
Accuracy of Three Types of Apex Locators versus Digital Periapical Radiography for Working Length Determination in Maxillary Premolars: An In Vitro Study

 , ,
, ,  and
and
Abstract
1. Introduction
2. Methods
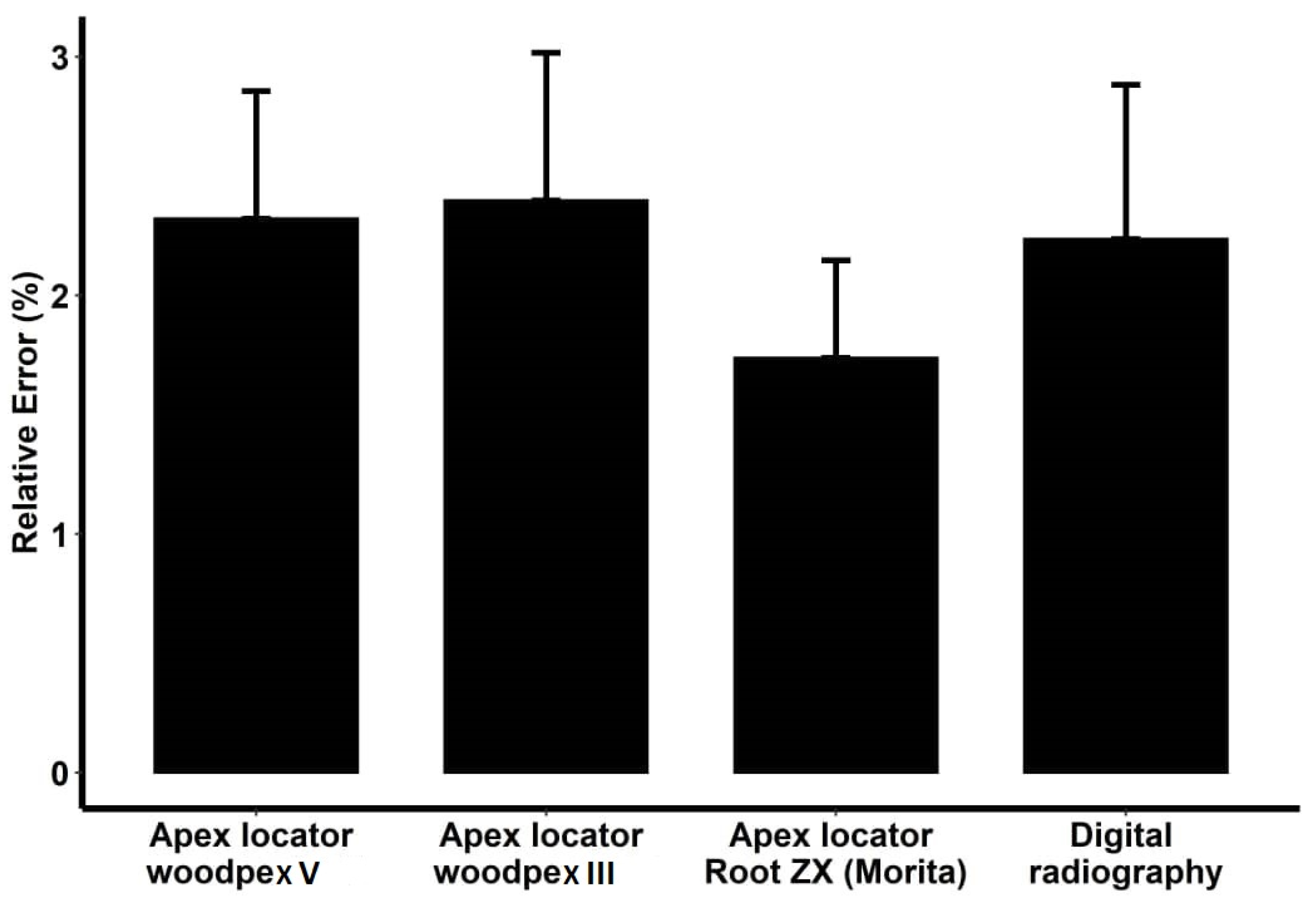
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yadav, R.K.; Bhoot, H.; Chandra, A.; Verma, P.; Bharti, R.; Shakya, V.K. A Comparative Evaluation of Four Different Techniques for Determining the Accuracy of Root Canal Working Length: An In Vitro Study. Dent. Hypotheses 2020, 11, 33–39. [Google Scholar] [CrossRef]
- De Santis, R.; Iaculli, F.; Lodato, V.; Gallicchio, V.; Simeone, M.; Spagnuolo, G.; Rengo, C. The Efficacy of Selected Sodium Hypochlorite Heating Methods for Increasing and Maintaining Its Intracanal Temperature—An Ex Vivo Study. Appl. Sci. 2022, 12, 891. [Google Scholar] [CrossRef]
- Nocca, G.; Ahmed, H.M.A.; Martorana, G.E.; Callà, C.; Gambarini, G.; Rengo, S.; Spagnuolo, G. Chromographic Analysis and Cytotoxic Effects of Chlorhexidine and Sodium Hypochlorite Reaction Mixtures. J. Endod. 2017, 43, 1545–1552. [Google Scholar] [CrossRef]
- Sameye, M.R.; Bahalkeh, A.M.; Izadi, A.; Jafaryan, A. Comparison of Digital Radiography, Conventional Film and Self-Developing Film for Working Length Determination. Iran. Endod. J. 2018, 13, 381–384. [Google Scholar] [CrossRef]
- Faraj, B.M. Preoperative Estimation of Endodontic Working Length with Cone-Beam Computed Tomography and Standardized Paralleling Technique in comparison to Its Real Length. BioMed Res. Int. 2020, 2020, 7890127. [Google Scholar] [CrossRef]
- Rotstein, I.; Ingle, J.I. (Eds.) Ingle’s Endodontics; PMPH USA: New Haven, CT, USA, 2019; p. 551. [Google Scholar]
- Manhas, S.; Lakra, S.; Mehak; Sharma, A.; Garg, K.; Arora, G. Apex Locator—Booster to Dentist: Literature Review. J. Curr. Med Res. Opin. 2020, 3, 508–515. [Google Scholar] [CrossRef]
