
Advantages and Limitations in the Evaluation of the Neurological and Functional Deficit in Patients with Spinal Cord Injuries

 , ,
, ,
Abstract
:1. Introduction
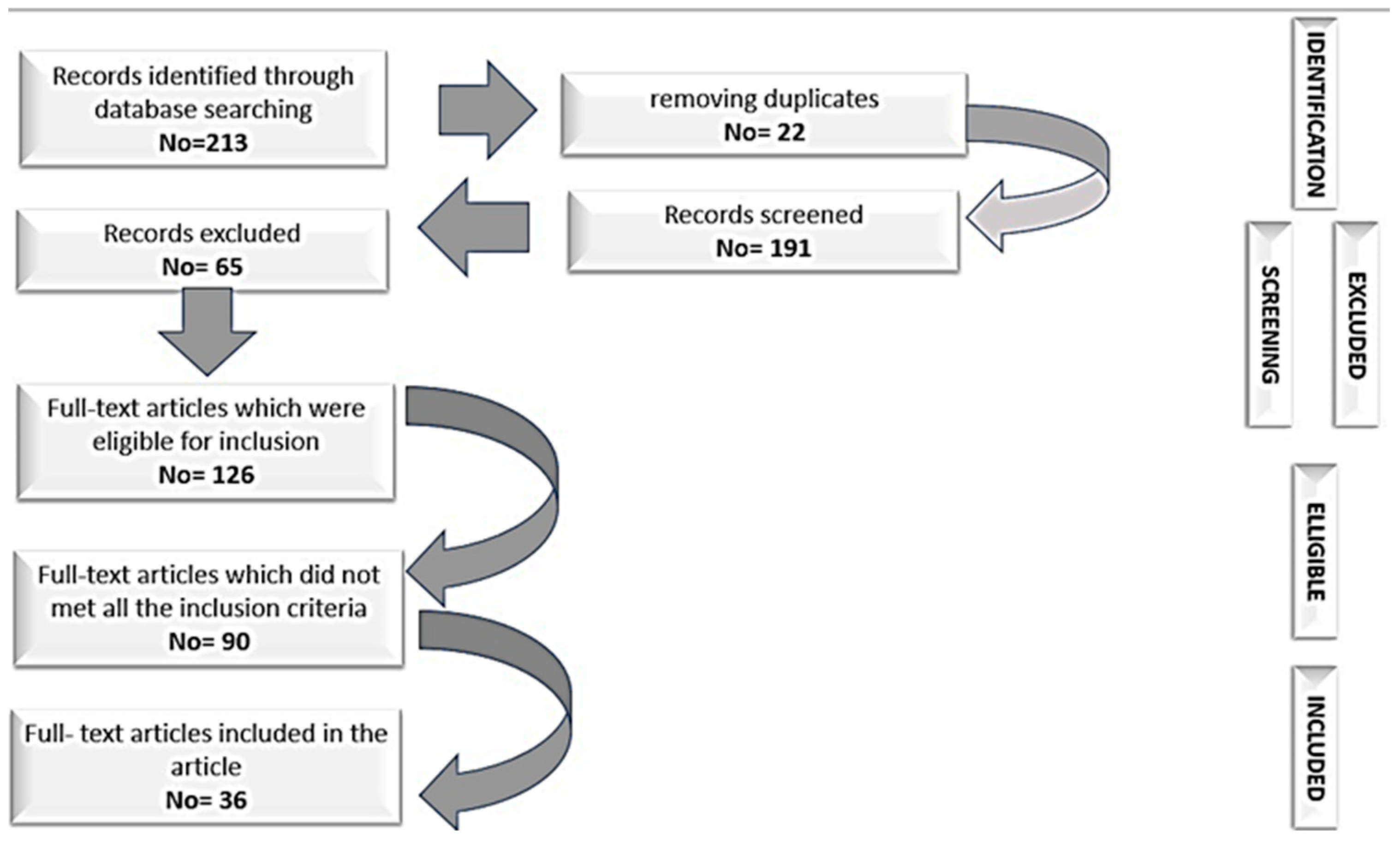
2. Materials and Methods
3. Results and Discussion
3.1. Neurological Deficit Assessment Scales
3.2. Scales for Functional Assessment of Spinal Cord Injuries
3.3. Scales That Evaluate Both the Neurological Deficit and Functional Assessment of Patients with SCI
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Ramírez-Villaescusa, J.; Hidalgo, J.L.; Ruiz-Picazo, D.; Martin-Benlloch, A.; Torres-Lozano, P.; Portero-Martinez, E. The impact of urgent intervention on the neurologic recovery in patients with thoracolumbar fractures. J. Spine Surg. 2018, 4, 388. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Schmit, B.D.; Kurpad, S.N.; Budde, M.D. Acute Magnetic Resonance Imaging Predictors of Chronic Motor Function and Tissue Sparing in Rat Cervical Spinal Cord Injury. J. Neurotrauma 2022, 39, 1727–1740. [Google Scholar] [CrossRef] [PubMed]
- Moga, T.D.; Moga, I.; Sabau, S.; Nistor-Cseppento, C.D.; Iovanovici, D.C.; Cavalu, S.; Dogaru, B.G. Sarcopenia, a major clinical problem in old age, potential causes, clinical consequences and therapeutic possibilities. Balneo PRM Res. J. 2022, 13, 492. [Google Scholar] [CrossRef]
- Zürcher, C.; Tough, H.; Fekete, C.; SwiSCI, Study Group. Mental health in individuals with spinal cord injury: The role of socioeconomic conditions and social relationships. PLoS ONE 2019, 14, e0206069. [Google Scholar] [CrossRef]
- Ahmed, N.; Quadir, M.M.; Rahman, M.A.; Alamgir, H. Community integration and life satisfaction among individuals with spinal cord injury living in the community after receiving institutional care in Bangladesh. Disabil. Rehabil. 2018, 40, 1033–1040. [Google Scholar] [CrossRef] [PubMed]
- Rico-Blázquez, M.; Quesada-Cubo, V.; Polentinos-Castro, E.; Sánchez-Ruano, R.; Rayo-Gómez, M.Á.; Del Cura-González, I.; CuidaCare Group. Health-related quality of life in caregivers of community-dwelling individuals with disabilities or chronic conditions. A gender-differentiated analysis in a cross-sectional study. BMC Nurs. 2022, 21, 69. [Google Scholar] [CrossRef] [PubMed]
- Moga, T.D.; Moga, I.; Venter, A.; Cavalu, S. Sarcopenia of Iliopsoas and Abdominal Muscles and Coexistence with Osteoporosis—Case Presentation. Pharmacophore 2021, 12, 61–66. [Google Scholar] [CrossRef]
- Holmlund, L.; Guidetti, S.; Eriksson, G.; Asaba, E. Return to work in the context of everyday life 7–11 years after spinal cord injury–a follow-up study. Disabil. Rehabil. 2018, 40, 2875–2883. [Google Scholar] [CrossRef]
- Mekeres, G.M.; Voiţă-Mekereş, F.; Tudoran, C.; Buhaş, C.L.; Tudoran, M.; Racoviţă, M.; Voiţă, N.C.; Pop, N.O.; Marian, M. Predictors for Estimating Scars’ Internalization in Victims with Post-Traumatic Scars versus Patients with Postsurgical Scars. Healthcare 2022, 10, 550. [Google Scholar] [CrossRef]
- Krause, J.S.; Terza, J.V.; Erten, M.; Focht, K.L.; Dismuke, C.E. Prediction of postinjury employment and percentage of time worked after spinal cord injury. Arch. Phys. Med. Rehabil. 2012, 93, 373–375. [Google Scholar] [CrossRef]
