Multi-Magnet Cochlear Implant Technology and Magnetic Resonance Imaging: The Safety Issue


 ,
, 
 , , , , ,
, , , , , 
 and
and
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Johnson, B.J.; Macielak, R.J.; Watson, R.E.; Heimer, J.M.; Wiste, B.J.; Lane, J.I.; Edmonson, H.A.; Carlson, M.L. Magnetic Resonance Imaging in Patients with Cochlear Implants without Magnet Removal: A Radiology-Administered Protocol to Enhance Operational Efficiency and Improve Workflow. Otol. Neurotol. 2023, 44, 664–671. [Google Scholar]
- Erhardt, J.B.; Fuhrer, E.; Gruschke, O.G.; Leupold, J.; Wapler, M.C.; Hennig, J.; Stieglitz, T.; Korvink, J.G. Should patients with brain implants undergo MRI? J. Neural. Eng. 2018, 15, 041002. [Google Scholar] [CrossRef]
- Bestourous, D.E.; Davidson, L.; Reilly, B.K. A Review of Reported Adverse Events in MRI-Safe and MRI-Conditional Cochlear Implants. Otol. Neurotol. 2022, 43, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Technavio. Cochlear Implants Market by End-user, Product, and Geography—Forecast and Analysis 2023–2027. 2023, p. 151. Available online: https://www.technavio.com/report/cochlear-implants-market-industry-analysis. (accessed on 3 February 2024).
- Srinivasan, R.; So, C.W.; Amin, N.; Jaikaransingh, D.; D‘Arco, F.; Nash, R. A review of the safety of MRI in cochlear implant patients with retained magnets. Clin. Radiol. 2019, 74, e9–e972. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.C.; Effendi, F.F.; Kosik, R.O.; Lee, W.J.; Wang, L.J.; Juan, C.J.; Chan, W.P. Utilization of CT and MRI scanning in Taiwan, 2000–2017. Insights Imaging 2023, 14, 23. [Google Scholar] [CrossRef] [PubMed]
- Businesswire. Growth of MRI Systems Market to Be Impacted by the Software Advances in MRI Technology|Technavio. Available online: https://www.businesswire.com/news/home/20191018005143/en/Growth-of-MRI-Systems-Market-to-Be-Impacted-by-the-Software-Advances-in-MRI-Technology-Technavio (accessed on 3 February 2024).
- Dong, S.Z.; Zhu, M.; Bulas, D. Techniques for minimizing sedation in pediatric MRI. J. Magn. Reason. Imaging 2019, 50, 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Advanced Bionics. MRI Safety Information for the HiRes Ultra 3D Cochlear Implant. Available online: https://www.advancedbionics.com/us/en/portals/professional-portal/products/mri-safety.html (accessed on 3 February 2024).
- Loth, A.G.; Fischer, K.; Hey, A.K.; Weiß, R.; Leinung, M.; Burck, I.; Linke, A.; Kramer, S.; Stöver, T.; Helbig, S. Magnetic Resonance Imaging in Patients with Hearing Implants—Follow-up on Prevalence and Complications. Otol. Neurotol. 2021, 42, 1334–1341. [Google Scholar] [CrossRef] [PubMed]
- Cass, N.D.; Honce, J.M.; O’Dell, A.L.; Gubbels, S.P. First MRI With New Cochlear Implant with Rotatable Internal Magnet System and Proposal for Standardization of Reporting Magnet-Related Artifact Size. Otol. Neurotol. 2019, 40, 883–891. [Google Scholar] [CrossRef] [PubMed]
- Fussell, W.L.; Patel, N.S.; Carlson, M.L.; Neff, B.A.; Watson, R.E.; Lane, J.I.; Driscoll, C.L.W. Cochlear Implants and Magnetic Resonance Imaging: Experience with over 100 Studies Performed with Magnets in Place. Otol. Neurotol. 2021, 42, 51–58. [Google Scholar] [CrossRef]
- Canzi, P.; Luzzi, S.; Carlotto, E.; Simoncelli, A.; Brondino, N.; Marconi, S.; Magnetto, M.; Lucifero, G.A.; Avato, I.; Manfrin, M.; et al. Customized Cochlear Implant Positioning in a Patient with a Low-Grade Glioma: Towards the Best MRI Artifact Management. Otol. Neurotol. 2022, 43, e628–e634. [Google Scholar] [CrossRef]
- MED-EL. Medical procedures for MED-EL Implant Systems. Available online: https://www.medel.com/docs/default-source/isi-important-safety-information/languages/en-english/ci-cochlear-implants/aw33289_150_manual-medical-procedures-ci-abi-systems-en-english-eu.pdf (accessed on 3 February 2024).
