
Stress, Anxiety, and Depression Levels among University Students: Three Years from the Beginning of the Pandemic

 ,
, 
 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample and Comparison Samples
2.2. Survey Tools
2.3. Statistical Analysis
3. Results
3.1. Demographic and DASS21
3.2. Multiple Correlation Analysis
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix B

{kind=link}
{kind=link}
| Stress | Anxiety | Depression | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Responses of Students | Normal | Mild to Severe | Extreme Severe | Normal | Mild to Severe | Extreme Severe | Normal | Mild to Severe | Extreme Severe | |
| Age range | 18–25 | 572 | 462 | 103 | 562 | 372 | 203 | 464 | 471 | 202 |
| ≥26 | 217 | 118 | 25 | 232 | 85 | 43 | 200 | 113 | 47 | |
| p-Values | 0.004 | <0.00001 | <0.00001 | |||||||
| Gender | Male | 324 | 143 | 31 | 310 | 136 | 52 | 253 | 184 | 61 |
| Female | 465 | 437 | 97 | 484 | 321 | 194 | 411 | 400 | 188 | |
| p-Values | <0.00001 | <0.00001 | 0.00027 | |||||||
| Marital status | Unmarried | 699 | 541 | 122 | 699 | 425 | 238 | 579 | 542 | 241 |
| Other | 90 | 39 | 6 | 95 | 32 | 8 | 85 | 42 | 8 | |
| p-Values | 0.023 | 0.00003 | <0.00001 | |||||||
| Cohabitation status | I live alone | 228 | 184 | 45 | 232 | 143 | 82 | 194 | 178 | 85 |
| With 1 person | 205 | 144 | 33 | 206 | 112 | 64 | 176 | 142 | 64 | |
| With 2 or more | 356 | 252 | 50 | 356 | 202 | 100 | 294 | 264 | 100 | |
| p-Values | 0.556 | 0.701 | 0.547 | |||||||
| Vaccinated | Yes | 634 | 501 | 113 | 652 | 382 | 214 | 541 | 489 | 218 |
| No | 155 | 79 | 15 | 142 | 75 | 32 | 123 | 95 | 31 | |
| p-Values | 0.0037 | 0.197 | 0.085 | |||||||
| Previous psychological or psychiatric treatment | Yes | 120 | 171 | 57 | 126 | 124 | 98 | 100 | 147 | 101 |
| No | 669 | 409 | 71 | 668 | 333 | 148 | 564 | 437 | 148 | |
| p-Values | <0.00001 | <0.00001 | <0.00001 | |||||||
| Current psychological or psychiatric treatment | Yes | 41 | 88 | 41 | 43 | 65 | 62 | 39 | 64 | 67 |
| No | 748 | 492 | 87 | 751 | 392 | 184 | 625 | 520 | 182 | |
| p-Values | <0.00001 | <0.00001 | <0.00001 | |||||||
| Current intake of psychoactive medication | Yes | 10 | 30 | 17 | 9 | 17 | 31 | 5 | 17 | 35 |
| No | 779 | 550 | 111 | 785 | 440 | 215 | 659 | 567 | 214 | |
| p-Values | <0.00001 | <0.00001 | <0.00001 | |||||||
References
- Platto, S.; Wang, Y.; Zhou, J.; Carafoli, E. History of the COVID-19 pandemic: Origin, explosion, worldwide spreading. Biochem. Biophys. Res. Commun. 2021, 538, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Singh, R.; Kaur, J.; Pandey, S.; Sharma, V.; Thakur, L.; Sati, S.; Mani, S.; Asthana, S.; Sharma, T.K.; et al. Wuhan to World: The COVID-19 Pandemic. Front. Cell. Infect. Microbiol. 2021, 11, 596201. [Google Scholar] [CrossRef] [PubMed]
- Chandu, V.C.; Marella, Y.; Panga, G.S.; Pachava, S.; Vadapalli, V. Measuring the Impact of COVID-19 on Mental Health: A Scoping Review of the Existing Scales. Indian J. Psychol. Med. 2020, 42, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Kavvadas, D.; Kavvada, A.; Karachrysafi, S.; Papaliagkas, V.; Cheristanidis, S.; Chatzidimitriou, M.; Papamitsou, T. Stress, Anxiety and Depression Prevalence among Greek University Students during COVID-19 Pandemic: A Two-Year Survey. J. Clin. Med. 2022, 11, 4263. [Google Scholar] [CrossRef]
