HPV in exhaled breath condensate of lung cancer patients. Br. J. Cancer 2011, 105, 1183–1190. [Google Scholar] [CrossRef] [PubMed]
- Rezaei, M.; Shayan, M.; Aghaei, A.; Hosseini, N.; Darabi, H.; Nouri, M.; Etemadi, A.; O’ Neill, A.; Nahand, J.S.; Mirzaei, H.; et al. The association between HPV gene expression, inflammatory agents and cellular genes involved in EMT in lung cancer tissue. BMC Cancer 2020, 20, 916. [Google Scholar] [CrossRef]
- Yu, Y.; Yang, A.; Hu, S.; Yan, H. Correlation of HPV-16/18 infection of human papillomavirus with lung squamous cell carcinomas in Western China. Oncol. Rep. 2009, 21, 1627–1632. [Google Scholar] [CrossRef]
- Gaur, P.; Bhattacharya, S.; Kant, S.; Kushwaha, R.A.S.; Singh, G.; Pandey, S. EGFR Mutation Detection and Its Association With Clinicopathological Characters of Lung Cancer Patients. World J. Oncol. 2018, 9, 151–155. [Google Scholar] [CrossRef]
- Kumar, A.; Kumar, A. Non-small-cell lung cancer-associated gene mutations and inhibitors. Adv. Cancer Biol. Metastasis 2022, 6, 100076. [Google Scholar] [CrossRef]
- Harabajsa, S.; Šefčić, H.; Klasić, M.; Milavić, M.; Židovec Lepej, S.; Grgić, I.; Zajc Petranović, M.; Jakopović, M.; Smojver-Ježek, S.; Korać, P. Infection with human cytomegalovirus, Epstein-Barr virus, and high-risk types 16 and 18 of human papillomavirus in EGFR-mutated lung adenocarcinoma. Croat. Med. J. 2023, 64, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Deng, F.; Qian, L.T.; Meng, S.P.; Zhang, Y.; Shan, W.L.; Zhang, X.L.; Wang, B.L. Association between human papillomavirus and EGFR mutations in advanced lung adenocarcinoma. Oncol. Lett. 2016, 12, 1953–1958. [Google Scholar] [CrossRef] [PubMed]
- Karnosky, J.; Dietmaier, W.; Knuettel, H.; Freigang, V.; Koch, M.; Koll, F.; Zeman, F.; Schulz, C. HPV and lung cancer: A systematic review and meta-analysis. Cancer Rep. 2021, 4, e1350. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.; Pan, Z.; Cai, X.; Wang, W.; Guo, C.; He, J.; Chen, Y.; Liu, Z.; Wang, B.; He, J.; et al. The association between human papillomavirus presence and epidermal growth factor receptor mutations in Asian patients with non-small cell lung cancer. Transl. Lung Cancer Res. 2018, 7, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Zhai, K.; Ding, J.; Shi, H.Z. HPV and lung cancer risk: A meta-analysis. J. Clin. Virol. 2015, 63, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Argyri, E.; Tsimplaki, E.; Marketos, C.; Politis, G.; Panotopoulou, E. Investigating the role of human papillomavirus in lung cancer. Papillomavirus Res. 2017, 3, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Tsyganov, M.M.; Ibramigova, M.K.; Rodionov, E.O.; Cheremisina, O.V.; Miller, S.V.; Tuzikov, S.A.; Litvyakov, N.V. Human Papillomavirus in Non-Small Cell Lung Carcinoma: Assessing Virus Presence in Tumor and Normal Tissues and Its Clinical Relevance. Microorganisms 2023, 11, 212. [Google Scholar] [CrossRef] [PubMed]
- Coissard, C.J.; Besson, G.; Polette, M.C.; Monteau, M.; Birembaut, P.L.; Clavel, C.E. Prevalence of human papillomaviruses in lung carcinomas: A study of 218 cases. Mod. Pathol. 2005, 18, 1606–1609. [Google Scholar] [CrossRef]
- Syrjanen, K. Detection of human papillomavirus in lung cancer: Systematic review and meta-analysis. Anticancer Res. 2012, 32, 3235–3250. [Google Scholar]