- Cochlear. CochlearTM Nucleus® Implants Magnetic Resonance Imaging (MRI) Guidelines. Available online: https://www.cochlear.com/us/en/professionals/resources-and-training/mri-guidelines (accessed on 4 February 2024).
- Eerkens, H.J.; Smits, C.; Hofman, M.B.M. Cochlear Implant Magnet Dislocation: Simulations and Measurements of Force and Torque at 1.5T Magnetic Resonance Imaging. Ear. Hear. 2021, 42, 1276–1283. [Google Scholar] [CrossRef]
- Leinung, M.; Loth, A.; Gröger, M.; Burck, I.; Vogl, T.; Stöver, T.; Helbig, S. Cochlear implant magnet dislocation after MRI: Surgical management and outcome. Eur. Arch. Otorhinolaryngol. 2020, 277, 1297–1304. [Google Scholar] [CrossRef]
- Alberalar, N.D.; Reis, J.; Piechotta, P.L.; Beetz, N.L.; Fehrenbach, U.; Geisel, D.; Thomas, A.; Busse, H.; Denecke, T. Complications of cochlear implants with MRI scans in different body regions: Type, frequency and impact. Insights Imaging 2023, 14, 9. [Google Scholar] [CrossRef] [PubMed]
- Canzi, P.; Aprile, F.; Simoncelli, A.; Manfrin, M.; Magnetto, M.; Lafe, E.; Minervini, D.; Avato, I.; Terrani, S.; Scribante, A.; et al. MRI-induced artifact by a cochlear implant with a novel magnet system: An experimental cadaver study. Eur. Arch. Otorhinolaryngol. 2021, 278, 3753–3762. [Google Scholar] [CrossRef] [PubMed]
- Tysome, J.R.; Tam, Y.C.; Patterson, I.; Graves, M.J.; Gazibegovic, D. Assessment of a Novel 3T MRI Compatible Cochlear Implant Magnet: Torque, Forces, Demagnetization, and Imaging. Otol. Neurotol. 2019, 40, e966–e974. [Google Scholar] [CrossRef]
- Canzi, P.; Berrettini, S.; Albera, A.; Barbara, M.; Bruschini, L.; Canale, A.; Carlotto, E.; Covelli, E.; Cuda, D.; Dispenza, F.; et al. Current trends on subtotal petrosectomy with cochlear implantation in recalcitrant chronic middle ear disorders. Acta Otorhinolaryngol. Ital. 2023, 43 (Suppl. S1), S67–S75. [Google Scholar] [CrossRef]
- Grupe, G.; Wagner, J.; Hofmann, S.; Stratmann, A.; Mittmann, P.; Ernst, A.; Todt, I. Prevalence and complications of MRI scans of cochlear implant patients. HNO 2017, 65 (Suppl. S1), 35–40. [Google Scholar] [CrossRef]
- Advanced Bionics. Technical Specifications HiRes Ultra 3D Cochlear Implant. Available online: https://www.advancedbionics.com/content/dam/advancedbionics/Documents/Regional/en-gb/Professional/Ultra-3D-Tech-Specs-Brochure.pdf (accessed on 7 April 2024).
- Med-El. Synchrony 2 Cochlear Implant. Available online: https://sf.cdn.medel.com/docs/librariesprovider2/product/synchrony2/med-el_synchrony-2-factsheet.pdf?sfvrsn=51f16642_4 (accessed on 7 April 2024).
- Cochlear. Cochlear Nucleus Profile Plus Series Implant. Available online: https://www.cochlear.com/us/en/professionals/products-and-candidacy/nucleus/implant/nucleus-profile-plus (accessed on 7 April 2024).