- McDaid, D.; Park, A.L.; Gall, A.; Purcell, M.; Bacon, M. Understanding and modelling the economic impact of spinal cord injuries in the United Kingdom. Spinal Cord 2019, 57, 778–788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badhiwala, J.H.; Ahuja, C.S.; Fehlings, M.G. Time is spine: A review of translational advances in spinal cord injury. J. Neurosurg. Spine 2018, 30, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zehravi, M.; Kabir, J.; Akter, R.; Malik, S.; Ashraf, G.M.; Tagde, P.; Ramproshad, S.; Mondal, B.; Rahman, M.H.; Mohan, A.G.; et al. A Prospective Viewpoint on Neurological Diseases and Their Biomarkers. Molecules 2022, 27, 3516. [Google Scholar] [CrossRef] [PubMed]
- McCaughey, E.J.; Purcell, M.; McLean, A.N.; Fraser, M.H.; Bewick, A.; Borotkanics, R.J.; Allan, D.B. Changing demographics of spinal cord injury over a 20-year period: A longitudinal population-based study in Scotland. Spinal Cord 2016, 54, 270–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahn, H.; Lewis, R.; Santos, A.; Cheng, C.L.; Noonan, V.K.; Dvorak, M.F.; Singh, A.; Linassi, A.G.; Christie, S.; Goytan, M.; et al. Forecasting Financial Resources for Future Traumatic Spinal Cord Injury Care Using Simulation Modeling. J. Neurotrauma 2017, 15, 2917–2923. [Google Scholar] [CrossRef] [Green Version]
- Voiță-Mekeres, F.; Buhaș, C.L.; Mekeres, G.M.; Tudoran, C.; Racovita, M.; Faur, C.I.; Tudoran, M.; Abu-Awwad, A.; Voiță, N.C.; Maghiar, T.A. Mekeres’ Psychosocial Internalization Scale: A Scale for the Evaluation of Aesthetic Prejudice in Victims of Accidents and Violence. Healthcare 2021, 9, 1440. [Google Scholar] [CrossRef]
- van Diemen, T.; Craig, A.; van Nes, I.J.W.; SELF-SCI Group; Stolwijk-Swuste, J.M.; Geertzen, J.H.B.; Middleton, J.; Post, M.W.M. Enhancing our conceptual understanding of state and trait self-efficacy by correlational analysis of four self-efficacy scales in people with spinal cord injury. BMC Psychol. 2020, 18, 108. [Google Scholar] [CrossRef]
- Oşvar, F.N.; Raţiu, A.C.; Voiţă-Mekereş, F.; Voiţă, G.F.; Bonţea, M.G.; Racoviţă, M.; Mekereş, G.M.; Bodog, F.D. Cardiac axis evaluation as a screening method for detecting cardiac abnormalities in the first trimester of pregnancy. Rom. J. Morphol. Embryol. 2020, 61, 137–142. [Google Scholar] [CrossRef]
- Schuld, C.; Franz, S.; Brüggemann, K.; Heutehaus, L.; Weidner, N.; Kirshblum, S.C.; Rupp, R.; EMSCI study group. International standards for neurological classification of spinal cord injury: Impact of the revised worksheet (revision 02/13) on classification performance. J. Spinal Cord Med. 2016, 39, 504–512. [Google Scholar] [CrossRef] [Green Version]
- Szabó, R.; Voiță-Mekereș, F.; Tudoran, C.; Abu-Awwad, A.; Tudoran, M.; Mihancea, P.; Ilea, C.D.N. Evaluation of Sleep Disturbances in Patients with Nocturnal Epileptic Seizures in a Romanian Cross-Sectional Study. Healthcare 2022, 10, 588. [Google Scholar] [CrossRef]
