

Psycho-Emotional Well-Being in Caregivers of People with Acquired Brain Injury: An Exploratory Study on the Human Immersion Model during the Omicron Wave


 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedures
2.2. Outcome Measures
2.3. Statistical Analysis
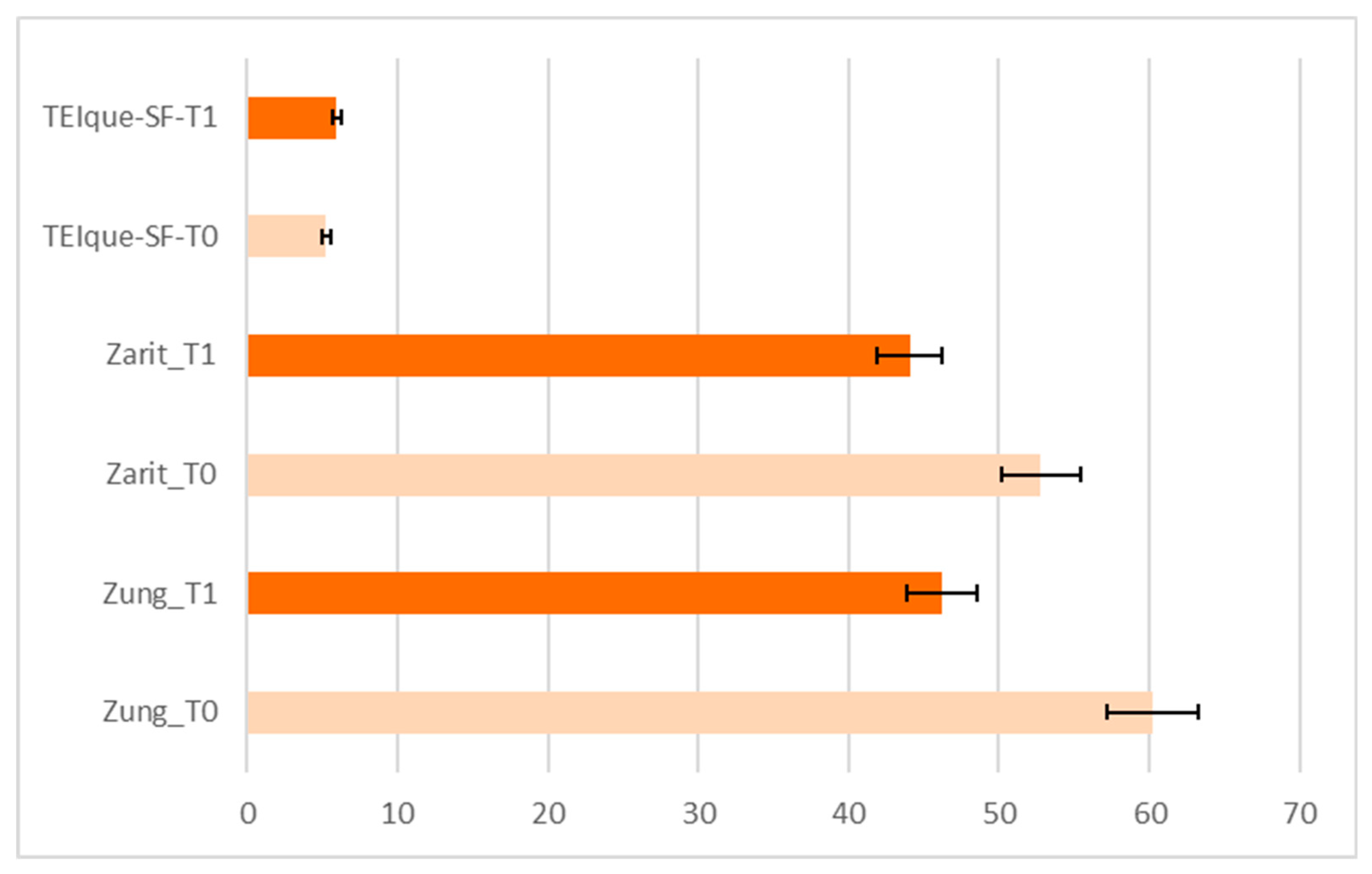
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- He, X.; Hong, W.; Pan, X.; Lu, G.; Wei, X. SARS-CoV-2 Omicron variant: Characteristics and prevention. MedComm 2021, 2, 838–845. [Google Scholar] [CrossRef] [PubMed]
- Meo, S.A.; Meo, A.S.; Al-Jassir, F.F.; Klonoff, D.C. Omicron SARS-CoV-2 new variant: Global prevalence and biological and clinical characteristics. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 8012–8018. [Google Scholar] [CrossRef] [PubMed]
- Wilkie, L.; Arroyo, P.; Conibeer, H.; Kemp, A.H.; Fisher, Z. The Impact of Psycho-Social Interventions on the Wellbeing of Individuals with Acquired Brain Injury During the COVID-19 Pandemic. Front. Psychol. 2021, 12, 648286. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Contact Tracing in the Context of COVID-19. Interim Guidance: 1 February 2021. Available online: https://www.who.int/publications/i/item/contact-tracing-in-the-context-of-covid-19 (accessed on 27 January 2022).
- Considerations for Quarantine of Contacts of COVID-19 Cases. Interim Guidance: 25 June 2021. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-IHR-Quarantine-2021.1 (accessed on 27 January 2022).
- Lefebvre, H.; Cloutier, G.; Josée Levert, M. Perspectives of survivors of traumatic brain injury and their caregivers on long-term social integration. Brain Inj. 2008, 22, 535–543. [Google Scholar] [CrossRef]
- Alzueta, E.; Perrin, P.; Baker, F.C.; Caffarra, S.; Ramos-Usuga, D.; Yuksel, D.; Arango-Lasprilla, J.C. How the COVID-19 pandemic has changed our lives: A study of psychological correlates across 59 countries. J. Clin. Psychol. 2021, 77, 556–570. [Google Scholar] [CrossRef]
- Dawson, D.L.; Golijani-Moghaddam, N. COVID-19: Psychological flexibility, coping, mental health, and wellbeing in the UK during the pandemic. J. Contextual. Behav. Sci. 2020, 17, 126–134. [Google Scholar] [CrossRef]
- Groarke, J.M.; Berry, E.; Graham-Wisener, L.; McKenna-Plumley, P.E.; McGlinchey, E.; Armour, C. Loneliness in the UK during the COVID-19 pandemic: Cross-sectional results from the COVID-19 Psychological Wellbeing Study. PLoS ONE 2020, 15, e0239698. [Google Scholar] [CrossRef]
- Piccenna, L.; Lannin, N.A.; Gruen, R.; Pattuwage, L.; Bragge, P. The experience of discharge for patients with an acquired brain injury from the inpatient to the community setting: A qualitative review. Brain Inj. 2016, 30, 241–251. [Google Scholar] [CrossRef]