- Todt, I.; Guerkov, R.; Gehl, H.B.; Sudhoff, H. Comparison of Cochlear Implant Magnets and Their MRI Artifact Size. BioMed Res. Int. 2020, 2020, 5086291. [Google Scholar] [CrossRef]
- Canzi, P.; Magnetto, M.; Simoncelli, A.; Manfrin, M.; Aprile, F.; Lafe, E.; Carlotto, E.; Avato, I.; Scribante, A.; Preda, L.; et al. The role of cochlear implant positioning on MR imaging quality: A preclinical in vivo study with a novel implant magnet system. Eur. Arch. Otorhinolaryngol. 2022, 279, 2889–2898. [Google Scholar] [CrossRef]
- Winchester, A.; Kay-Rivest, E.; Bruno, M.; Hagiwara, M.; Moonis, G.; Jethanamest, D. Image Quality and Artifact Reduction of a Cochlear Implant with Rotatable Magnets. Otol. Neurotol. 2023, 44, e223–e229. [Google Scholar] [CrossRef]
- Ay, N.; Gehl, H.B.; Sudhoff, H.; Todt, I. Effect of head position on cochlear implant MRI artifact. Eur. Arch. Otorhinolaryngol. 2021, 278, 2763–2767. [Google Scholar] [CrossRef] [PubMed]
- Sharon, J.D.; Northcutt, B.G.; Aygun, N.; Francis, H.W. Magnetic Resonance Imaging at 1.5 Tesla with a Cochlear Implant Magnet in Place: Image Quality and Usability. Otol. Neurotol. 2016, 37, 1284–1290. [Google Scholar] [CrossRef] [PubMed]
- Amin, N.; Pai, I.; Touska, P.; Connor, S.E.J. Utilization of SEMAC-VAT MRI for improved visualization of posterior fossa structures in patients with cochlear implants. Otol. Neurotol. 2021, 42, e451–e458. [Google Scholar] [CrossRef] [PubMed]
- Canzi, P.; Carlotto, E.; Simoncelli, A.; Lafe, E.; Scribante, A.; Minervini, D.; Nardo, M.; Malpede, S.; Chiapparini, L.; Benazzo, M. The usefulness of the O-MAR algorithm in MRI skull base assessment to manage cochlear implant-related artifacts. Acta Otorhinolaryngol. Ital. 2023, 43, 273–282. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Questions | Answers | |
|---|---|---|
| D E M | Have you ever had an MRI scan since you had been provided with an CI? If no, end of questionnaire | |
| What is your gender and date of birth? | ||
| When did you undergo cochlear implantation? | ||
| M R I | When did you undergo your first MRI scan with the CI? | |
| Which was the manufacturer of the MRI scanner? | ||
| Which was the magnetic field strength used? | ||
| Where conditions regarding maximum specific absorption rate (SAR) observed? | ||
| Which body region was examined? | ||
| What was the indication for the execution of the MRI scan? | ||
| Do you know if and what precautions have been taken regarding MRI? | ||
| C O M P L I C | Has the examination been discontinued? If yes why? | |
| Did you have any pain during the examination? If yes, how strong this was? where was it located? | ||