- Bremer, E.; Liska, T.M.; Arbour-Nicitopoulos, K.P.; Best, K.L.; Sweet, S.N. Examining long-term motivational and behavioral outcomes of two physical activity interventions. J. Spinal Cord Med. 2022, 7, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Frankel, H.L.; Hancock, D.O.; Hyslop, G.; Melzak, J.; Michaelis, L.S.; Ungar, G.H.; Vernon, J.D.; Walsh, J.J. The value of postural reduction in the initial management of closed injuries of the spine with paraplegia and tetraplegia. I. Paraplegia 1969, 7, 179–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirshblum, S.; Botticello, A.; Benedetto, J.; Donovan, J.; Marino, R.; Hsieh, S.; Wagaman, N. A Comparison of Diagnostic Stability of the ASIA Impairment Scale Versus Frankel Classification Systems for Traumatic Spinal Cord Injury. Arch. Phys. Med. Rehabil. 2020, 101, 1556–1562. [Google Scholar] [CrossRef] [PubMed]
- Furlan, J.C.; Fehlings, M.G.; Tator, C.H.; Davis, A.M. Motor and sensory assessment of patients in clinical trials for pharmacological therapy of acute spinal cord injury: Psychometric properties of the ASIA Standards. J. Neurotrauma 2008, 25, 1273–1301. [Google Scholar] [CrossRef] [PubMed]
- van Middendorp, J.J.; Goss, B.; Urquhart, S.; Atresh, S.; Williams, R.P.; Schuetz, M. Diagnosis and prognosis of traumatic spinal cord injury. Glob. Spine J. 2011, 1, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Bracken, M.B.; Webb, S.B., Jr.; Wagner, F.C. Classification of the severity of acute spinal cord injury: Implications for management. Paraplegia 1978, 15, 319–326. [Google Scholar] [CrossRef] [Green Version]
- Burns, S.P.; Tansey, K.E. The Expedited International Standards for Neurological Classification of Spinal Cord Injury (E-ISNCSCI). Spinal Cord 2020, 58, 633–634. [Google Scholar] [CrossRef] [PubMed]
- Lucas, J.T.; Ducker, T.B. Motor classification of spinal cord injuries with mobility, morbidity and recovery indices. Am. Surg. 1979, 45, 151–158. [Google Scholar]
- Poplawski, M.M.; Alizadeh, M.; Oleson, C.V.; Fisher, J.; Marino, R.J.; Gorniak, R.J.; Leiby, B.E.; Flanders, A.E. Application of Diffusion Tensor Imaging in Forecasting Neurological Injury and Recovery after Human Cervical Spinal Cord Injury. J. Neurotrauma 2019, 36, 3051–3061. [Google Scholar] [CrossRef]
- Chehrazi, B.; Wagner, F.C., Jr.; Collins, W.F., Jr.; Freeman, D.H., Jr. A scale for evaluation of spinal cord injury. J. Neurosurg. 1981, 54, 310–315. [Google Scholar] [CrossRef] [Green Version]
- Tator, C.H. Sunnybrook cord injury scales for assessing neurological injury and neurological recovery. In Early Management of Acute Spinal Cord Injury; Tator, C.H., Ed.; Raven Press: New York, NY, USA, 1982. [Google Scholar]
- Badhiwala, J.H.; Wilson, J.R.; Kwon, B.K.; Casha, S.; Fehlings, M.G. A Review of Clinical Trials in Spinal Cord Injury Including Biomarkers. J. Neurotrauma 2018, 15, 1906–1917. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, J.A.S.; Sharif, S.; Costa, F.; Rangel, J.A.I.R.; Anania, C.D.; Zileli, M. Early Management of Spinal Cord Injury: WFNS Spine Committee Recommendations. Neurospine 2020, 17, 759–784. [Google Scholar] [CrossRef] [PubMed]
- Hadley, M.N.; Walters, B.C.; Grabb, P.A.; Oyesiku, N.M.; Przybylski, G.J.; Resnick, D.K.; Ryken, T.C. Clinical assessment after acute cervical spinal cord injury. Neurosurgery 2002, 50, S21–S29. [Google Scholar] [CrossRef] [PubMed]