- Krause, P.R.; Fleming, T.R.; Peto, R.; Longini, I.M.; Figueroa, J.P.; Sterne, J.A.C.; Cravioto, A.; Rees, H.; Higgins, J.P.T.; Boutron, I.; et al. Considerations in boosting COVID-19 vaccine immune responses. Lancet 2021, 398, 1377–1380. [Google Scholar] [CrossRef]
- Palgen, J.L.; Feraoun, Y.; Dzangué-Tchoupou, G.; Joly, C.; Martinon, F.; Le Grand, R.; Beignon, A.S. Optimize Prime/Boost Vaccine Strategies: Trained Immunity as a New Player in the Game. Front. Immunol. 2021, 12, 612747. [Google Scholar] [CrossRef]
- De Luca, R.; Rifici, C.; Pollicino, P.; Di Cara, M.; Miceli, S.; Sergi, G.; Sorrenti, L.; Romano, M.; Naro, A.; Billeri, L.; et al. ‘Online therapy’ to reduce caregiver’s distress and to stimulate post-severe acquired brain injury motor and cognitive recovery: A Sicilian hospital experience in the COVID era. J. Telemed. Telecare 2021, 2021, 1357633X21990195. [Google Scholar] [CrossRef] [PubMed]
- De Luca, R.; Rifici, C.; Pollicino, P.; Parisi, S.; Bonanno, M.; Torregrossa, W.; Ferrara, D.; Caminiti, A.; Piccione, M.; Calabrò, R.S.; et al. Is the “Family Glass Cabin” Useful to Safely Allow Inpatient-Caregiver Interaction in the COVID-19 Era? A Pilot Study on Severe Acquired Brain Injury. J. Clin. Med. 2022, 11, 1623. [Google Scholar] [CrossRef] [PubMed]
- Tyerman, A. The Impact of Lockdown on Brain Injury Survivors and Their Families. 2020. Available online: https://www.headway.org.uk/media/8564/the-impact-of-lockdown-on-brain-injury-survivors-and-their-families.pdf (accessed on 29 December 2020).
- Zung, W.W.K. A rating instrument for anxiety disorders. Psychosomatics 1971, 12, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Zarit, S.H.; Reever, K.E.; Back-Peterson, J. Relatives of the impaired elderly: Correlates of feelings of burden. Gerontologist 1980, 20, 649–655. [Google Scholar] [CrossRef] [Green Version]
- Cooper, A.; Petrides, K. A psychometric analysis of the Trait Emotional Intelligence Questionnaire–Short Form (TEIQue–SF) using item response theory. J. Pers. Assess 2010, 92, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Petrides, K.V. Psychometric properties of the Trait Emotional Intelligence Questionnaire. In Advances in the Assessment of Emotional Intelligence; Stough, C., Saklofske, D., Parker, J.D., Eds.; Springer: New York, NY, USA. [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: https://www.R-project.org/ (accessed on 2 April 2022).
