
An Increase in Aspartate Aminotransferase Can Predict Worsening Disease Severity in Japanese Patients with COVID-19

 , ,
, ,
Abstract
1. Introduction
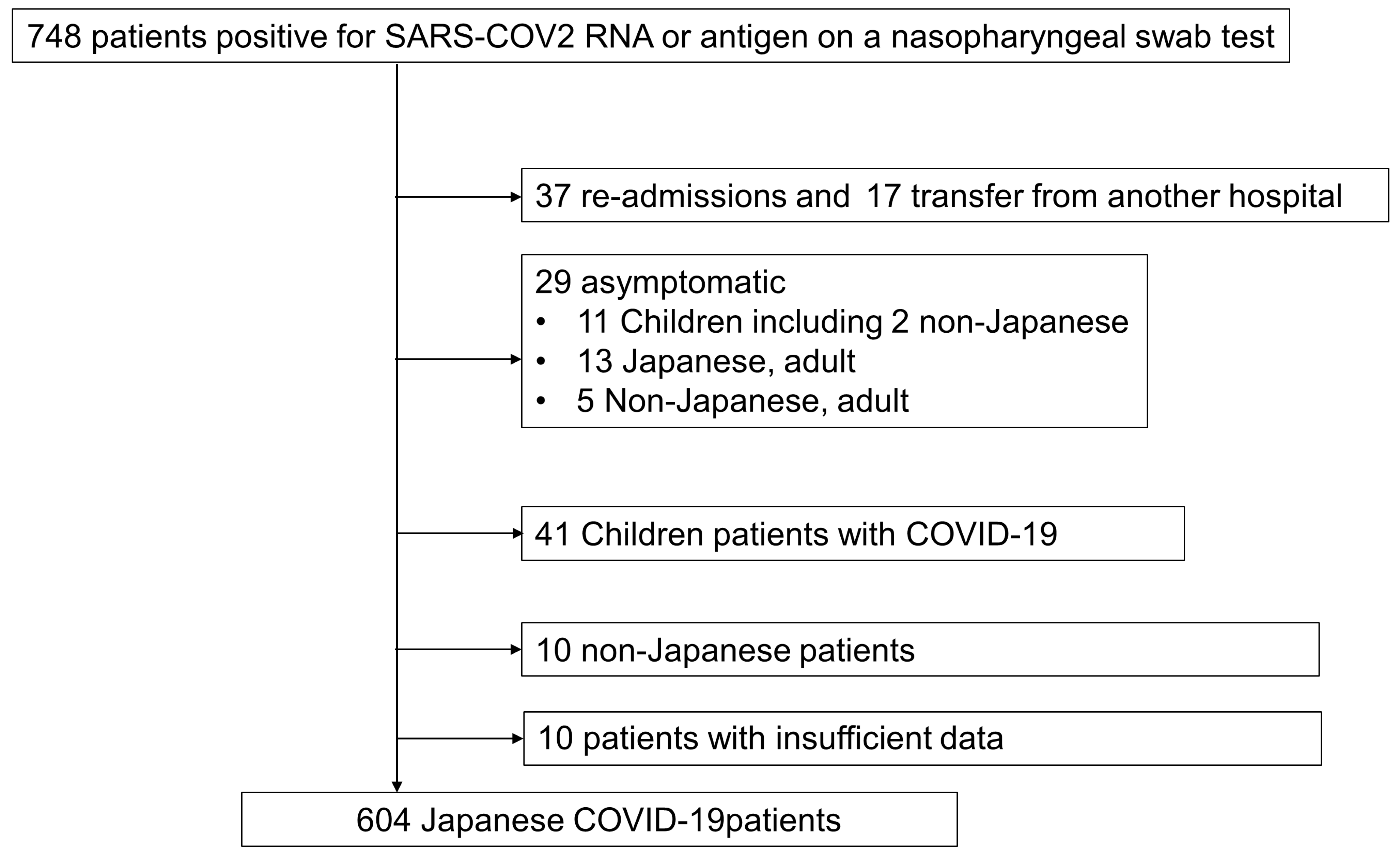
2. Patients and Methods
Statistical Analysis
3. Results
3.1. Liver Function Tests at Admission Can Be Used to Predict Worsening Disease Severity in Japanese Patients with COVID-19
3.2. Univariate Logistic Analysis and Univariate Cox Proportional Hazards Analysis of Risk Factors for Progression to Severe COVID-19
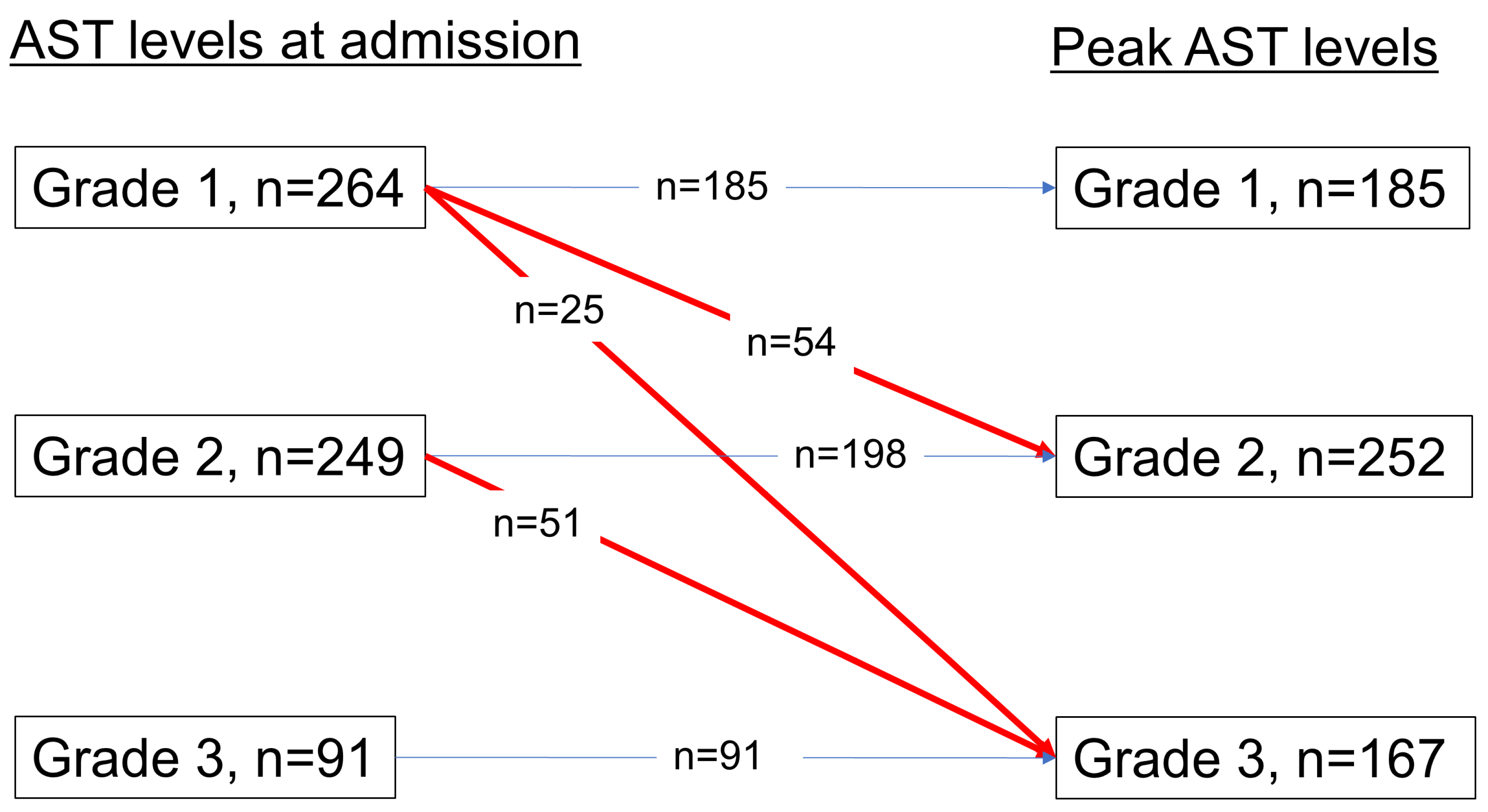
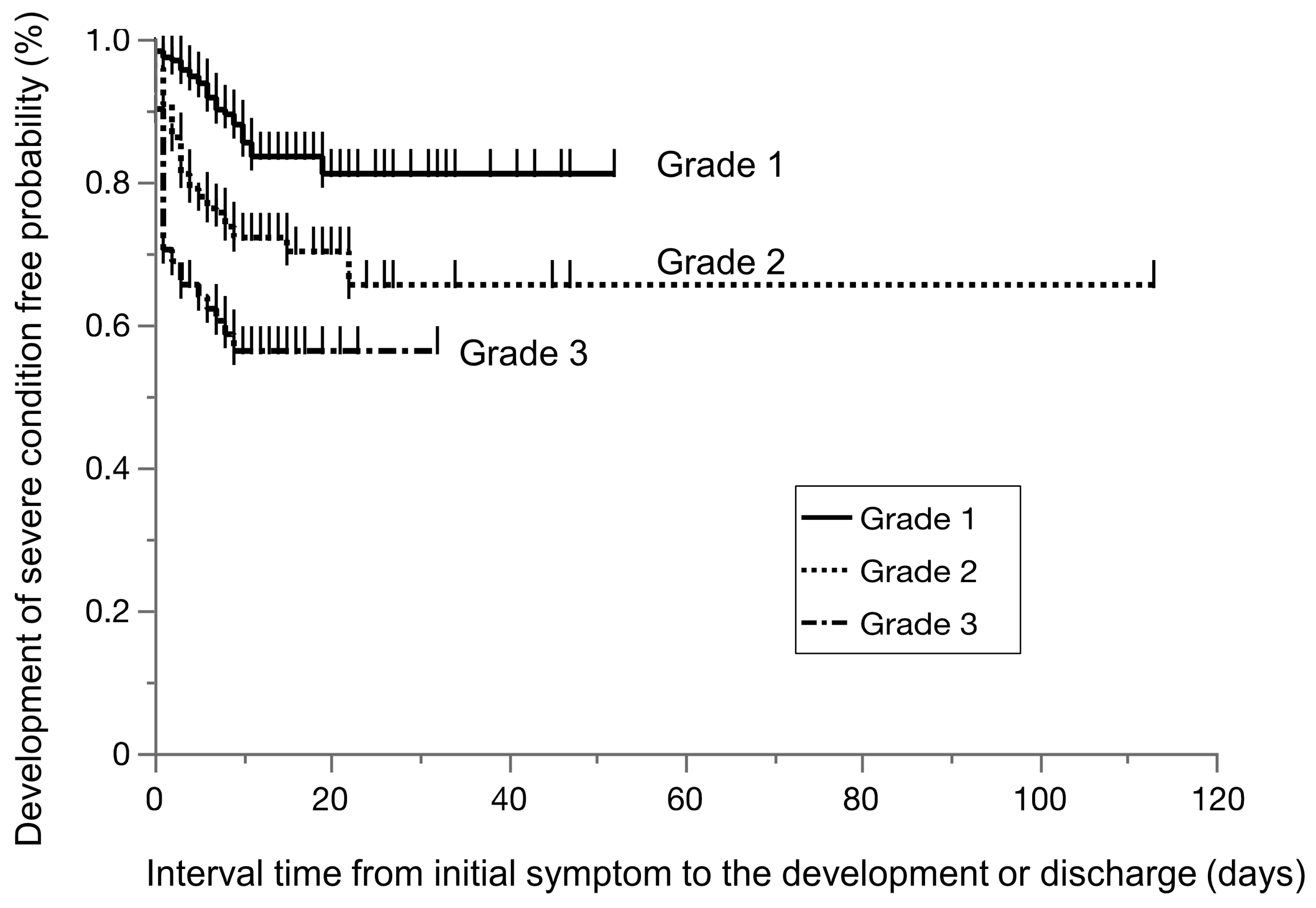
3.3. Clinical Course of COVID-19 Patients Based on AST Grade
3.4. Patients with Underlying Liver Disease
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Japanese Ministry of Health Labour and Welfare. The Guidance on the Medical Treatment of COVID-19 (In Japanese) (ver 8.0). Available online: https://www.mhlw.go.jp/content/000936655.pdf (accessed on 23 June 2022).