- Odriozola-González, P.; Planchuelo-Gómez, Á.; Irurtia, M.J.; de Luis-García, R. Psychological effects of the COVID-19 outbreak and lockdown among students and workers of a Spanish university. Psychiatry Res. 2020, 290, 113108. [Google Scholar] [CrossRef]
- Son, C.; Hegde, S.; Smith, A.; Wang, X.; Sasangohar, F. Effects of COVID-19 on College Students’ Mental Health in the United States: Interview Survey Study. J. Med. Internet Res. 2020, 22, e21279. [Google Scholar] [CrossRef]
- Ma, Z.; Zhao, J.; Li, Y.; Chen, D.; Wang, T.; Zhang, Z.; Chen, Z.; Yu, Q.; Jiang, J.; Fan, F.; et al. Mental health problems and correlates among 746 217 college students during the coronavirus disease 2019 outbreak in China. Epidemiol. Psychiatr. Sci. 2020, 29, e181. [Google Scholar] [CrossRef]
- Chang, J.; Yuan, Y.; Wang, D. Mental health status and its influencing factors among college students during the epidemic of COVID-19. Nan Fang Yi Ke Da Xue Xue Bao 2020, 40, 171–176. [Google Scholar] [CrossRef]
- Tang, W.; Hu, T.; Hu, B.; Jin, C.; Wang, G.; Xie, C.; Chen, S.; Xu, J. Prevalence and correlates of PTSD and depressive symptoms one month after the outbreak of the COVID-19 epidemic in a sample of home-quarantined Chinese university students. J. Affect. Disord. 2020, 274, 1–7. [Google Scholar] [CrossRef]
- Browning, M.H.E.M.; Larson, L.R.; Sharaievska, I.; Rigolon, A.; McAnirlin, O.; Mullenbach, L.; Cloutier, S.; Vu, T.M.; Thomsen, J.; Reigner, N.; et al. Psychological impacts from COVID-19 among university students: Risk factors across seven states in the United States. PLoS ONE 2021, 16, e0245327. [Google Scholar] [CrossRef]
- Wathelet, M.; Duhem, S.; Vaiva, G.; Baubet, T.; Habran, E.; Veerapa, E.; Debien, C.; Molenda, S.; Horn, M.; Grandgenèvre, P.; et al. Factors Associated with Mental Health Disorders Among University Students in France Confined During the COVID-19 Pandemic. JAMA Netw. Open 2020, 3, e2025591. [Google Scholar] [CrossRef]
- Riboldi, I.; Capogrosso, C.A.; Piacenti, S.; Calabrese, A.; Paioni, S.L.; Bartoli, F.; Crocamo, C.; Carrà, G.; Armes, J.; Taylor, C. Mental Health and COVID-19 in University Students: Findings from a Qualitative, Comparative Study in Italy and the UK. Int. J. Environ. Res. Public Health 2023, 20, 4071. [Google Scholar] [CrossRef]
- Kornilaki, A. The psychological consequences of COVID-19 pandemic on University students in Greece. The role of daily activities during the quarantine. Psychol. J. Hell. Psychol. Soc. 2022, 26, 144–164. [Google Scholar] [CrossRef]
- Dazzio, R.E.; Daley, S.S.; Budesheim, T.L.; Earl, A.K.K. The interaction between Greek affiliation and religiosity on problem drinking in college students. J. Am. Coll. Health 2021, 2021, 1–8. [Google Scholar] [CrossRef]
- Kontoangelos, K.; Tsiori, S.; Koundi, K.; Pappa, X.; Sakkas, P.; Papageorgiou, C.C. Greek college students and psychopathology: New insights. Int. J. Environ. Res. Public Health 2015, 12, 4709–4725. [Google Scholar] [CrossRef]
- Economou, M.; Peppou, L.; Fousketaki, S.; Theleritis, C.; Patelakis, A.; Alexiou, T.; Madianos, M.; Stefanis, C. Economic crisis and mental health: Effects on the prevalence of common mental disorders. Psychiatriki 2013, 24, 247–261. Available online: http://www.ncbi.nlm.nih.gov/pubmed/24486974 (accessed on 13 January 2023).