- El Masry, W.S.; Tsubo, M.; Katoh, S.; El Miligui, Y.H.; Khan, A. Validation of the American Spinal Injury Association (ASIA) motor score and the National Acute Spinal Cord Injury Study (NASCIS) motor score. Spine 1996, 1, 614–619. [Google Scholar] [CrossRef]
- Yugué, I.; Okada, S.; Maeda, T.; Ueta, T.; Shiba, K. Sensitivity and specificity of the ‘knee-up test’ for estimation of the American Spinal Injury Association Impairment Scale in patients with acute motor incomplete cervical spinal cord injury. Spinal Cord 2018, 56, 347–354. [Google Scholar] [CrossRef] [Green Version]
- Roberts, T.T.; Leonard, G.R.; Cepela, D.J. Classifications in Brief: American Spinal Injury Association (ASIA) Impairment Scale. Clin. Orthop. Relat. Res. 2017, 475, 1499–1504. [Google Scholar] [CrossRef] [Green Version]
- Botsford, D.J.; Esses, S.I. A new scale for the clinical assessment of spinal cord function. Orthopedics 1992, 15, 1309–1313. [Google Scholar] [CrossRef]
- Eli, I.; Lerner, D.P.; Ghogawala, Z. Acute Traumatic Spinal Cord Injury. Neurol. Clin. 2021, 39, 471–488. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Shah, S.; Vanclay, F.; Cooper, B. Improving the sensitivity of the Barthel Index for stroke rehabilitation. J. Clin. Epidemiol. 1989, 42, 703–709. [Google Scholar] [CrossRef]
- Ohura, T.; Hase, K.; Nakajima, Y.; Nakayama, T. Validity and reliability of a performance evaluation tool based on the modified Barthel Index for stroke patients. BMC Med. Res. Methodol. 2017, 17, 131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forer, S.; Granger, C.V. Functional Independence Measure; The Buffalo General Hospital State University of New York at Buffalo: Buffalo, NY, USA, 1987. [Google Scholar]
- Khamnon, N.; Amatachaya, S.; Wattanapan, P.; Musika, N.; Jitmongkolsri, P.; Kongngoen, N.; Haisirikul, M.; Jaikarsen, K.; Thaweewannakij, T.; Namwong, W. Reliability and concurrent validity of the Spinal Cord Independence Measure III among rehabilitation professionals. Spinal Cord 2022, 60, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Kidd, D.; Stewart, G.; Baldry, J.; Johnson, J.; Rossiter, D.; Petruckevitch, A.; Thompson, A.J. The Functional Independence Measure: A comparative validity and reliability study. Disabil. Rehabil. 1995, 17, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Gresham, G.E.; Labi, M.L.; Dittmar, S.S.; Hicks, J.T.; Joyce, S.Z.; Stehlik, M.A. The Quadriplegia Index of Function (QIF): Sensitivity and reliability demonstrated in a study of thirty quadriplegic patients. Paraplegia 1986, 24, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Brizuela, G.; Sinz, S.; Aranda, R.; Martínez-Navarro, I. The effect of arm-crank exercise training on power output, spirometric and cardiac function and level of autonomy in persons with tetraplegia. Eur. J. Sport Sci. 2020, 20, 926–934. [Google Scholar] [CrossRef]
- Catz, A.; Itzkovich, M.; Agranov, E.; Ring, H.; Tamir, A. SCIM–spinal cord independence measure: A new disability scale for patients with spinal cord lesions. Spinal Cord 1997, 35, 850–856. [Google Scholar] [CrossRef]
- Harvey, L.A.; Glinsky, J.V.; Chu, J. Do any physiotherapy interventions increase spinal cord independence measure or functional independence measure scores in people with spinal cord injuries? A systematic review. Spinal Cord 2021, 59, 705–715. [Google Scholar] [CrossRef]
