Abstract
The inactivated COVID-19 vaccine has demonstrated high efficacy in the general population through extensive clinical and real-world studies. However, its effectiveness in immunocompromised individuals, particularly those living with HIV (PLWH), remains limited. In this study, 20 PLWH and 15 HIV-seronegative individuals were recruited to evaluate the immunogenicity of an inactivated COVID-19 vaccine in PLWH through a prospective cohort study. The median age of the 20 PLWH and 15 HIV-seronegative individuals was 42 years and 31 years, respectively. Of the PLWH, nine had been on ART for over five years. The median anti-SARS-CoV-2 S-RBD IgG antibody level on d224 was higher than that on d42 (8188.7 ng/mL vs. 3200.9 ng/mL, P < 0.05). Following COVID-19 infection, the antibody level increased to 29,872.5 ng/mL on dre+90, 12.19 times higher than that on d300. Compared with HIV-seronegative individuals, the antibody level in PLWH was lower on d210 (183.3 ng/mL vs. 509.3 ng/mL, P < 0.01), while there was no difference after d224. The symptoms of COVID-19 infection in PLWH were comparable to those in HIV-seronegative individuals. In this study, the inactivated COVID-19 vaccine demonstrated good immunogenicity in PLWH. The protective benefit of booster vaccinations for PLWH cannot be ignored. Implementing a booster vaccination policy for PLWH is an effective approach to providing better protection against the COVID-19 pandemic.
1. Introduction
SARS-CoV-2 is the pathogen responsible for COVID-19. It primarily targets the respiratory system, resulting in mild infections. In severe cases, it can progress to acute respiratory distress syndrome, leading to multiple organ failure and mortality [1]. As of 12 April 2023, the COVID-19 pandemic has resulted in over 762 million confirmed cases and more than 6.897 million deaths worldwide [2]. Although several clinical trials [3,4,5] and real-world studies [6] have demonstrated the effectiveness of different vaccines against COVID-19 infection, these studies have not provided sufficient information on the immunogenicity of the vaccine in immunocompromised individuals. Some studies have assessed the immune response to COVID-19 vaccination in immunocompromised populations, particularly in individuals who have undergone solid organ transplantation [7], those receiving immunosuppressive therapy [8], individuals with multiple myeloma [9], and those with cancer [10]. However, limited research has evaluated the immunogenicity of inactivated COVID-19 vaccination in HIV-infected individuals, especially considering the significant impact of HIV infection on an individual’s immune status and behavior, as indicated in other diseases [11].
HIV infection is a leading cause of immunodeficiency worldwide, primarily destroying the immune system [12]. By the end of 2021, UNAIDS reported that approximately 38.4 million people were living with HIV [13]. In China, the cumulative number of people living with HIV (PLWH) was 1.223 million by the end of 2022 [14]. Guangxi is located in Southwest China, bordering Southeast Asia. Due to its unique geography and complex population movements, the HIV/AIDS epidemic in Guangxi remains serious, with reported cases ranking among the top three in China [15]. Additionally, PLWH experience higher rates of comorbidities and age-related illnesses [16]. A systematic review and meta-analysis of 22 studies found that PLWH had a 24% higher risk of SARS-CoV-2 infection and a 78% higher risk of mortality from COVID-19 compared to HIV-seronegative individuals [17]. PLWH face the dual challenge of HIV and COVID-19 infection, highlighting the urgent need for effective prevention and protection measures.
Studies have shown that patients with other immunodeficiency diseases, such as cancer [18] and rheumatism [19], can still produce high levels of anti-SARS-CoV-2 S-RBD IgG antibodies after receiving the COVID-19 vaccine. Many mRNA and adenoviral vector COVID-19 vaccines, such as the BNT162b2 COVID-19 mRNA vaccine [20,21,22] and the ChAdOx1 nCOVID-19 vaccine [4,23], were immunogenic and safe in PLWH. However, research on inactivated vaccines against COVID-19 remains relatively limited. It is worth investigating whether inactivated vaccines exhibit good immunogenicity in PLWH. A non-randomized cohort study conducted in Hubei Province provided preliminary evidence regarding the immunogenicity of inactivated vaccines in PLWH [24]. Furthermore, a subsequent cross-sectional study in Beijing supported these findings [25]. However, their study observed PLWH for only a short period after vaccination and did not track them from the time they were unvaccinated until they received all three doses of the vaccine or even after a COVID-19 infection. This limitation restricts the dynamic assessment of immune responses over time in PLWH.
Therefore, we selected a cohort of 20 PLWH undergoing antiretroviral therapy (ART) and 15 HIV-seronegative individuals as the control group for this study. We followed up with study subjects regularly from 20 July 2021 to 20 March 2023 and collected their samples at various time points after vaccination. We analyzed the dynamic changes in the levels of anti-SARS-CoV-2 S-RBD IgG antibodies produced by PLWH after receiving the inactivated COVID-19 vaccine to assess their immune response. At the same time, we evaluated the protective effect of a booster dose of the inactivated COVID-19 vaccine in PLWH by comparing IgG antibody levels between the PLWH group and the control group after administration of the booster dose and recovery from COVID-19 infection. Our study represents a pioneering prospective cohort investigation. This study comprehensively evaluates the immunogenicity of the inactivated COVID-19 vaccine in PLWH from pre-vaccination through post-vaccination completion. It provides a scientific basis for advocating the necessity of COVID-19 vaccination and booster doses in response to the COVID-19 pandemic and promotes the development and optimization of vaccination strategies for PLWH.
2. Methods
2.1. Ethics Statement
This study was approved by the Ethics and Human Subjects Committee (EHSC) of Guangxi Medical University (No. 20210153).
2.2. Study Subjects
With the help of the Guigang Center for Disease Control and Prevention, we recruited a cohort of 20 PLWH who met the predefined inclusion and exclusion criteria. The inclusion criteria were as follows: (1) age ≥ 18 years; (2) confirmed HIV-positive status; (3) absence of COVID-19 infection; and (4) duration of ART treatment ≥ 6 months. The exclusion criteria included: (1) major chronic diseases such as cardiac, renal, pulmonary, endocrine, metabolic, or autoimmune diseases; (2) concurrent infection with hepatitis B/C virus, syphilis, or tuberculosis; (3) hypersensitivity to vaccines and vaccine components; and (4) pregnancy or lactation. Additionally, we recruited 15 HIV-seronegative individuals as controls for this study to assess the effect of HIV infection status on the levels of antibodies produced by comparing the differences in antibody levels between the PLWH and controls. The HIV-seronegative individuals were required to be seronegative for HIV, following inclusion criteria (1) and (3) and the exclusion criteria above. All participants signed the informed consent forms.
2.3. Vaccine Information
In this study, subjects were vaccinated with the inactivated COVID-19 vaccine CoronaVac (Vero cells), developed by Beijing Sinovac Zhongwei Biotechnology Co., Ltd., and administered intramuscularly at 0.5 mL per dose. The vaccine was a killed whole virus vaccine, retaining its antigenicity to stimulate an immune response. The batch numbers of the three doses administered to PLWH were the first dose (Lot#: 202106031Z), the second dose (Lot#: 202107094Z), and the booster dose (Lot#: 202112116S). The batch numbers of the vaccine administered to the healthy control group were the first dose (Lot#: 202104010B), the second dose (Lot#: 202105056F), and the booster dose (Lot#: 202111221K).
2.4. Information Collection
Information regarding the study subjects, including demographic information such as age, occupation, marital status, the route of infection, ART regimens, and duration of treatment for PLWH, was obtained during the inclusion process, while height and weight were measured. The CD4+ T-cell counts of PLWH were obtained by labeling blood cells with anti-CD4-FITC and anti-CD3-PE, collecting the cells via flow cytometry, and gating the analysis to identify CD3+CD4+ lymphocytes, thereby calculating the absolute counts of CD4+ T-cells. The COVID-19 infection was detected by collecting nasopharyngeal or oropharyngeal swab samples for nucleic acid testing. A positive result indicated an active COVID-19 infection, while a negative result indicated that the subject was either not infected with COVID-19 or had recovered from it. Symptoms of the COVID-19 infection were collected via face-to-face questionnaires. Fever was defined as an axillary temperature exceeding 37.3 °C. Symptoms such as cough, sore throat, and headache were classified according to medical diagnostic criteria. In terms of infection status, “No symptoms” indicated the absence of any discomfort. “Mild symptoms” referred to conditions that had little impact on daily life and allowed patients to continue their activities, including a slight increase in body temperature (higher than normal but not meeting the criteria for fever), mild malaise or fatigue, and mild headache. “Ordinary symptoms” were more severe than mild symptoms, requiring patients to adjust daily activities but not hospitalization, and included persistent fever, noticeable dry cough, severe muscle or joint pain, headache, and sore throat. “Severe and critical symptoms” required hospitalization, medical intervention, and urgent medical care and included a high fever that did not subside, severe respiratory distress, significant hypoxemia, and respiratory failure.