- Fu, Y.; Zhu, R.; Bai, T.; Han, P.; He, Q.; Jing, M.; Xiong, X.; Zhao, X.; Quan, R.; Chen, C.; et al. Clinical Features of Patients Infected with Coronavirus Disease 2019 With Elevated Liver Biochemistries: A Multicenter, Retrospective Study. Hepatology 2021, 73, 1509–1520. (In English) [Google Scholar] [CrossRef]
- Bertolini, A.; Van De Peppel, I.P.; Bodewes, F.A.; Moshage, H.; Fantin, A.; Farinati, F.; Fiorotto, R.; Jonker, J.W.; Strazzabosco, M.; Verkade, H.J.; et al. Abnormal Liver Function Tests in Patients with COVID-19: Relevance and Potential Pathogenesis. Hepatology 2020, 72, 1864–1872. [Google Scholar] [CrossRef]
- Higuchi, T.; Nishida, T.; Iwahashi, H.; Morimura, O.; Otani, Y.; Okauchi, Y.; Yokoe, M.; Suzuki, N.; Inada, M.; Abe, K. Early clinical factors predicting the development of critical disease in Japanese patients with COVID-19: A single-center, retrospective, observational study. J. Med. Virol. 2021, 93, 2141–2148. (In English) [Google Scholar] [CrossRef] [PubMed]
- Okauchi, Y.; Matsuno, K.; Nishida, T.; Sawada, K.; Kawasaki, A.; Ito, N.; Morimura, O.; Otani, Y.; Yokoe, M.; Abe, K.; et al. Obesity, glucose intolerance, advanced age, and lymphocytopenia are independent risk factors for oxygen requirement in Japanese patients with Coronavirus disease 2019 (COVID-19). Endocr. J. 2021, 68, 849–856. (In English) [Google Scholar] [CrossRef] [PubMed]
- Nishida, T.; Iwahashi, H.; Yamauchi, K.; Noriko, K.; Yukiyoshi, O.; Norihiro, S.; Masami, I.; Kinya, A. Seroprevalence of SARS-CoV-2 antibodies among 925 staff members in an urban hospital accepting COVID-19 patients in Osaka prefecture, Japan: A cross-sectional study. Medicine 2021, 100, e26433. (In English) [Google Scholar] [CrossRef] [PubMed]
- Tamai, M.; Maekawa, A.; Goto, N.; Ge, L.; Nishida, T.; Iwahashi, H.; Yokomi, A. Three cases of COVID-19 patients presenting with erythema. J. Dermatol. 2020, 47, 1175–1178. [Google Scholar] [CrossRef] [PubMed]
- Nishida, T.; Suzuki, N.; Ono, Y.; Shimizu, J.; Nakamatsu, D.; Matsumoto, K.; Yamamoto, M. How to make an alternative plastic gown during the personal protective equipment shortage due to the COVID-19 pandemic. Endoscopy 2020, 52, E388–E389. [Google Scholar] [CrossRef]
- World Health Oraganization. Clinical Management of COVID-19: Living Guideline. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2022-1 (accessed on 23 June 2022).
