

Guided Superficial Enhanced Fluid Fat Injection (SEFFI) Procedures for Facial Rejuvenation: An Italian Multicenter Retrospective Case Report
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
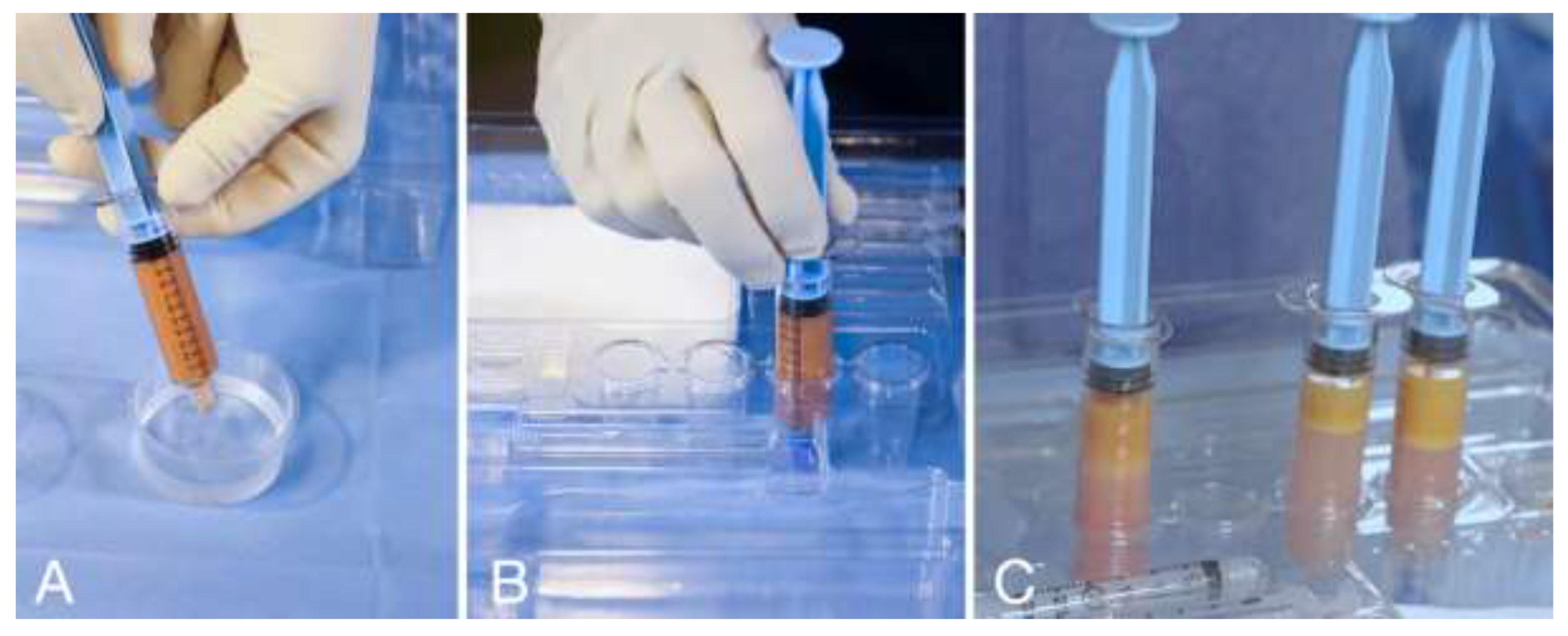
2.1. Adipose Tissue Harvesting Procedure
2.2. Guided SEFFI Single Treatment
2.3. Guided SEFFI and Hyaluronic Acid
2.4. Guided SEFFI and Suspension Threads
2.5. Guided SEFFI and Microneedling
2.6. Guided SEFFI and Botulin Toxin
2.7. Guided SEFFI and Carboxytherapy
2.8. Guided SEFFI and Calcium Hydroxylapatite
2.9. Guided SEFFI and Endolift
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fisher, G.J.; Kang, S.; Varani, J.; Bata-Csorgo, Z.; Wan, Y.; Datta, S.; Voorhess, J.J. Mechanisms of photoaging and chronological skin aging. Arch. Dermatol. 2002, 138, 1462–1470. [Google Scholar] [CrossRef] [PubMed]
- Taub, A.F.; Pham, K. Stem cells in dermatology and anti-aging care of the skin. Facial Plast. Surg. Clin. N. Am. 2018, 26, 425–437. [Google Scholar] [CrossRef]
- Tobin, D.J. Introduction to skin aging. J. Tissue Viability 2017, 26, 37–46. [Google Scholar] [CrossRef] [Green Version]
- Cui, H.; Kong, Y.; Zhang, H. Oxidative stress, mitochondrial dysfunction, and aging. J. Signal Transduct. 2012, 2012, 64635. [Google Scholar] [CrossRef] [Green Version]
- Rohrich, R.J.; Pessa, J.E. The fat compartments of the face: Anatomy and clinical implications for cosmetic surgery. Plast. Reconstr. Surg. 2007, 119, 2219–2227. [Google Scholar] [CrossRef] [Green Version]
- Fitzgerald, R.; Graivier, M.H.; Kane, M.; Lorenc, Z.P.; Vleggaar, D.; Werschler, W.P.; Kenkel, J.M. Facial aesthetic analysis. Aesthetic Surg. J. 2010, 30, S25–S27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCafferty, L.R. The fat compartments of the face: Anatomy and clinical implications for cosmetic surgery. Plast. Reconstr. Surg. 2008, 121, 1061. [Google Scholar] [CrossRef] [PubMed]
- Donofrio, L.M. Fat distribution: A morphologic study of the aging face. Dermatol. Surg. 2000, 26, 1107–1112. [Google Scholar] [CrossRef] [PubMed]
- Gaur, M.; Dobke, M.; Lunyak, V.V. Mesenchymal stem cells from adipose tissue in clinical applications for dermatological indications and skin aging. Int. J. Mol. Sci. 2017, 18, 208. [Google Scholar] [CrossRef] [Green Version]
- Nailor, E.C.; Watson, R.E.; Sherratt, M.J. Molecular aspects of skin ageing. Maturitas 2011, 69, 249–256. [Google Scholar] [CrossRef]
- Cotta-Pereira, G.; Rodrigo, F.G.; Bittencourt-Sampaio, S. Oxytalan, elaulin and elastic fibers in the human skin. J. Investig. Dermatol. 1976, 66, 143–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gennai, A.; Tesauro, P.; Colli, M.; Roda, B.; Zattoni, A. Infranatant portion of microfragmented adipose tissue: A promising source of SVF for the management of androgenic alopecia. J. Regen. Med. 2021, 1–7. [Google Scholar] [CrossRef]