2.5. Sample Collection
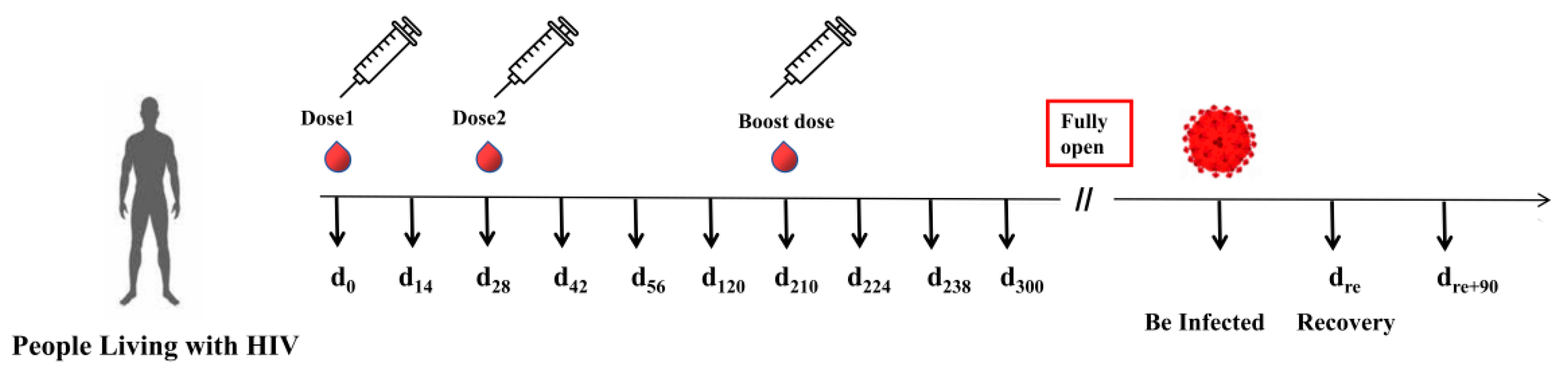
To investigate the dynamics of antibody production and durability in PLWH, we collected peripheral blood samples from participants at various time points. The first dose of the vaccine for PLWH was administered on 20 July 2021 (d0); the second dose was on 17 August 2021 (d28); and the booster dose was on 16 February 2022 (d210). Blood samples from PLWH were collected on the following days: prior to the first dose (d0), day 14 (d14), day 42 (d42), day 56 (d56), day 120 (d120), day 210 (d210), day 224 (d224), day 238 (d238), day 300 (d300), and day 90 after recovery from COVID-19 infection (dre+90) (Figure 1). In addition, we followed up with the control group and collected their blood samples on d210, d224, d238, d300, and dre+90.
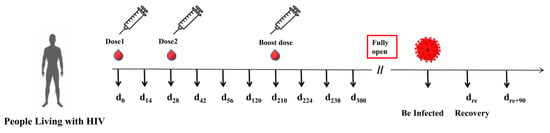
Figure 1.
Timeline of peripheral blood sample collection in the cohort of PLWH receiving the inactivated COVID-19 vaccine.
Protocol of the prospective cohort study: PLWH were recruited prior to vaccination and received three doses of the inactivated COVID-19 vaccine. Peripheral blood samples were collected at various time points: d0, d14, d42, d56, d120, d210, d224, d238, d300, and dre+90.
2.6. Plasma Separation
Peripheral blood samples were collected from study subjects via the antecubital vein using vacuum blood collection tubes containing EDTA at predetermined time points. Samples were promptly processed, and plasma was separated by centrifugation. Subsequently, the upper plasma portion was transferred into sterile 1.5 mL EP tubes, labeled, and stored at −80 °C for future testing.
2.7. Anti-SARS-CoV-2 S-RBD IgG Antibody Detection
All samples and reagents were equilibrated at room temperature for 30 min before the experiment. Based on preliminary testing, samples were diluted at various time points after vaccination with ratios ranging from 1:10 to 1:20,000. According to the provided instructions, each sample was tested in duplicate wells using commercial ELISA kits (Proteintech, Wuhan, China), which are commonly used to detect anti-SARS-CoV-2 S-RBD IgG antibodies and have been employed in several studies [26,27,28]. Absorbance values were measured at 450 nm and 630 nm using a microplate reader, and antibody concentration was determined based on these readings. A four-parameter logistic curve fit was used to establish the most appropriate standard curve, with an R2 ≥ 0.99 considered acceptable.
2.8. Statistical Analysis
Descriptive statistics were used to analyze the general characteristics of the study population. As the data did not follow a normal distribution, quantitative variables such as age and BMI were presented as medians and interquartile ranges (IQR), while categorical variables such as gender, ethnicity, and occupation were expressed as frequencies or percentages. The rank-sum test for randomized block design (Friedman’s test), adjusted for significance using the Bonferroni method, was employed to assess differences in IgG antibody concentrations at various time points. The Wilcoxon rank-sum test and Kruskal–Wallis H test were used to compare and analyze differences in different demographic characteristics and antibody levels between PLWH and HIV-seronegative individuals. A logistic regression analysis was conducted to explore the relationship between antibody levels and various demographic characteristics, with specific assignment instructions provided in Table S1. The odds ratio (OR), 95% confidence interval (CI), and P-value were used to identify potential influencing factors. Fisher’s exact test was employed to compare differences in categorical variables. Spearman’s rank correlation analysis was conducted to explore the relationship between IgG antibody concentration and the demographic characteristics of PLWH. Statistical analysis was performed using SPSS (version 26.0) software, and figures were created using GraphPad Prism 8. A significance level of P < 0.05 was considered statistically significant.
3. Results
3.1. Subject Characteristics
A total of 20 PLWH and 15 HIV-seronegative controls were included in this study. The PLWH group had a median age of 42 years (IQR: 37, 50), while the control group had a median age of 31 years (IQR: 29, 34). The median body mass index (BMI) for PLWH was 24.24 kg/m2 (IQR: 21.39, 27.24), while the BMI for the controls was 20.50 kg/m2 (IQR: 18.82, 22.04). There were statistically significant differences (P < 0.05) in gender, age, occupation, educational level, and BMI between the two groups. There were no statistically significant differences (P < 0.05) in ethnicity or marital status between the two groups (Table 1). For the PLWH group, the median baseline CD4+ T-cell count was 431.5 cells/μL (IQR: 381.25, 562.25). Additionally, 80% (16/20) of the patients had a CD4+ T-cell count above 350 cells/μL, 85% (17/20) acquired HIV through heterosexual transmission, 75% (15/20) were treated with a combination of NRTIs and NNRTIs, and 45% (9/20) had been undergoing treatment for more than 5 years.

Table 1.
Demographic characteristics at baseline in the PLWH and control groups.
3.2. The Conversion Rate of Anti-SARS-CoV-2 S-RBD IgG Antibodies after Vaccination Is Not Associated with Different Characteristics in PLWH
Several factors, including vaccine dosage, gender, age, and immunodeficiency, may influence the overall effectiveness of vaccination. In our study, 17 out of 20 PLWH (85%) demonstrated the production of anti-SARS-CoV-2 IgG antibodies within 14 days after receiving the second dose of the vaccine, classifying them as the IgG-positive group. However, the remaining three individuals (15%), referred to as the IgG-negative group, did not produce anti-SARS-CoV-2 IgG antibodies after receiving the second dose of the vaccine. Nonetheless, all three individuals underwent seroconversion and tested positive for IgG antibodies after receiving the third booster dose. Analysis of clinical characteristics between the IgG-positive and IgG-negative groups revealed no significant differences (P > 0.05) in gender, age, ethnicity, occupation, BMI, route of infection, CD4+ T-cell count, ART regimen, and duration of ART (Table 2).
Table 2.
Comparison of various characteristics between the IgG-positive and IgG-negative groups of PLWH after the second dose of the vaccine.