- Hasegawa, Y.; Ando, M.; Kubo, A.; Isa, S.; Yamamoto, S.; Tsujino, K.; Kurata, T.; Ou, S.H.; Takada, M.; Kawaguchi, T. Human papilloma virus in non-small cell lung cancer in never smokers: A systematic review of the literature. Lung Cancer 2014, 83, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.W.; Chiou, H.L.; Sheu, G.T.; Hsieh, L.L.; Chen, J.T.; Chen, C.Y.; Su, J.M.; Lee, H. The association of human papillomavirus 16/18 infection with lung cancer among nonsmoking Taiwanese women. Cancer Res. 2001, 61, 2799–2803. [Google Scholar] [PubMed]
- Fei, Y.; Yang, J.; Hsieh, W.C.; Wu, J.Y.; Wu, T.C.; Goan, Y.G.; Lee, H.; Cheng, Y.W. Different human papillomavirus 16/18 infection in Chinese non-small cell lung cancer patients living in Wuhan, China. Jpn. J. Clin. Oncol. 2006, 36, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, A.; Jiang, R.; Pan, H.; Huang, B.; Lu, Y.; Wu, C. Human papillomavirus type 16 and 18 infection is associated with lung cancer patients from the central part of China. Oncol. Rep. 2008, 20, 333–339. [Google Scholar] [PubMed]
- Lin, F.C.; Huang, J.Y.; Tsai, S.C.; Nfor, O.N.; Chou, M.C.; Wu, M.F.; Lee, C.T.; Jan, C.F.; Liaw, Y.P. The association between human papillomavirus infection and female lung cancer: A population-based cohort study. Medicine 2016, 95, e3856. [Google Scholar] [CrossRef] [PubMed]
- Ragin, C.; Obikoya-Malomo, M.; Kim, S.; Chen, Z.; Flores-Obando, R.; Gibbs, D.; Koriyama, C.; Aguayo, F.; Koshiol, J.; Caporaso, N.E.; et al. HPV-associated lung cancers: An international pooled analysis. Carcinogenesis 2014, 35, 1267–1275. [Google Scholar] [CrossRef] [PubMed]
- Zafer, E.; Ergun, M.A.; Alver, G.; Sahin, F.I.; Yavuzer, S.; Ekmekci, A. Detection and Typing of Human Papillomavirus in Non-Small Cell Lung Cancer. Respiration 2004, 71, 88–90. [Google Scholar] [CrossRef] [PubMed]
- Kaya, H.; Kotiloğlu, E.; Inanli, S.; Ekicioğlu, G.; Bozkurt, S.U.; Tutkun, A.; Küllü, S. Prevalence of human papillomavirus (HPV) DNA in larynx and lung carcinomas. Pathologica 2001, 93, 531–534. [Google Scholar] [PubMed]
- Buyru, N.; Altinisik, J.; Isin, M.; Dalay, N. p53 codon 72 polymorphism and HPV status in lung cancer. Med. Sci. Monit. 2008, 14, CR493–CR497. [Google Scholar]
- Peña, N.; Carrillo, D.; Muñoz, J.P.; Chnaiderman, J.; Urzúa, U.; León, O.; Tornesello, M.L.; Corvalán, A.H.; Soto-Rifo, R.; Aguayo, F. Tobacco Smoke Activates Human Papillomavirus 16 p97 Promoter and Cooperates with High-Risk E6/E7 for Oxidative DNA Damage in Lung Cells. PLoS ONE 2015, 10, e0123029. [Google Scholar] [CrossRef]
- Li, Y.J.; Tsai, Y.C.; Chen, Y.C.; Christiani, D.C. Human papilloma virus anf female lung adenocarcinoma. Semin. Oncol. 2009, 36, 542–552. [Google Scholar] [CrossRef] [PubMed]
- Schabath, M.B.; Villa, L.L.; Lazcano-Ponce, E.; Salmerón, J.; Quiterio, M.; Giuliano, A.R.; HIM Study. Smoking and human papillomavirus (HPV) infection in the HPV in Men (HIM) study. Cancer Epidemiol. Biomark. Prev. 2012, 21, 102–110. [Google Scholar] [CrossRef]
- Baba, M.; Castillo, A.; Koriyama, C.; Yanagi, M.; Matsumoto, H.; Natsugoe, S.; Shuyama, K.Y.; Khan, N.; Higashi, M.; Itoh, T.; et al. Human papillomavirus is frequently detected in gefitinib-responsive lung adenocarcinomas. Oncol. Rep. 2010, 23, 1085–1092. [Google Scholar] [CrossRef] [PubMed]
- Hsu, N.Y.; Cheng, Y.W.; Chan, I.P.; Ho, H.C.; Chen, C.Y.; Hsu, C.P.; Lin, M.H.; Chou, M.C. Association between expression of human papillomavirus 16/18 E6 oncoprotein and survival in patients with stage I non-small cell lung cancer. Oncol. Rep. 2009, 21, 81–87. [Google Scholar]