- Ceccarelli, S.; Pontecorvi, P.; Anastasiado, E.; Napoli, C.; Marchese, C. Immunomodulatory Effect of Adipose-Derived Stem Cells: The Cutting Edge of Clinical Application Frontiers in Cell and Developmental. Biology 2020, 8, 236. [Google Scholar]
- Tallone, T.; Realini, C.; Böhmler, A.; Kornfeld, C.; Vassalli, G.; Moccetti, T.; Bardelli, S.; Soldati, G. Adult human adipose tissue contains several types of multipotent cells. J. Cardiovasc. Transl. Res. 2011, 4, 200–210. [Google Scholar] [CrossRef]
- Del Papa, N.; Di Luca, G.; Sambataro, D.; Zaccara, E.; Maglione, W.; Gabrielli, A.; Fraticelli, P.; Moroncini, G.; Beretta, L.; Santianello, A.; et al. Regional implantation of autologous adipose tissue-derived cells induces a prompt healing of long-lasting indolent digital ulcers in patients with systemic sclerosis. Cell Transplant. 2015, 24, 2297–2305. [Google Scholar] [CrossRef]
- Rigotti, G.; Marchi, A.; Galiè, M.; Baroni, G.; Benati, D.; Krampera, M.; Pasini, A.; Sbarbati, A. Clinical treatment of radiotherapy tissue damage by lipoaspirate transplant: A healing process mediated by adipose-derived adult stem cells. Plast. Reconstr. Surg. 2007, 119, 1409–1422. [Google Scholar] [CrossRef]
- Rossi, M.; Roda, B.; Zia, S.; Vigliotta, I.; Zannini, C.; Alviano, F.; Bonsi, L.; Zattoni, A.; Reschiglian, P.; Gennai, A. Characterization of the Tissue and Stromal Cell Components of Micro-Superficial Enhanced Fluid Fat Injection (Micro-SEFFI) for Facial Aging Treatment. Aesthetic Surg. J. 2018, 40, 679–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogura, F.; Wakao, S.; Kuroda, Y.; Tsuchiyama, K.; Bagheri, M.; Heneidi, S.; Chazenbalk, G.; Aiba, S.; Dezawa, M. Human Adipose Tissue Possesses a Unique Population of Pluripotent Stem Cells with Nontumorigenic and Low Telomerase Activities: Potential Implications in Regenerative Medicine. Stem Cell Dev. 2013, 2, 7. [Google Scholar] [CrossRef]
- Planat-Benard, V.; Silvestre, J.S.; Cousin, B.; André, M.; Nibbelink, M.; Tamarat, R.; Clergue, M.; Manneville, C.; Saillan-Barreau, C.; Duriez, M.; et al. Plasticity of human adipose lineage cells toward endothelial cells: Physiological and therapeutic perspectives. Circulation 2004, 109, 656–663. [Google Scholar] [CrossRef]
- Trivisonno, A.; Di Rocco, G.; Cannistra, C.; Finocchi, V.; Farr, S.T.; Monti, M.; Toietta, G. Harvest of superficial layers of fat with a microcannula and isolation of adipose tissue-derived stromal and vascular cells. Aesthetic Surg. J. 2014, 34, 601–613. [Google Scholar] [CrossRef] [Green Version]