3.3. The Administration of a Booster Dose or Infection with COVID-19 after Vaccination Can Quickly Boost Antibody Titers in PLWH
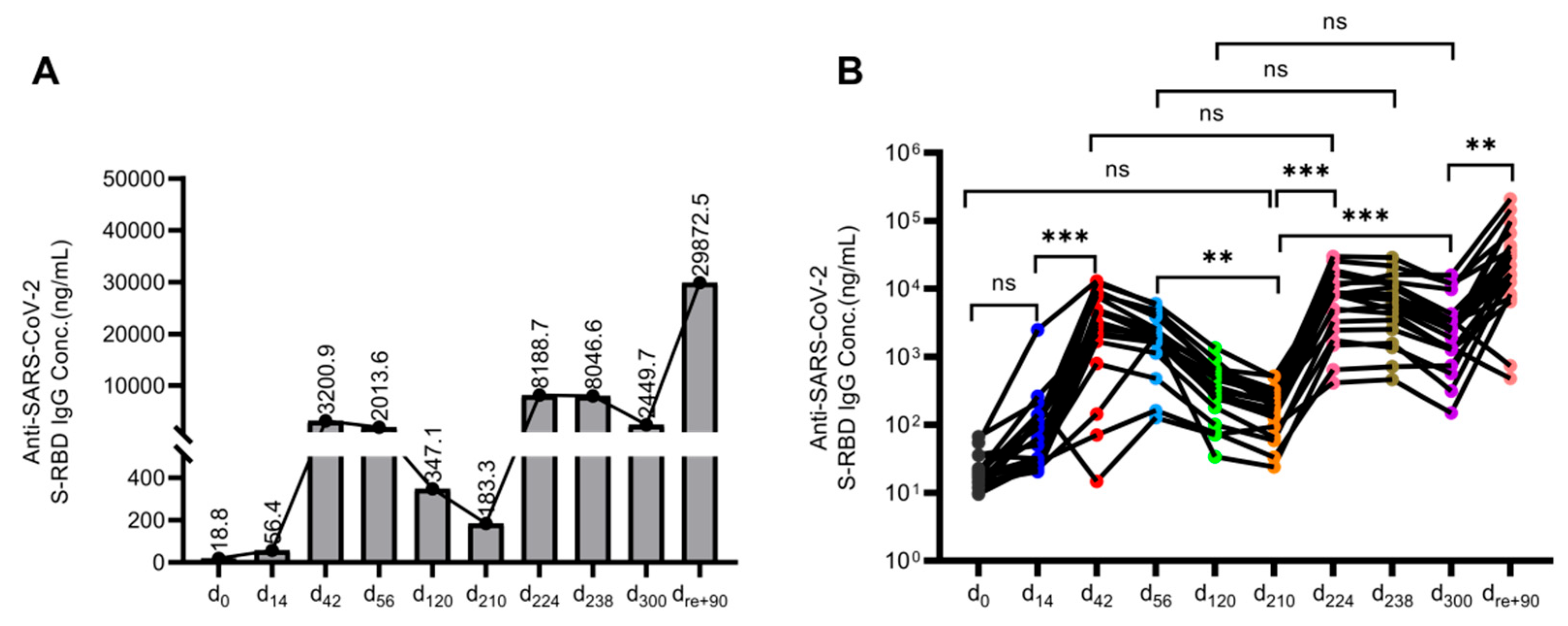
We observed a modest increase in IgG antibodies targeting the SARS-CoV-2 S-RBD region after the first vaccine dose in PLWH. However, following the second dose, the median IgG antibody concentration peaked at 3200.9 ng/mL on d42 and gradually declined over time (Figure 2A). By d56, d120, and d210, median antibody concentrations had decreased to 2013.6 ng/mL, 347.1 ng/mL, and 183.3 ng/mL, respectively. There was a statistically significant difference (P < 0.005) in antibody levels between d56 and d210. Remarkably, following the administration of the third booster dose, antibody concentrations on d224, d238, and d300 were 8188.7 ng/mL, 8046.6 ng/mL, and 2449.7 ng/mL, respectively. These values represented a 2.56-fold, 3.99-fold, and 7.06-fold increase compared to the levels observed on d42, d56, and d120, respectively. The antibody concentration showed a substantial 44.67-fold increase on d224 and a significant 13.36-fold increase on d300 (P < 0.001) compared to the levels on d210. Following the adjustment of COVID-19 prevention and control measures, the study population experienced successive infections. Notably, the median antibody concentration surged to 29,872.5 ng/mL on dre+90, representing a remarkable 12.19-fold increase compared to the level on d300 (P < 0.005) (Figure 2B).
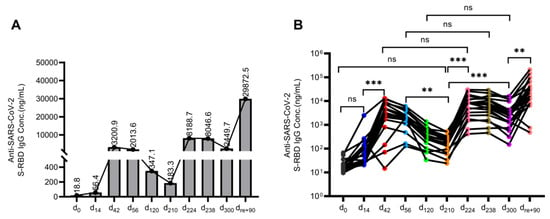
Figure 2.
Temporal dynamics of antibody levels in PLWH following inactivated COVID-19 vaccination. (A) Changes in median antibody concentration at different time points in PLWH after vaccination and COVID-19 infection. The dots represent median antibody concentrations. The value indicates the specific median antibody concentrations. (B) IgG antibody titers of individuals in PLWH are represented by dots. Antibody levels were compared at different time points after vaccination and recovery from the COVID-19 infection using Friedman’s test. The Bonferroni method was used to adjust the test size. P′ < 0.005 was considered statistically significant. ** P′ < 0.005, *** P′ < 0.001, and “ns” indicates no statistical difference.
3.4. The Antibody Levels in PLWH after Vaccination or COVID-19 Infection Are Not Influenced by Various Characteristics
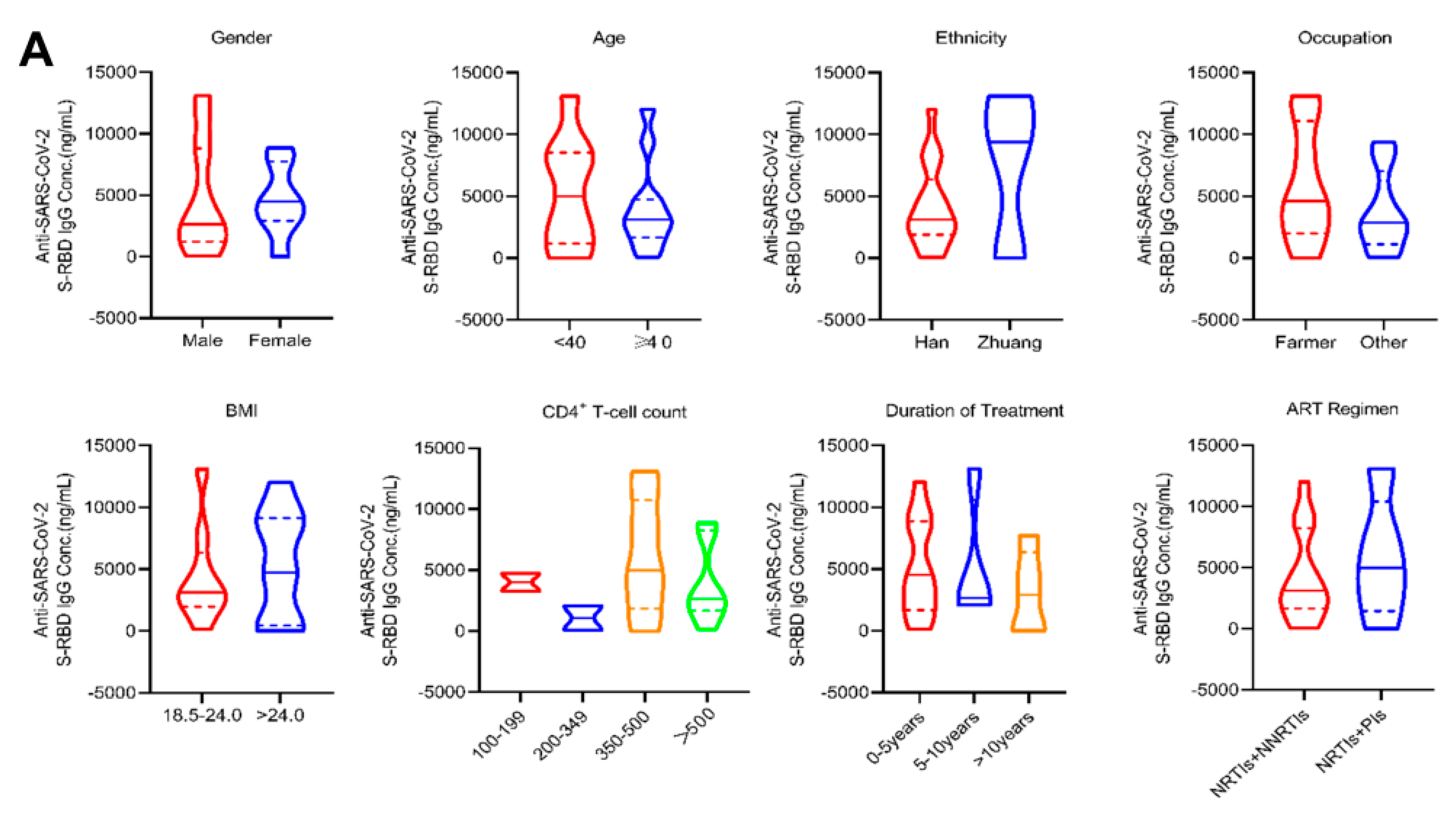
The analysis of various demographic and clinical characteristics among PLWH in terms of antibody levels after vaccination showed no significant differences in gender, age, ethnicity, occupation, BMI, CD4+ T-cell count, duration of treatment, or ART regimen (P > 0.05) (Figure 3A). Furthermore, the correlation analysis for age, BMI, CD4+ T-cell count, and antibody concentration revealed no significant correlations (P > 0.05) (Figure 3B).
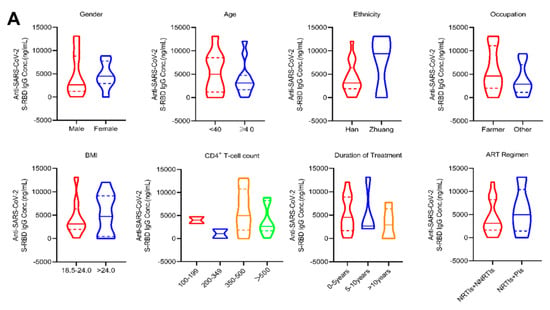
Figure 3.
Antibody levels in PLWH with different characteristics after the second dose of vaccination and the COVID-19 infection. (A,C) The violin plots show the differences in antibody levels by gender, age, ethnicity, occupation, BMI, CD4+ T-cell count, duration of treatment, and the ART regimen in PLWH on d42 (A) and dre+90 (C); (B,D) Correlation analysis between age, BMI, CD4+ T-cell count, duration of treatment, and antibody levels in PLWH on d42 (B) and dre+90 (D). (E) The line chart shows changes in antibody levels of the individual with the lowest CD4+ T-cell count and in the median antibody levels in PLWH. Comparison of antibody levels with different characteristics was conducted using the Wilcoxon rank-sum test and the Kruskal–Wallis H test. Correlation analysis was performed using Spearman’s rank correlation. Only P-values indicating a significant difference were marked.
