
Full Familiarisation Is Not Required for the Self-Paced 1 km Treadmill Walk to Predict Peak Oxygen Uptake in Phase IV Cardiac Patients



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Ethical Approval
2.2. Experimental Visits
2.3. Statistical Analysis
3. Results
3.1. Baseline Observations at Rest
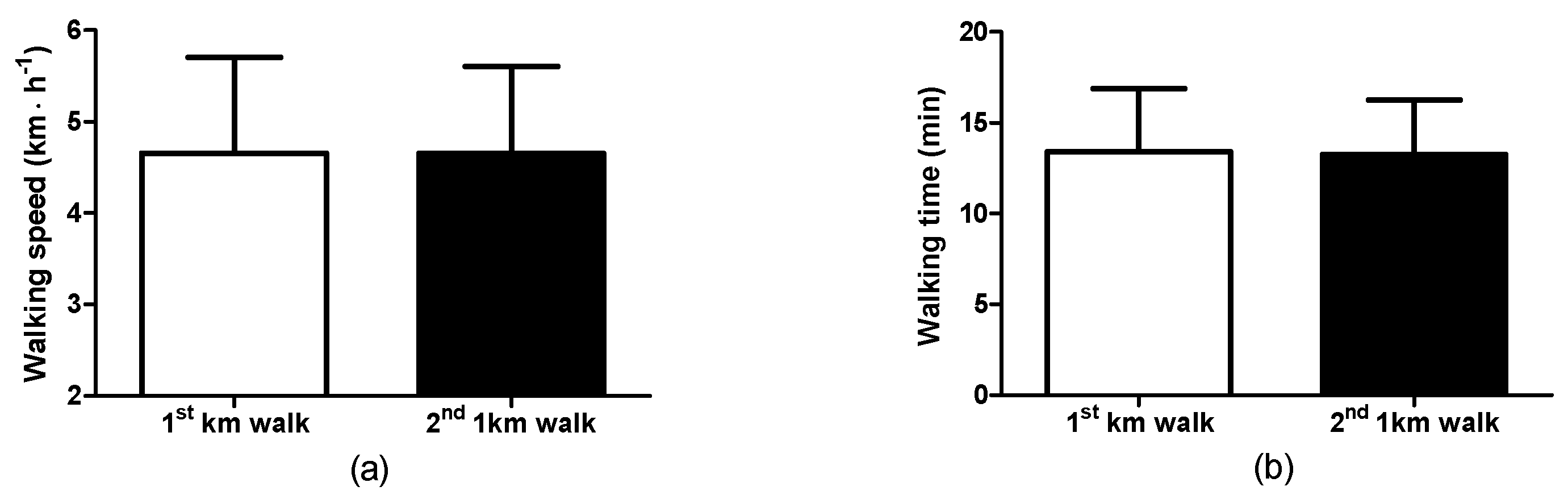
3.2. Walking Observations: Self-Selected Walking Speed and Walking Time