- Nasiri, K.; Wrbas, K.-T. Accuracy of different generations of apex locators in determining working length; a systematic review and meta-analysis. Saudi Dent. J. 2022, 34, 11–20. [Google Scholar] [CrossRef]
- Eid, B.M.; Wally, A.S. Accuracy of two apex locators in calculating working length in molar primary teeth: An ex vivo study. Egypt. Dent. J. 2018, 64, 1507–1512. [Google Scholar] [CrossRef]
- Bolbolian, M.; Golchin, S.; Faegh, S. In vitro Evaluation of the Accuracy of the Root Zx in the Presence of Naocl 2.5% and Chlorhexidine 0.2%. J. Clin. Exp. Dent. 2018, 10, e1054–e1057. [Google Scholar] [CrossRef]
- Kayabasi, M.; Oznurhan, F. Evaluation of the accuracy of electronic apex locators, cone-beam computed tomography, and radiovisiography in primary teeth: An in vitro study. Microsc. Res. Tech. 2020, 83, 1330–1335. [Google Scholar] [CrossRef]
- Nam, J.-M.; Blackwelder, W.C. Analysis of the ratio of marginal probabilities in a matched-pair setting. Stat. Med. 2002, 21, 689–699. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.W. A comparison of canal preparations in straight and curved root canals. Oral Surgery, Oral Med. Oral Pathol. 1971, 32, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Fikri, N.; Azlan, A.; Kamaruzaman, M.; Mahmood, N. Application of Micro-computed Tomography to Compare the Accuracy of Two Clinical Methods in Length Determination. J. Int. Dent. Med. Res. 2019, 12, 422–428. [Google Scholar]
- Nahidi, Z.; Izadi, A.; Naeimi, S.; Rezai, R. Evaluation of the Accuracy of Three Different Electronic Apex Locators by Histologic Sectioning as the Gold Standard. J. Isfahan Dent. Sch. 2019, 15, 218–225. [Google Scholar]
- Suprastiwi, E.; Meidyawati, R. Comparison of Two Electronic Root Canal Length Measurement Devices: The Differences between Ratio Two Impedance Frequencies and Multi Frequencies. Open J. Stomatol. 2014, 04, 263–267. [Google Scholar] [CrossRef]