- Oyesanya, T. The experience of patients with ABI and their families during the hospital stay: A systematic review of qualitative literature. Brain Inj. 2017, 31, 151–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Z.; Heffernan, C.; Tan, J. Caregiver burden: A concept analysis. Int. J. Nurs. Sci. 2020, 7, 438–445. [Google Scholar] [CrossRef]
- Qadeer, A.; Khalid, U.; Amin, M.; Murtaza, S.; Khaliq, M.F.; Shoaib, M. Caregiver’s Burden of the Patients with Traumatic Brain Injury. Cureus 2017, 9, e1590. [Google Scholar] [CrossRef] [Green Version]
- Rossi, R.; Socci, V.; Talevi, D.; Mensi, S.; Niolu, C.; Pacitti, F.; Di Marco, A.; Rossi, A.; Siracusano, A.; Di Lorenzo, G. COVID-19 Pandemic and Lockdown Measures Impact on Mental Health Among the General Population in Italy. Front. Psychiatry 2020, 11, 790. [Google Scholar] [CrossRef]
- Riley, G.A. Stress and depression in family carers following traumatic brain injury: The influence of beliefs about difficult behaviours. Clin. Rehabil. 2007, 21, 82–88. [Google Scholar] [CrossRef]
- Gan, C.; Campbell, K.A.; Gemeinhardt, M.; McFadden, G.T. Predictors of family system functioning after brain injury. Brain Inj. 2006, 20, 587–600. [Google Scholar] [CrossRef] [PubMed]
- Karpa, J.; Chernomas, W.; Roger, K.; Heinonen, T. Families’ Experiences Living with Acquired Brain Injury: “Thinking Family”-A Nursing Pathway for Family-Centered Care. Nurs. Res. Pract. 2020, 2020, 8866534. [Google Scholar] [CrossRef]
- Javed, B.; Sarwer, A.; Soto, E.B.; Mashwani, Z.U. The coronavirus (COVID-19) pandemic’s impact on mental health. Int. J. Health Plann. Manag. 2020, 35, 993–996. [Google Scholar] [CrossRef] [PubMed]
- Allé, M.C.; Berntsen, D. Self-isolation, psychotic symptoms and cognitive problems during the COVID-19 worldwide outbreak. Psychiatry Res. 2021, 302, 114015. [Google Scholar] [CrossRef] [PubMed]
- von Mohr, M.; Kirsch, L.P.; Fotopoulou, A. Social touch deprivation during COVID-19: Effects on psychological wellbeing and craving interpersonal touch. R. Soc. Open Sci. 2021, 8, 210287. [Google Scholar] [CrossRef] [PubMed]
- Keyan, D.; Dawson, K.; Azevado, S.; Yadav, S.; Tran, J.; Bryant, R.A. Brief videoconferencing psychological intervention for reducing COVID-19 related distress: Study protocol for a randomized controlled trial. BMC Public Health 2021, 21, 474. [Google Scholar] [CrossRef]
- Cohen, S.A.; Kunicki, Z.J.; Drohan, M.M.; Greaney, M.L. Exploring Changes in Caregiver Burden and Caregiving Intensity due to COVID-19. Gerontol. Geriatr. Med. 2021, 7, 2333721421999279. [Google Scholar] [CrossRef]