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef] [PubMed]
- Kermali, M.; Khalsa, R.K.; Pillai, K.; Ismail, Z.; Harky, A. The role of biomarkers in diagnosis of COVID-19—A systematic review. Life Sci. 2020, 254, 117788. [Google Scholar] [CrossRef]
- Li, Y.; Regan, J.; Fajnzylber, J.; Coxen, K.; Corry, H.; Wong, C.; Rosenthal, A.; Atyeo, C.; Fischinger, S.; Gillespie, E.; et al. Liver Fibrosis Index FIB-4 Is Associated with Mortality in COVID-19. Hepatol. Commun. 2021, 5, 434–445. [Google Scholar] [CrossRef]
- Yoneda, M.; Fujii, H.; Sumida, Y.; Hyogo, H.; Itoh, Y.; Ono, M.; Eguchi, Y.; Suzuki, Y.; Aoki, N.; Kanemasa, K.; et al. Platelet count for predicting fibrosis in nonalcoholic fatty liver disease. J. Gastroenterol. 2011, 46, 1300–1306. [Google Scholar] [CrossRef]
- Lippi, G.; Plebani, M.; Henry, B.M. Thrombocytopenia is associated with severe coronavirus disease 2019 (COVID-19) infections: A meta-analysis. Clin. Chim. Acta 2020, 506, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Zaki, N.; Alashwal, H.; Ibrahim, S. Association of hypertension, diabetes, stroke, cancer, kidney disease, and high-cholesterol with COVID-19 disease severity and fatality: A systematic review. Diabetes Metab. Syndr. 2020, 14, 1133–1142. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.; Long, F.; Yang, Y.; Chen, X.; Xu, L.; Yang, M. Serum ferritin as an independent risk factor for severity in COVID-19 patients. J. Infect. 2020, 81, 647–679. [Google Scholar] [CrossRef] [PubMed]
- Chai, X.; Hu, L.; Zhang, Y.; Han, W.; Lu, Z.; Ke, A.; Zhou, J.; Shi, G.; Fang, N.; Fan, J.; et al. Specific ACE2 Expression in Cholangiocytes May Cause Liver Damage After 2019-nCoV Infection. bioRxiv 2020, preprint. [Google Scholar] [CrossRef]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. (In English) [Google Scholar]
- Xu, L.; Liu, J.; Lu, M.; Yang, D.; Zheng, X. Liver injury during highly pathogenic human coronavirus infections. Liver Int. 2020, 40, 998–1004. [Google Scholar] [CrossRef]
- Kral, A.H.; Lambdin, B.H.; Wenger, L.D.; Davidson, P.J. Evaluation of an Unsanctioned Safe Consumption Site in the United States. N. Engl. J. Med. 2020, 383, 589–590. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of Covid-19—Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef]
- Matsuyama, S.; Kawase, M.; Nao, N.; Shirato, K.; Ujike, M.; Kamitani, W.; Shimojima, M.; Fukushi, S. The Inhaled Steroid Ciclesonide Blocks SARS-CoV-2 RNA Replication by Targeting the Viral Replication-Transcription Complex in Cultured Cells. J. Virol. 2020, 95, e01648-20. [Google Scholar] [CrossRef]
- Recovery Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [PubMed]
- Thachil, J.; Tang, N.; Gando, S.; Falanga, A.; Cattaneo, M.; Levi, M.; Clark, C.; Iba, T. ISTH interim guidance on recognition and management of coagulopathy in COVID-19. J. Thromb. Haemost. 2020, 18, 1023–1026. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Cao, R.; Zhang, L.; Yang, X.; Liu, J.; Xu, M.; Shi, Z.; Hu, Z.; Zhong, W.; Xiao, G. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020, 30, 269–271. [Google Scholar] [CrossRef] [PubMed]