Following COVID-19 infection in PLWH, no significant differences in antibody concentrations were observed based on gender, age, ethnicity, occupation, BMI, CD4+ T-cell count, duration of treatment, and the ART regimen (P > 0.05) (Figure 3C). Correlation analysis demonstrated a significant negative correlation between the duration of treatment and antibody concentration, as indicated by Spearman’s rank correlation coefficient (rs = −0.6143, P = 0.0102). A longer duration of treatment was associated with a more stable level of antibody production in response to SARS-CoV-2 stimulation. The correlation analysis also included age, BMI, and CD4+ T-cell count, but no significant correlations were observed (P > 0.05) (Figure 3D). Additionally, we compared the post-vaccination antibody levels of the individual with the lowest CD4+ T-cell count (151 cells/μL) to the median antibody levels in PLWH. It was found that the individual’s antibody levels approached or even exceeded the median levels (Figure 3E).
3.5. PLWH Can Produce Antibody Levels Similar to Those of HIV-Seronegative Individuals after a Booster Vaccine and Following Infection
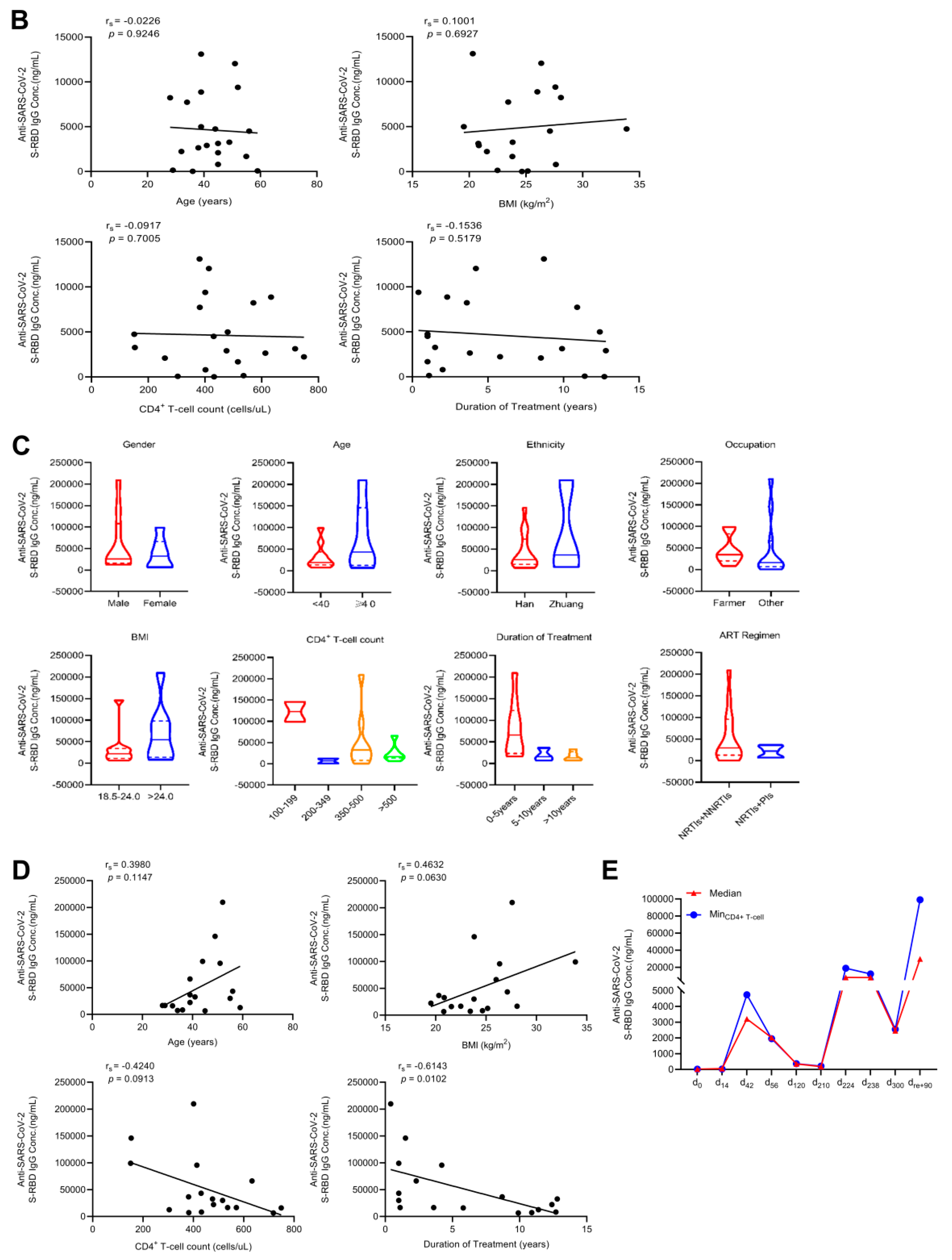
We compared the antibody levels on d210 as well as on d224, d238, d300, and dre+90 between PLWH and the controls. After the booster dose, the antibody level in PLWH increased significantly to 8188.7 ng/mL on d224, representing a 44.67-fold increase from 183.3 ng/mL on d210. Furthermore, the antibody concentration of dre+90 was 29,872.5 ng/mL, which was 12.19 times higher than the concentration of d300 at 2449.7 ng/mL. In the control group, the average antibody concentration on d210 was 509.3 ng/mL. This concentration increased significantly to 9411.1 ng/mL on d224, representing an 18.49-fold increase from d210. On dre+90, the mean antibody concentration was 20,986.3 ng/mL, a 3.90-fold increase compared to the level on d300 (5385.7 ng/mL). Notably, the median antibody concentration of PLWH on dre+90 was slightly higher than that in the control group. This observation may be attributed to the immune system of PLWH, which enables a rapid and robust antibody response upon encountering viral stimulation. Additionally, the median antibody concentration in the controls on d210 was 509.3 ng/mL, 2.78 times higher than that in PLWH, which was 183.3 ng/mL (P < 0.01). However, there were no significant differences in antibody levels between PLWH and controls on d224, d238, d300, or dre+90 (Figure 4).
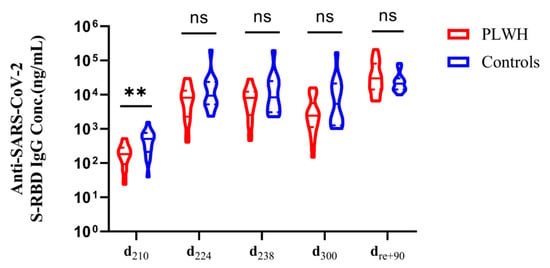
Figure 4.
Antibody levels in PLWH and controls following booster vaccination and COVID-19 infection. The violin plots illustrate the comparative analysis of antibody levels in PLWH and controls after administering the booster vaccine and COVID-19 infection, as assessed by the Wilcoxon rank sum test. ** P < 0.01, and “ns” indicates no statistical difference.
The results may be influenced by potential confounding factors, such as age and BMI. Consequently, the 35 subjects were divided into two groups based on their total average antibody concentrations: low concentration and high concentration. A logistic regression analysis was used to explore the association between antibody concentrations and various demographic characteristics. The results demonstrated that age, BMI, and other factors had no significant impact on antibody concentration (P > 0.05) (Table S2). It was observed that PLWH could achieve protective antibody levels comparable to those of the controls after receiving the booster dose and the COVID-19 infection. In other words, PLWH benefit significantly from the booster dose and COVID-19 infection in terms of antibody production.