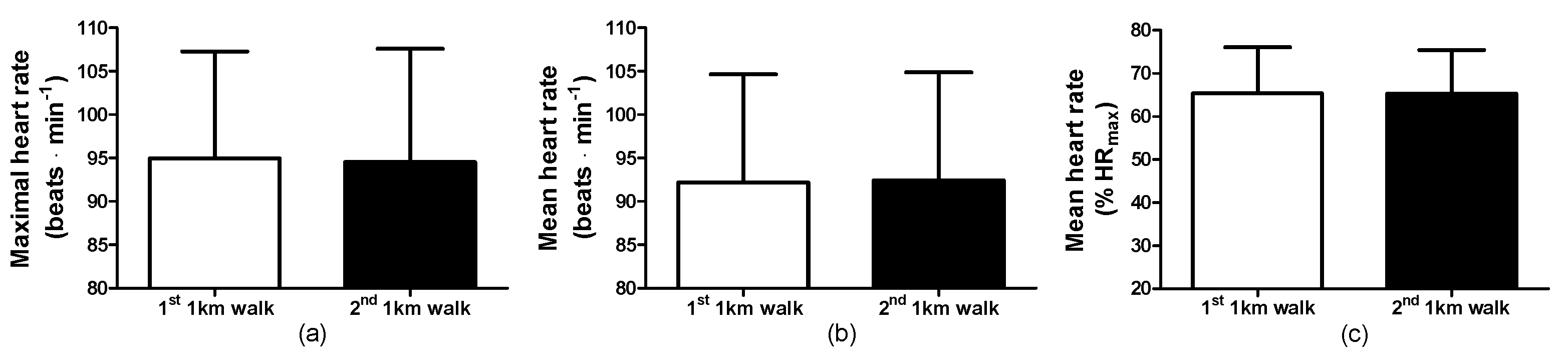
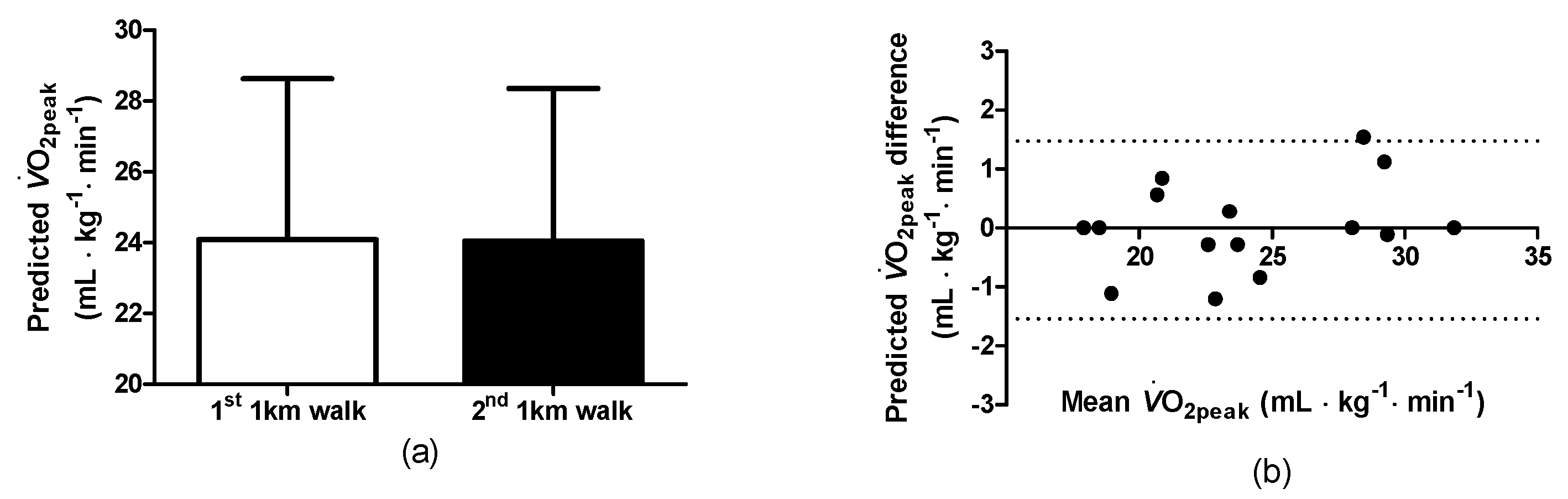
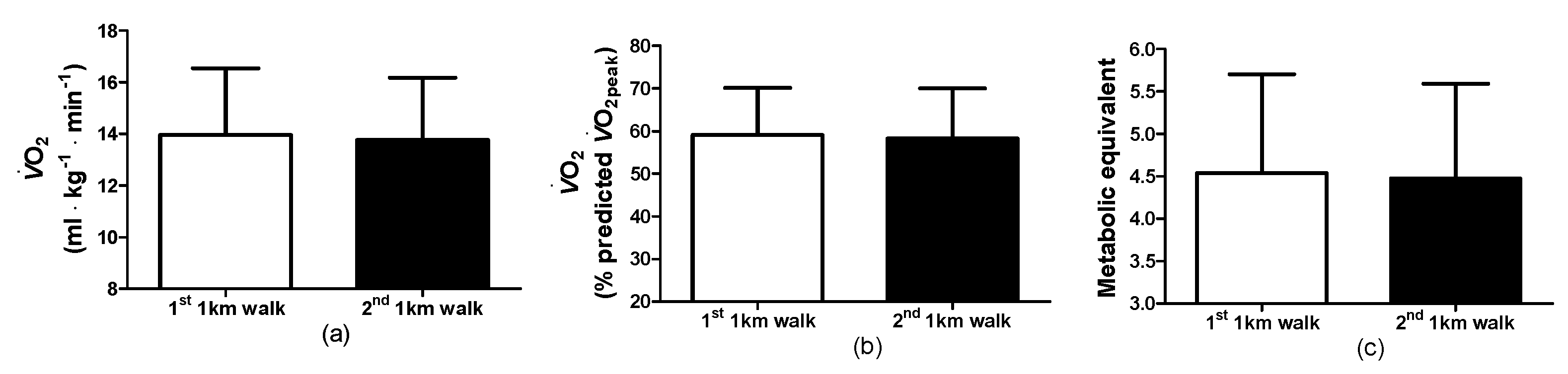
3.3. Walking Observations: Physiological and Cardiovascular Responses
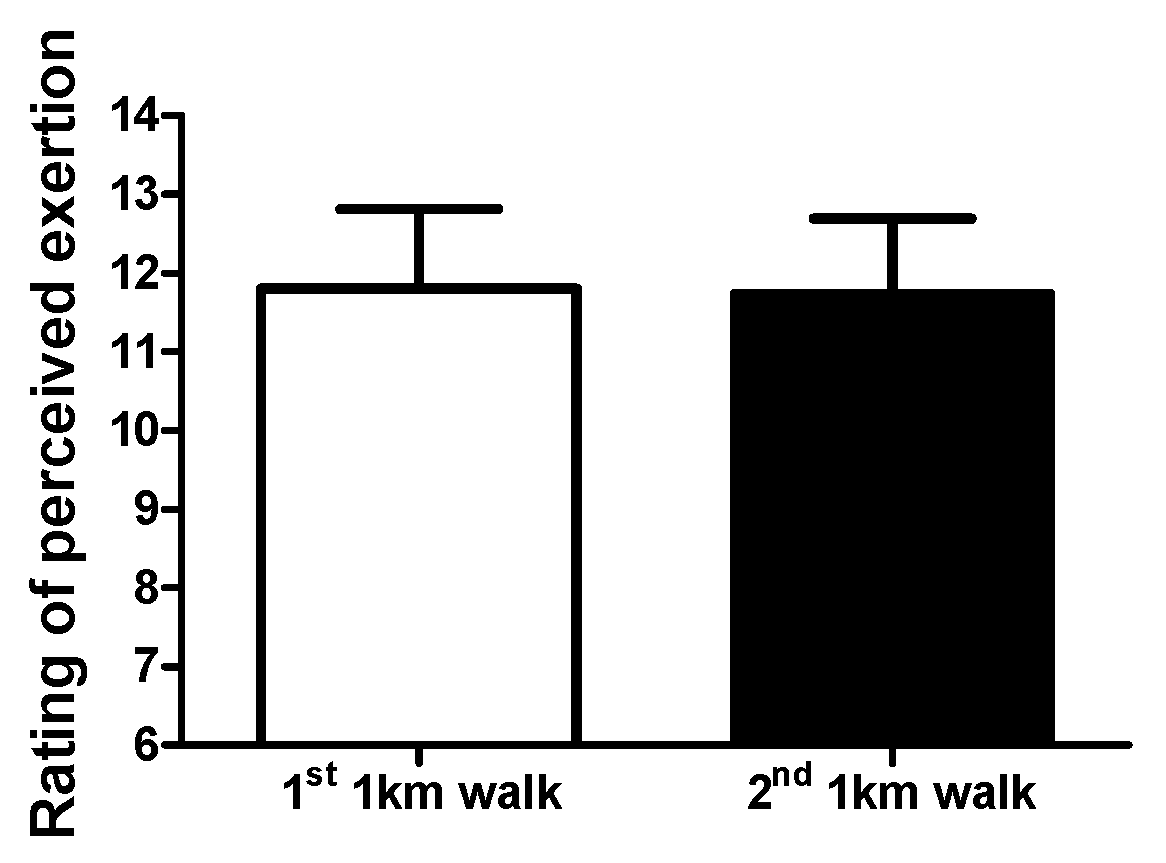
3.4. Walking Observations: Rating of Perceived Exertion
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jones, J.; Furze, G.; Buckley, J. Cardiovascular Disease Prevention and Rehabilitation. In Cardiovascular Prevention and Rehabilitation in Practice, 2nd ed.; Jones, J., Furze, G., Buckley, J., Sheppard, G., Eds.; John Wiley & Sons Ltd.: Hoboken, NJ, USA, 2020; pp. 1–19. [Google Scholar]
- National Audit of Cardiac Rehabilitation. Annual Statistical Report 2017. Available online: https://www.bhf.org.uk/ (accessed on 6 December 2016).