- Itzkovich, M.; Gelernter, I.; Biering-Sorensen, F.; Weeks, C.; Laramee, M.T.; Craven, B.C.; Tonack, M.; Hitzig, S.L.; Glaser, E.; Zeilig, G.; et al. The Spinal Cord Independence Measure (SCIM) version III: Reliability and validity in a multi-center international study. Disabil. Rehabil. 2007, 29, 1926–1933. [Google Scholar] [CrossRef]
- Burns, A.S.; Delparte, J.J.; Patrick, M.; Marino, R.J.; Ditunno, J.F. The reproducibility and convergent validity of the walking index for spinal cord injury (WISCI) in chronic spinal cord injury. Neurorehabil. Neural Repair. 2011, 25, 149–157. [Google Scholar] [CrossRef]
- Dittuno, P.L.; Ditunno, J.F., Jr. Walking index for spinal cord injury (WISCI II): Scale revision. Spinal Cord 2001, 39, 654–656, Erratum in: Spinal Cord 2009, 47, 349. [Google Scholar] [CrossRef]
- Ditunno, J.; Scivoletto, G. Clinical relevance of gait research applied to clinical trials in spinal cord injury. Brain Res. Bull. 2009, 78, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Field-Fote, E.C.; Fluet, G.G.; Schafer, S.D.; Schneider, E.M.; Smith, R.; Downey, P.A.; Ruhl, C.D. The Spinal Cord Injury Functional Ambulation Inventory (SCI-FAI). J. Rehabil. Med. 2001, 33, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Eckert, M.J.; Martin, M.J. Trauma: Spinal Cord Injury. Surg. Clin. N. Am. 2017, 97, 1031–1045. [Google Scholar] [CrossRef] [PubMed]
- Kirshblum, S.; Snider, B.; Rupp, R.; Read, M.S. International Standards Committee of ASIA and ISCoS. Updates of the International Standards for Neurologic Classification of Spinal Cord Injury: 2015 and 2019. Phys. Med. Rehabil. Clin. N. Am. 2020, 31, 319–330. [Google Scholar] [CrossRef]


{kind=link}
| Nr. | Scale | Year | When to Use | Advantage | Limitation | References |
|---|---|---|---|---|---|---|
| 1. | Scala Frankel | 1969 | - Neurological deficit: A–E - A (complete neurological damage) - E (clinically normal) | - The first publicly available neurological scale - Synthetic - Clinically easy to use | - Unclear differentiation between grade C and D - Subjective nature in judging “usefulness” of any remaining motor movements - The level of the injury is not incorporated in the classification - Limited responsiveness to subtle neurological improvements during recovery. | [22,23,24,25] |
| 2. | Bracken Scale | 1978 | - 2 subscales: 7 sensitive items and 5 motor items | - Acute hospitalization | - Clinically rarely used | [26,27] |
| 3. | Lucas and Ducker’s Neuro-trauma Motor Index | 1979 | - Evaluates 23 muscles | - Predictive value of patient’s functional independence | - Heavy calculations in the evaluation of motor function | [28,29] |
| 4. | Yale Scale | 1981 | - Tests sensory and motor function | - Numerical grading of selected functions below the level of the lesion | - The multiple calculations make it difficult to use in current practice | [29,30] |
| 5. | Sunnybrook Scale | 1982 | - 10 degrees with motor and sensory deficit | -Differentiation of sensory and motor deficits between the equivalent degrees C and D from Frankel scale | - Multiple calculations | [31,32,33] |