- Tung, M.C.; Wu, H.H.; Cheng, Y.W.; Wang, L.; Chen, C.Y.; Yeh, S.D.; Wu, T.C.; Lee, H. Association of epidermal growth factor receptor mutations with human papillomavirus 16/18 E6 oncoprotein expression in non-small cell lung cancer. Cancer 2013, 119, 3367–3376. [Google Scholar] [CrossRef] [PubMed]
- Kato, T.; Koriyama, C.; Khan, N.; Samukawa, T.; Yanagi, M.; Hamada, T.; Yokomakura, N.; Otsuka, T.; Inoue, H.; Sato, M.; et al. EGFR mutations and human papillomavirus in lung cancer. Lung Cancer 2012, 78, 144–147. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.H.; Wu, J.Y.; Cheng, Y.W.; Chen, C.Y.; Lee, M.C.; Goan, Y.G.; Lee, H. cIAP2 upregulated by E6 oncoprotein via epidermal growth factor receptor/phosphatidylinositol 3-kinase/AKT pathway confers resistance to cisplatin in human papillomavirus 16/18-infected lung cancer. Clin. Cancer Res. 2010, 16, 5200–5210. [Google Scholar] [CrossRef] [PubMed]
- Psyrri, A.; Dimaio, D. Human papillomavirus in cervical and head-and-neck cancer. Nat. Clin. Pract. Oncol. 2008, 5, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Anantharaman, D.; Gheit, T.; Waterboer, T.; Halec, G.; Carreira, C.; Abedi-Ardekani, B.; McKay-Chopin, S.; Zaridze, D.; Mukeria, A.; Szeszenia-Dabrowska, N.; et al. No causal association identified for human papillomavirus infections in lung cancer. Cancer Res. 2014, 74, 3525–3534. [Google Scholar] [CrossRef]
- Lin, S.; Zhang, X.; Li, X.; Qin, C.; Zhang, L.; Lu, J.; Chen, Q.; Jin, J.; Wang, T.; Wang, F.; et al. Detection of human papillomavirus distinguishes second primary tumors from lung metastases in patients with squamous cell carcinoma of the cervix. Thorac. Cancer 2020, 11, 2297–2305. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | HPV Positive (n) | HPV Negative (n) | HPV and p16 Positive (n) | |
|---|---|---|---|---|
| Age (years) | ≤62 | 20 | 1 | 3 |
| >62 | 23 | 13 | 9 | |
| Gender | Female | 8 | 7 | 3 |
| Male | 35 | 7 | 9 | |
| Smoking history | Smoker | 25 | 9 | 6 |
| Non-smoker | 18 | 5 | 6 | |
| Histopathological diagnosis | Squamous cell carcinoma | 20 | 11 | 7 |
| Adenocarcinoma | 13 | 0 | 1 | |
| Other tumors | 6 | 0 | 4 | |
| Non-neoplastic | 4 | 3 | - * | |
| EGFR status | Wild type | 36 | 11 | 11 |
| Mutated | 3 | 0 | 1 | |
| Not applied | 4 | 3 | 0 | |
| HPV-Positive (n = 39) | HPV-Negative (n = 11) | p * | ||
|---|---|---|---|---|
| P16 | Positive | 12 (30.8) | 0 (0) | 0.05 |
| Negative | 27 (69.2) | 11 (100) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alikanoğlu, A.S.; Karaçay, İ.A. Detection of High-Risk Human Papillomavirus (HPV), p16 and EGFR in Lung Cancer: Insights from the Mediterranean Region of Turkey. Viruses 2024, 16, 1201. https://doi.org/10.3390/v16081201
Alikanoğlu AS, Karaçay İA. Detection of High-Risk Human Papillomavirus (HPV), p16 and EGFR in Lung Cancer: Insights from the Mediterranean Region of Turkey. Viruses. 2024; 16(8):1201. https://doi.org/10.3390/v16081201
Chicago/Turabian StyleAlikanoğlu, Arsenal Sezgin, and İrem Atalay Karaçay. 2024. "Detection of High-Risk Human Papillomavirus (HPV), p16 and EGFR in Lung Cancer: Insights from the Mediterranean Region of Turkey" Viruses 16, no. 8: 1201. https://doi.org/10.3390/v16081201
APA StyleAlikanoğlu, A. S., & Karaçay, İ. A. (2024). Detection of High-Risk Human Papillomavirus (HPV), p16 and EGFR in Lung Cancer: Insights from the Mediterranean Region of Turkey. Viruses, 16(8), 1201. https://doi.org/10.3390/v16081201