3.6. PLWH with COVID-19 Infection Exhibit That Are Comparable to or Milder than Those in HIV-Seronegative Individuals
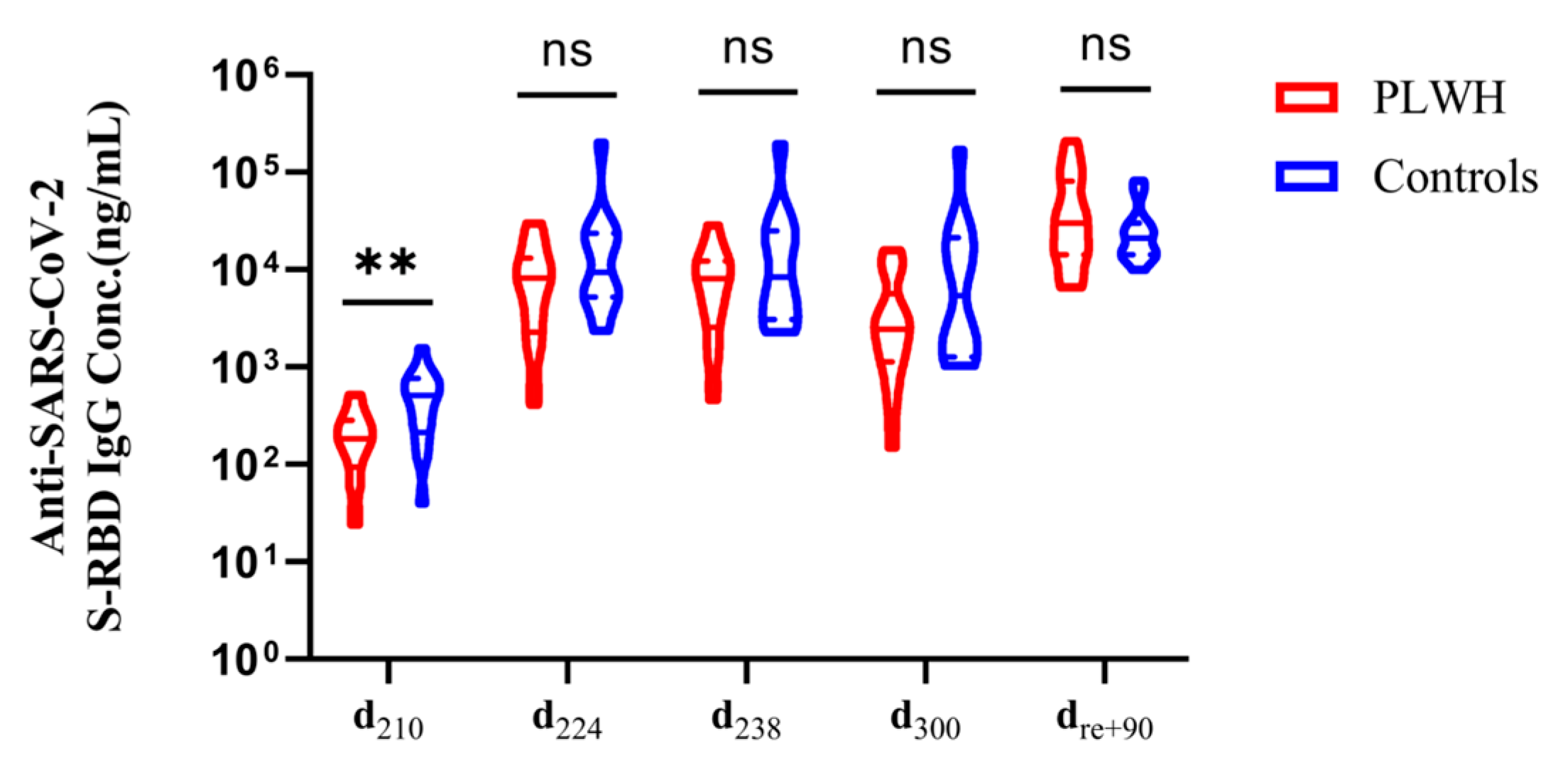
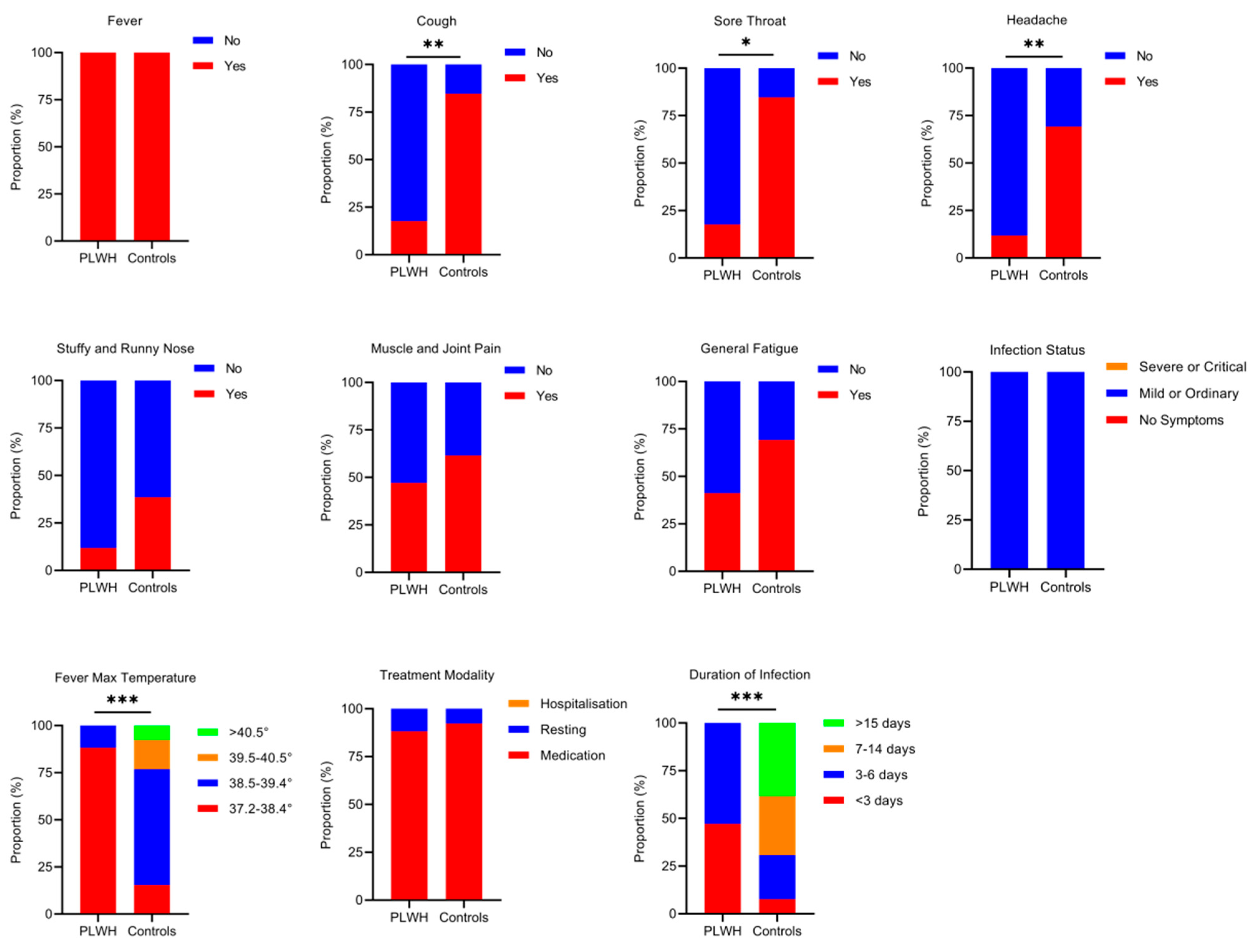
After adjusting the national epidemic prevention and control measures, 17 out of 20 PLWH and 13 out of 15 HIV-seronegative individuals were found to be infected with SARS-CoV-2 in this study. To assess potential differences in symptom severity between PLWH and the controls following COVID-19 infection, we distributed 30-point questionnaires, achieving a 100% response rate with 30 completed questionnaires. The 30 study subjects, including both PLWH and controls, exhibited mild to ordinary symptoms of COVID-19 infection. No fatalities or hospitalization occurred; instead, they were able to recover at home with rest and medication. The symptoms of infection were similar in both groups. There were no significant differences in symptoms, such as fever, stuffy and runny nose, muscle and joint pain, and general fatigue (P > 0.05). However, controls exhibited a higher proportion of symptoms, including cough, sore throat, and headache, compared to PLWH. Additionally, controls showed significantly higher values for maximum fever temperature and duration of infection (P < 0.05) (Figure 5).
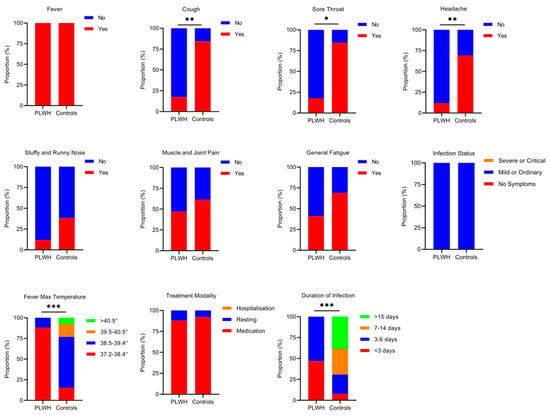
Figure 5.
Symptoms of COVID-19 infection in PLWH and the controls. The differences in COVID-19 symptoms between PLWH and controls were analyzed using Fisher’s exact test. The size of the colored squares represents the proportion of various symptoms. Only P-values indicating a significant difference are marked. * P < 0.05, ** P < 0.01; *** P < 0.001.
4. Discussion
Our study is the first long-term prospective cohort study to track immunogenicity from pre-vaccination through post-COVID-19 recovery. Based on the observed trend in anti-SARS-CoV-2 S-RBD IgG antibody levels in PLWH following inactivated COVID-19 vaccination and infection, our results demonstrated that PLWH exhibited robust immunogenicity in response to the vaccine, with no significant differences in antibody levels observed across various characteristics. Although the level of protective antibodies decreased over time, PLWH who received a booster dose and were subsequently infected with COVID-19 experienced a significant increase in antibody levels. Our study provides new evidence supporting the efficacy of the inactivated COVID-19 vaccine in PLWH.
As of 30 March 2023, there are 199 COVID-19 vaccines in preclinical development and 183 in clinical development worldwide [29]. In China, two inactivated vaccines, the Corona Vac vaccine and the BBIBP-CorV vaccine, have been widely used and show satisfactory immunogenicity in the general population [30,31]. A non-randomized cohort study by Yanmeng Feng [24] found that the HIV-1 viral load among PLWH decreased significantly after BBIBP-CorV vaccination, and their immune responses were comparable to those of healthy individuals. Another single-center study reported serological conversion rates of 94.1%, 99.8%, and 98.6% for PLWH receiving ART after the first, second, and third doses of the BNT162b2 COVID-19 mRNA vaccine, respectively, indicating good immunogenicity [20]. Our study found that the plasma antibody conversion rate in PLWH 14 days after receiving the second dose was 85%, which was lower than the 98% conversion rate reported for healthy individuals receiving the inactivated vaccine during the Phase II clinical trial. The difference may be due to lower immunity and a reduced humoral response to the vaccine in PLWH compared to healthy individuals, or it could result from variations in testing methods. Notably, the antibody conversion rate in PLWH increased to 100% after administration of the booster dose, highlighting the importance of booster vaccination for immunocompromised individuals.