- Uvnäs-Moberg, K.; Handlin, L.; Petersson, M. Self-soothing behaviors with particular reference to oxytocin release induced by non-noxious sensory stimulation. Front. Psychol. 2015, 5, 1529. [Google Scholar] [CrossRef]
- McParlin, Z.; Cerritelli, F.; Friston, K.J.; Esteves, J.E. Therapeutic Alliance as Active Inference: The Role of Therapeutic Touch and Synchrony. Front. Psychol. 2022, 13, 783694. [Google Scholar] [CrossRef]
- Roy, M.; Shohamy, D.; Wager, T.D. Ventromedial prefrontal-subcortical systems and the generation of affective meaning. Trends Cogn. Sci. 2012, 16, 147–156. [Google Scholar] [CrossRef] [Green Version]
- Kikusui, T.; Winslow, J.T.; Mori, Y. Social buffering: Relief from stress and anxiety. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2006, 361, 2215–2228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, J.E.; Eng, J.J.; Miller, W.C.; Dawson, A.S. The role of caregiver involvement in upper-limb treatment in individuals with subacute stroke. Phys Ther. 2010, 90, 1302–1310. [Google Scholar] [CrossRef] [Green Version]
- Ong, P.H.; Tai, B.C.; Wong, W.P.; Wee, L.E.; Chen, C.; Cheong, A.; Fong, N.P.; Chan, K.M.; Tan, B.Y.; Menon, E.; et al. Caregivers: Do they make a difference to patient recovery in subacute stroke? Arch. Phys. Med. Rehab. 2017, 98, 2009–2020. [Google Scholar] [CrossRef] [PubMed]
- Shepherd-Banigan, M.E.; Shapiro, A.; McDuffie, J.R.; Brancu, M.; Sperber, N.R.; van Houtven, C.H.; Kosinski, A.S.; Mehta, N.N.; Nagi, A.; Williams, J.W., Jr. Interventions that support or involve caregivers or families of patients with traumatic injury: A systematic review. J. Gen. Intern. 2018, 33, 1177–1186. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| All | Males | Females | p-Value | |
|---|---|---|---|---|
| Caregivers | 15 | 5 (33.33) | 10 (66.67) | |
| Age (years) | 48.67 (9.54) | 45.40 (11.55) | 50.30 (8.58) | 0.43 |
| Education | 0.05 | |||
| Elementary school | 1 (6.67) | 1 (20.00) | 0 (0.00) | |
| Middle school | 6 (40.00) | 0 (0.00) | 6 (60.00) | |
| High school | 8 (53.33) | 4 (80.00) | 4 (40.00) | |
| University | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| Relationship with patient | 0.06 | |||
| Spouse | 6 (40.00) | 0 (0.00) | 6 (60.00) | |
| Parents | 3 (20.00) | 1 (20.00) | 2 (20.00) | |
| Son/Daughter | 3 (20.00) | 1 (20.00) | 2 (20.00) | |
| Brother/Sister | 1 (6.67) | 1 (20.00) | 0 (0.00) | |
| Other | 2 (13.33) | 2 (40.00) | 0 (0.00) |
| HIM Family Session | Caregiver Domain Intervention | Time–Session Modality Interaction | Meeting–Number |
|---|---|---|---|
| Face-to-face caregiver meeting model | Anxiety, depression, andemotional burden | 72 h full time | One weekly real “face-to-face” meeting |