- Sodeifian, F.; Seyedalhosseini, Z.S.; Kian, N.; Eftekhari, M.; Najari, S.; Mirsaeidi, M.; Farsi, Y.; Nasiri, M.J. Drug-Induced Liver Injury in COVID-19 Patients: A Systematic Review. Front. Med. 2021, 8, 731436. [Google Scholar] [CrossRef]
- Golomb, B.A.; Han, J.H.; Langsjoen, P.H.; Dinkeloo, E.; Zemljic-Harpf, A.E. Statin Use in Relation to COVID-19 and Other Respiratory Infections: Muscle and Other Considerations. J. Clin. Med. 2023, 12, 4659. [Google Scholar] [CrossRef]
- REMAP-CAP Investigators; Hills, T.E.; Lorenzi, E.; Berry, L.R.; Shyamsundar, M.; Al-Beidh, F.; Annane, D.; Arabi, Y.; Aryal, D.; Au, C.; et al. Simvastatin in Critically Ill Patients with COVID-19. N. Engl. J. Med. 2023, 389, 2341–2354. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patients with COVID-19, n = 604 |
|---|---|
| Age, median (IQR) | 62 (47, 78) |
| Sex, male n (%) | 335 (55.5) |
| Body mass index, median (IQR) | 23.9 (21.0, 26.9) |
| Smoking history (none/past/current) | 393/33/178 |
| Drinking history, yes n (%) | 211 (34.9) |
| Days from the onset of symptoms to admission, median (IQR) | 6 (4, 9) |
| Laboratory data on admission | |
| WBC, median (IQR) count/μL | 5100 (4050, 6800) |
| Lymphocyte, median (IQR) (count/μL) | 920 (672, 1240) |
| Neutrophilia, median (IQR) (count/μL) | 3699 (2663, 5252) |
| Hemoglobin, median (IQR) (g/dL) | 13.7 (12.3, 14.8) |
| Platelet count, median (IQR) (109/L) | 18.4 (14.7, 23.0) |
| AST, median (IQR) (IU/L) | 32 (23, 49) |
| ALT, median (IQR) (IU/L) | 24 (15, 40) |
| ALP, median (IQR) (IU/L) ※1 | 168 (74, 216) |
| γGTP, median (IQR) (IU/L) ※2 | 35 (18, 69) |
| T-bil, median (IQR) (mg/dL) | 0.55 (0.4, 0.71) |
| FIB-4 index, median (IQR) | 2.19 (1.32, 3.60) |
| Cr, median (IQR) (mg/dL) | 0.81 (0.63, 1.10) |
| BUN, median (IQR) (mg/dL) | 14 (11, 20) |
| LDH, median (IQR) (IU/L) | 262 (201, 356) |
| CRP, median (IQR) (mg/dL) | 3.6 (0.78, 7.9) |
| eGFR (mL/min/1.73m2), median (IQR) | 69.1 (50.7, 87.7) |
| HbA1c, median, median (IQR) (%) | 6 (5.7, 6.6) |
| Casual blood glucose, median (IQR) (mg/dL) | 115 (100, 140) |
| T-Chol, median (IQR) (mg/dL) | 164 (142, 189) |
| Comorbidities | |
| Hypertension, n (%) | 270 (44.1) |
| Cardiovascular diseases, n (%) | 103 (17.2) |
| Chronic obstructive pulmonary disease, n (%) | 32 (5.4) |
| Asthma, n (%) | 49 (8.2) |
| Diabetes mellitus, n (%) | 168 (27.9) |
| Hyperlipidemia, n (%) | 133 (23.3) |
| Chronic kidney disease, n (%) | 71 (11.9) |
| Hemodialysis, n (%) | 36 (6.1) |
| Solid cancer, n (%) ※3 | 48 (8.0) |
| Pregnancy, n (%) | 23 (3.8) |
| Concomitant liver disease | |
| HBs Ag positive, n (%) | 3 (0.53) |
| HCV Ab positive n (%) | 18 (3.2) |
| AIH or PBC, n (%) | 0 (0) |
| Use of medication for comorbidities | |
| ACEi/ARB, n (%) | 148 (24.5) |
| Calcium blocker, n (%) | 190 (31.6) |
| Statin, n (%) | 110 (18.3) |
| PPI, n (%) | 133 (22.2) |
| Initial Presentation | |
|---|---|
| Fever, n (%) | 559 (92.7) |
| Fatigue, n (%) | 206 (48) |