- Zeltzer, A.A.; Tonnard, P.L.; Verpaele, A.M. Sharp-needle intradermal fat grafting (SNIF). Aesthetic Surg. J. 2012, 32, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Senesi, L.; De Francesco, F.; Farinelli, L.; Manzotti, S.; Gagliardi, G.; Papalla, G.F.; Riccio, M.; Gigante, A. Mechanical and Enzymatic Procedures to Isolate the Stromal Vascular Fraction from Adipose Tissue: Preliminary Results. Front. Cell Dev. Biol. 2019, 7, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubina, K.; Kalinina, N.; Efimenko, A.; Lopatina, T.; Melikhova, V.; Tsokolaeva, Z.; Sysoeva, V.; Tkachk, V.; Parfyonova, Y. Adipose stromal cells stimulate angiogenesis via promoting progenitor cell differentiation, secretion of angiogenic factors, and enhancing vessel maturation. Tissue Eng. Part A 2009, 15, 2039–2050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, L.; Johnstone, B.H.; Cook, T.G.; Tan, J.; Fishbein, M.C.; Chen, P.S.; Marcha, K.L. IFATS Collection: Human Adipose Tissue-Derived Stem Cells Induce Angiogenesis and Nerve Sprouting Following Myocardial Infarction, in Conjunction with Potent Preservation of Cardiac Function. Stem Cells 2009, 27, 230–237. [Google Scholar] [CrossRef] [Green Version]
- Cao, Y.; Sun, Z.; Liao, L.; Meng, Y.; Han, Q.; Zhao, R.C. Human adipose tissue-derived stem cells differentiate into endothelial cells in vitro and improve postnatal neovascularization in vivo. Biochem. Biophys. Res. Commun. 2005, 332, 370–379. [Google Scholar] [CrossRef]
- Guo, J.; Dardik, A.; Fang, K.; Huang, R.; Gu, Y. Meta-analysis on the treatment of diabetic foot ulcers with autologous stem cells. Stem Cell Res. Ther. 2017, 8, 228. [Google Scholar] [CrossRef]
- Akita, S.; Akino, K.; Hirano, A.; Ohtsuru, A.; Yamashita, S. Noncultured Autologous Adipose-Derived Stem Cells Therapy for Chronic Radiation Injury. Stem Cells Int. 2010, 2010, 532704. [Google Scholar] [CrossRef] [Green Version]
- Bernardini, F.P.; Gennai, A.; Izzo, L.; Zambelli, A.; Repaci, E.; Baldelli, I.; Fraternali-Orcioni, G.; Hartstein, M.E.; Santi, P.L.; Quarto, R. Superficial Enhanced Fluid Fat Injection (SEFFI) to Correct Volume Defects and Skin Aging of the Face and Periocular Region. Aesthetic Surg. J. 2015, 35, 504–515. [Google Scholar] [CrossRef] [Green Version]
- Bernardini, F.P.; Gennai, A. Superficial Enhanced Fluid Fat Injection for Volume Restoration and Skin Regeneration of the Periocular Aesthetic Unit. An Improved Fat Grafting Technique to enhance the beauty of the eye. JAMA Plast. Facial Surg. 2016, 18, 1. [Google Scholar] [CrossRef]
- Ghatge, A.S.; Ghatge, S.B. The Effectiveness of Injectable Hyaluronic Acid in the Improvement of the Facial Skin Quality: A Systematic Review. Clin. Cosmet. Investig. Dermatol. 2023, 16, 891–899. [Google Scholar] [CrossRef]
- Gennai, A.; Zambelli, A.; Repaci, E.; Quarto, R.; Baldelli, I.; Fraternali, G.; Bernardini, F.P. Skin Rejuvenation and Volume Enhancement with the Micro Superficial Enhanced Fluid Fat Injection (M-SEFFI) for Skin Aging of the Periocular and Perioral Regions. Aesthetic Surg. J. 2017, 37, 14–23. [Google Scholar] [CrossRef] [Green Version]
- Gennai, A.; Bernardini, F.P. Rejuvenation faciale par lifting endoscopique avec le petite incision incision vertical associée à une injection superficielle de graisse: Un repositionement endoscopique, une regeneration tissulaire et une restauration volumetrique (La technique R3). J. Med. Esth. Chir. Derm. 2017, 174, 87–95. (In French) [Google Scholar]
