

Hypercalcemic Crisis Due to a Giant Intrathyroidal Parathyroid Adenoma, with Postsurgical Severe Hypocalcemia and Hungry Bone Syndrome: A Case Report

 , and
, and
Abstract
1. Introduction
2. Case Presentation
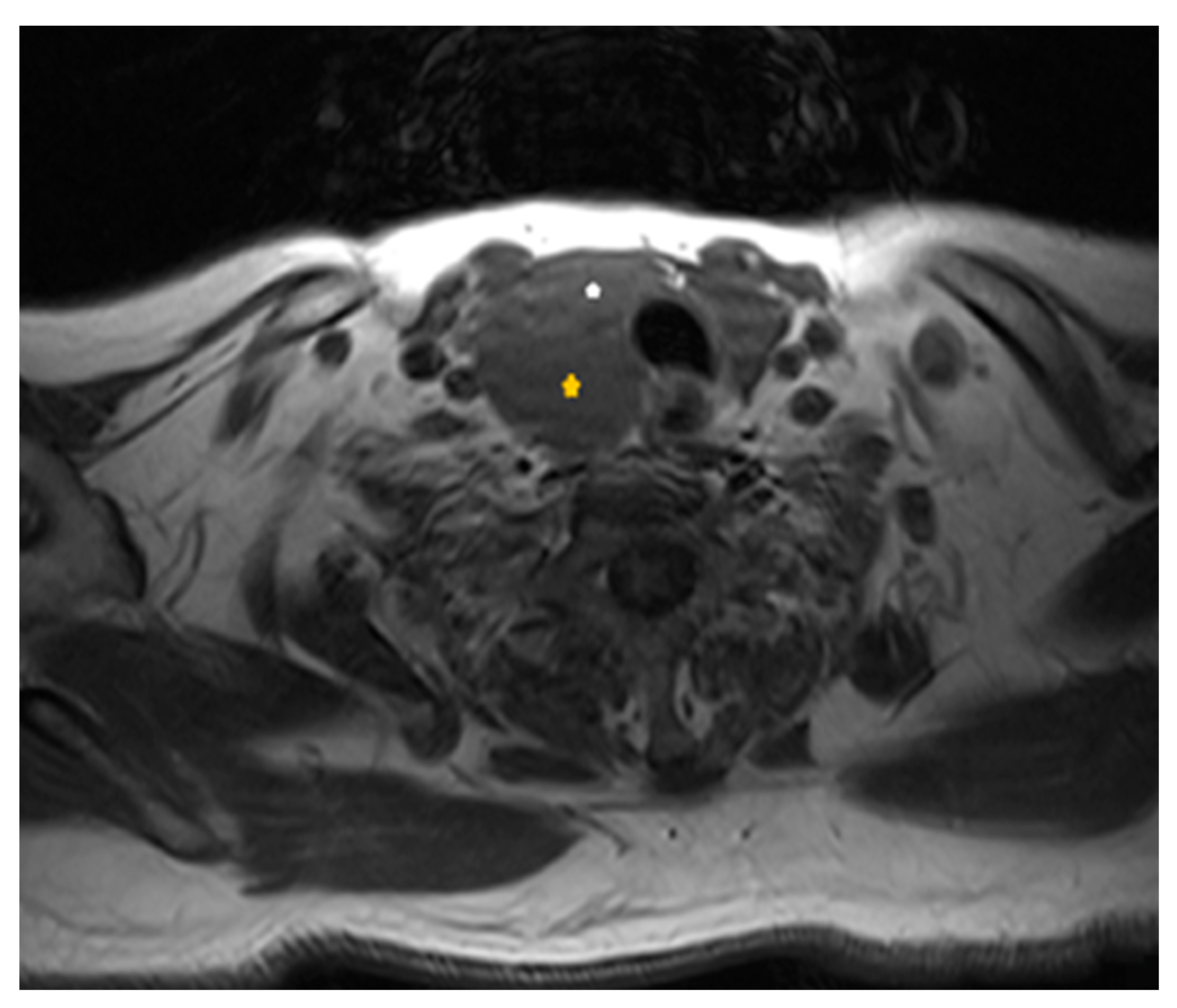
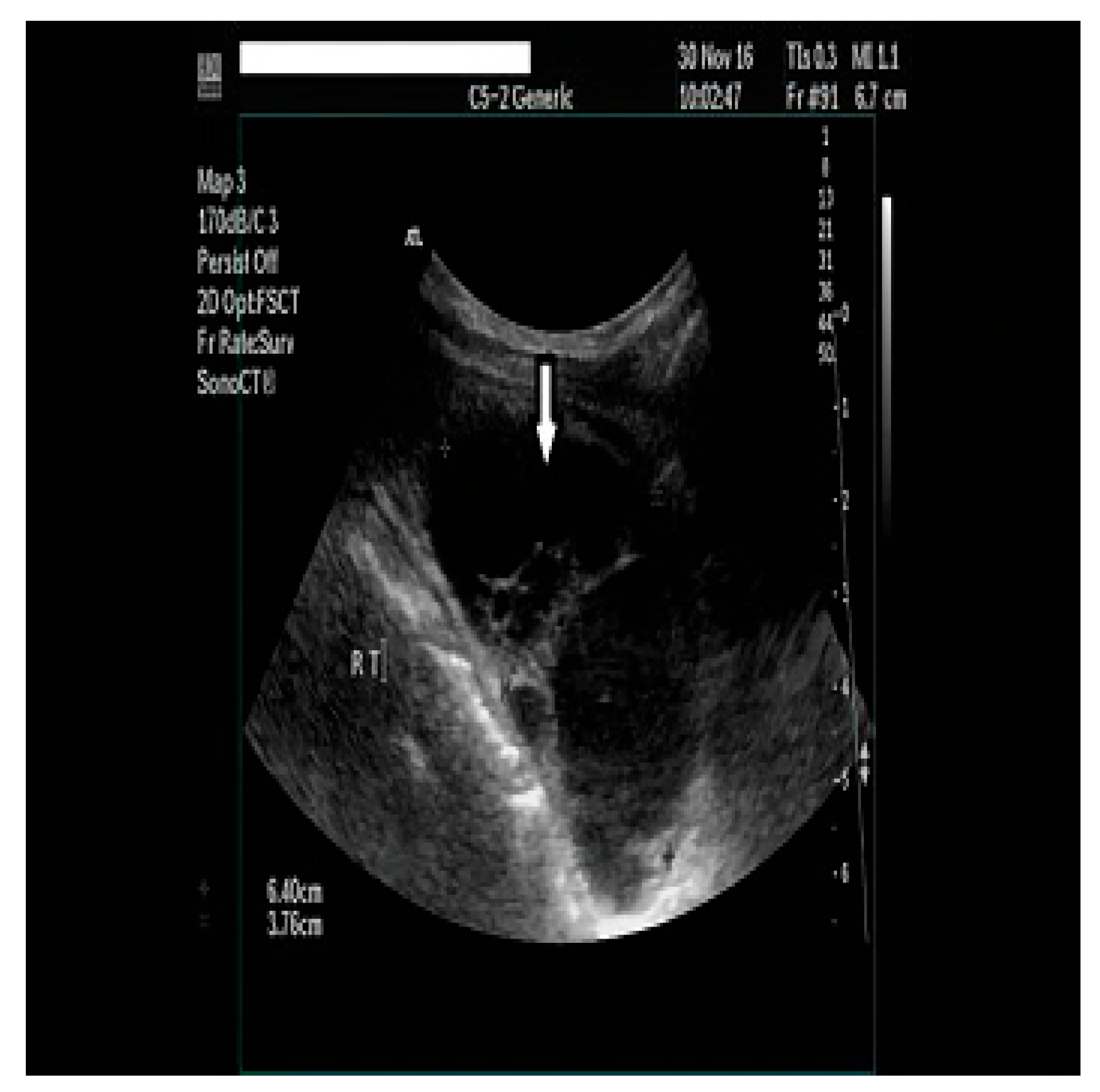
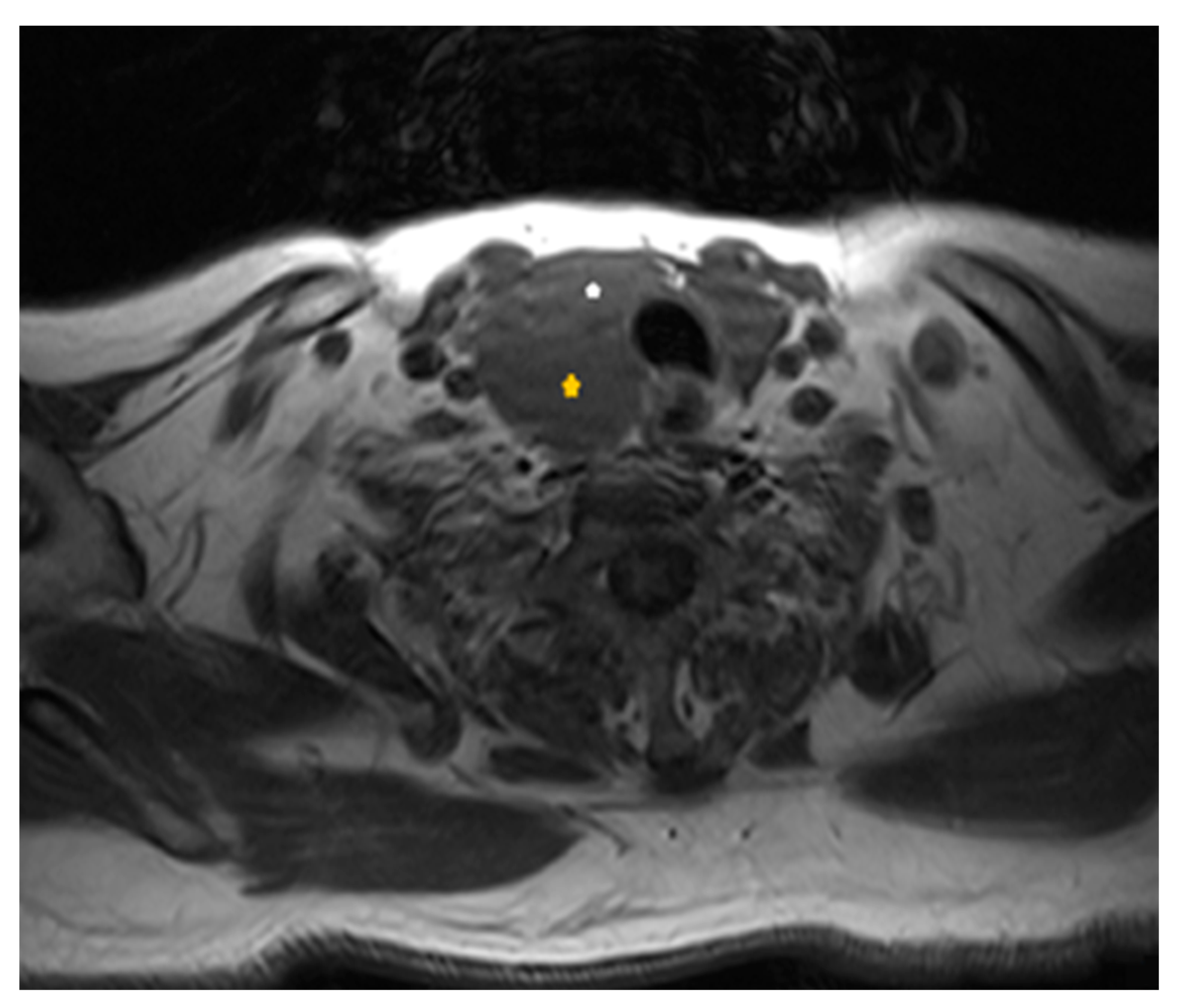
2.1. Diagnostic Assessment
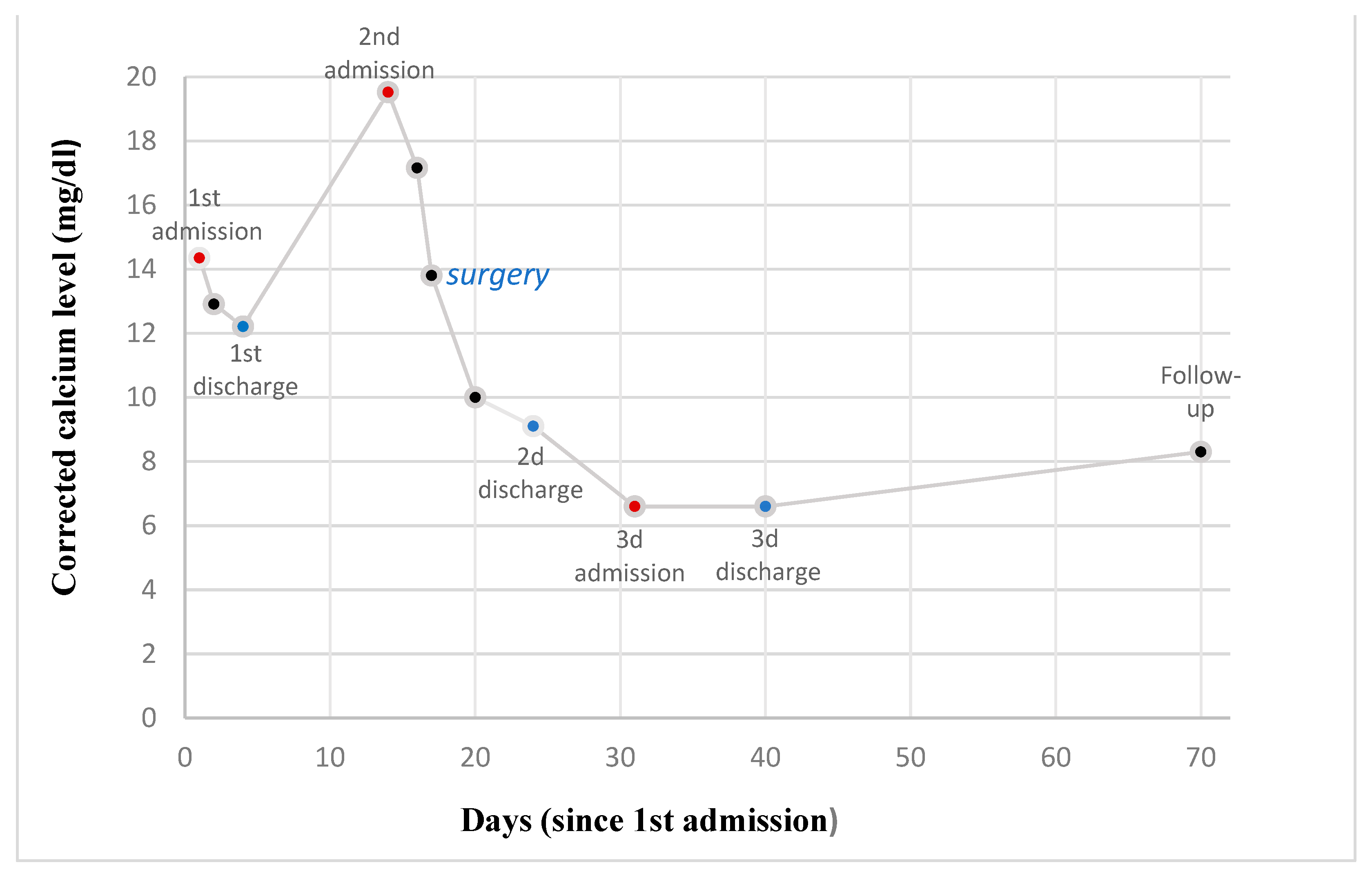
2.2. Treatment
2.3. Outcome and Follow-Up
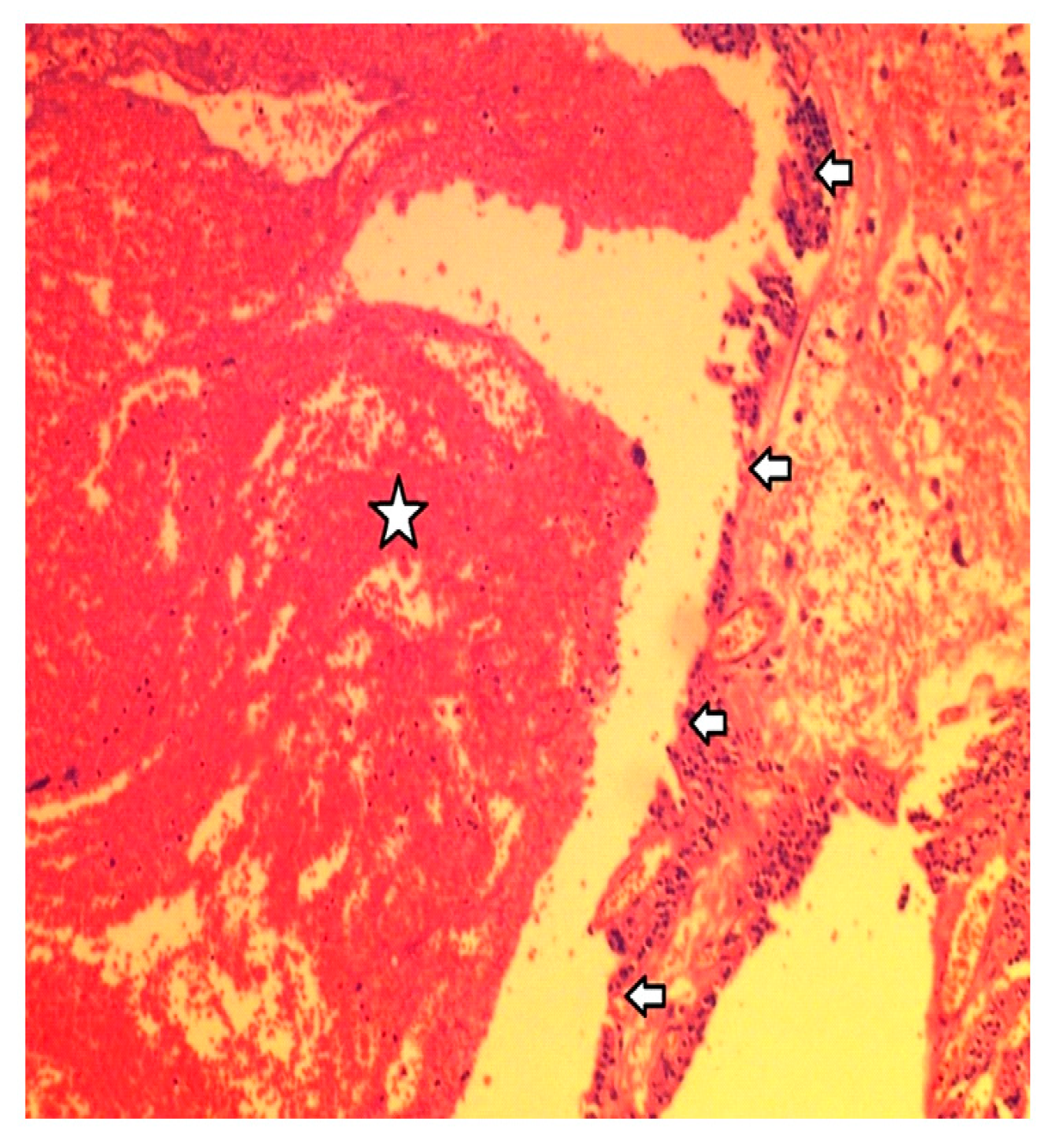
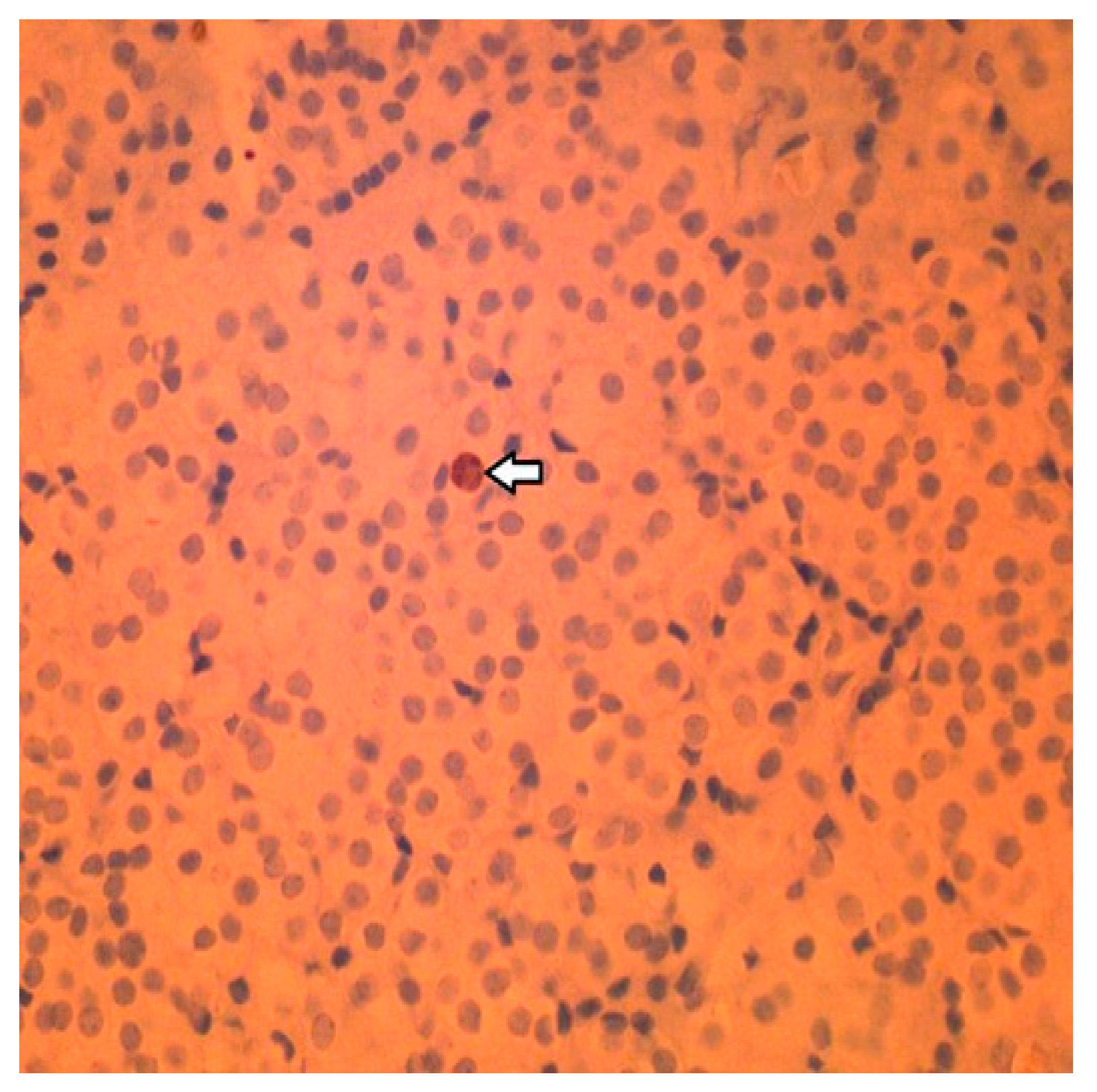
2.4. Histology
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pallan, S.; Rahman, M.O.; Khan, A.A. Diagnosis and management of primary hyperparathyroidism. BMJ 2012, 344, e1013. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.; Kuraganti, G.; Steenkamp, D. Hypercalcemic crisis: A clinical review. Am. J. Med. 2015, 128, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Insogna, K.L. Primary Hyperparathyroidism. N. Engl. J. Med. 2018, 379, 1050–1059. [Google Scholar] [CrossRef] [PubMed]
- Marcocci, C.; Cetani, F. Clinical practice. Primary hyperparathyroidism. N. Engl. J. Med. 2011, 365, 2389–2397. [Google Scholar] [CrossRef] [PubMed]
- Zuberi, K.A.; Urquhart, A.C. Serum PTH and ionized calcium levels as predictors of symptomatic hypocalcemia after parathyroidectomy. Laryngoscope 2010, 120 (Suppl. S4), S192. [Google Scholar] [CrossRef] [PubMed]
- Anwar, F.; Abraham, J.; Nakshabandi, A.; Lee, E. Treatment of hypocalcemia in hungry bone syndrome: A case report. Int. J. Surg. Case Rep. 2018, 51, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Richards, M.L.; Thompson, G.B.; Farley, D.R.; Grant, C.S. An optimal algorithm for intraoperative parathyroid hormone monitoring. Arch. Surg. 2011, 146, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Fraser, W.D. Hyperparathyroidism. Lancet 2009, 374, 145–158. [Google Scholar] [CrossRef] [PubMed]
- Aygün, N.; Uludağ, M. Surgical Treatment of Primary Hyperparathyroidism: Which Therapy to Whom? Sisli Etfal Hastan. Tip Bul. 2019, 53, 201–214. [Google Scholar] [CrossRef] [PubMed]
- Boonen, S.; Haentjens, P.; Vandenput, L.; Vanderschueren, D. Preventing osteoporotic fractures with antiresorptive therapy: Implications of microarchitectural changes. J. Intern. Med. 2004, 255, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Farford, B.; Presutti, R.J.; Moraghan, T.J. Nonsurgical management of primary hyperparathyroidism. Mayo Clin. Proc. 2007, 82, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Norasyikin, A.W.; Nani, M.L. The role of intra-operative parathyroid hormone assay in non-localized adenoma. Pak. J. Med. Sci. 2022, 38, 2376–2379. [Google Scholar] [CrossRef]
- Papavramidis, T.S.; Chorti, A.; Pliakos, I.; Panidis, S.; Michalopoulos, A. Parathyroid cysts: A review of 359 patients reported in the international literature. Medicine 2018, 97, e11399. [Google Scholar] [CrossRef] [PubMed]
- Witteveen, J.E.; van Thiel, S.; Romijn, J.A.; Hamdy, N.A.T. Therapy of Endocrine Disease: Hungry bone syndrome: Still a challenge in the post-operative management of primary hyperparathyroidism: A systematic review of the literature. Eur. J. Endocrinol. 2013, 168, R45–R53. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Test Name | Initial Laboratory Values | Highest Values Observed | Reference Range |
|---|---|---|---|
| Calcium, serum (Ca) | 3.6 | 4.9 | 2.1–2.5 mmol/L |
| Parathyroid hormone (PTH) | 47.6 | 225.3 | 1.0–6.5 pmol/L |
| Creatinine, serum (CREA) | 97 | 495 | 53–124 Umol/L |
| Alkaline phosphatase (ALP) | 85 | 86 | 23–129 U/L |
| Alboumin (ALB) | 44 | 46 | 35–50 g/L |
| Magnesium (MG) | 0.7 | 0.5 | 0.6–1.0 mmol/L |
| Phosphorus (PHOS) | 1.2 | 1.5 | 0.8–1.3 mmol/L |
| Thyroid-stimulating hormone (TSH) | N/A | 19.3 | 0.3–4.7 mlU/L |