| Did you experiment any other symptoms during the MRI? | ||
| Did your hearing get worse after the MRI? | ||
| Did your need a refit of the speech processor after the MRI? | ||
| Did you need an external stronger magnet after the MRI? | ||
| Did the internal magnet change its position during the MRI? | ||
| Have other complications occurred? | ||
| Have any special measures been taken after MRI? (Please specify) |
| Authors, Year | Subjects | Scans | Scanner Model | Tesla | SAR | Examined Region | Preventive Measures | Complications |
|---|---|---|---|---|---|---|---|---|
| Cass et al., 2019 [11] | 1 | 1 | Philips | 1.5 | NA | Brain | NA | None |
| Fussel et al., 2020 [12] | 1 | 1 | NA | 1.5 | Max 3.2 | NA | None | None |
| Johnson et al., 2023 [1] | 22 | 22 | NA | 1.5, 3 | Max 1 | NA | None | None |
| Canzi et al., 2022 [13] | 1 | 1 | Philips | 1.5 | 2.6 | Brain | None | None |
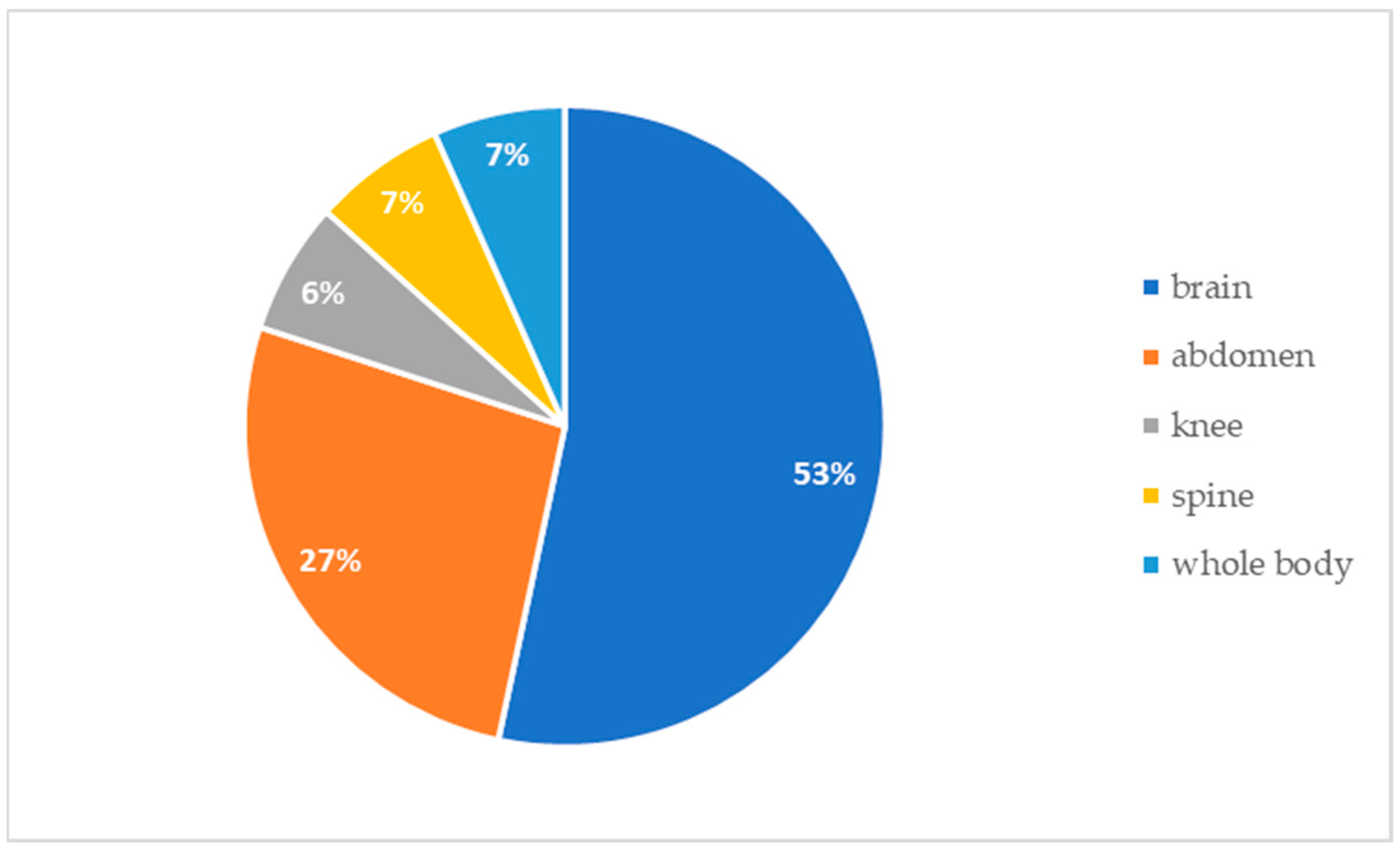
| Our experience | 47 | 65 | Philips, General Electric | 1.5 | Max 3.2 head Max 2.6 body | 1 Whole body 1 Spine 1 Knee 4 Abdomen 58 Brain | 55 None 8 Wrap (6 with LA) 2 Sedation | 62 None 3 Pain (1 exam interruption) |
| 3 | Max 2.6 head Max 2.0 body |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Canzi, P.; Carlotto, E.; Zanoletti, E.; Frijns, J.H.M.; Borsetto, D.; Caruso, A.; Chiapparini, L.; Ciorba, A.; Conte, G.; Creber, N.; et al. Multi-Magnet Cochlear Implant Technology and Magnetic Resonance Imaging: The Safety Issue. Audiol. Res. 2024, 14, 401-411. https://doi.org/10.3390/audiolres14030034
Canzi P, Carlotto E, Zanoletti E, Frijns JHM, Borsetto D, Caruso A, Chiapparini L, Ciorba A, Conte G, Creber N, et al. Multi-Magnet Cochlear Implant Technology and Magnetic Resonance Imaging: The Safety Issue. Audiology Research. 2024; 14(3):401-411. https://doi.org/10.3390/audiolres14030034
Chicago/Turabian StyleCanzi, Pietro, Elena Carlotto, Elisabetta Zanoletti, Johan H. M. Frijns, Daniele Borsetto, Antonio Caruso, Luisa Chiapparini, Andrea Ciorba, Giorgio Conte, Nathan Creber, and et al. 2024. "Multi-Magnet Cochlear Implant Technology and Magnetic Resonance Imaging: The Safety Issue" Audiology Research 14, no. 3: 401-411. https://doi.org/10.3390/audiolres14030034
APA StyleCanzi, P., Carlotto, E., Zanoletti, E., Frijns, J. H. M., Borsetto, D., Caruso, A., Chiapparini, L., Ciorba, A., Conte, G., Creber, N., Criscuolo, S., Di Lella, F., Franchella, S., Hensen, E. F., Lauda, L., Malpede, S., Mandalà, M., Rotteveel, L. J. C., Simoncelli, A., ... Benazzo, M. (2024). Multi-Magnet Cochlear Implant Technology and Magnetic Resonance Imaging: The Safety Issue. Audiology Research, 14(3), 401-411. https://doi.org/10.3390/audiolres14030034