- Cianconi, L.; Angotti, V.; Felici, R.; Conte, G.; Mancini, M. Accuracy of Three Electronic Apex Locators Compared with Digital Radiography: An Ex Vivo Study. J. Endod. 2010, 36, 2003–2007. [Google Scholar] [CrossRef]
- Guise, G.M.; Goodell, G.G.; Imamura, G.M. In Vitro Comparison of Three Electronic Apex Locators. J. Endod. 2010, 36, 279–281. [Google Scholar] [CrossRef]
- Shabahang, S.; Goon, W.W.; Gluskin, A.H. An in vivo evaluation of root ZX electronic apex locator. J. Endod. 1996, 22, 616–618. [Google Scholar] [CrossRef]
- Peker, B.U.; Hepsenoglu, Y.E.; Ersahan, S.; Eyuboglu, T.F. Accuracy of working length measurement by Raypex 6: Electronic apex locator versus actual measurements under stereomicroscope. Balk. J. Dent. Med. 2022, 26, 15–21. [Google Scholar] [CrossRef]
- Herrera, M.; Ábalos, C.; Lucena, C.; Jiménez-Planas, A.; Llamas, R. Critical Diameter of Apical Foramen and of File Size Using the Root ZX Apex Locator: An In Vitro Study. J. Endod. 2011, 37, 1306–1309. [Google Scholar] [CrossRef]
- Mahmoud, O.; Abdelmagied, M.H.A.; Dandashi, A.H.; Jasim, B.N.; Kayali, H.A.T.; Al Shehadat, S. Comparative Evaluation of Accuracy of Different Apex Locators: Propex IQ, Raypex 6, Root ZX, and Apex ID with CBCT and Periapical Radiograph—In Vitro Study. Int. J. Dent. 2021, 2021, 5563426. [Google Scholar] [CrossRef] [PubMed]
- Elshinawy, M.I. In-vitro comparison of four different working length determination techniques. Tanta Dent. J. 2017, 14, 12–16. [Google Scholar] [CrossRef]
- Kamaraj, P.S.; Parandhaman, H.; Raguganesh, V. Comparison of Five different methods of Working length determination: An ex vivo study. Endodontology 2020, 32, 187–192. [Google Scholar] [CrossRef]