- Heran, B.S.; Chen, J.M.; Ebrahim, S.; Moxham, T.; Oldridge, N.; Rees, K.; Thompson, D.R.; Taylor, R.S. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst. Rev. 2011, 7, CD001800. [Google Scholar] [CrossRef]
- Dibben, G.; Faulkner, J.; Oldridge, N.; Rees, K.; Thompson, D.R.; Zwisler, A.; Taylor, R.S. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst. Rev. 2021, 11, CD001800. [Google Scholar] [CrossRef]
- Lim, C.; Dunford, E.C.; Valentino, S.E.; Oikawa, S.Y.; McGlory, C.; Baker, S.K.; Macdonald, M.J.; Phillips, S.M. Both Traditional and Stair Climbing-based HIIT Cardiac Rehabilitation Induce Beneficial Muscle Adaptations. Med. Sci. Sports Exerc. 2021, 53, 1114–1124. [Google Scholar] [CrossRef] [PubMed]
- Dunford, E.C.; Valentino, S.E.; Dubberley, J.; Oikawa, S.Y.; McGlory, C.; Lonn, E.; Jung, M.E.; Gibala, M.J.; Phillips, S.M.; MacDonald, M.J. Brief Vigorous Stair Climbing Effectively Improves Cardiorespiratory Fitness in Patients with Coronary Artery Disease: A Randomized Trial. Front. Sports Act. Living 2021, 3, 630912. [Google Scholar] [CrossRef] [PubMed]
- Ross, R.; Blair, S.N.; Arena, R.; Church, T.S.; Després, J.P.; Franklin, B.A.; Haskell, W.L.; Kaminsky, L.A.; Levine, B.D.; Lavie, C.J.; et al. Importance of Assessing Cardiorespiratory Fitness in Clinical Practice: A Case for Fitness as a Clinical Vital Sign: A Scientific Statement from the American Heart Association. Circulation 2016, 134, e653–e699. [Google Scholar] [CrossRef] [PubMed]
- Wenger, H.A.; Bell, G.J. The interactions of intensity, frequency and duration of exercise training in altering cardiorespiratory fitness. Sports Med. 1986, 3, 346–356. [Google Scholar] [CrossRef]
- Bruce, R.A.; Kusumi, F.; Hosmer, D. Maximal oxygen intake and nomographic assessment of functional aerobic impairment in cardiovascular disease. Am. Heart J. 1973, 85, 546–562. [Google Scholar] [CrossRef]
- Chiaranda, G.; Myers, J.; Mazzoni, G.; Terranova, F.; Bernardi, E.; Grossi, G.; Codecà, L.; Conconi, F.; Grazzi, G. Peak oxygen uptake prediction from a moderate, perceptually regulated, 1-km treadmill walk in male cardiac patients. J. Cardiopulm. Rehabil. Prev. 2012, 32, 262–269. [Google Scholar] [CrossRef]
- Weber, K.T.; Kinasewitz, G.T.; Janicki, J.S.; Fishman, A.P. Oxygen utilization and ventilation during exercise in patients with chronic cardiac failure. Circulation 1982, 65, 1213–1223. [Google Scholar] [CrossRef]
- Wass, E.; Taylor, N.F.; Matsas, A. Familiarisation to treadmill walking in unimpaired older people. Gait Posture 2005, 21, 72–79. [Google Scholar] [CrossRef]
- Franklin, B.A.; Eijsvogels, T.M.H.; Pandey, A.; Quindry, J.; Toth, P.P. Physical activity, cardiorespiratory fitness, and cardiovascular health: A clinical practice statement of the American Society for Preventive Cardiology Part II: Physical activity, cardiorespiratory fitness, minimum and goal intensities for exercise training, prescriptive methods, and special patient populations. Am. J. Prev. Cardiol. 2022, 12, 100425. [Google Scholar] [CrossRef]
- Franklin, B.A.; Eijsvogels, T.M.H.; Pandey, A.; Quindry, J.; Toth, P.P. Physical activity, cardiorespiratory fitness, and cardiovascular health: A clinical practice statement of the ASPC Part I: Bioenergetics, contemporary physical activity recommendations, benefits, risks, extreme exercise regimens, potential maladaptations. Am. J. Prev. Cardiol. 2022, 12, 100424. [Google Scholar] [CrossRef]
- Spelman, C.C.; Pate, R.R.; Macera, C.A.; Ward, D.S. Self-selected exercise intensity of habitual walkers. Med. Sci. Sports Exerc. 1993, 25, 1174–1179. [Google Scholar] [CrossRef] [PubMed]