- Martinez, H.S.; Klanecky, A.K.; McChargue, D.E. Problem drinking among at-risk college students: The examination of Greek involvement, freshman status, and history of mental health problems. J. Am. Coll. Health 2018, 66, 579–587. [Google Scholar] [CrossRef]
- Antonopoulou, M.; Mantzorou, M.; Serdari, A.; Bonotis, K.; Vasios, G.; Pavlidou, E.; Trifonos, C.; Vadikolias, K.; Petridis, D.; Giaginis, C. Evaluating Mediterranean diet adherence in university student populations: Does this dietary pattern affect students’ academic performance and mental health? Int. J. Health Plan. Manag. 2020, 35, 5–21. [Google Scholar] [CrossRef]
- Kaparounaki, C.K.; Koraka, C.A.; Kotsi, E.S.; Ntziovara, A.M.P.; Kyriakidis, G.C.; Fountoulakis, K.N. Greek university student’s attitudes and beliefs concerning mental illness and its treatment. Int. J. Soc. Psychiatry 2019, 65, 515–526. [Google Scholar] [CrossRef]
- Economou, M. Social Distance in COVID-19: Drawing the line between protective behavior and stigma manifestation. Psychiatriki 2021, 32, 183–186. [Google Scholar] [CrossRef]
- Wong, S.S.; Wong, C.C.; Ng, K.W.; Bostanudin, M.F.; Tan, S.F. Depression, anxiety, and stress among university students in Selangor, Malaysia during COVID-19 pandemics and their associated factors. PLoS ONE 2023, 18, e0280680. [Google Scholar] [CrossRef] [PubMed]
- Dasor, M.M.; Jafridin, A.A.; Azhar, A.A.; Asma, A.A.A.; Manivannan, P.C.; Bilal, S.; Yusof, N.; Sabri, B.A.M. Emotional Intelligence, Depression, Stress and Anxiety Amongst Undergraduate Dental Students During the COVID-19 Pandemic. Int. J. Public. Health 2023, 68, 1604383. [Google Scholar] [CrossRef] [PubMed]
- Xu, T.; Wang, H. High prevalence of anxiety, depression, and stress among remote learning students during the COVID-19 pandemic: Evidence from a meta-analysis. Front. Psychol. 2023, 13, 1103925. [Google Scholar] [CrossRef] [PubMed]
- Aslan, I.; Çınar, O. Predictors and prevalence of stress, anxiety, depression, and PTSD among university students during the second wave of the COVID-19 pandemic in Turkey. Front. Psychol. 2023, 13, 1087528. [Google Scholar] [CrossRef]
- Daniali, H.; Martinussen, M.; Flaten, M.A. A global meta-analysis of depression, anxiety, and stress before and during COVID-19. Health Psychol. 2023, 42, 124–138. [Google Scholar] [CrossRef]