| Psychoeducational | Residential human immersion modality “next” to a family member | Four monthly meetings | |
| Emotional training for specific caregiver’s needs | Eight face-to-face meetings in total |
| Organization Time 72 h | Staff Trainer | Technical Competencies | Topic-Training for Caregiver’s Needs |
|---|---|---|---|
| One-day residential caregiver’s training activities | Nurse | Nursing Educational | Cardiocirculatory parameters Vital signs detection Management of venous and/or bladder catheters Dressing sores Use of aids (lifter, chair, braces, communicator, and augmentative alternative communication) |
| Two-day residential caregiver’s training activities | Speech Therapist | Speech Educational | Breathing Communication Nutrition |
| Three-day residential caregiver’s training activities | Psychologist Psychiatric Therapist | Psycho-Educational Emotional training | Emotionality, motivation, empathy, and social skills |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Luca, R.; Pollicino, P.; Rifici, C.; Mondo, N.; Iorio, S.; Cassaniti, A.; Ferrara, D.; Caminiti, A.; Famà, F.; Bonanno, M.; et al. Psycho-Emotional Well-Being in Caregivers of People with Acquired Brain Injury: An Exploratory Study on the Human Immersion Model during the Omicron Wave. Clin. Pract. 2023, 13, 487-496. https://doi.org/10.3390/clinpract13020044
De Luca R, Pollicino P, Rifici C, Mondo N, Iorio S, Cassaniti A, Ferrara D, Caminiti A, Famà F, Bonanno M, et al. Psycho-Emotional Well-Being in Caregivers of People with Acquired Brain Injury: An Exploratory Study on the Human Immersion Model during the Omicron Wave. Clinics and Practice. 2023; 13(2):487-496. https://doi.org/10.3390/clinpract13020044
Chicago/Turabian StyleDe Luca, Rosaria, Patrizia Pollicino, Carmela Rifici, Natale Mondo, Stefania Iorio, Angela Cassaniti, Donatella Ferrara, Angelo Caminiti, Fausto Famà, Mirjam Bonanno, and et al. 2023. "Psycho-Emotional Well-Being in Caregivers of People with Acquired Brain Injury: An Exploratory Study on the Human Immersion Model during the Omicron Wave" Clinics and Practice 13, no. 2: 487-496. https://doi.org/10.3390/clinpract13020044
APA StyleDe Luca, R., Pollicino, P., Rifici, C., Mondo, N., Iorio, S., Cassaniti, A., Ferrara, D., Caminiti, A., Famà, F., Bonanno, M., & Calabrò, R. S. (2023). Psycho-Emotional Well-Being in Caregivers of People with Acquired Brain Injury: An Exploratory Study on the Human Immersion Model during the Omicron Wave. Clinics and Practice, 13(2), 487-496. https://doi.org/10.3390/clinpract13020044