- Pintar, J.A.; Robertson, R.J.; Kriska, A.M.; Nagle, E.; Goss, F.L. The influence of fitness and body weight on preferred exercise intensity. Med. Sci. Sports Exerc. 2006, 38, 981–988. [Google Scholar] [CrossRef]
- Dishman, R.K.; Farquhar, R.P.; Cureton, K.J. Responses to preferred intensities of exertion in men differing in activity levels. Med. Sci. Sports Exerc. 1994, 26, 783–790. [Google Scholar] [CrossRef] [PubMed]
- Kravitz, L.; Robergs, R.A.; Heyward, V.H.; Wagner, D.R.; Powers, K. Exercise mode and gender comparisons of energy expenditure at self-selected intensities. Med. Sci. Sports Exerc. 1997, 29, 1028–1035. [Google Scholar] [CrossRef] [PubMed]
- Kanegusuku, H.; Cucato, G.G.; Longano, P.; Okamoto, E.; Piemonte, M.E.P.; Correia, M.A.; Ritti-Dias, R.M. Acute Cardiovascular Responses to Self-selected Intensity Exercise in Parkinson’s Disease. Int. J. Sports Med. 2022, 43, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Barros, T.A.R.; do Prado, W.L.; Tenório, T.R.S.; Ritti-Dias, R.M.; Germano-Soares, A.H.; Balagopal, B.P.; Hill, J.O.; Freitas-Dias, R. Cardiovascular Effects of Aerobic Exercise with Self-Selected or Predetermined Intensity in Adolescents with Obesity. Pediatr. Exerc. Sci. 2021, 33, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Costa, I.B.B.; Schwade, D.; Macêdo, G.A.D.; Browne, R.A.V.; Farias-Junior, L.F.; Freire, Y.A.; Sócrates, J.; Boreskie, K.F.; Duhamel, T.A.; Caldas Costa, E. Acute antihypertensive effect of self-selected exercise intensity in older women with hypertension: A crossover trial. Clin. Interv. Aging 2019, 14, 1407–1418. [Google Scholar] [CrossRef] [PubMed]
- Bethell, H.J.N. Exercise-based cardiac rehabilitation. Medicine 2006, 34, 195–196. [Google Scholar] [CrossRef]
- Gordon, N.F.; Duncan, J.J. Effect of beta-blockers on exercise physiology: Implications for exercise training. Med. Sci. Sports Exerc. 1991, 23, 668–676. [Google Scholar] [CrossRef]
- Resnick, B.; Jenkins, L.S. Testing the reliability and validity of the Self-Efficacy for Exercise scale. Nurs. Res. 2000, 49, 154–159. [Google Scholar] [CrossRef]
- McInnis, K.J.; Balady, G.J. Comparison of submaximal exercise responses using the Bruce vs modified Bruce protocols. Med. Sci. Sports Exerc. 1994, 26, 103–107. [Google Scholar] [CrossRef]
- Byrne, N.M.; Hills, A.P.; Hunter, G.R.; Weinsier, R.L.; Schutz, Y. Metabolic equivalent: One size does not fit all. J. Appl. Physiol. 2005, 99, 1112–1119. [Google Scholar] [CrossRef]
- Gault, M.L.; Clements, R.E.; Willems, M.E.T. Functional mobility of older adults after concentric and eccentric endurance exercise. Eur. J. Appl. Physiol. 2012, 112, 3699–3707. [Google Scholar] [CrossRef]
- Rossignol, S.; Dubuc, R.; Gossard, J.P. Dynamic sensorimotor interactions in locomotion. Physiol. Rev. 2006, 86, 89–154. [Google Scholar] [CrossRef] [PubMed]
- Van de Putte, M.; Hagemeister, N.; St-Onge, N.; Parent, G.; de Guise, J.A. Habituation to treadmill walking. Biomed. Mater. Eng. 2006, 16, 43–52. [Google Scholar] [PubMed]
- Meyer, C.; Killeen, T.; Easthope, C.S.; Curt, A.; Bolliger, M.; Linnebank, M.; Zörner, B.; Filli, L. Familiarization with treadmill walking: How much is enough? Sci. Rep. 2019, 9, 5232. [Google Scholar] [CrossRef] [PubMed]
- Malatesta, D.; Canepa, M.; Menendez Fernandez, A. The effect of treadmill and overground walking on preferred walking speed and gait kinematics in healthy, physically active older adults. Eur. J. Appl. Physiol. 2017, 117, 1833–1843. [Google Scholar] [CrossRef] [PubMed]
- Faulkner, J.; Gerhard, J.; Stoner, L.; Lambrick, D. Self-Paced Walking within a Diverse Topographical Environment Elicits an Appropriate Training Stimulus for Cardiac Rehabilitation Patients. Rehabil. Res. Pract. 2012, 2012, 140871. [Google Scholar] [CrossRef] [PubMed]