The ideal outcome of vaccination is the development of long-lasting and highly effective protective antibodies, which establish high levels of population immunity and help control the COVID-19 pandemic [32]. However, evidence suggests that PLWH may experience a diminished or shorter duration of vaccine response [33]. Therefore, long-term follow-up studies are needed to assess the persistence of the vaccine response in PLWH. Studies have demonstrated that, 6 months after vaccination, most PLWH still maintain measurable immune responses, which are greater than their pre-vaccination baseline but show evidence of a decline in both humoral and cell-mediated immunity [34]. A booster dose is needed to maintain long-term memory against the SARS-CoV-2 variant. A study published in The Lancet found that, among healthy adults aged 18–59 years, the initial neutralizing antibody response to two doses of CoronaVac declined to near or below the lower limit of seropositivity after 6 months. A third dose of CoronaVac administered 8 months after the second dose resulted in a strong boost in immunity, effectively enhancing the validity, breadth, and likely duration of the memory response to SARS-CoV-2. Compared with the antibody titers 28 days after the second dose, the neutralizing antibody titers had increased approximately three to five times [35]. The detailed immune mechanism underlying the exponential increase in antibody levels following a long-term interval between the second and third doses was determined previously [5]. In our study, similar results were observed in PLWH, where anti-SARS-CoV-2 S-RBD IgG antibodies returned to baseline levels comparable to those observed before vaccination 6 months after the second dose. Antibody concentrations increased significantly 28 days after the booster dose, reaching levels 3.48 times higher than those observed 28 days after the second dose. The booster dose in PLWH not only elevated the conversion rate but also augmented antibody levels.
In addition, our study found that the antibody levels of PLWH 3 months after COVID-19 recovery were significantly higher, showing a 10.86-fold increase compared to those 3 months after the booster dose. Jennifer M. Dan and her team [36] analyzed immune memory to SARS-CoV-2 in 188 COVID-19 cases and found that 88% of subjects were RBD IgG seropositive 6–8 months after out of symptom. Various studies have indicated that patients who recover from COVID-19 may develop longer-lasting protective antibodies and T cells [37]. Research by Goel Rishi R et al. [38] also showed that individuals who had not been infected by SARS-CoV-2 required two doses of vaccine to achieve optimal increases in antibodies. Conversely, those who had recovered from COVID-19 could only need a single dose to achieve peak antibody and memory B cell responses, with antibody levels comparable to those of uninfected individuals who had received two doses of the COVID-19 vaccine. This suggests that natural infection with COVID-19 can induce the production of higher titers of more persistent neutralizing antibodies compared to the inactivated COVID-19 vaccine.
Studies have shown that PLWH may have an impaired immune status, potentially leading to inadequate vaccine-induced immune responses [39,40]. However, growing evidence suggests that PLWH develop a humoral immune response to the vaccine similar to that of the general population. A randomized, double-blind, controlled trial conducted in South Africa demonstrated that PLWH exhibited good immunogenicity after receiving the COVID-19 vaccine, with RBD-binding IgG and SARS-CoV-2 neutralizing response patterns comparable to those of HIV-negative, SARS-CoV-2 naive individuals following two doses of the vaccine [23]. John Frater [41] also noted that PLWH, who responded well to ART, did not exhibit significant differences in serological and cell-mediated immune responses compared to HIV-negative individuals after receiving two doses of the vaccine. Our study yielded similar results, with no difference in antibody levels between the two groups after receiving a booster dose and recovering from COVID-19 infection.
Some studies indicated that factors such as age [42], sex [43], and CD4+ T-cell counts [25] were related to differences in immune responses to vaccines. Nonetheless, our long-term follow-up study revealed that PLWH aged 18–59 years with varying CD4+ T-cell counts demonstrated a good humoral immune response 14 days after the second dose, with no significant difference in antibody levels produced. Moreover, no significant differences were observed in the levels of S-RBD IgG antibodies among PLWH after two doses of vaccine with respect to gender, age, ethnicity, occupation, BMI, ART regimens, and duration of ART (P > 0.05). Logistic regression analysis also showed no significant correlation between the various demographic characteristics and antibody levels. Soto-Nava et al. found no associations between SARS-CoV-2 neutralization and HIV-related variables (CD4+ T-cell counts, viral load, number of years in viral suppression, ART regimen) in multivariable analysis [44]. These results suggested that various demographic factors had a minimal impact on IgG antibody levels, indicating that PLWH with different immune statuses can achieve equivalent benefits after receiving the inactivated COVID-19 vaccine. However, there was a negative correlation between the antibody level on dre+90 and the duration of treatment. This may be because PLWH with a long treatment period were more likely to have a longer duration of HIV infection and exhibit poorer immune function, thereby impacting the antibody levels produced after vaccination.
Furthermore, we investigated the differences in symptoms during COVID-19 infection between PLWH and HIV-seronegative individuals. Our findings revealed that fever, cough, and fatigue remained prevalent symptoms of COVID-19 infection after vaccination, similar to those observed in the SARS-CoV-2 infection without vaccination [45]. The controls exhibited a higher proportion of symptoms, including cough, sore throat, and headache, compared to PLWH. This difference may be attributed to the relatively late timing of vaccination in PLWH, particularly the shorter interval between the booster vaccination and COVID-19 infection, suggesting a more pronounced protective effect of the vaccine. In contrast, the controls were vaccinated earlier and experienced a greater decline in pre-infection antibodies, leading to an increased incidence of COVID-19 symptoms. Remarkably, none of the PLWH experienced any exacerbations of AIDS due to the COVID-19 infection. After the COVID-19 infection, the symptoms of PLWH were comparable to those of the controls. There were no fatalities or hospitalizations, and recovery was achieved through self-administered medication, home monitoring, and rest. However, a cohort study showed that HIV infection was an independent prognostic factor for poor outcomes of COVID-19 infection, suggesting that PLWH with low CD4+ T-cell counts experience a more severe COVID-19 clinical course than those who are HIV-seronegative [46]. It is important to note that some studies have not found a direct association between HIV status and COVID-19 severity but instead highlight the critical role of comorbidities in determining COVID-19 outcomes. A case-control study in Spain found that hospitalized PLWH had a higher risk of death compared to HIV-seronegative individuals, primarily related to the presence of comorbidities rather than virological, immunological, or ART factors [47]. Inciarte’s study also showed that the clinical presentation, severity rate, and mortality of PLWH with COVID-19 infection were not dependent on any HIV-related or ART-related factors [48]. In our study, none of the PLWH reported significant comorbidities and developed protective antibodies after vaccination, which may explain their milder symptoms after COVID-19 infection and also highlight the good immunogenicity and protective effect of the inactivated vaccine in PLWH. This suggests that the inactivated COVID-19 vaccine offers similar protection to both PLWH and HIV-seronegative individuals. Fatima Samar’s study also indicated that non-vaccinated SARS-CoV-2 patients experienced significantly more intensive care hospitalizations and higher mortality than fully vaccinated patients [49], which is consistent with our findings. In other words, even though the antibody titers gradually decline following vaccination, the immune response can be rapidly recalled upon subsequent viral stimulation to prevent disease progression.
This study has several limitations. Firstly, the sample size was small and did not include PLWH aged 60 years and older. Additionally, we did not collect certain data on PLWH, such as viral loads, which may influence antibody titers. Secondly, the use of questionnaires could not eliminate recall bias, as symptom information was gathered 3 months after the subjects had recovered from COVID-19. Thirdly, the HIV-seronegative individuals did not match with the PLWH group in terms of demographic information, leading to discrepancies in several variables.
In conclusion, the inactivated COVID-19 vaccine demonstrates good immunogenicity in PLWH. The immune responses produced by PLWH after vaccination and COVID-19 infection are comparable to those in healthy individuals. Although the antibody-positive conversion rate is slightly lower and the persistence of protective antibodies in PLWH is poor, they can be recalled with a booster dose of the vaccine. Therefore, implementing a booster dose vaccination strategy in PLWH is crucial to enhancing the protection of the immunocompromised population against worsening AIDS progression.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/v16091481/s1, Table S1: Assignment description of logistic regression analysis; Table S2: A multivariate logistic regression model of antibody concentration and demographic characteristics.
Author Contributions
J.J., H.L. and L.Y. supervised the study. Y.W., X.W. and Y.H. contributed equally to the study. J.J., H.L., L.Y., W.J.L., Y.W. and X.W. contributed to the protocol and design of the study. Y.H., R.C., Y.X., W.W., F.Q. and J.L. (Jie Liu) recruited study subjects and collected blood samples. Y.W., X.W., X.C., L.W., M.S., T.Q., Y.L., B.L. and X.T. performed the experiments and collected data. C.W., S.C. and J.L. (Jinmiao Li) performed the data analysis and icon production. W.W., Z.Y. and J.S. conducted data verification and chart production guidance. Y.W., X.W. and R.C. drafted the manuscript. F.Q. and W.J.L. proposed revisions to the manuscript. J.J., H.L. and L.Y. made critical revisions to the manuscript. All authors contributed to the interpretation of data. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by the Guangxi Science and Technology Base and Talent Project (Guike AD21220013), the Guangxi Medical University Training Program for Young Leading Talents (to Jiang Junjun), and the Innovation Project of Guangxi Graduate Education (YCSW2023247).