- Pignata, G.; Gennai, A.; Bernardini, F.P. Rejuvenation of the centre of the face: A new paradigm Endoscopic lifting with fat grafting. Plast. Aesthet. Res. 2018, 5, 23. [Google Scholar] [CrossRef]
- Gennai, A.; Bovani, B.; Colli, M.; Melfa, F.; Piccolo, D.; Russo, R.; Roda, B.; Zattoni, A.; Reschiglian, P.; Zia, S. Comparison of Harvesting and Processing Technique for Adipose Tissue Graft: Evaluation of Cell Viability. Int. J. Regen. Med. 2021, 4, 2–5. [Google Scholar] [CrossRef]
- Gennai, A.; Bernardini, F.P.; Baldessin, M.; Bovani, B.; Camporese, A.; Colli, M.; Diaspro, A.; Melfa, F.; Piccolo, D.; Russo, R.; et al. Evaluation of the Viability and Phenotype of Adipose Derived Cells Harvested Using Different Harvesting and Processing Procedures: A Pilot Study. J. Stem Cells Clin. Pract. 2022, 2, 101. [Google Scholar]
- Gennai, A.; Zia, S.; Roda, B.; Maggio, A.; Bonsi, L.; Alviano, F.; Zattoni, A.; Reschiglian, P.; Bernardini, F.P. SEFFI (Superficial Enhanced Fluid Fat Injection) for aesthetic and clinical regenerative treatments. Glob. J. Dermatol. Venereol. 2020, 8, 32–40. [Google Scholar] [CrossRef]
- Cucchiani, M.D.R.; Luis Corrales, M.D. The Effects of Fat Harvesting and Preparation, Air Exposure, Obesity, and Stem Cell Enrichment on Adipocyte Viability Prior to Graft Transplantation. Aesthetic Surg. J. 2016, 36, 1164–1173. [Google Scholar] [CrossRef]
- Charles de Sá, L.; Gontijo de Amorim, N.F.; Takiya, C.M.; Borojevic, R.; Benati, D.; Bernardi, P.; Sbarbati, A.; Rigotti, G. Antiaging treatment of the facial skin by fat graft and adipose-derived stem cells. Plast. Reconstr. Surg. 2015, 135, 999–1009. [Google Scholar] [CrossRef] [Green Version]
- Gennai, A.; Bovani, B.; Colli, M.; Melfa, F.; Piccolo, D.; Russo, R.; Clementoni, M.T.; Zia, S.; Roda, B.; Zattoni, A. Evaluation of the Number, Biophysical and Multipotent Characteristics of Adipose Derived Stem Cells Harvested by SEFFI Procedure and Interaction with Different Type of Hyaluronic Acids. Int. J. Regen. Med. 2021, 4, 2–10. [Google Scholar] [CrossRef]
- Molliard, S.G.; Bétemps, J.B.; Hadjab, B.; Topchian, D.; Micheels, P.; Salomon, D. Key rheological properties of hyaluronic acid fillers: From tissue integration to product degradation. Plast. Aesthet. Res. 2018, 5, 17. [Google Scholar] [CrossRef] [Green Version]
- Altman, A.M.; Khalek, F.J.A.; Seidensticker, M.; Minilla, S.; Yan, Y.; Coleman, M.; Song, Y.H.; Butler, C.E.; Alt, E.U. Human tissue-resident stem cells combined with hyaluronic acid gel provide fibrovascular-integrated soft-tissue augmentation in a murine photoaged skin model. Plast. Reconstr. Surg. 2010, 125, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Colli, M.; Gennai, A.; Russo, R.; Tomeo, A.; Bovani, B.; Piccolo, D.; Melfa, F.; Tesauro, P.; Diaspro, A. Non-surgical Jowl and Jawline Rejuvenation with Resorbable Suspension Threads and Superficial Enhanced Fluid Fat Injection (SEFFI). J. Reg. Med. Biol. Res. 2022, 3, 1–19. [Google Scholar] [CrossRef]