- Grazzi, G.; Mazzoni, G.; Myers, J.; Codecà, L.; Pasanisi, G.; Mandini, S.; Piepoli, M.; Volpato, S.; Conconi, F.; Chiaranda, G. Determining the best percent-predicted equation for estimated VO2 peak by a 1-km moderate perceptually-regulated treadmill walk to predict mortality in outpatients with cardiovascular disease. J. Sci. Med. Sport. 2018, 21, 307–311. [Google Scholar] [CrossRef]
- Chiaranda, G.; Myers, J.; Arena, R.; Kaminsky, L.; Sassone, B.; Pasanisi, G.; Mandini, S.; Mazzoni, G.; Grazzi, G. Prognostic comparison of the FRIEND and Wasserman/Hansen peak VO2 equations applied to a submaximal walking test in outpatients with cardiovascular disease. Eur. J. Prev. Cardiol. 2021, 28, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Raisi, A.; Bernardi, E.; Myers, J.; Piva, T.; Zerbini, V.; Massotti, S.; Menegatti, E.; Caruso, L.; Mazzoni, G.; Grazzi, G.; et al. Change in Peak Oxygen Uptake Predicted by the Moderate 1-km Treadmill Walking Test After Walking Training in Outpatients with Cardiovascular Disease. J. Cardiopulm. Rehabil. Prev. 2023, in press. [Google Scholar] [CrossRef] [PubMed]
- Raisi, A.; Piva, T.; Myers, J.; Lordi, R.; Zerbini, V.; Massotti, S.; Chiaranda, G.; Grazzi, G.; Mazzoni, G.; Mandini, S. A Moderate Walking Test Predicts Survival in Women with Cardiovascular Diseases. Am. J. Prev. Med. 2023, 65, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Zerbini, V.; Raisi, A.; Myers, J.; Piva, T.; Lordi, R.; Chiaranda, G.; Mazzoni, G.; Grazzi, G.; Mandini, S. Peak Oxygen Uptake Estimation From A Moderate 1-KM Treadmill Walk in Women with Cardiovascular Disease. J. Cardiopulm. Rehabil. Prev. 2021, 41, 432–434. [Google Scholar] [CrossRef] [PubMed]
- Savage, P.D.; Toth, M.J.; Ades, P.A. A re-examination of the metabolic equivalent concept in individuals with coronary heart disease. J. Cardiopulm. Rehabil. Prev. 2007, 27, 143–148. [Google Scholar] [CrossRef]
- Williams, P.T.; Thompson, P.D. Increased cardiovascular disease mortality associated with excessive exercise in heart attack survivors. Mayo Clin. Proc. 2014, 89, 1187–1194. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cardiac Condition/Intervention | n |
|---|---|
| Myocardial infarction and percutaneous intervention | 6 |
| Angina and percutaneous intervention | 1 |
| Valve replacement surgery | 3 |
| Myocardial infarction and coronary artery bypass graph surgery | 3 |
| Pacemaker | 1 |
| Heart failure (class I/II) | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gault, M.L.; Willems, M.E.T. Full Familiarisation Is Not Required for the Self-Paced 1 km Treadmill Walk to Predict Peak Oxygen Uptake in Phase IV Cardiac Patients. Clin. Pract. 2024, 14, 327-336. https://doi.org/10.3390/clinpract14010025
Gault ML, Willems MET. Full Familiarisation Is Not Required for the Self-Paced 1 km Treadmill Walk to Predict Peak Oxygen Uptake in Phase IV Cardiac Patients. Clinics and Practice. 2024; 14(1):327-336. https://doi.org/10.3390/clinpract14010025
Chicago/Turabian StyleGault, Mandy L., and Mark E. T. Willems. 2024. "Full Familiarisation Is Not Required for the Self-Paced 1 km Treadmill Walk to Predict Peak Oxygen Uptake in Phase IV Cardiac Patients" Clinics and Practice 14, no. 1: 327-336. https://doi.org/10.3390/clinpract14010025
APA StyleGault, M. L., & Willems, M. E. T. (2024). Full Familiarisation Is Not Required for the Self-Paced 1 km Treadmill Walk to Predict Peak Oxygen Uptake in Phase IV Cardiac Patients. Clinics and Practice, 14(1), 327-336. https://doi.org/10.3390/clinpract14010025