| 6. | American Spinal Injury Association (ASIA) | 1984 | - Derived from the Frankel scale - Designated as an assessment tool to classify baseline neurological impairment. | - Classifies neurological injuries based on a practical way to admission - Provides information regarding the improvement of the patient’s condition during the follow-up | - Does not reveal the objective anatomic origin of the causal injury - Does not decide injury severity | [34,35,36,37] |
| 7. | Botsford Scale | 1992 | - Assesses motor and sensory function, rectal tone and bladder control - The motor score is obtained by testing 15 key muscles scored between 0–5 points (maximum 75 points) - The maximum sensitive score is 10 points - Anal tonus 10 points - Bladder tonus 5 points | - Introduces anal sphincter and bladder tonus control testing into the neurological assessment, as a measure of outstanding functionality - Can be used at the patient’s bedside - It does not require special tests other than those performed in a routine clinical neurological examination - Motor function is assessed in a functional assessment system | - Few clinical studies have used this scale. | [38,39] |
| Nr. | Scale | Year | When to Use | Advantages | Limitation | References |
|---|---|---|---|---|---|---|
| 1 | Barthel Index (BI) | 1965 | - Functional evaluation of patients with stroke and TVM - Score between 0–100 points, evaluates the tone of the anal sphincter, bladder tonus - Personal hygiene - Using the toilet - Food - Transfer from bed to cart and vice-versa - Mobility - Dressing - Climbing steps - Bathing | - Evaluates daily activities and some physiological functions - Easy to use | The examination time is long | [40] |
| 2 | Modified Barthel Index (MBI) | 1989 | - Allows anyone to assess the activities of daily living | - Measures independence in ADL | Evaluates only stroke patients | [41,42] |
| 3 | Functional Independence Measure (FIM) | 1987 | - Consists of 13 motor and 5 cognitive items with a score between 18 and 126 points - Divided into main categories and subcategories: self-care (feeding, brushing, bathing, dressing, toileting) sphincter control (bladder and anal), transfer mobility (transfer from bed to chair or wheelchair, from toilet to wheelchair, using the shower), locomotion (walking/wheelchair, stairs), communication (understanding, expression), social cognition (social interaction, problem solving, memory) | - Measures global independence during specific functional tasks - Records progress results - Specifies the patient’s functional mobility and independence - More sensitive, detailed and comprehensive compared to the Barthel index, socio-economically meaningful improvements | Long examination time | [43,44,45] |
| 4 | Quadriplegia Index of Function QIF | 1980 | - Quadriplegic patients | - More sensitive and reliable than the Barthel Index | Use only in quadriplegic patients | [46,47] |
| 5 | Spinal Cord Independence Measure (SCIM) | 1997 | - Functional categories: selfcare (subscore 0–20), breathing and sphincter management (0–40) and mobility (0–40); - Final score between 0 and 100 | - Disability scale developed specifically for patients with spinal cord injuries, to make functional assessments sensitive to changes occurring in the follow-up of patients with para- or tetraplegia | Use only in SCI | [48,49,50] |