- Zduńska, K.; Kołodziejczak, A.; Rotsztejn, H. Is skin microneedling a good alternative method of various skin defects removal. Dermatol. Ther. 2018, 31, e12714. [Google Scholar] [CrossRef]
- Gentile, P.; Garcovich, S. Adipose-Derived Mesenchymal Stem Cells (AD-MSCs) against Ultraviolet (UV) Radiation Effects and the Skin Photoaging. Biomedicines 2021, 9, 532. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Zhang, D.; Wu, H.; Xie, S.; Zhang, M.; Zhang, B.; Tang, S. Basic Fibroblast Growth Factor Influences Epidermal Homeostasis of Living Skin Equivalents through Affecting Fibroblast Phenotypes and Functions. Skin Pharmacol. Physiol. 2018, 31, 229–237. [Google Scholar] [CrossRef]
- Carruthers, A.; Carruthers, J. Botulinum toxin. In Dermatology, 2nd ed.; Bolognia, J.L., Jorizzo, J.L., Rapini, R.P., Eds.; Mosby Elsevier: New York, NY, USA, 2008; pp. 2381–2390. [Google Scholar]
- Gart, M.S.; Gutowski, K.A. Overview of botulinum toxins for aesthetic uses. Clin. Plast. Surg. 2016, 43, 459–471. [Google Scholar] [CrossRef]
- Satriyasa, B.K. Botulinum toxin (Botox) A for reducing the appearance of facial wrinkles: A literature review of clinical use and pharmacological aspect. Clin. Cosmet. Investig. Dermatol. 2019, 12, 223–228. [Google Scholar] [CrossRef] [Green Version]
- Kroumpouzos, G.; Arora, G.; Kassir, M.; Galadari, H.; Wollina, U.; Lotti, T.; Grabbe, S.; Goldust, M. Carboxytherapy in dermatology. Clin. Dermatol. 2022, 40, 305–309. [Google Scholar] [CrossRef]
- El-Domyati, M.; El-Din, W.H.; Medhat, W.; Ibrahim, M.R.; Khaled, Y. The use of Carboxytherapy alone or in combination with fractional CO2 laser for facial rejuvenation: A split-face comparative study. J. Cosmet. Dermatol. 2020, 19, 1648–1655. [Google Scholar] [CrossRef]
- Courderot-Masuyer, C.; Robin, S.; Tauzin, H.; Humbert, P. Evaluation of lifting and antiwrinkle effects of calcium hydroxylapatite filler. In vitro quantification of contractile forces of human wrinkle and normal aged fibroblasts treated with calcium hydroxylapatite. J. Cosmet. Dermatol. 2016, 15, 260–268. [Google Scholar] [CrossRef]
- Lorenc, Z.P.; Bass, L.M.; Fitzgerald, R.; Goldberg, D.J.; Graivier, M.H. Physiochemical Characteristics of Calcium Hydroxylapatite (CaHA). Aesthetic Surg. J. 2018, 38 (Suppl. S1), S8–S12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rovatti, P.P.; Pellacani, G.; Guida, S. Hyperdiluted Calcium Hydroxylapatite 1:2 for Mid and Lower Facial Skin Rejuvenation: Efficacy and Safety. Dermatol. Surg. 2020, 46, e112–e117. [Google Scholar] [CrossRef] [PubMed]