- Yılmaz, F.; Kamburoğlu, K.; Şenel, B. Endodontic Working Length Measurement Using Cone-beam Computed Tomographic Images Obtained at Different Voxel Sizes and Field of Views, Periapical Radiography, and Apex Locator: A Comparative Ex Vivo Study. J. Endod. 2017, 43, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Van Pham, K.; Khuc, N.K. The Accuracy of Endodontic Length Measurement Using Cone-beam Computed Tomography in Comparison with Electronic Apex Locators. Iran. Endod. J. 2020, 15, 12–17. [Google Scholar] [CrossRef]
- Ebrahim, A.K.; Wadachi, R.; Suda, H. In vitro evaluation of the accuracy of five different electronic apex locators for determining the working length of endodontically retreated teeth. Aust. Endod. J. 2007, 33, 7–12. [Google Scholar] [CrossRef]
- ElAyouti, A.; Kimionis, I.; Chu, A.-L.; Lost, C. Determining the apical terminus of root-end resected teeth using three modern apex locators: A comparative ex vivo study. Int. Endod. J. 2005, 38, 827–833. [Google Scholar] [CrossRef]
- Alothmani, O.S. The accuracy of Root ZX electronic apex locator. Saudi Endod. J. 2012, 2, 115–130. [Google Scholar] [CrossRef]
- ElAyouti, A.; Weiger, R.; Löst, C. The Ability of Root ZX Apex Locator to Reduce the Frequency of Overestimated Radiographic Working length. J. Endod. 2002, 28, 116–119. [Google Scholar] [CrossRef]
- Pagavino, G.; Pace, R.; Baccetti, T. A SEM study of in vivo accuracy of the Root ZX electronic apex locator. J. Endod. 1998, 24, 438–441. [Google Scholar] [CrossRef]
- Piasecki, L.; Carneiro, E.; Neto, U.X.D.S.; Westphalen, V.P.D.; Brandão, C.G.; Gambarini, G.; Azim, A.A. The Use of Micro–Computed Tomography to Determine the Accuracy of 2 Electronic Apex Locators and Anatomic Variations Affecting Their Precision. J. Endod. 2016, 42, 1263–1267. [Google Scholar] [CrossRef] [PubMed]