| Respiratory-related symptoms, n (%) | 468 (77.3) |
| Pneumonia, n (%) | 456 (75.6) |
| Headache, n (%) | 55 (12.3) |
| New loss of taste or smell, n (%) | 117 (23.2) |
| Days from onset of symptoms to admission, median (IQR) | 5 (3, 8) |
| Severity of COVID-19 on admission | |
| Mild to moderate symptoms, n (%) | 579 (95.9) |
| Severe symptoms, n (%) | 25 (4.1) |
| Progression to severe disease, n (%) | 141 (23.3) |
| Treatment | |
| Required oxygen, n (%) | 375 (62.1) |
| Medication for COVID-19 | |
| Ciclesonide, n (%) | 156 (31.2) |
| Hydroxychloroquine, n (%) | 16 (2.6) |
| Favipiravir, n (%) | 291 (48.1) |
| Heparin, n (%) | 52 (8.6) |
| Remdesivir, n (%) | 35 (5.8) |
| Dexamethasone, n (%) | 305 (50.5) |
| Clinical course | |
| Peak AST, median (IQR) (IU/L) | 41 (27, 64) |
| Peak ALT, median (IQR) (IU/L) | 39 (21, 73) |
| Length of hospital stay, median (IQR) (days) | 10 (7, 15) |
| Time from admission to aggravation (IQR) (days) | 2 (1, 5) |
| Required mechanical ventilatory support, n (%) | 125 (24.3) |
| Mortality, n (%) | 43 (7.1) |
| Univariate Logistic Analysis | Multivariate Logistic Analysis | |||||
|---|---|---|---|---|---|---|
| Variables | Odds Ratio | 95% CI | p Value | Odds Ratio | 95% CI | p Value |
| Aged 65 years and over, yes | 2.1 | 1.43–3.09 | 0.0002 | 1.32 | 0.78–2.23 | 0.29 |
| BMI 30 and over, yes | 1.51 | 0.87–2.62 | 0.14 | 1.39 | 0.72–1.88 | 0.32 |
| Smoking history, yes | 1.33 | 0.88–2.03 | 0.17 | 1.05 | 0.64–1.71 | 0.84 |
| Hypertension, yes | 2.94 | 1.99–4.37 | <0.0001 | 2.24 | 1.32–3.78 | 0.0026 |
| Diabetes mellitus, yes | 1.84 | 1.23–2.75 | 0.003 | 1.25 | 0.76–2.07 | 0.38 |
| Hyperlipidemia, yes | 1.73 | 1.12–2.67 | 0.01 | 1.12 | 0.66–1.88 | 0.67 |
| Chronic kidney disease (eGFR < 70), yes | 2.38 | 1.60–3.54 | <0.0001 | 1.52 | 0.92–2.50 | 0.10 |
| Chronic lung disease, yes | 1.55 | 0.71–3.36 | 0.27 | 1.28 | 0.51–3.21 | 0.60 |
| Solid cancer, yes | 1.00 | 0.50–2.02 | 0.99 | 0.97 | 0.42–2.20 | 0.93 |
| Pregnancy, yes | 3.30 | 0.76–14.3 | 0.11 | 2.01 | 0.41–9.91 | 0.39 |
| Lymphocyte count < 1000, yes | 3.03 | 1.98–4.67 | <0.0001 | 2.72 | 1.63–4.56 | <0.0001 |
| LDH ≥ 300, yes | 3.42 | 2.31–5.06 | <0.0001 | 1.87 | 1.10–3.16 | 0.020 |
| CRP ≥ 3, yes | 3.29 | 2.15–5.02 | <0.0001 | 1.96 | 1.13–3.40 | 0.016 |
| Elevated AST | ||||||
| Grade 1, AST < 30 IUL | 1 | |||||
| Grade 2, 30 < AST < 60 | 2.36 | 1.50–3.71 | 0.0002 | 1.83 | 1.04–3.24 | 0.038 |
| Grade 3, AST > 60 | 5.13 | 2.96–8.86 | <0.0001 | 3.35 | 1.64–6.81 | 0.0009 |
| Elevated ALT | ||||||
| Grade 1, ALT < 30 IU/L | 1 | |||||
| Grade 2, 30 < ALT < 60 | 1.65 | 1.08–2.52 | 0.02 | |||
| Grade 3, ALT > 60 | 1.07–3.27 | 0.02 | ||||
| Characteristics | Grade 1 Normal AST n = 264 | Grade 2 30 ≤ AST < 60 n = 249 | Grade 3 ALT > 60 n = 91 | p Value |
|---|---|---|---|---|
| Age, median (IQR) | 60 (37, 80) | 63 (50, 78) | 64 (53, 73) | 0.1200 |
| Men Sex, n (%) | 110 (41.7) | 156 (62.65) | 69 (75.8) | <0.0001 |
| Body mass index > 30, n (%) | 21 (8.6) | 37 (15.7) | 14 (15.9) | 0.0400 |