- Moutinho, I.L.D.; Maddalena, N.D.C.P.; Roland, R.K.; Lucchetti, A.L.G.; Tibiriçá, S.H.C.; Ezequiel, O.D.S.; Lucchetti, G. Depression, stress and anxiety in medical students: A cross-sectional comparison between students from different semesters. Rev. Assoc. Med. Bras. 2017, 63, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Castaldelli-Maia, J.M.; Lewis, T.; dos Santos, N.M.; Picon, F.; Kadhum, M.; Farrell, S.M.; Molodynski, A.; Ventriglio, A. Stressors, psychological distress, and mental health problems amongst Brazilian medical students. Int. Rev. Psychiatry 2019, 31, 603–607. [Google Scholar] [CrossRef] [PubMed]
- Zolotareva, A.; Belousova, S.; Danilova, I.; Tseilikman, V.; Lapshin, M.; Sarapultseva, L.; Makhniova, S.; Kritsky, I.; Ibragimov, R.; Hu, D.; et al. Somatic and psychological distress among Russian university students during the COVID-19 pandemic. Int. J. Psychiatry Med. 2023, 58, 119–129. [Google Scholar] [CrossRef]
- Liverpool, S.; Moinuddin, M.; Aithal, S.; Owen, M.; Bracegirdle, K.; Caravotta, M.; Walker, R.; Murphy, C.; Karkou, V. Mental health and wellbeing of further and higher education students returning to face-to-face learning after Covid-19 restrictions. PLoS ONE 2023, 18, e0280689. [Google Scholar] [CrossRef]
- Eibensteiner, F.; Ritschl, V.; A Nawaz, F.; Fazel, S.S.; Tsagkaris, C.; Kulnik, S.T.; Crutzen, R.; Klager, E.; Völkl-Kernstock, S.; Schaden, E.; et al. People’s willingness to vaccinate against covid-19 despite their safety concerns: Twitter poll analysis. J. Med. Internet Res. 2021, 23, e28973. [Google Scholar] [CrossRef]
- Snehota, M.; Vlckova, J.; Cizkova, K.; Vachutka, J.; Kolarova, H.; Klaskova, E. Acceptance of a vaccine against COVID-19—A systematic review of surveys conducted worldwide. Bratisl. Med. J. 2021, 122, 538–547. [Google Scholar] [CrossRef]
- Snehota, M.; Vlckova, J.; Cizkova, K.; Vachutka, J.; Kolarova, H.; Klaskova, E. Psychological Distress in Primary Healthcare Workers during the COVID-19 Pandemic in Greece. Acta Med. Acad. 2021, 50, 252–263. [Google Scholar] [CrossRef] [PubMed]
- Cascini, F.; Pantovic, A.; Al-Ajlouni, Y.; Failla, G.; Ricciardi, W. Attitudes, acceptance and hesitancy among the general population worldwide to receive the covid-19 vaccines and their contributing factors: A systematic review. EClinicalMedicine 2021, 40, 101113. [Google Scholar] [CrossRef]
- Hou, Z.; Tong, Y.; Du, F.; Lu, L.; Zhao, S.; Yu, K.; Piatek, S.J.; Larson, H.J.; Lin, L. Assessing covid-19 vaccine hesitancy, confidence, and public engagement: A global social listening study. J. Med. Internet Res. 2021, 23, e27632. [Google Scholar] [CrossRef]
- Bendau, A.; Plag, J.; Petzold, M.B.; Ströhle, A. Covid-19 vaccine hesitancy and related fears and anxiety. Int. Immunopharmacol. 2021, 97, 107724. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Wyka, K.; Rauh, L.; Rabin, K.; Ratzan, S.; Gostin, L.O.; Larson, H.J.; El-Mohandes, A. Hesitant or not? the association of age, gender, and education with potential acceptance of a covid-19 vaccine: A country-level analysis. J. Health Commun. 2020, 25, 799–807. [Google Scholar] [CrossRef]