Institutional Review Board Statement
This study was approved by the Ethics and Human Subjects Committee (EHSC) of Guangxi Medical University (No. 20210153).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All data from this study are included in this manuscript and are available from the primary contract (Junjun Jiang, Email: jiangjunjun@gxmu.edu.cn) upon request.
Acknowledgments
This study was supported by the Guangxi Science and Technology Base and Talent Project (Guike AD21220013), the Guangxi Medical University Training Program for Young Leading Talents (to Jiang Junjun), and the Innovation Project of Guangxi Graduate Education (YCSW2023247). The funder has no role in study design, sample collection, data analysis, manuscript grafting, or publication decisions. We also would like to thank the Guigang Center for Disease Control and Prevention for their help in collecting blood samples. Thanks to everyone for their support and assistance with this study.
Conflicts of Interest
The authors have declared that no competing interests exist.
References
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and Clinical Characteristics of 99 Cases of 2019 Novel Coronavirus Pneumonia in Wuhan, China: A Descriptive Study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Coronavirus (COVID-19) Dushboard. 2023. Available online: https://covid19.who.int/ (accessed on 12 April 2023).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and Efficacy of the ChAdOx1 nCoV-19 Vaccine (AZD1222) against SARS-CoV-2: An Interim Analysis of Four Randomised Controlled Trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.; Zhao, Y.; Huang, F.; Yang, Y.; Huang, Y.; Zhuang, Z.; Wang, Y.; Wang, Z.; Lin, X.; Zheng, Y.; et al. Immune Response and Homeostasis Mechanism Following Administration of BBIBP-CorV SARS-CoV-2 Inactivated Vaccine. Innovation 2023, 4, 100359. [Google Scholar] [CrossRef]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA COVID-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Antibody Response to 2-Dose SARS-CoV-2 mRNA Vaccine Series in Solid Organ Transplant Recipients. JAMA 2021, 325, 2204–2206. [Google Scholar] [CrossRef]
- Geisen, U.M.; Berner, D.K.; Tran, F.; Sümbül, M.; Vullriede, L.; Ciripoi, M.; Reid, H.M.; Schaffarzyk, A.; Longardt, A.C.; Franzenburg, J.; et al. Immunogenicity and Safety of Anti-SARS-CoV-2 mRNA Vaccines in Patients with Chronic Inflammatory Conditions and Immunosuppressive Therapy in a Monocentric Cohort. Ann. Rheum. Dis. 2021, 80, 1306–1311. [Google Scholar] [CrossRef]
- Bird, S.; Panopoulou, A.; Shea, R.L.; Tsui, M.; Saso, R.; Sud, A.; West, S.; Smith, K.; Barwood, J.; Kaczmarek, E.; et al. Response to First Vaccination against SARS-CoV-2 in Patients with Multiple Myeloma. Lancet Haematol. 2021, 8, e389–e392. [Google Scholar] [CrossRef]
- Monin, L.; Laing, A.G.; Muñoz-Ruiz, M.; McKenzie, D.R.; Del Molino Del Barrio, I.; Alaguthurai, T.; Domingo-Vila, C.; Hayday, T.S.; Graham, C.; Seow, J.; et al. Safety and Immunogenicity of One Versus Two Doses of the COVID-19 Vaccine BNT162b2 for Patients with Cancer: Interim Analysis of a Prospective Observational Study. Lancet Oncol. 2021, 22, 765–778. [Google Scholar] [CrossRef]
- Liu, W.J.; Hu, H.Y.; Su, Q.D.; Zhang, Z.; Liu, Y.; Sun, Y.L.; Yang, X.D.; Sun, D.P.; Cai, S.J.; Yang, X.X.; et al. HIV Prevalence in Suspected Ebola Cases during the 2014-2016 Ebola Epidemic in Sierra Leone. Infect. Dis. Poverty 2019, 8, 15. [Google Scholar] [CrossRef]
- Marcello, A. Latency: The Hidden HIV-1 Challenge. Retrovirology 2006, 3, 7. [Google Scholar] [CrossRef] [PubMed]
- UNAIDS. Global HIV & AIDS Statistics—Face Sheet. 2022. Available online: https://www.unaids.org/en/resources/fact-sheet (accessed on 12 March 2023).
- Han, M.J. Analysis of the epidemic situation and prospects of HIV/AIDS prevention and control in China. Chin. J. AIDS STD 2023, 29, 247–250. [Google Scholar] [CrossRef]
- Qiao, Y.C.; Xu, Y.; Jiang, D.X.; Wang, X.; Wang, F.; Yang, J.; Wei, Y.S. Epidemiological Analyses of Regional and Age Differences of HIV/AIDS Prevalence in China, 2004–2016. Int. J. Infect. Dis. 2019, 81, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Rajasuriar, R.; Crane, H.M.; Semeere, A.S. Growing Older with HIV in the Treat-All Era. J. Int. AIDS Soc. 2022, 25 (Suppl. 4), e25997. [Google Scholar] [CrossRef] [PubMed]
- Ssentongo, P.; Heilbrunn, E.S.; Ssentongo, A.E.; Advani, S.; Chinchilli, V.M.; Nunez, J.J.; Du, P. Epidemiology and Outcomes of COVID-19 in HIV-Infected Individuals: A Systematic Review and Meta-Analysis. Sci. Rep. 2021, 11, 6283. [Google Scholar] [CrossRef] [PubMed]
- Palich, R.; Veyri, M.; Marot, S.; Vozy, A.; Gligorov, J.; Maingon, P.; Marcelin, A.G.; Spano, J.P. Weak Immunogenicity after a Single Dose of SARS-CoV-2 mRNA Vaccine in Treated Cancer Patients. Ann. Oncol. 2021, 32, 1051–1053. [Google Scholar] [CrossRef]
- Ruddy, J.A.; Connolly, C.M.; Boyarsky, B.J.; Werbel, W.A.; Christopher-Stine, L.; Garonzik-Wang, J.; Segev, D.L.; Paik, J.J. High Antibody Response to Two-Dose SARS-CoV-2 Messenger RNA Vaccination in Patients with Rheumatic and Musculoskeletal Diseases. Ann. Rheum. Dis. 2021, 80, 1351–1352. [Google Scholar] [CrossRef]
- Milano, E.; Ricciardi, A.; Casciaro, R.; Pallara, E.; De Vita, E.; Bavaro, D.F.; Larocca, A.M.V.; Stefanizzi, P.; Tafuri, S.; Saracino, A. Immunogenicity and Safety of the BNT162b2 COVID-19 mRNA Vaccine in PLWH: A Monocentric Study in Bari, Italy. J. Med. Virol. 2022, 94, 2230–2236. [Google Scholar] [CrossRef]
- Levy, I.; Wieder-Finesod, A.; Litchevsky, V.; Biber, A.; Indenbaum, V.; Olmer, L.; Huppert, A.; Mor, O.; Goldstein, M.; Levin, E.G.; et al. Immunogenicity and Safety of the BNT162b2 mRNA COVID-19 Vaccine in People Living with HIV-1. Clin. Microbiol. Infect. 2021, 27, 1851–1855. [Google Scholar] [CrossRef]
- Skowronski, D.M.; De Serres, G. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2021, 384, 1576–1577. [Google Scholar] [CrossRef]
- Madhi, S.A.; Koen, A.L.; Izu, A.; Fairlie, L.; Cutland, C.L.; Baillie, V.; Padayachee, S.D.; Dheda, K.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and Immunogenicity of the ChAdOx1 nCoV-19 (AZD1222) Vaccine against SARS-CoV-2 in People Living with and without HIV in South Africa: An Interim Analysis of a Randomised, Double-Blind, Placebo-Controlled, Phase 1B/2A Trial. Lancet HIV 2021, 8, e568–e580. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Zhang, Y.; He, Z.; Huang, H.; Tian, X.; Wang, G.; Chen, D.; Ren, Y.; Jia, L.; Wang, W.; et al. Immunogenicity of an Inactivated SARS-CoV-2 Vaccine in People Living with HIV-1: A Non-Randomized Cohort Study. EClinicalMedicine 2022, 43, 101226. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Han, J.; Li, X.; Chen, D.; Zhao, X.; Qiu, Y.; Zhang, L.; Xiao, J.; Li, B.; Zhao, H. COVID-19 Vaccination in People Living with HIV (Plwh) in China: A Cross Sectional Study of Vaccine Hesitancy, Safety, and Immunogenicity. Vaccines 2021, 9, 1458. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.C.; Hsu, W.T.; Chiu, C.H.; Chang, F.Y.; Lo, H.R.; Liao, C.Y.; Yang, H.I.; Chou, Y.C.; Tsai, C.H.; Chao, Y.C. An Integrated Platform for Serological Detection and Vaccination of COVID-19. Front. Immunol. 2021, 12, 771011. [Google Scholar] [CrossRef] [PubMed]
- Asashima, H.; Mohanty, S.; Comi, M.; Ruff, W.E.; Hoehn, K.B.; Wong, P.; Klein, J.; Lucas, C.; Cohen, I.; Coffey, S.; et al. PD-1(High)CXCR5(-)CD4(+) Peripheral Helper T Cells Promote CXCR3(+) Plasmablasts in Human Acute Viral Infection. Cell Rep. 2023, 42, 111895. [Google Scholar] [CrossRef]
- Wang, Y.C.; Tsai, C.H.; Wang, Y.C.; Yen, L.C.; Chang, Y.W.; Sun, J.R.; Lin, T.Y.; Chiu, C.H.; Chao, Y.C.; Chang, F.Y. SARS-CoV-2 Nucleocapsid Protein, Rather than Spike Protein, Triggers a Cytokine Storm Originating from Lung Epithelial Cells in Patients with COVID-19. Infection 2023, 52, 955–983. [Google Scholar] [CrossRef]
- WHO. COVID-19 Vaccine Tracker and Landscape. 2023. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 30 March 2023).