| Smoking history, yes, n (%) | 77 (29.2) | 91 (36.6) | 43 (47.3) | <0.0001 |
| Severity of COVID-19 | ||||
| Mild to moderate symptom, n (%) | 259 (98.1%) | 236 (94.8%) | 84 (92.3%) | 0.03 |
| Severe symptom, n (%) | 5 (1.9%) | 13 (5.2%) | 7 (7.69%) | 0.03 |
| Progression to severe disease, n (%) | 35 (13.3) | 66 (26.5) | 40 (44.0) | <0.0001 |
| Diabetes mellitus, n (%) | 58 (22.1) | 82 (32.9) | 28 (30.8) | 0.0200 |
| Hyperlipidemia, n (%) | 34 (13.4) | 72 (30.8) | 27 (32.9) | <0.0001 |
| Chronic kidney disease, n (%) | 44 (16.7) | 21 (8.6) | 6 (6.6) | 0.005 |
| Hemodialysis, n (%) | 28 (10.9) | 7 (2.85) | 1 (1.16) | 0.0001 |
| Solid cancer, n (%) | 17 (6.5) | 24 (9.8) | 7 (7.7) | 0.38 |
| Pregnancy, n (%) | 20 (7.6) | 3 (1.2) | 0 (0.0) | <0.0001 |
| Concomitant liver disease | ||||
| HBs Ag positive, n (%) | 2 (0.8) | 1 (0.44) | 0 (0) | 0.76 |
| HCV Ab positive n (%) | 11 (4.4) | 4 (1.8) | 3 (3.8) | 0.45 |
| AIH or PBC, n (%) | 0 | 0 | 0 | |
| Use of medication for comorbidities | ||||
| ACEi/ARB, n (%) | 53 (20.1) | 71 (28.5) | 24 (26.4) | 0.07 |
| Calcium blocker, n (%) | 74 (28.0) | 89 (36.2) | 27 (29.7) | 0.13 |
| Statin, n (%) | 35 (13.3) | 58 (23.6) | 17 (18.9) | 0.02 |
| PPI, n (%) | 55 (20.8) | 59 (24.0) | 19 (20.9) | 0.66 |
| Laboratory data | ||||
| Lymphocytes, median (IQR) (count/μL) | 1011 (724, 1336) | 890 (637, 1113) | 856 (616, 1145) | 0.0001 |
| LDH, median (IQR) (IU/L) | 205 (172, 253) | 298 (239, 368) | 422 (342, 553) | <0.0001 |
| CRP, median (IQR) (mg/dL) | 1.41 (0.37, 4.84) | 4.62 (1.96, 9.25) | 6.69 (3.94, 12.64) | <0.0001 |
| eGFR (mL/min/1.73 m2), median (IQR) | 71.6 (48.8, 90.7) | 65.6 (50.7, 81.3) | 70 (52.8, 85.7) | 0.0900 |
| HbA1c, median, (IQR) (%) | 5.8 (5.5, 6.3) | 6.2 (5.8, 6.7) | 6.3 (5.9, 6,9) | <0.0001 |
| Platelets, median (IQR) (109/L) | 19 (15.1, 23.7) | 17.9 (14.5, 22) | 18.3 (14.7, 22.8) | 0.24 |
| Characteristic | Patients with Liver Disease, n = 20 |
|---|---|
| HBs Ag positive, n | 3 |
| HCV infection (Current/preexisting), n | 9/9 |
| Age, median (IQR) | 70 (48.5, 78) |
| Sex, male n (%) | 13 (65) |
| Laboratory data on admission | |
| AST, median (IQR) (IU/L) | 29 (23, 39) |
| AST levels on admission n (Grade 1/Grade 2/Grade 3) | 13/4/3 |
| ALT, median (IQR) (IU/L) | 18 (14, 32) |
| Platelet count, median (IQR) (109/L) | 13.55 (11.83, 17.33) |
| Fib-4 index, median (IQR) | 2.81 (1.71, 4.38) |
| Clinical course | |
| Peak AST, median (IQR) (IU/L) | 40 (26, 97) |
| Peak AST levels n (Grade 1/Grade 2/Grade 3) | 8/6/6 |
| Peak ALT, median (IQR) (IU/L) | 39 (20, 71) |
| Progression to severe disease, n (%) | 6 (30) |
| Time from admission to severe disease (IQR) (days) | 3 (0, 3.5) |
| Mortality, n (%) | 3 (15%) |
| Characteristics | Within the Period from the First to Third Wave n = 371 | Within the Period from the Fourth to Fifth Wave n = 233 | p Value |
|---|---|---|---|
| Age, median (IQR) | 57 (43,71) | 69 (49, 81) | <0.0001 |
| Male sex, n (%) | 200 (59.7%) | 135 (57.9) | 0.33 |
| Body mass index, median (IQR) | 24.3 (21.1, 27.2) | 23.5 (20.8, 26.7) | 0.17 |