- Grochowska, M.; Ratajczak, A.; Zdunek, G.; Adamiec, A.; Waszkiewicz, P.; Feleszko, W. A Comparison of the level of acceptance and hesitancy towards the influenza vaccine and the forthcoming COVID-19 vaccine in the medical community. Vaccines 2021, 9, 475. [Google Scholar] [CrossRef]
- Zuberi, A.; Waqas, A.; Naveed, S.; Hossain, M.M.; Rahman, A.; Saeed, K.; Fuhr, D.C. Prevalence of Mental Disorders in the WHO Eastern Mediterranean Region: A Systematic Review and Meta-Analysis. Front. Psychiatry 2021, 12, 665019. [Google Scholar] [CrossRef]
- Karaivazoglou, K.; Konstantopoulou, G.; Kalogeropoulou, M.; Iliou, T.; Vorvolakos, T.; Assimakopoulos, K.; Gourzis, P.; Alexopoulos, P. Psychological distress in the Greek general population during the first COVID-19 lockdown. BJPsych Open 2021, 7, e59. [Google Scholar] [CrossRef]
- Rahman, A. Mental disorders in the Eastern Mediterranean Region. Int. J. Public Health 2017, 63 (Suppl. S1), 9–10. [Google Scholar] [CrossRef]
- Eskin, M. Suicidal Behavior in the Mediterranean Countries. Clin. Pract. Epidemiol. Ment. Health 2020, 16, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Dong, D.; Chen, Z.; Zong, M.; Zhang, P.; Gu, W.; Feng, Y.; Qiao, Z. What protects us against the COVID-19 threat? Cultural tightness matters. BMC Public Health 2021, 22, 2139. [Google Scholar] [CrossRef] [PubMed]
- Riboldi, I.; Cavaleri, D.; Calabrese, A.; Capogrosso, C.A.; Piacenti, S.; Bartoli, F.; Crocamo, C.; Carrà, G. Digital mental health interventions for anxiety and depressive symptoms in university students during the COVID-19 pandemic: A systematic review of randomized controlled trials. Rev. Psiquiatr. Salud Ment. 2022. [Google Scholar] [CrossRef] [PubMed]
- Hatta, M.H.; Sidi, H.; Koon, C.S.; Roos, N.A.C.; Sharip, S.; Samad, F.D.A.; Xi, O.W.; Das, S.; Saini, S.M. Virtual Reality (VR) Technology for Treatment of Mental Health Problems during COVID-19: A Systematic Review. Int. J. Environ. Res. Public. Health 2022, 19, 5389. [Google Scholar] [CrossRef] [PubMed]
- Hatta, M.H.; Sidi, H.; Sharip, S.; Das, S.; Saini, S.M. The Role of Virtual Reality as a Psychological Intervention for Mental Health Disturbances during the COVID-19 Pandemic: A Narrative Review. Int. J. Environ. Res. Public Health 2022, 19, 2390. [Google Scholar] [CrossRef]
- Das, N. Psychiatrist in post-COVID-19 era: Are we prepared? Asian J. Psychiatr. 2020, 51, 102082. [Google Scholar] [CrossRef]