- Wrbas, K.T.; Ziegler, A.A.; Altenburger, M.J.; Schirrmeister, J.F. In vivo comparison of working length determination with two electronic apex locators. Int. Endod. J. 2007, 40, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Orosco, F.A.; Da Silva, G.F.; Weckwerth, P.H.; Dds, M.T.M.L.; Garcia, A.M.R.; Duarte, M.A.H.; De Moraes, I.G. Influence of different sized files on the accuracy of two electronic apex locators. Aust. Endod. J. 2017, 44, 251–254. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
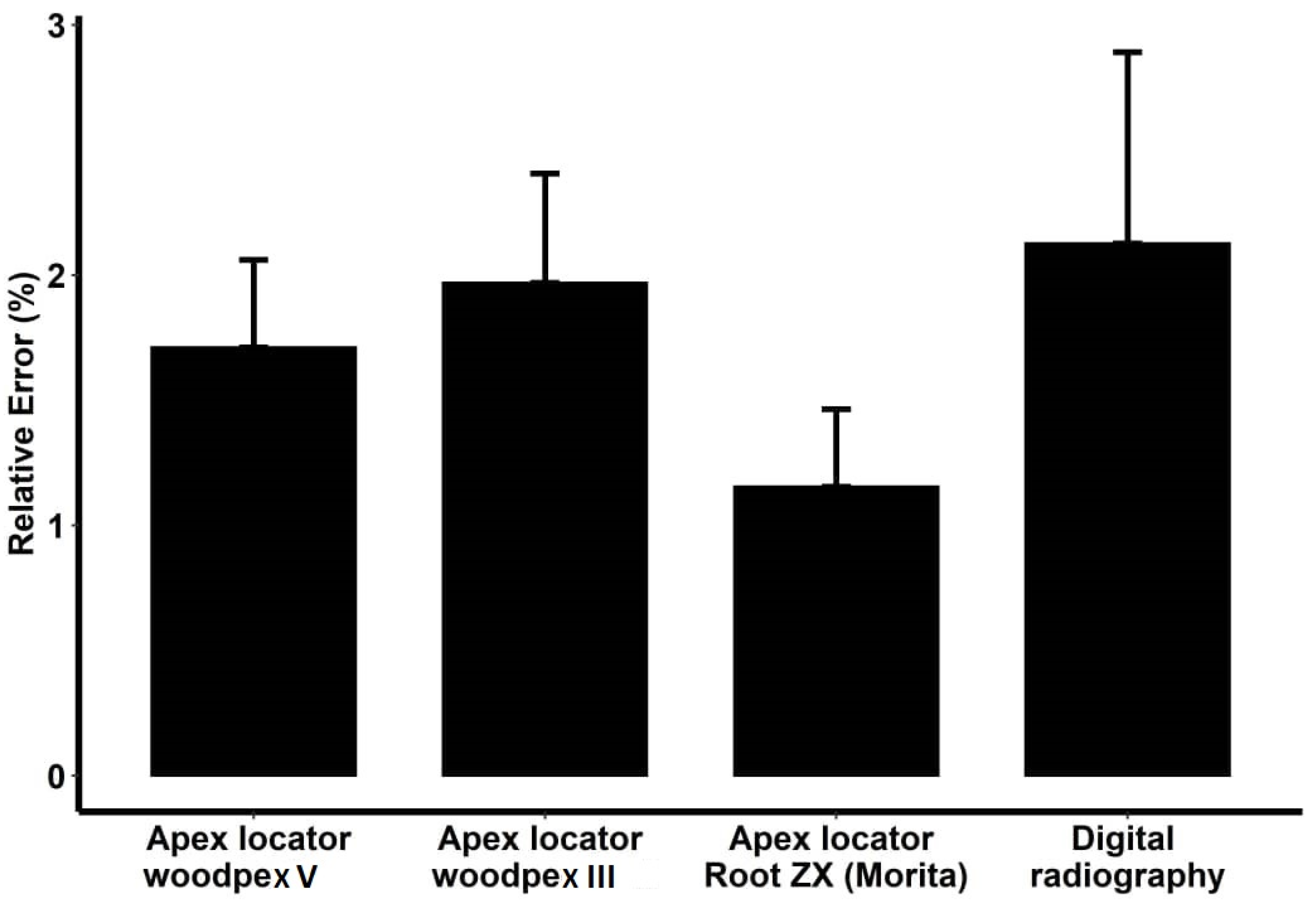
| Instrument | Difference > ±0.5 mm and ˂±1 from the Actual WL* | Difference ≥ ±1 mm from the Actual WL* | ||
|---|---|---|---|---|
| Frequency | Percentage | Frequency | Percentage | |
| Woodpex V | 6 | 10.34 | 0 | 0 |
| Woodpex III | 7 | 12.07 | 0 | 0 |
| Root ZX | 0 | 0 | 0 | 0 |
| Digital radiography | 9 | 15.52 | 2 | 3.45 |
| Comparison | Difference (Effect Size) | Standard Deviation | Degree of Freedom | T | p-Value |
|---|---|---|---|---|---|
| Woodpex V—Actual | 0.07810345 | 0.037658 | 228 | 2.074 | 0.039 |
| Woodpex III—Actual | 0.24931034 | 0.037658 | 228 | 6.6204 | <0.001 |
| Root ZX—Actual | 0.13172414 | 0.037658 | 228 | 3.4979 | 0.001 |
| Digital radiography—Actual | 0.04706897 | 0.037658 | 228 | 1.2499 | 0.213 |
| Woodpex V—Root ZX | −0.0536207 | 0.037658 | 228 | −1.424 | 0.156 |
| Woodpex III—Root ZX | 0.11758621 | 0.037658 | 228 | 3.1225 | 0.002 |
| Digital radiography—Root ZX | −0.0846551 | 0.037658 | 228 | 2.248 | 0.026 |
| Woodpex V—Digital radiography | 0.03103448 | 0.037658 | 228 | 0.8241 | 0.411 |
| Woodpex III—Digital radiography | 0.20224138 | 0.037658 | 228 | 5.3705 | <0.001 |
| Woodpex V—Woodpex III | −0.1712069 | 0.037658 | 228 | −4.546 | <0.001 |
| Position | Central (Mean and Std. Deviation) | Lateral (Mean and Std. Deviation) | p-Value | |
|---|---|---|---|---|
| Instrument | ||||