- Bartoletti, E.; Melfa, F.; Renzi, M.; Rovatti, P. Systematic review of the literature on the properties, quality and reliability of calcium hydroxyapatite: Results of an Italian experts’ meeting. Aesthetic Med. 2022, 8. [Google Scholar]
- Coleman, S.R. Structural fat grafts: The ideal filler? Clin. Plast. Surg. 2001, 28, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Tonnard, P.L.; Verpaele, A.M.; Peeters, G.; Hamdi, M.; Cornelissen, M.; Declercq, H. Nanofat grafting basic research and clinical applications. Plast. Reconstr. Surg. J. 2013, 132, 1017–1026. [Google Scholar] [CrossRef]
- Bernardini, F.P.; Gennai, A.; Izzo, L.; Devoto, M.H. Minimal incisions vertical endoscopic lifting and fat grafting as a systematic approach to the rejuvenation of the periocular esthetic unit. Ophthalmic Plast. Reconstr. Surg. 2013, 29, 308–315. [Google Scholar] [CrossRef]
- Nguyen, P.S.; Desouches, C.; Gay, A.M.; Hautier, A.; Magalon, G. Development of micro-injection as an innovative autologous fat graft technique: The use of adipose tissue as dermal filler. J. Plast. Reconstr. Aesthet. Surg. 2012, 65, 1692–1699. [Google Scholar] [CrossRef] [PubMed]
- James, I.B.; Coleman, S.R.; Rubin, J.P. Fat, stem cells, and platelet-rich plasma. Clin. Plast. Surg. 2016, 43, 473–488. [Google Scholar] [CrossRef]
- Mengzhu, L.V.; Zhang, S.; Jiang, B.; Cao, S.; Dong, Y.; Cao, L.; Guo, S. Adipose Adipose-derived stem cells regulate metabolic homeostasis and delay aging by promoting mitophagy. J. FASEB 2021, 35, e21709. [Google Scholar]
- Kikap, K.; Fan, Y.; Lin, G.; Park, Y.K.; Pak, C.S.; Jeong, J.H.; Kim, S. Synergistic Effect of Adipose-Derived Stem Cells and Fat Graft on Wrinkles in Aged Mice. Plast. Reconstr. Surg. 2019, 143, 1637–1646. [Google Scholar]
- Di Taranto, G.; Cicione, C.; Visconti, G.; Isgrò, M.A.; Barba, M.; Di Stasio, E.; Stigliano, E.; Bernardini, C.; Michetti, F.; Salgarello, M.; et al. Qualitative and quantitative differences of adipose-derived stromal cells from superficial and deep subcutaneous lipoaspirates: A matter of fat. Cytotherapy 2015, 17, 1076–1089. [Google Scholar] [CrossRef] [PubMed]
- Schiraldi, L.; Sapino, G.; Meuli, J.; Maruccia, M.; Cherubino, M.; Raffoul, W.; di Summa, P.G. Facial Fat Grafting (FFG): Worth the Risk? A Systematic Review of Complications and Critical Appraisal. J. Clin. Med. 2022, 11, 4708. [Google Scholar] [CrossRef] [PubMed]
- Clauser, L.; Lucchi, A.; Tocco-Tussardi, I.; Gardin, C.; Zavan, B. Autologous Fat Transfer for Facial Augmentation and Regeneration: Role of Mesenchymal Stem Cells. Atlas Oral. Maxillofac. Surg. Clin. N. Am. 2018, 26, 25–32. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Fat harvesting | Donor site | Avarage harvested volume (mL) | Number of patients (%) |
| Abdomen | 27.1 | 1231 (52.1) | |
| Thocantheric | 27.1 | 761 (32.4) | |
| Hip | 22.6 | 296 (12.6) | |
| Knee | 6.8 | 67 (2.8) | |
| Others | 2.1 | 3 (0.1) | |
| SEFFI injection | Injection area | Avarage injected volume (mL) | Number of patients (%) |