- Liu, S.; Yang, L.; Zhang, C.; Xiang, Y.-T.; Liu, Z.; Hu, S.; Zhang, B. Online mental health services in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, e17–e18. [Google Scholar] [CrossRef]
- D’Agostino, A.; Demartini, B.; Cavallotti, S.; Gambini, O. Mental health services in Italy during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, 385–387. [Google Scholar] [CrossRef]
- Imperatori, C.; Dakanalis, A.; Farina, B.; Pallavicini, F.; Colmegna, F.; Mantovani, F.; Clerici, M. Global Storm of Stress-Related Psychopathological Symptoms: A Brief Overview on the Usefulness of Virtual Reality in Facing the Mental Health Impact of COVID-19. Cyberpsychol Behav. Soc. Netw. 2020, 23, 782–788. [Google Scholar] [CrossRef]
- Di Carlo, F.; Sociali, A.; Picutti, E.; Pettorruso, M.; Vellante, F.; Verrastro, V.; Martinotti, G.; di Giannantonio, M. Telepsychiatry and other cutting-edge technologies in COVID-19 pandemic: Bridging the distance in mental health assistance. Int. J. Clin. Pract. 2021, 75. [Google Scholar] [CrossRef]
- Peng, X.; Menhas, R.; Dai, J.; Younas, M. The COVID-19 Pandemic and Overall Wellbeing: Mediating Role of Virtual Reality Fitness for Physical-Psychological Health and Physical Activity. Psychol. Res. Behav. Manag. 2022, 15, 1741–1756. [Google Scholar] [CrossRef]
| Part A | Demographic, academic and other personal questions (1 to 15, Appendix A) |
| Part B | The Likert-4 DASS21 set of questions (16 to 36, Appendix A) |
| Scores | Stress | Anxiety | Depression | ||||||
|---|---|---|---|---|---|---|---|---|---|
| M (±STD) | Md | N (%) | M (±STD) | Md | N (%) | M (±STD) | Md | N (%) | |
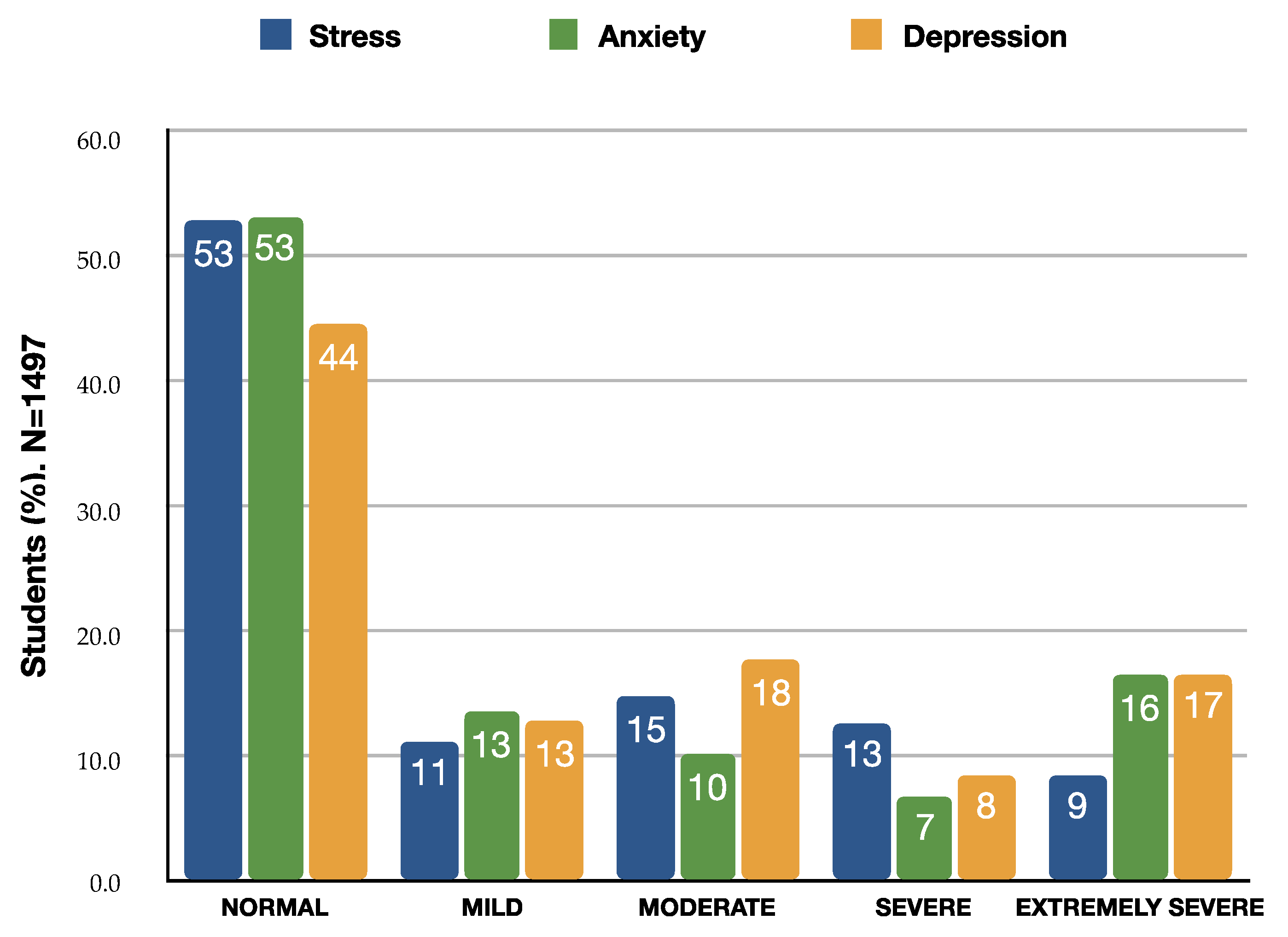
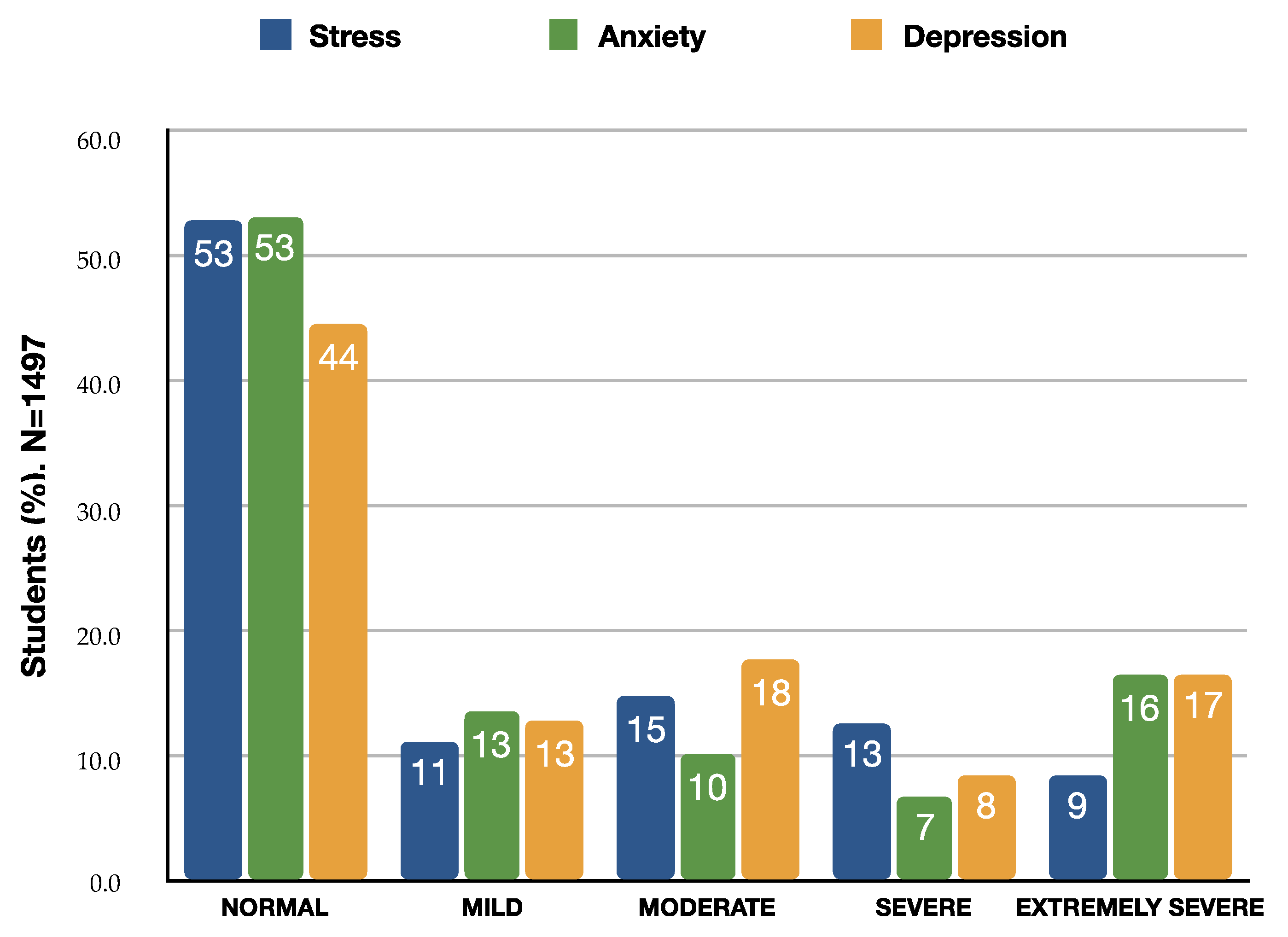
| Normal | 3.58 (±2.36) | 4.0 | 789 (52.7) | 1.22 (±1.11) | 1.0 | 794 (53.0) | 1.68 (±1.47) | 2.0 | 664 (44.4) |
| Mild | 8.47 (±0.50) | 8.0 | 169 (11.3) | 4.45 (±0.50) | 4.0 | 202 (13.5) | 5.47 (±0.50) | 5.0 | 192 (12.8) |
| Moderate | 10.90 (±0.79) | 11.0 | 221 (14.8) | 6.49 (±0.50) | 6.0 | 152 (10.2) | 8.25 (±1.08) | 8.0 | 265 (17.7) |
| Severe | 14.41 (±1.13) | 14.0 | 190 (12.7) | 8.55 (±0.50) | 9.0 | 103 (6.9) | 11.91 (±0.82) | 12.0 | 127 (8.5) |
| Extreme severe | 18.64 (±1.35) | 18.0 | 128 (8.6) | 13.65 (±2.87) | 13.0 | 246 (16.4) | 17.16 (±2.28) | 17.0 | 249 (16.6) |
| Mean (±Standard Deviation) | Stress | Anxiety | Depression | |
|---|---|---|---|---|
| Age range | 18–25 | 8.19 (±5.42) | 5.05 (±4.80) | 7.18 (±5.83) |
| ≥26 | 6.88 (±5.46) | 3.76 (±4.66) | 5.48 (±5.79) | |
| t-test (95% CI) | 1.31 (0.66 to 1.95) ** | 1.30 (0.73 to 1.87) ** | 1.71 (1.02 to 2.40) ** | |