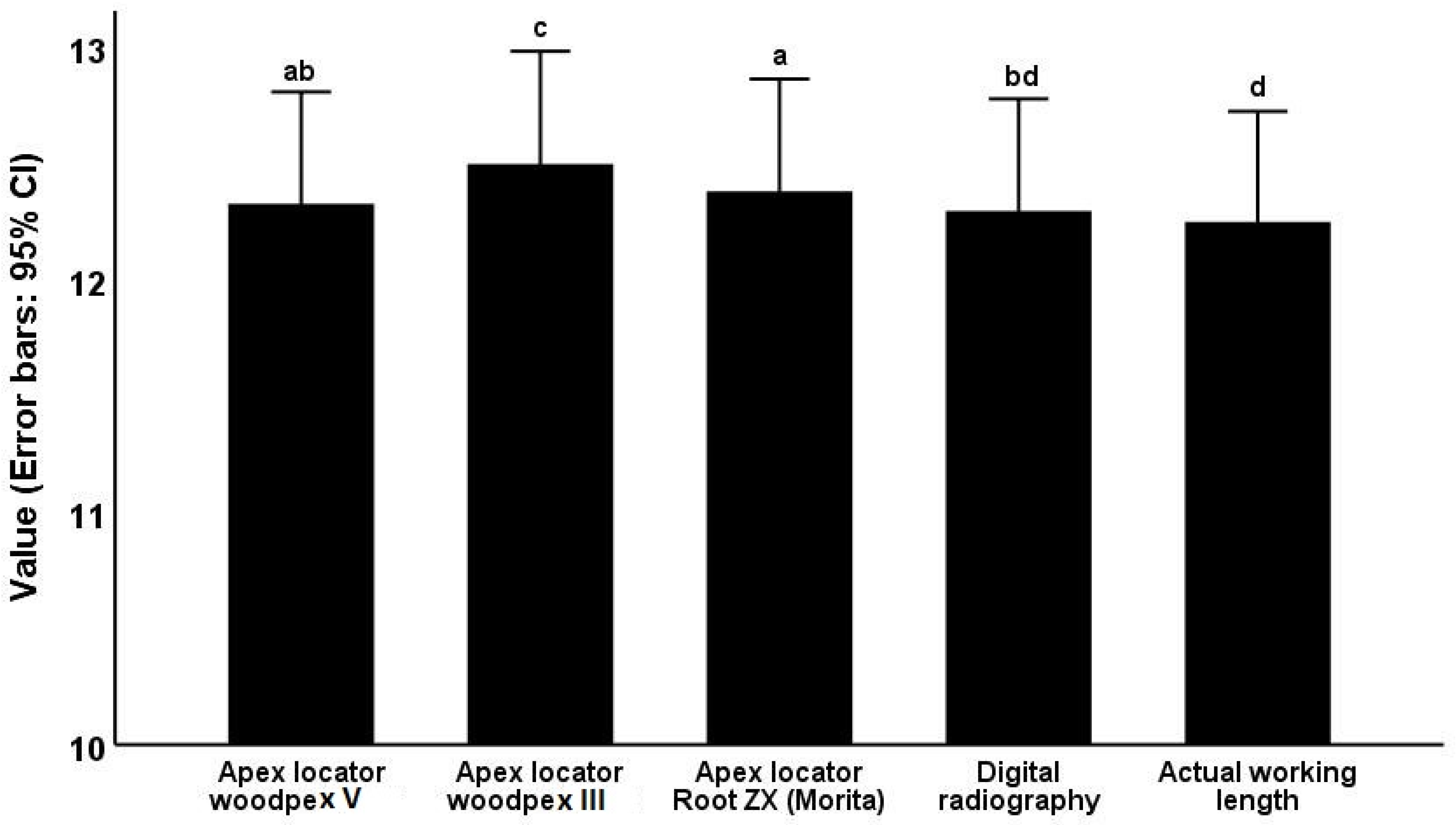
| Woodpex V | 12.211 ± 1.814 | 12.443 ± 1.875 | 0.634 | |
| Woodpex III | 12.417 ± 1.827 | 12.580 ± 1.894 | 0.740 | |
| Root ZX | 12.284 ± 1.819 | 12.478 ± 1.888 | 0.693 | |
| Digital radiography | 12.134 ± 1.791 | 12.459 ± 1.899 | 0.506 | |
| Actual | 12.179 ± 1.765 | 12.319 ± 1.883 | 0.771 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramezani, M.; Bolbolian, M.; Aliakbari, M.; Alizadeh, A.; Tofangchiha, M.; Faegh, S.M.; Patini, R.; D’Amato, G. Accuracy of Three Types of Apex Locators versus Digital Periapical Radiography for Working Length Determination in Maxillary Premolars: An In Vitro Study. Clin. Pract. 2022, 12, 1043-1053. https://doi.org/10.3390/clinpract12060107
Ramezani M, Bolbolian M, Aliakbari M, Alizadeh A, Tofangchiha M, Faegh SM, Patini R, D’Amato G. Accuracy of Three Types of Apex Locators versus Digital Periapical Radiography for Working Length Determination in Maxillary Premolars: An In Vitro Study. Clinics and Practice. 2022; 12(6):1043-1053. https://doi.org/10.3390/clinpract12060107
Chicago/Turabian StyleRamezani, Masoumeh, Marjan Bolbolian, Mohaddeseh Aliakbari, Ahad Alizadeh, Maryam Tofangchiha, Seyed Mohammad Faegh, Romeo Patini, and Giuseppe D’Amato. 2022. "Accuracy of Three Types of Apex Locators versus Digital Periapical Radiography for Working Length Determination in Maxillary Premolars: An In Vitro Study" Clinics and Practice 12, no. 6: 1043-1053. https://doi.org/10.3390/clinpract12060107
APA StyleRamezani, M., Bolbolian, M., Aliakbari, M., Alizadeh, A., Tofangchiha, M., Faegh, S. M., Patini, R., & D’Amato, G. (2022). Accuracy of Three Types of Apex Locators versus Digital Periapical Radiography for Working Length Determination in Maxillary Premolars: An In Vitro Study. Clinics and Practice, 12(6), 1043-1053. https://doi.org/10.3390/clinpract12060107