- Zhang, Y.; Zeng, G.; Pan, H.; Li, C.; Hu, Y.; Chu, K.; Han, W.; Chen, Z.; Tang, R.; Yin, W.; et al. Safety, Tolerability, and Immunogenicity of an Inactivated SARS-CoV-2 Vaccine in Healthy Adults Aged 18–59 Years: A Randomised, Double-Blind, Placebo-Controlled, Phase 1/2 Clinical Trial. Lancet Infect. Dis. 2021, 21, 181–192. [Google Scholar] [CrossRef]
- Xia, S.; Zhang, Y.; Wang, Y.; Wang, H.; Yang, Y.; Gao, G.F.; Tan, W.; Wu, G.; Xu, M.; Lou, Z.; et al. Safety and Immunogenicity of an Inactivated SARS-CoV-2 Vaccine, BBIBP-CorV: A Randomised, Double-Blind, Placebo-Controlled, Phase 1/2 Trial. Lancet Infect. Dis. 2021, 21, 39–51. [Google Scholar] [CrossRef]
- Gao, G.F.; Liu, W.J. Let’s Get Vaccinated for Both Flu and COVID-19: On the World Flu Day 2021. China CDC Wkly. 2021, 3, 915–917. [Google Scholar] [CrossRef]
- Kernéis, S.; Launay, O.; Turbelin, C.; Batteux, F.; Hanslik, T.; Boëlle, P.Y. Long-Term Immune Responses to Vaccination in Hiv-Infected Patients: A Systematic Review and Meta-Analysis. Clin. Infect. Dis. 2014, 58, 1130–1139. [Google Scholar] [CrossRef]
- Ogbe, A.; Pace, M.; Bittaye, M.; Tipoe, T.; Adele, S.; Alagaratnam, J.; Aley, P.K.; Ansari, M.A.; Bara, A.; Broadhead, S.; et al. Durability of ChAdOx1 nCoV-19 Vaccination in People Living with HIV. JCI Insight 2022, 7, e157031. [Google Scholar] [CrossRef] [PubMed]
- Zeng, G.; Wu, Q.; Pan, H.; Li, M.; Yang, J.; Wang, L.; Wu, Z.; Jiang, D.; Deng, X.; Chu, K.; et al. Immunogenicity and Safety of a Third Dose of CoronaVac, and Immune Persistence of a Two-Dose Schedule, in Healthy Adults: Interim Results from Two Single-Centre, Double-Blind, Randomised, Placebo-Controlled Phase 2 Clinical Trials. Lancet Infect. Dis. 2022, 22, 483–495. [Google Scholar] [CrossRef] [PubMed]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological Memory to SARS-CoV-2 Assessed for up to 8 Months after Infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Lin, H.; Ye, B.; Zhao, M.; Zhan, J.; Dong, S.; Guo, Y.; Zhao, Y.; Li, M.; Liu, S.; et al. One-Year Sustained Cellular and Humoral Immunities in Coronavirus Disease 2019 (COVID-19) Convalescents. Clin. Infect. Dis. 2022, 75, e1072–e1081. [Google Scholar] [CrossRef] [PubMed]
- Goel, R.R.; Apostolidis, S.A.; Painter, M.M.; Mathew, D.; Pattekar, A.; Kuthuru, O.; Gouma, S.; Hicks, P.; Meng, W.; Rosenfeld, A.M.; et al. Distinct Antibody and Memory B Cell Responses in SARS-CoV-2 Naïve and Recovered Individuals following mRNA Vaccination. Sci. Immunol. 2021, 6, eabi6950. [Google Scholar] [CrossRef] [PubMed]
- George, V.K.; Pallikkuth, S.; Parmigiani, A.; Alcaide, M.; Fischl, M.; Arheart, K.L.; Pahwa, S. HIV Infection Worsens Age-Associated Defects in Antibody Responses to Influenza Vaccine. J. Infect. Dis. 2015, 211, 1959–1968. [Google Scholar] [CrossRef]
- Avelino-Silva, V.I.; Miyaji, K.T.; Hunt, P.W.; Huang, Y.; Simoes, M.; Lima, S.B.; Freire, M.S.; Caiaffa-Filho, H.H.; Hong, M.A.; Costa, D.A.; et al. CD4/CD8 Ratio and KT Ratio Predict Yellow Fever Vaccine Immunogenicity in HIV-Infected Patients. PLoS Negl. Trop. Dis. 2016, 10, e0005219. [Google Scholar] [CrossRef]
- Frater, J.; Ewer, K.J.; Ogbe, A.; Pace, M.; Adele, S.; Adland, E.; Alagaratnam, J.; Aley, P.K.; Ali, M.; Ansari, M.A.; et al. Safety and Immunogenicity of the ChAdOx1 nCoV-19 (AZD1222) Vaccine against SARS-CoV-2 in HIV Infection: A Single-Arm Substudy of a Phase 2/3 Clinical Trial. Lancet HIV 2021, 8, e474–e485. [Google Scholar] [CrossRef]
- Müller, L.; Andrée, M.; Moskorz, W.; Drexler, I.; Walotka, L.; Grothmann, R.; Ptok, J.; Hillebrandt, J.; Ritchie, A.; Rabl, D.; et al. Age-dependent Immune Response to the Biontech/Pfizer BNT162b2 Coronavirus Disease 2019 Vaccination. Clin. Infect. Dis. 2021, 73, 2065–2072. [Google Scholar] [CrossRef]
- Shapiro, J.R.; Sitaras, I.; Park, H.S.; Aytenfisu, T.Y.; Caputo, C.; Li, M.; Lee, J.; Johnston, T.S.; Li, H.; Wouters, C.; et al. Association of Frailty, Age, and Biological Sex With Severe Acute Respiratory Syndrome Coronavirus 2 Messenger RNA Vaccine-Induced Immunity in Older Adults. Clin. Infect. Dis. 2022, 75, S61–S71. [Google Scholar] [CrossRef]
- Soto-Nava, M.; Dávila-Conn, V.; Venancio-Rocha, J.P.; García-Esparza, P.; Tapia-Trejo, D.; Hernández-Juan, R.; Zarza-Sánchez, E.; Murakami-Ogasawara, A.; Ávila-Ríos, S. SARSCoV-2 Antibody Prevalence and Titers in Persons Living with HIV Cared for at a Large Tertiary Reference Center in Mexico City. Virol. J. 2023, 20, 300. [Google Scholar] [CrossRef] [PubMed]
- Mizrahi, B.; Shilo, S.; Rossman, H.; Kalkstein, N.; Marcus, K.; Barer, Y.; Keshet, A.; Shamir-Stein, N.; Shalev, V.; Zohar, A.E.; et al. Longitudinal Symptom Dynamics of COVID-19 Infection. Nat. Commun. 2020, 11, 6208. [Google Scholar] [CrossRef] [PubMed]
- Risk Factors for Coronavirus Disease 2019 (COVID-19) Death in a Population Cohort Study from the Western Cape Province, South Africa. Clin. Infect. Dis. 2021, 73, e2005–e2015. [CrossRef] [PubMed]
- José Luis Santiago, B.; Jesús, C.; José Ramón, B.; Julián, O.; Lazzari, E.L.D.; Leire, B.; Jesús, T.; Hugo, H.K.; Sanza-Moreno, J.; Alicia Hernández, G.; et al. A Prospective Case-Cohort Study of COVID-19 in Persons with Hiv: COVIH-19 Study. Top. Antivir. Med. 2021. Available online: https://www.croiconference.org/abstract/a-prospective-case-cohort-study-of-covid-19-in-persons-with-hiv-covih-19-study/ (accessed on 30 March 2023).
- Inciarte, A.; Gonzalez-Cordon, A.; Rojas, J.; Torres, B.; de Lazzari, E.; de la Mora, L.; Martinez-Rebollar, M.; Laguno, M.; Callau, P.; Gonzalez-Navarro, A.; et al. Clinical Characteristics, Risk Factors, and Incidence of Symptomatic Coronavirus Disease 2019 in a Large Cohort of Adults Living with HIV: A Single-Center, Prospective Observational Study. AIDS 2020, 34, 1775–1780. [Google Scholar] [CrossRef]
- Fatima, S.; Zafar, A.; Afzal, H.; Ejaz, T.; Shamim, S.; Saleemi, S.; Subhan Butt, A. COVID-19 Infection among Vaccinated and Unvaccinated: Does It Make any Difference? PLoS ONE 2022, 17, e0270485. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).