| Days from onset of symptoms to admission, median (IQR) | 7 (4, 9) | 6 (4, 10) | 0.86 |
| Severity of COVID-19 on admission | |||
| Mild to moderate symptoms, n (%) | 359 (96.8) | 220 (94.4) | 0.16 |
| Severe symptoms, n (%) | 12 (3.2) | 13 (5.6) | 0.16 |
| Progression to severe disease, n (%) | 74 (20.0) | 67 (28.8) | 0.013 |
| Medications | |||
| hydroxychloroquine, n (%) | 16 (4.3) | 0 (0) | 0.0001 |
| favipiravir, n (%) | 185 (49.9 | 106 (45.5) | 0.83 |
| ciclesonide, n (%) | 154 (41.5) | 2 (0.86) | <0.0001 |
| heparin, n (%) | 7 (1.9) | 45 (19.3) | <0.0001 |
| dexamethasone, n (%) | 153 (41.2) | 152 (65.2) | <0.0001 |
| remdesivir, n (%) | 0 (0) | 35 (15.0) | <0.0001 |
| AST levels at admission, n (%) | |||
| Grade 1, AST < 30 U/L | 181 (48.8) | 83 (35.6) | 0.0014 |
| Grade 2, 30 < AST < 60 | 148 (39.9) | 101 (43.4) | 0.4 |
| Grade 3, 60 < AST | 42 (11.3) | 49 (21.0) | 0.0013 |
| Peak AST levels | |||
| Grade 1, AST < 30 U./L | 128 (34.5) | 5 7 (24.5) | 0.009 |
| Grade 2, 30 < AST < 60 | 158 (42.6) | 94 (40.3) | 0.58 |
| Grade 3, 60 < AST | 85 (22.9) | 82 (35.2) | 0.0011 |
| Increased AST grade, n (%) | 81 (21.8) | 49 (21.0) | 0.81 |
| Univariate Logistic Analysis | |||
|---|---|---|---|
| Drugs | Odds Ratio | 95% CI | p Value |
| hydroxychloroquine, yes | 1.19 | 0.34–4.25 | 0.78 |
| favipiravir, yes | 2.92 | 1.93–4.41 | <0.0001 |
| ciclesonide, yes | 1.73 | 1.14–2.63 | 0.01 |
| heparin, yes | 1.24 | 0.64–2.40 | 0.52 |
| dexamethasone, yes | 2.18 | 1.46–3.27 | 0.0002 |
| remdesivir, yes | 1.50 | 0.69–3.20 | 0.30 |
| Progression to severe symptoms, yes | 1.81 | 1.17–2.78 | 0.0068 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsumoto, K.; Nishida, T.; Nakamatsu, D.; Yamamoto, M.; Fukui, K.; Morimura, O.; Abe, K.; Okauchi, Y.; Iwahashi, H.; Inada, M. An Increase in Aspartate Aminotransferase Can Predict Worsening Disease Severity in Japanese Patients with COVID-19. Clin. Pract. 2024, 14, 1601-1614. https://doi.org/10.3390/clinpract14040129
Matsumoto K, Nishida T, Nakamatsu D, Yamamoto M, Fukui K, Morimura O, Abe K, Okauchi Y, Iwahashi H, Inada M. An Increase in Aspartate Aminotransferase Can Predict Worsening Disease Severity in Japanese Patients with COVID-19. Clinics and Practice. 2024; 14(4):1601-1614. https://doi.org/10.3390/clinpract14040129
Chicago/Turabian StyleMatsumoto, Kengo, Tsutomu Nishida, Dai Nakamatsu, Masashi Yamamoto, Koji Fukui, Osamu Morimura, Kinya Abe, Yukiyoshi Okauchi, Hiromi Iwahashi, and Masami Inada. 2024. "An Increase in Aspartate Aminotransferase Can Predict Worsening Disease Severity in Japanese Patients with COVID-19" Clinics and Practice 14, no. 4: 1601-1614. https://doi.org/10.3390/clinpract14040129
APA StyleMatsumoto, K., Nishida, T., Nakamatsu, D., Yamamoto, M., Fukui, K., Morimura, O., Abe, K., Okauchi, Y., Iwahashi, H., & Inada, M. (2024). An Increase in Aspartate Aminotransferase Can Predict Worsening Disease Severity in Japanese Patients with COVID-19. Clinics and Practice, 14(4), 1601-1614. https://doi.org/10.3390/clinpract14040129