| 24 h urine total metanephrines | 2576 | 2576 | 449–2264 nmol/24 h |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papanikos, V.; Papadodima, E.; Bantouna, D.; Paparodis, R.D.; Livadas, S.; Angelopoulos, N.; Karvounis, E. Hypercalcemic Crisis Due to a Giant Intrathyroidal Parathyroid Adenoma, with Postsurgical Severe Hypocalcemia and Hungry Bone Syndrome: A Case Report. Clin. Pract. 2024, 14, 179-187. https://doi.org/10.3390/clinpract14010015
Papanikos V, Papadodima E, Bantouna D, Paparodis RD, Livadas S, Angelopoulos N, Karvounis E. Hypercalcemic Crisis Due to a Giant Intrathyroidal Parathyroid Adenoma, with Postsurgical Severe Hypocalcemia and Hungry Bone Syndrome: A Case Report. Clinics and Practice. 2024; 14(1):179-187. https://doi.org/10.3390/clinpract14010015
Chicago/Turabian StylePapanikos, Vasileios, Elli Papadodima, Dimitra Bantouna, Rodis D. Paparodis, Sarantis Livadas, Nicholaos Angelopoulos, and Evangelos Karvounis. 2024. "Hypercalcemic Crisis Due to a Giant Intrathyroidal Parathyroid Adenoma, with Postsurgical Severe Hypocalcemia and Hungry Bone Syndrome: A Case Report" Clinics and Practice 14, no. 1: 179-187. https://doi.org/10.3390/clinpract14010015
APA StylePapanikos, V., Papadodima, E., Bantouna, D., Paparodis, R. D., Livadas, S., Angelopoulos, N., & Karvounis, E. (2024). Hypercalcemic Crisis Due to a Giant Intrathyroidal Parathyroid Adenoma, with Postsurgical Severe Hypocalcemia and Hungry Bone Syndrome: A Case Report. Clinics and Practice, 14(1), 179-187. https://doi.org/10.3390/clinpract14010015