| Single area | Reriocular | 1.4 | 63 (2.7) |
| Temporal | 1.1 | 5 (0.2) | |
| Malar-zygomatic | 4.4 | 233 (9.9) | |
| Perioral–lip | 1.3 | 34 (1.4) | |
| Jawline | 2.8 | 91 (3.8) | |
| Other | 5.2 | 14 (0.6) | |
| Total | 440 (18.6) | ||
| Combined area | Full face | 14.8 | 557 (23.6) |
| Two areas | 5.1 | 561 (23.7) | |
| Three areas | 2.8 | 639 (27.0) | |
| Four areas | 8.3 | 246 (10.4) | |
| Total | 1935 (81.4) |
| Guided SEFFI Procedures | Number of Procedures | Percentage of Patients | |
|---|---|---|---|
| Single procedure | 1484 | 62.7 | |
| Combined procedures | Botulin toxin | 295 | 12.5 |
| Hyaluronic acids | 233 | 9.9 | |
| Threads | 122 | 5.2 | |
| Microneedling | 85 | 3.6 | |
| Calcium hydroxylapatite | 65 | 2.7 | |
| Carboxytherapy | 51 | 2.6 | |
| Endolift | 24 | 1.0 | |
| Other | 0 | 0 | |
| Total | 875 | 37.0 |
| Site of Complication | Type of Complication | Number of Events | Percentage of Patients |
|---|---|---|---|
| Donor site | Ecchymosis | 336 | 14.2 |
| Hematoma | 31 | 1.3 | |
| Prolonged erythema (>48 h) | 0 | 0 | |
| Skin necrosis | 0 | 0 | |
| Prolonged edema (>20 days) | 0 | 0 | |
| Infection | 0 | 0 | |
| Fat necrosis | 0 | 0 | |
| Telangiectasias | 0 | 0 | |
| Skin irregularities (>20 days) | 5 | 0.2 | |
| Embolism | 0 | 0 | |
| Other | 0 | 0 | |
| Injection site | Ecchymosis | 914 | 38.6 |
| Hematoma | 18 | 0.8 | |
| Prolonged erythema (>48 h) | 0 | 0 | |
| Skin necrosis | 0 | 0 | |
| Prolonged edema (>5 days) | 14 | 0.6 | |
| Infection | 1 | <0.1 | |
| Fat necrosis | 0 | 0 | |
| Telangiectasias | 0 | 0 | |
| Activation of acne | 0 | 0 | |
| Visibility | 2 | 0.1 | |
| Skin irregularities (>48 h) | 1 | <0.1 | |
| Blindness | 0 | 0 | |
| Asymmetry | 3 | 0.1 | |
| Other | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gennai, A.; Baldessin, M.; Melfa, F.; Bovani, B.; Camporese, A.; Claysset, B.; Colli, M.; Diaspro, A.; Russo, R.; Strano, P.; et al. Guided Superficial Enhanced Fluid Fat Injection (SEFFI) Procedures for Facial Rejuvenation: An Italian Multicenter Retrospective Case Report. Clin. Pract. 2023, 13, 924-943. https://doi.org/10.3390/clinpract13040085
Gennai A, Baldessin M, Melfa F, Bovani B, Camporese A, Claysset B, Colli M, Diaspro A, Russo R, Strano P, et al. Guided Superficial Enhanced Fluid Fat Injection (SEFFI) Procedures for Facial Rejuvenation: An Italian Multicenter Retrospective Case Report. Clinics and Practice. 2023; 13(4):924-943. https://doi.org/10.3390/clinpract13040085
Chicago/Turabian StyleGennai, Alessandro, Monica Baldessin, Fabrizio Melfa, Bruno Bovani, Alessandra Camporese, Barbara Claysset, Mattia Colli, Alberto Diaspro, Rosalba Russo, Placido Strano, and et al. 2023. "Guided Superficial Enhanced Fluid Fat Injection (SEFFI) Procedures for Facial Rejuvenation: An Italian Multicenter Retrospective Case Report" Clinics and Practice 13, no. 4: 924-943. https://doi.org/10.3390/clinpract13040085