| 6 | Walking Index for Spinal Cord Injury WISCI | 2000 | - Originally described with 19 levels, it was revised and expanded in 2001 to include 21 levels, thus resulting in the WISCI II for use in clinical trials | - Measures improvement in walking after SCI | Cannot be used in clinical trials | [51] |
| 7 | Walking Index for Spinal Cord Injury II (WISCI II) | 2001 | - Improvements in walking following SCI | - Incorporates physical assistance, the use of dental aids and appliances to be able to adapt to the needs of patients with varying degrees of post SCI impairment - Self-explanatory | Does not take psycho-metric properties into account | [52,53] |
| 8 | Spinal Cord Injury Functional Ambulation Inventory (SCI-FAI) | 2001 | - 6 parameters: weight shift, step width, step rhythm, step height, foot contact and step length - Each limb is scored individually, so the same score for each limb indicates symmetry between bilateral limbs, the patient is assessed from the frontal plane, then sagittal - Divided into 3 areas: walking (6 parameters and symmetry between the lower limbs)—maximum score of 20 points, 14 points for the use of assistive devices and 5 points for the walking mobility score | - Observational assessment of walking ability in people with SCI - Can be performed directly or from video recordings | - The three scores of the SCI-FAI instrument are intended to measure different domains of functioning - Not relevant to combine them to obtain a global score | [54,55] |
| Nr. | Scale | Year | When to Use | Advantages | Limitation | References |
|---|---|---|---|---|---|---|
| 1. | American Spinal Injury Association/International Medical Society of Paraplegia Standards (ASIA/IMSOP) | 1992 | - Assesses sensory level, motor function - Incorporated in the Functional Independence Measure (FIM) | - Functional status based on their ability to perform ADL plus social interaction - Good discrimination in severity of SCI - Predictability of outcome | - Weak interobserver reliability for the grading of incomplete SCI | [56] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lascu, C.F.; Buhaș, C.L.; Mekeres, G.M.; Bulzan, M.; Boț, R.B.; Căiță, G.A.; Voiță, I.B.; Pogan, M.D. Advantages and Limitations in the Evaluation of the Neurological and Functional Deficit in Patients with Spinal Cord Injuries. Clin. Pract. 2023, 13, 14-21. https://doi.org/10.3390/clinpract13010002
Lascu CF, Buhaș CL, Mekeres GM, Bulzan M, Boț RB, Căiță GA, Voiță IB, Pogan MD. Advantages and Limitations in the Evaluation of the Neurological and Functional Deficit in Patients with Spinal Cord Injuries. Clinics and Practice. 2023; 13(1):14-21. https://doi.org/10.3390/clinpract13010002
Chicago/Turabian StyleLascu, Camelia Florentina, Camelia Liana Buhaș, Gabriel Mihai Mekeres, Mădălin Bulzan, Robert Bogdan Boț, Georgiana Albina Căiță, Ioan Bogdan Voiță, and Mihaela Dana Pogan. 2023. "Advantages and Limitations in the Evaluation of the Neurological and Functional Deficit in Patients with Spinal Cord Injuries" Clinics and Practice 13, no. 1: 14-21. https://doi.org/10.3390/clinpract13010002