| Gender | Male | 6.47 (±5.28) | 3.70 (±4.29) | 5.91 (±5.65) |
| Female | 8.57 (±5.41) | 5.25 (±4.95) | 7.19 (±5.91) | |
| t-test (95% CI) | 2.10 (1.52 to 2.68) ** | 1.55 (1.04 to 2.06) ** | 1.28 (0.65 to 1.91) ** | |
| Marital status | Unmarried | 5.90 (±5.15) | 2.80 (±3.93) | 3.96 (±4.71) |
| Other | 8.07 (±5.45) | 4.93 (±4.84) | 7.05 (±5.89) | |
| t-test (95% CI) | 2.17 (1.20 to 3.13) ** | 2.13 (1.28 to 2.97) ** | 3.10 (2.07 to 4.13) ** | |
| Cohabitation status | Alone | 8.18 (±5.48) | 4.99 (±4.77) | 7.14 (±6.00) |
| Not Alone | 7.74 (±5.45) | 4.62 (±4.81) | 6.61 (±5.80) | |
| t-test (95% CI) | 0.43 (−0.17 to 1.04) | 0.37 (−0.16 to 0.90) | 0.52 (−0.12 to 1.17) | |
| Vaccinated | Yes | 8.12 (±5.49) | 4.89 (±4.86) | 6.96 (±5.95) |
| No | 6.65 (±5.17) | 3.99 (±4.43) | 5.82 (±5.29) | |
| t-test (95% CI) | 1.47 (0.73 to 2.21) * | 0.90 (0.24 to 1.55) * | 1.14 (0.35 to 1.94) * | |
| Students | BSc/MD | 7.99 (±5.42) | 4.92 (±4.81) | 6.93 (±5.83) |
| MSc/PhD | 7.63 (±5.57) | 4.24 (±4.76) | 6.37 (±5.92) | |
| t-test (95% CI) | 0.36 (−0.28 to 1.00) | 0.68 (0.12 to 1.24) * | 0.56 (−0.12 to 1.24) | |
| Worry/Fear for impending lockdown | Much/Very Much | 9.65 (±6.00) | 6.67 (±5.67) | 8.39 (±6.52) |
| Not at all/A Little | 7.22 (±5.22) | 4.24(±4.42) | 6.36 (±5.62) | |
| t-test (95% CI) | 2.23 (1.55 to 2.91) ** | 2.43 (1.84 to 3.02) * | 2.03 (1.29 to 2.76) | |
| Previous psychological or psychiatric treatment | Yes | 10.21 (±5.67) | 6.73 (±5.32) | 9.22 (±6.34) |
| No | 7.17 (±5.19) | 4.13 (±4.46) | 6.03 (±5.50) | |
| t-test (95% CI) | 3.04 (2.40 to 3.68) ** | 2.60 (2.04 to 3.16) ** | 3.19 (2.50 to 3.87) ** | |
| Current psychological or psychiatric treatment | Yes | 11.63 (±5.64) | 7.88 (±5.59) | 10.82 (±6.59) |
| No | 7.39 (±5.25) | 4.33 (±4.54) | 6.25 (±5.56) | |
| t-test (95% CI) | 4.23 (3.39 to 5.08) ** | 3.55 (2.80 to 4.30) ** | 4.57 (3.66 to 5.48) ** | |
| Current intake of psychoactive medication | Yes | 13.37 (±5.04) | 9.95 (±5.54) | 13.84 (±5.92) |
| No | 7.66 (±5.37) | 4.74 (±4.80) | 6.77 (±5.82) | |
| t-test (95% CI) | 5.71 (4.29 to 7.13) ** | 5.42 (4.17 to 6.66) ** | 7.35 (5.84 to 8.86) ** | |
| Predictors | Stress | Anxiety | Depression | |
|---|---|---|---|---|
| Age range | 18–25 | 0.24 | 0.27 | 0.29 |
| ≥26 | ||||
| Gender | Male | 0.41 | 0.33 | 0.22 |
| Female | ||||
| Marital status | Unmarried | 0.41 | 0.48 | 0.58 |
| Other | ||||
| Cohabitation status | Alone | 0.29 | 0.08 | 0.09 |
| Not Alone | ||||
| Vaccinated | Yes | 0.26 | 0.19 | 0.20 |
| No | ||||
| Students | BSc/MD | 0.07 | 0.14 | 0.10 |
| MSc/PhD | ||||
| Worry/Fear for impending lockdown | Much/Very Much | 0.43 | 0.48 | 0.34 |
| Not at all/A Little | ||||
| Previous psychological or psychiatric treatment | Yes | 0.56 | 0.53 | 0.54 |
| No | ||||
| Current psychological or psychiatric treatment | Yes | 0.78 | 0.70 | 0.75 |
| No | ||||
| Current intake of psychoactive medication | Yes | 1.09 | 1.01 | 1.20 |
| No |
| Mild to Severe Scales | Stress | Anxiety | Depression |
|---|---|---|---|
| Age 18–25 vs. ≥26 | 1.40 | 1.57 | 1.55 |
| Female vs. Male | 1.93 | 1.26 | 1.14 |
| Unmarried vs. Other | 1.62 | 1.46 | 1.46 |
| Vaccinated: Yes vs. No | 1.44 | 1.02 | 1.04 |
| Previous psychological or psychiatric treatment | |||
| Yes vs. No | 1.75 | 1.36 | 1.19 |
| Current psychological or psychiatric treatment | |||
| Yes vs. No | 1.82 | 1.48 | 0.94 |
| Current intake of psychoactive medication | |||
| Yes vs. No | 1.80 | 0.97 | 0.65 |
| Extreme Severe Scale | Stress | Anxiety | Depression |
|---|---|---|---|
| Age: 18–25 vs. ≥26 | 1.33 | 1.60 | 1.44 |
| Female vs. Male | 1.62 | 2.07 | 1.66 |
| Unmarried vs. Other | 2.12 | 3.36 | 3.41 |
| Vaccinated: Yes vs. No | 1.55 | 1.40 | 1.49 |
| Previous psychological or psychiatric treatment | |||
| Yes vs. No | 2.97 | 2.65 | 2.77 |
| Current psychological or psychiatric treatment | |||
| Yes vs. No | 4.53 | 3.57 | 4.09 |
| Current intake of psychoactive medication | |||
| Yes vs. No | 5.09 | 6.79 | 9.11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kavvadas, D.; Kavvada, A.; Karachrysafi, S.; Papaliagkas, V.; Chatzidimitriou, M.; Papamitsou, T. Stress, Anxiety, and Depression Levels among University Students: Three Years from the Beginning of the Pandemic. Clin. Pract. 2023, 13, 596-609. https://doi.org/10.3390/clinpract13030054
Kavvadas D, Kavvada A, Karachrysafi S, Papaliagkas V, Chatzidimitriou M, Papamitsou T. Stress, Anxiety, and Depression Levels among University Students: Three Years from the Beginning of the Pandemic. Clinics and Practice. 2023; 13(3):596-609. https://doi.org/10.3390/clinpract13030054
Chicago/Turabian StyleKavvadas, Dimitrios, Asimoula Kavvada, Sofia Karachrysafi, Vasileios Papaliagkas, Maria Chatzidimitriou, and Theodora Papamitsou. 2023. "Stress, Anxiety, and Depression Levels among University Students: Three Years from the Beginning of the Pandemic" Clinics and Practice 13, no. 3: 596-609. https://doi.org/10.3390/clinpract13030054
APA StyleKavvadas, D., Kavvada, A., Karachrysafi, S., Papaliagkas, V., Chatzidimitriou, M., & Papamitsou, T. (2023). Stress, Anxiety, and Depression Levels among University Students: Three Years from the Beginning of the Pandemic. Clinics and Practice, 13(3), 596-609. https://doi.org/10.3390/clinpract13030054